
Abstract
Pain assessment tools are often used by patients to report their pain and by health professionals to assess patients’ reported pain. Although valid and reliable assessment of pain is essential for high-quality clinical care, there are still many patients who experience inappropriate pain management. The aim of this scoping review is to examine an overview of how hospitalized patients evaluate and report their pain in collaboration with nurses. Systematic searches were conducted, and ten research articles were included using the PRISMA guidelines for scoping reviews. Content analysis revealed four main themes: 1) the relationship between the patient and nurse is an important factor of how hospitalized patients evaluate and report their post-surgery pain, 2) the patient’s feelings of inconsistency in how pain assessments are administered by nurses, 3) the challenge of hospitalized patients reporting post-surgery pain numerically, and 4) previous experiences and attitudes affect how hospitalized patients report their pain. Pain assessment tools are suitable for nurses to observe and assess pain in patients. Nevertheless, just using pain assessment tools is not sufficient for nurses to obtain a comprehensive clinical picture of each individual patient with pain.
Introduction
Approximately 50% of adult patients have pain when they seek health services, and more than 50% of adult patients experience pain as a symptom of a severe or acute illness. Pain can also affect the way physicians and nurses are able to determine the causes of patients’ diseases. In addition, insufficient health examinations can lead to inappropriate pain management.1
Acute pain occurs due to tissue damage that stimulates nociceptive nerves. The causes of pain include cell damage, childbirth, and different acute illnesses, such as cardiac infarction, ischaemic pain, and physical trauma, such as accidents or surgery. Acute pain disappears when the causes are eliminated or treated. If pain persists more than three months, the case of pain is classified as chronic. 2
Valid and reliable assessment of pain is essential for high-quality clinical care. Pain assessment is also necessary to determine the type of pain, whether pain management is adequate, whether analgesics or analgesic dose changes are required, and whether additional interventions are warranted, including whether specialty consultation is needed. Although pain is universally acknowledged to be a complex subjective multidimensional experience, different assessment tools are often used by health professionals.3 The most used pain assessment tools for acute pain in clinical settings are the Numerical Rating Scales (NRS), Verbal Rating Scales (VRS), Visual Analog Scales (VAS), and the Faces Pain Scale-Revised (FPS-R).3–6
Research has shown that pain assessments are not carried out properly by nurses. 7 Yin, Tse and Wong7 also pointed out that the less nurses know about pain treatment, the lower the quality of the patients’ pain treatment. High-quality pain treatment is associated with high-quality observations and assessments of pain. Pain is assessed by nurses based on the patients’ descriptions of their pain experience; for example, nurses determine whether the type of pain resembles squeezing pain, intermittent pain, or constant pain. Nurses often observe and assess patients’ pain by using pain assessment tools, as well as by communicating with the patients and using palpation and percussion methods. 8 Because studies have shown that nurses do not carry out pain assessment properly,1, 7 it is useful to examine hospitalized patients evaluating and reporting pain in collaboration with nurses.
Methods
Scoping reviews are useful for examining emerging evidence when it is still unclear what other, more specific questions can be posed and valuably addressed by a more precise systematic review.9–11 Furthermore, scoping reviews can report types of evidence that address and inform practice in the field and the way the research has been conducted. 9 , 10 Given the breadth of the topic, and to allow a comprehensive exploration and identification of the patient perspective, a systematic scoping review was performed based on the PRISMA guidelines. 11
Aim
The aim of this scoping review is to examine an overview of how hospitalized patients evaluate and report their pain in collaboration with the nurses.
Design
This scoping review involved literature searches of different databases, a critical evaluation of all the articles that were relevant to the study and an analysis, presentation, and discussion of the results of the scoping review. 11 , 12 The scoping review was conducted in accordance with the PRISMA guidelines. 11
Literature search
Defining the search terms using the PIO framework. 13
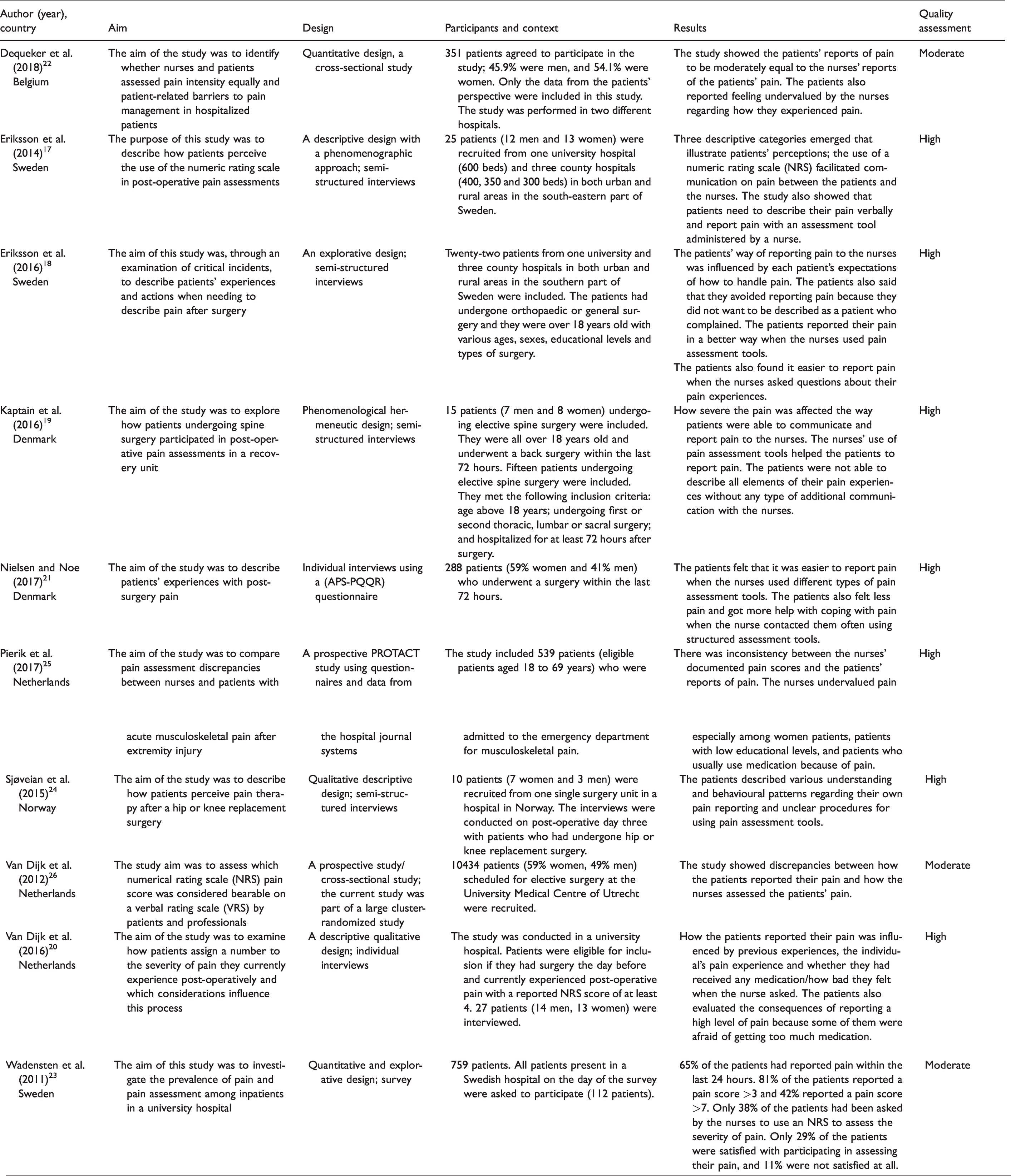
Characteristics of the included studies.
Peer-reviewed primary research studies that included how hospitalized post-surgery patients perceived the nurses observing, identifying, and assessing their pain.
Studies which described how patients at hospitals report their pain.
Studies in which the participants were over 18 years old.
Articles published after 2009.
Studies describing children’s, relatives’ or nurses’ experiences observing, identifying, and assessing patients’ pain.
Articles more than ten years old.
Studies from non-Western societies and non-Scandinavian or non-English-language studies were excluded to focus on studies conducted in contexts like Norway.
Editorials, meta-analyses, scoping reviews and literature reviews.
Search outcome
The literature search initially yielded 605 titles with relevance to the aim of the scoping review (see Appendix I). After duplicates were removed, 545 articles remained. These 545 articles were screened by reading the abstracts based on the defined inclusion and exclusion criteria, reducing the sample to 13. All articles were peer-reviewed, full-text articles written in English or a Nordic language. The full texts of the articles were read individually by all the authors, and ten articles remained after each of the 13 articles was assessed by using a methodological quality checklist appropriate for the method used in each of the different studies.14 Three studies were excluded because they did not pass the authors’ assessment of the studies’ methodological quality, due to limited ethical considerations and insufficient description of the strategy for recruiting the informants. The ten included articles in this scoping review were assessed to have moderate (three of the articles) or high (seven of the articles) methodological quality after an overall assessment process using methodological quality checklists. The main reason three of the included articles were assessed to have only moderate methodological quality was that only 63–75% of the patients who were asked, agreed to participate in the studies. The article selection process is shown in Figure 1 and the included articles are presented in Table 2. 15
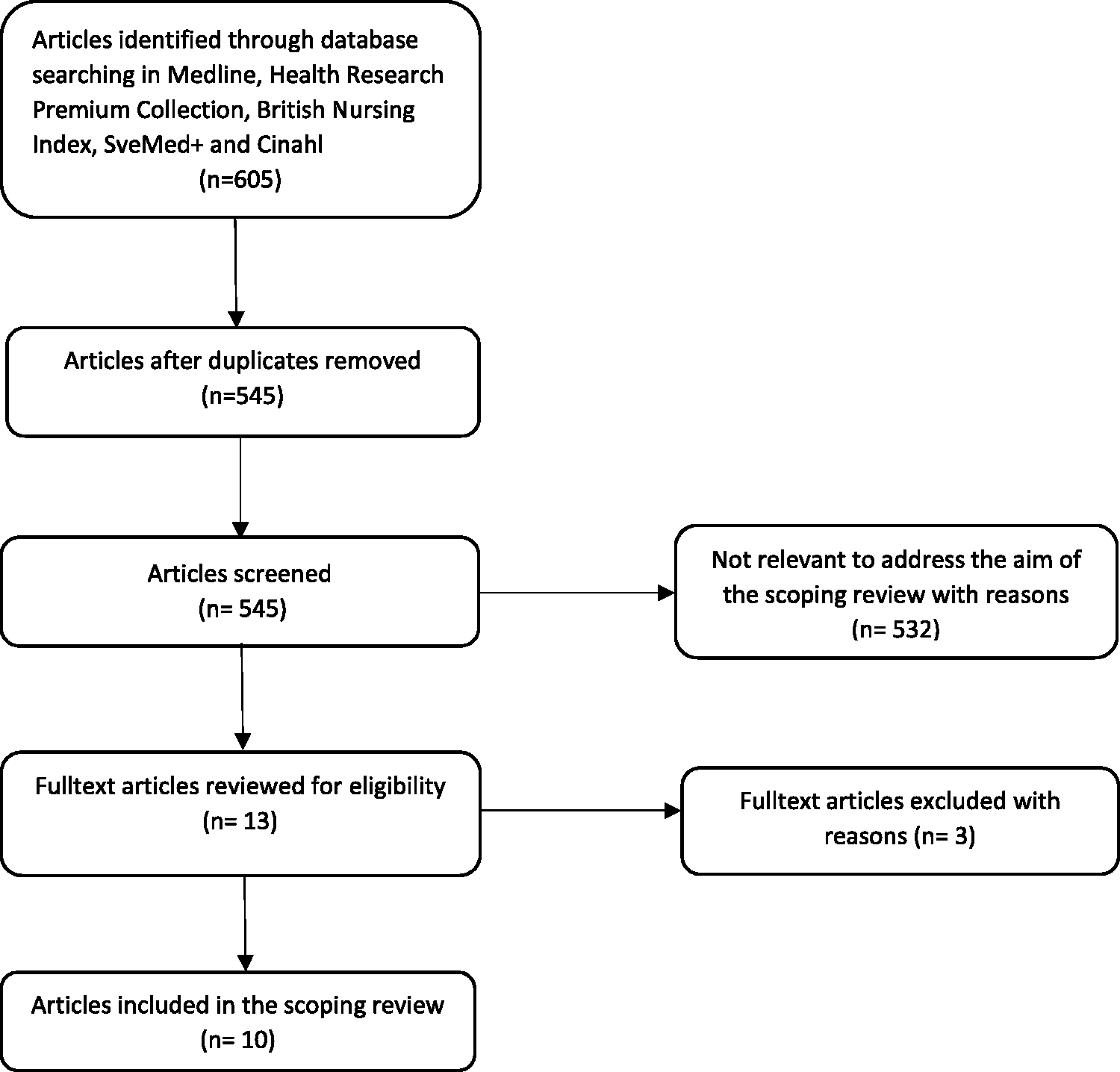
The article selection process.15
Data analyses
The data were analysed using content analysis based on Evans’s theory.16 Evans’s method for descriptive data synthesis is based on four phases, and is useful to analyze the findings from published interpretive articles in a scoping review.
16
Gather the sample of studies (already described in this scoping review), Identify the key findings of each study, Determine how these findings relate to those of other studies, and Bring common findings together to generate a description of the phenomenon.
The data were analysed to describe the data and to interpret and synthesize the findings. 16 The full texts of the results presented in all the articles were read by all the authors to summarize the main topics and key findings relevant to the aim of the study (phase 2).
The key findings, in the form of words or phrases, were then selected and condensed to become more manageable while the main content was preserved. The condensed material was marked, and codes were created based on similar findings in the different articles included (phase 3). Subsequently, all researchers searched for similarities and differences among the codes created during the condensation process, thus forming groups of related codes. This comparative analysis process resulted in the identification of four different themes after the researchers’ individually developed syntheses were compared and discussed (phase 4).
Results
The relationship between the patient and nurse is an important factor of how hospitalized patients evaluate and report their post-surgery pain
The relationship between the nurse and patient affected the way patients reported their pain to nurses.17–19 How a patient established trust with the nurse also affected whether they reported any pain and to what extent they described their pain. The patients also suggested that the nurses’ way of talking and asking questions about the importance of reporting pain affected whether they reported pain. If a nurse visited a patient often, the patient felt that it was easier to report whether the pain had increased or how they perceived the effect of the medicine they received.17–19
The response of the nurse when he or she realized the patient was in pain, especially in periods with high-intensity pain, was also an important factor for whether the patient felt comfortable reporting pain. The patients stated that the nurses’ availability and use of pain assessment tools increased their feeling of security in a demanding period in the hospital. When a nurse noticed that the patient was in pain, the patient felt that the communication with the nurse was more constructive and the patient’s level of pain and needs were assessed more accurately. The nurses’ levels of kindness and empathy were important for the pain assessment process. 17 , 18 , 20
Logistics and the nurses’ level of availability also affected how the patients felt the nurses met their needs. When patients noticed the nurses were in a hurry, they avoided reporting pain, even though the nurses told them to report pain. 18 , 19 The patients were often waiting for the nurses to assess their pain rather than asking for help. When patients misunderstand the importance of reporting pain and there is insufficient information provided by and communication with the nurses, unnecessary pain can occur. The patients often had problems communicating with the nurses because of high-intensity pain. The patients also wondered whether the nurses understood their pain reports because they often had to wait a long time for medicine. 17 , 18 The patients also misunderstood the importance of reporting any changes related to pain. In particular, mobilization led to more pain that was not reported, and the patients became paralysed and immobilized because of pain.17–19
Some patients found it hard to report pain by using numbers and pain assessment scales. They wished they had more information about when they should ask the nurses for more analgesics and how severe the pain should be before they call for the nurses. 18 , 19 , 21
The patients’ feelings of inconsistency in how pain assessments are administered by nurses
The patients stated it was difficult to report the severity of pain they experienced with dissimilar and inconsistent pain assessment approaches taken by the nurses. In many studies, the patients stated that the nurses used the same pain assessment scale in different ways and that different nurses used different pain assessment scales. 18 , 22 , 23 Wadensten et al. 23 reported that pain was assessed by using both pain assessment scales and clinical observations by the nurses in less than 7% of the patients. Dequeker et al. 22 and Wadensten et al. 23 found that pain was not assessed at all in 18–20% of patients with acute pain, and pain was assessed using an assessment tool in only 45.7% of the patients. 22 Pain was assessed by the nurses on the first day after surgery but not at all on the second day after surgery in some of the patients in the study by Eriksson et al. 18 When the nurses used different assessment tools and provided less help for patients to cope with pain, the patients trusted the nurses less. 19 Some of the patients received analgesics based on the NRS score, but other patients with the same NRS score did not receive any medicine. 19 , 20
The patients in the study by Eriksson et al. 18 thought that the nurses were responsible for initiating the pain assessment, but in the study by Sjøveian and Leegaard,24 the patients felt responsible for asking the nurses for help when they recognized changes. Some of the patients felt that it was difficult to ask for help, which can lead to the underreporting of pain. 24 Although the patients received the relevant information before the surgery, they often forgot the importance of reporting post-surgery pain. 18 , 23
In many of the studies, the patients misunderstood the way nurses were administering the pain assessment tools, which can lead to an underestimation of the severity of acute pain.17–20, 25 Some of the patients decided not to report pain so that they would get help when the severity of pain increased severely. A few of the patients also thought that nurses think patients report excessively high levels of pain to get more analgesics. 17 The patients who had reported a high pain score also experienced discomfort when the nurses asked different types of questions. When the nurses used different methods to assess pain, the patients felt confused and did not describe their pain in an optimal way. 17 , 18 , 20 , 25
The challenge of hospitalized patients reporting post-surgery pain numerically
Most of the patients stated that it was nice that the nurses used pain assessment scales and tools and that these tools increased the quality of communication between the nurses and the patients. Without information about how to assess pain, the patients felt that it was very difficult to grade their pain on a numerical scale. The patients mostly wanted to describe their pain verbally instead of using a scale.17–19
Other patients reported the severity of pain because they found it hard to select one number; for example, no pain, some pain, moderate pain, or bad pain. 17 , 18 , 20 , 24 The studies by van Dijk et al. 20 and Pierik et al. 25 showed discrepancies in how nurses defined unacceptable pain and how the patients described unacceptable pain. The patients reported a higher NRS score to get more analgesics than were routinely given by the nurses to patients with pain. In the study by Kaptain et al., 19 the patients suggested that it was difficult to report pain numerically because they often had different types of pain at the same time.
Previous experiences and attitudes affect how hospitalized patients report their pain
Women experience and report pain more often than do men. In addition, patients under 65 years old report a higher level of pain than do elderly patients. 21 , 23 , 26 The patients often felt that it was hard to report different types of pain because some had no previous pain experiences, while others had chronic pain that affected the way they reported, for example, acute pain after surgery. 19 , 20 , 26 Women also found it hard to report acute pain after surgery because they compared their situation with childbirth, which made them less likely to ask for help post-surgery. 20 , 26
In addition, patients’ attitudes related to using medication affected their way of reporting pain. As many as 40.7% of the patients found it hard to report pain, and 37.9% also found that communicating with the nurse about pain was difficult. Other patients were afraid of being addicted. 22 In addition, the patients did not know whether to, and felt anxious about, asking for more medicine because they thought they could be perceived as drug misusers. Often, the patients truly had severe pain but did not feel comfortable asking for help from the nurses.18–21
Discussion
The aim of this scoping review was to examine an overview of how hospitalized patients evaluate and report their pain in collaboration with nurses. This scoping review shows that nurses are the main health professional who works closely with patients when needed to assess pain. Nurses working at hospitals are responsible for observation and registration of patients’ pain, for example pain location, type of pain and level of the patient’s pain intensity.2
Due to their job description, nurses are also responsible for treating pain in patients, and reporting and discussing the effect of the given analgesic with doctors.2 This scoping review therefore showed that a well-established and trusting relationship between nurses and patients is important, and affects whether and how pain is reported by the patients and assessed by the nurses. In line with the conclusions of Diener, Kargela and Louw,27 we found that the relation between patients and nurses is important and affects the level of trust patients have with nurses and how well nurses can assess pain. A poor relationship will probably lead to the underreporting of pain, even when a patient has severe pain. Often, patients feel uncomfortable talking to nurses who they do not know during the vulnerable period of hospitalization. A lack of trust can therefore increase the risk of patients not reporting pain or incorrectly reporting pain, which can lead to severe consequences for the patients.
The scoping review also shows that patients report pain based on what they think the nurses expect them to report. Patients do not honestly describe the severity of pain they are experiencing to protect themselves from being suspected by the nurses of being drug misusers. Pain assessment conventionally has been viewed hierarchically, with the patient’s self-report as the ‘gold-standard’. To note, the ‘gold-standard’ was mainly designed for patients who have no cognitive or communication issues, which can exclude many patients from being able to report pain after a surgery. 28 Despite patients’ problems with expressing their pain, it is important for nurses to recognize the patient’s subjectivity related to their pain experience. The patients in a study by Haverfield et al. 29 were afraid of being suspected of lying about pain to get more medicine, which shows that patients do not report their pain correctly. 30 Therefore, nurses need to pay attention to the need for trustful communication with patients, which leads to a more honest and correct report of how patients experience their pain.
Furthermore, this review shows that patients lack an understanding of the importance of reporting pain for opiates in the period after surgery. Less knowledge or a misunderstanding of the given information leads to increased immobility of the patients because of severe pain. Patients therefore need to be provided with credible and customized information31, 32 for both pain assessment and pain treatment.
Among the healthcare professionals who care for patients with pain, nurses should be made aware of how nurses’ attitudes and knowledge of patients’ pain affect the quality of pain assessment. This scoping review also showed that nurses working in the same unit need to consistently and continuously use the same pain assessment tools to improve the assessment of pain in patients.
A surprising finding of this scoping review is that patients often believe that nurses do not believe patients are experiencing the severity of pain that they report. However, the experience of pain is subjective and differs by patient, which may explain why pain is often observed differently by the nurses. Vuille et al. 33 also found that nurses not to believe the patients’ pain reports if the nurses did not observe any clinical symptoms at the same time. The patient’s vital parameters do not need to be affected for patients to experience acute pain. 34 Many patients in the scoping review did not report pain if they knew that the nurses would ask questions, which showed that the nurses doubted the level of pain the patients reported. The patients would often be immobilized if they stayed in bed because of severe pain. Wiborg et al. 35 therefore pointed out the importance of nurses guiding patients in using pain assessment scales and acknowledging each patient’s individual experience of pain.
The nurses in this review often took a considerable amount of time to provide patients with analgesics when they reported an increased level of pain, which can be explained by nurses having little knowledge about pharmacology. 35 More than 50% of the nurses in the study by Granheim et al. 36 did not want to suggest opioids to patients before all causes of the pain were identified because pain relief can make it more difficult to identify the real cause of pain. Nurses often have insufficient knowledge about pain assessment and pain treatment,1, 36 , 37 and it is important to increase the knowledge of nurses so that they can assess patients’ pain in a holistic way8, 31 by developing health services that meet patients’ needs. To reach this main goal, nurses must use pain assessment tools as well as communicate clearly with, provide information to, and establish trusting relationships with patients.
Methodological discussion/limitations
The literature searches in this scoping review resulted in ten articles being included, which limits the generalizability of the results and the strength of the conclusions. Even though the literature searches conducted for this scoping review covered the databases believed to be of relevance, one cannot guarantee that all relevant existing research in the area was included.
This scoping review included ten articles from different journals and different European cultures and countries. It may be a threat to the scoping review’s external validity if the results are transferred in a more general context. 38 Since the ten included articles included are just from European countries, our results may be only partly applicable to the broad area of how patients with pain and nurses use pain assessment tools. In this study, possible cultural differences were not addressed, which could be a limitation. However, the results and conclusions of the articles were similar. This indicates that patients with pain report pain and perceive nurses’ ways of identifying, observing, and assessing pain similarly across different European countries. Another possible limitation is that the databases differ in their search strategies for the same topics. To minimize this limitation, the searches were carried out with the assistance of a university librarian.
‘Hospitalized post-surgery patients’ was defined as an inclusion criterion in this scoping review. Nine of the ten articles are based on data from patients who had been through a variation of surgeries such as hip and knee replacement, elective surgery, orthopaedic or general surgery. One article was based on data from hospitalized patients with musculoskeletal pain after extremity injury, which can be a limitation. However, the data from all the included articles were similar.
All ten included articles were considered to have moderate (3) or high (7) quality according to widely accepted critical checklists, which strengthens the validity of the scoping review. The inclusion of both qualitative and quantitative studies may have limited the comparability of the studies since the aim of this scoping review was to examine an overview of how hospitalized patients evaluate and report their pain in collaboration with nurses. Experiences are usually best described by using qualitative methods,12 but including studies which have been carried out using quantitative methods can also provide insight into the topic from different perspectives.
Data analyses are always influenced by the authors’ preconceptions. These preconceptions can be considered a limitation when researchers do not work reflexively throughout the whole process. 39 , 40 Therefore, throughout the analysis process, all the researchers discussed the analysed texts to reduce any bias due to prior knowledge on the research topic. The similarities and differences between themes were also assessed in these discussions to strengthen the study’s credibility and reliability. 36
Conclusion
The aim of this scoping review was to examine an overview of how hospitalized patients evaluate and report their pain in collaboration with the nurses. The findings show a variety of ways in which patients perceive nurses regarding the use of pain assessment tools, and some differences in how patients report their post-surgery pains in hospitals. The scoping review indicates that the relationship between patients and nurses is important for improving the quality of both the pain assessment process and the treatment of patients’ pain. In addition, the scoping review shows that nurses have a large influence on patients and can both promote and prevent patients from reporting pain. The nurses’ way of identifying, observing, and assessing pain is important to patients, and we conclude that nurses’ clinical competence in assessing pain is not sufficient. However, pain assessment tools and scales can help nurses assess pain when patients receive guidance and feel confident in how they can report pain.