
Abstract
In this article, we describe and critically reflect on how the PEPPA framework, a
Keywords
Introduction
Nurses in the emergency care department should be prepared to treat a broad variety of conditions, and care for patients of all ages. In the emergency department, medical competency is essential to make correct decisions based on patients’ anamnesis, symptoms and vital signs. However, nurses also need competencies within the caring paradigm to take on a holistic approach that allows person-centred care. To meet these varied needs, competence corresponding to the scope of practice of nurse practitioners (NPs) is suggested. NPs are advanced practice nurses ‘who has acquired, through additional graduate education (minimum of a master’s degree), the expert knowledge base, complex decision-making skills and clinical competencies for Advanced Nursing Practice, the characteristics of which are shaped by the context in which they are credentialed to practice’.
1
To support NP role development, implementation and evaluation in practice, a
Background
There is a long history of NP practice in emergency care in different countries around the world, including Australia, Canada, Holland, the United Kingdom and the United States of America. Researchers have found that NP practice in emergency care has a positive impact on the quality of care, patient satisfaction and waiting time reduction. 4 , 5 Some researchers have seen that NPs undertaking duties traditionally performed by junior physicians in acute hospital settings can have a positive impact on a range of indicators related to patients, staff members and organizational outcomes. 5 Furthermore, when compared to physician care alone, i.e. traditional models of care, NP practice has been seen to result in equivalent or better outcomes. 6 Nurses, including NPs, have a tradition to engage more in-depth with patients and significant others, building on creating a relationship attributed with trust, empathy and confidence, i.e. the foundation of establishing person-centred care. 7
Having understood that NPs can contribute to the provision of emergency care services, an emergency department (ED) management team in Norway chose to develop and implement an NP model of care. When this decision was made, the NP role in Norway was in its infancy and there was no NP education in the region. Consequently, an action research project entitled, ‘Providing person-centred healthcare – Development of new models of advanced nursing practice in cooperation with patients, clinical field and higher education’, was initiated (March 2015–June 2020). To date, 14 registered nurses affiliated with the local hospital’s ED have enrolled in the programme. To help in the development of the NP role, the PEPPA framework 2 , 3 was chosen to support the process.
The PEPPA framework is based on the principles of PAR and on a previous body of research on the implementation of advanced practice nursing roles. 2 The relevant principles in the framework are, ‘active participation in cycles of reflection–action; valuing what people know and believe by building on their present reality; collective investigation, analysis, learning, and conscious production of new knowledge; collective action in using new knowledge to address problems; and evaluating the impact of these actions’. 2 The framework includes nine steps, of which the first five are presented and discussed in this article: 1) Define patient population and describe current model of care; 2) Identify stakeholders and recruit participants; 3) Determine need for a new model of care; 4) Identify priority problems and goals; 5) Define the new model of care and NP role. 2
While the PEPPA framework has been widely used in research, practice and policies, the degree to which it has been used as intended, i.e. as a tool for supporting the NP development and implementation process, has varied. Therefore, the aim here was to describe and critically reflect on how the PEPPA framework was used to develop a new model of care for the NP role in an ED in Norway.
Setting
The setting for the project was an ED in a region in Norway with approximately 170,000 inhabitants. The studied ED provides 24-hour care for patients with medical, surgical or orthopaedic illness. The ED unit receives about 30,300 annual patient visits.
Materials and methods
In line with the PEPPA framework, different sources of material were used to support the process of developing a new model of care including the NP role. The research team performed two rounds of semi-structured interviews with nurses and representatives from the management team at the studied ED: at the beginning (December 2015 and March 2016) and midpoint (January 2017) of the project. The interviews are described elsewhere. 8 , 9 Observations were performed on two separate occasions (January and June 2017). One of the authors (EB) shadowed nine nurses working in the ED for a total of 40 hours. The nurses were recruited through convenience sampling, and to facilitate the collection of data during the observations, a structured observational instrument was developed.
Five workshops, which were recorded, were arranged to engage stakeholders and obtain their points of view. The workshops were led by the project leader. The international definitions and scope of practice of NPs as well as how new NP roles could be implemented in Norwegian acute care settings were discussed. In addition, grey literature, such as national directives, work descriptions, statistical reports and scientific papers were searched.
Ethical considerations
Permission to perform the interviews and observations was obtained from the Norwegian Centre for Research Data (NSD; Ref. no. 37218/2 and 50160/3). Informed consent was collected from the healthcare organization responsible for the study setting and all participants.
Description and reflections on the implementation of the PEPPA framework to develop a new model of care for an emergency department
Here, we describe how the PEPPA framework guided our work to develop a new model of care including the NP role, and we reflect on the process from a PAR perspective.
Step 1: Define patient population and describe current model of care
The first step in the PEPPA framework is to define the patient population, how patients enter the healthcare system and the current model of care. 2 In this project, this included an assessment of the principles of access to healthcare in Norway, and assessment of the ED setting including visitor statistics, job descriptions, interviews and observations of nursing staff.
In PAR projects, the establishment of a common ground based on a shared understanding is important. 10 While the staff in the ED were familiarized with the current model of care, the project’s research team was international and had limited literacy in the Norwegian healthcare system, including how patients enter the healthcare system and ED policies and routines. From this process, we all learnt that the Norwegian healthcare system is founded on the principle of universal access and is mainly financed by taxation. A ‘gatekeeper system’ is used to determine a patient’s need for emergency care. As a rule, a patient first enters the healthcare system through contact with his/her general practitioner (GP) or via an emergency primary health centre. Accordingly, the majority of those coming to the ED have undergone a first assessment. From a PAR perspective, this collaborative learning process can be considered a ‘discursive validation’ through which knowledge was generated; 10 knowledge that was vital for discussions between the research team, stakeholders and participants.
Step 2: Identify stakeholders and recruit participants
The second step is to identify stakeholders and recruit participants. According to Bryant-Lukosius and Dicenso, 2 ‘(S)takeholders include patients and families, advocacy groups, volunteer agencies, healthcare organizations, the healthcare team, professional associations, support staff, administrators, educators, and government agencies involved in health policy and funding. Stakeholders represent vested interests, values, perceived power and expectations’. Also, ‘Participants refer to stakeholders involved in implementing the framework. The term participant rather than stakeholder is used to reflect the active role individuals play in defining tasks and working as planners, learners, data collectors and decision-makers’. 2
In the current project, the stakeholders included the healthcare organization responsible for the study setting, the ED, the staff working at the ED, the local university, patients visiting the ED and these patients’ significant others. The participants included the head physician overseeing the ED, the ED management team, the NP students, and the research team.
From a PAR perspective, the participation of stakeholders and participants is important, because intersubjectivity and practical wisdom are significant in the pursuit of objectivity. 11 We found the inclusion of the head physician, ED management team and NP students to be crucial. The project would have benefited from greater involvement from the nurse management team, and even the involvement of organizational administrators responsible for financial management and the planning of staff resources and skill-mix would have been positive.
As per the PEPPA framework, patients’, significant others’ and care providers’ perspectives should be included. We made a decision not to actively engage patients and significant others in this process, based on the understanding that patients in need of emergency care can be considered particularly vulnerable and as such deserve protection. Instead, results from relatively recent research on patient satisfaction in the studied context were taken into consideration. One could consider the lack of patients’ and significant others’ involvement here to be a limitation. Engagement of patients and significant others has become a cornerstone of quality of care, even in organizational design and governance, and we would strongly recommend others to involve them in this type of project. Views of patients and significant others can provide insights into effectiveness and satisfaction of care, and will be heard in the evaluation of the NP practice in future outcome analysis.
Step 3: Determine need for a new model of care
In the third step, the strengths and limitations of the current model were assessed from various perspectives to determine the need for a new model of care. It was found that the ED’s patient flow was slowed down because of hold-ups in medical assessment and/or treatment. Another issue was that, generally speaking, patients needed to repeat their story and/or answer the same questions again and again because of a relatively high number of staff transitions (for example nurse–physician transitions). A high number of staff transitions can lead to key information being missed because it is not delivered to the correct individual. Furthermore, we found that patients with non-urgent conditions (conditions for which a delay of several hours would not increase the likelihood of an adverse outcome) could experience long wait times, e.g. patients with minor orthopaedic conditions, such as ankle or wrist injuries. Patients with chronic and/or palliative conditions, who often seek help because of a deterioration of general health or the need to adjust pain relief, were also seen to experience long wait times. We saw that both of these groups were triaged as low priority. As one participant stated: The point is you see that there is nothing acute with these patients … they perhaps only come in for rehydration or [so on]. And what triage [score] are they given? They are not given a 2nd or a 3rd either. Probably a 4th. And on a busy day, when the ED is full and more [are coming], so they consequently [lay there]. Yes … and they in fact [lay there] a lot longer than they should … because they are [given low priority].
In literature on change management, it is argued that to succeed with leading change a ‘driving force for change’ or ‘a sense of urgency’ is needed. 12 Here, we saw the research team as helpful, from an outsider perspective, to identify and formulate the needs in concrete form; a process that can be challenging for those working in the context on a daily basis. This work continued in the fourth step.
Step 4: Identify priority problems and goals
In the fourth step, a more complete understanding of patient needs and the strengths and limitations of the current model should be developed. 10 The slow treatment of patients with non-urgent conditions was found to be a problem. To help resolve this problem, it was decided that NPs would care for a specific group of non-urgent conditions, defined in the project as patients with minor orthopaedic injuries (injuries in the elbow or distal of the elbow, or distal of the knee; more specified in Boman et al. 13 ). The goal was for wait times for non-urgent patients to decrease without compromising patient safety. Another prioritized group was orthogeriatric patients with hip fractures, and another goal was set up: orthogeriatric patients will undergo a comprehensive assessment, and adherence to care guidelines for hip fracture patients will be improved. Lastly, a more overarching goal with NP practice was formulated: that the person-centred approach will be strengthened, including the improvement of the information given to patients and patients’ significant others.
Early in the process, the stakeholders and participants were actively engaged in the organized and recorded workshops (i.e. formal discussions) together with the research team. When the focus of the dialogues changed from structural to more practical issues, discussions became more informal and mainly occurred in the ED setting. In the ED setting, an NP student part of the management team acted as the link between the unit and the research team. During this process, the stakeholders became less involved. In that the richness of perspectives was reduced, the ‘perspective validation’ may have been reduced, which can be seen as a threat to objectivity; the possibility for an open democratic dialogue may have been threatened. 11 We nonetheless maintain that this can be considered beneficial, because in PAR one of the challenges is to ensure full participant collaboration, through which participants drive the process. Moreover, we maintain that the inclusion of the most knowledgeable persons, who have rich and extensive experience of the praxis inherent to the setting, increased ‘intuitive validation’. 10 Thus, we recommend that the participants are empowered and get to ‘own the process’. It is, however, important to have a sounding board, in this case the research team, reflecting on practice from an outsider perspective.
Step 5: Define the new model of care and NP role
In the fifth step, the new model of care, including the NP role, should be defined. This, while also determining whether there was evidence-based research that support the proposed changes. 2 We used the Nursing Role Effectiveness Model, 14 which is based on the Structure–Process–Outcome model of quality care, 15 to define the proposed new model of care. In the Nursing Role Effectiveness Model, it is assumed that there are relationships between structure, process, and outcome, i.e. the different roles that nurses assume and the outcomes of nursing care. In that model, structure consists of the nurse (experience, knowledge, and skill levels), patient (personal and health-related characteristics, e.g. age, type and severity of illness) and organizational (staffing, nursing assignment patterns) variables that influence patient care. Process consists of nurses’ independent (activities initiated that do not require a physician’s order), medical-care related (functions and responsibilities associated with implementing medical orders and medical treatments), and interdependent (activities and functions that are partially or totally dependent on the functions of other healthcare providers) roles. Outcome consists of nursing-sensitive patient outcomes (prevention of complications, symptom control, knowledge of the disease and its treatment, management of side effects, functional health outcomes, satisfaction with care, and cost) (cf. Irvine et al. 14 ).
The new model of care will enlist orthogeriatric patients with hip fractures (Figure 1) and patients with minor orthopaedic injuries (Figure 2). The model includes NPs that should hold a NP master’s degree; a degree that is preceded by a minimum of three years of relevant work experience (relevance is assessed by management team).
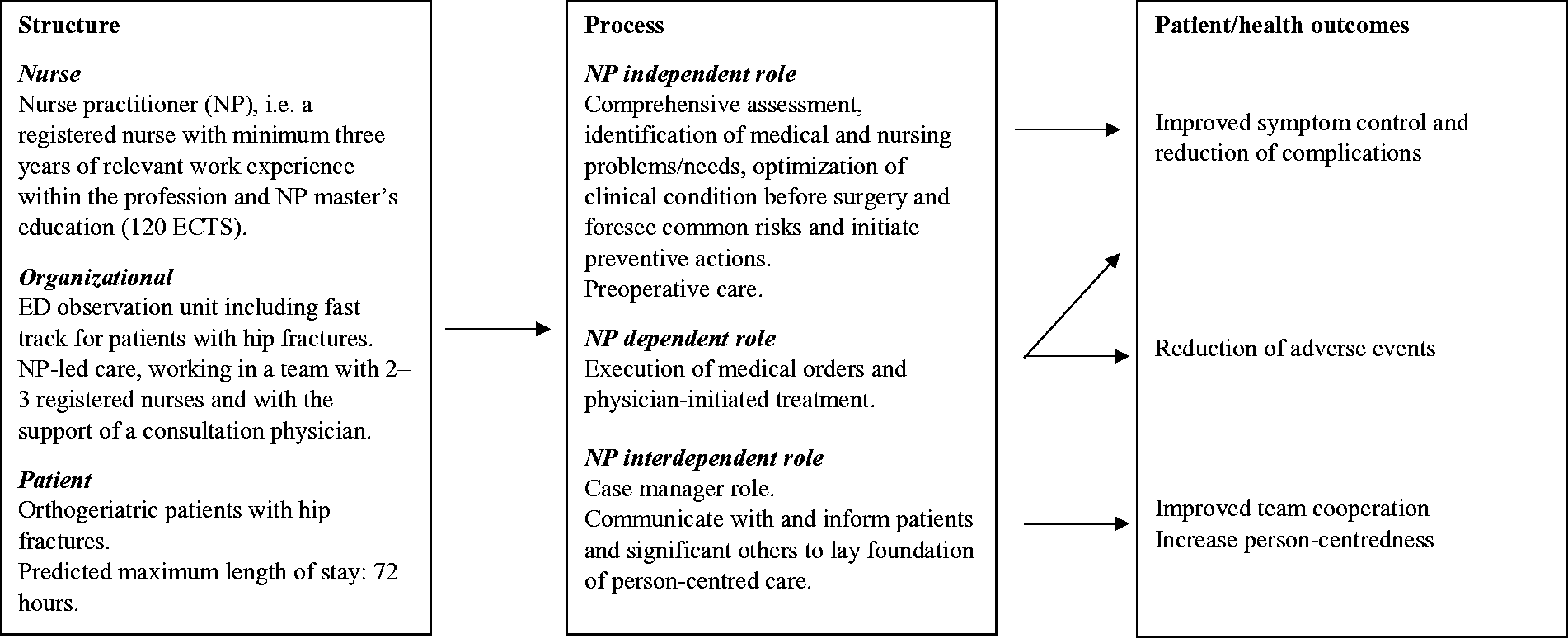
The nursing role effectiveness model for orthogeriatric patients with hip fractures.
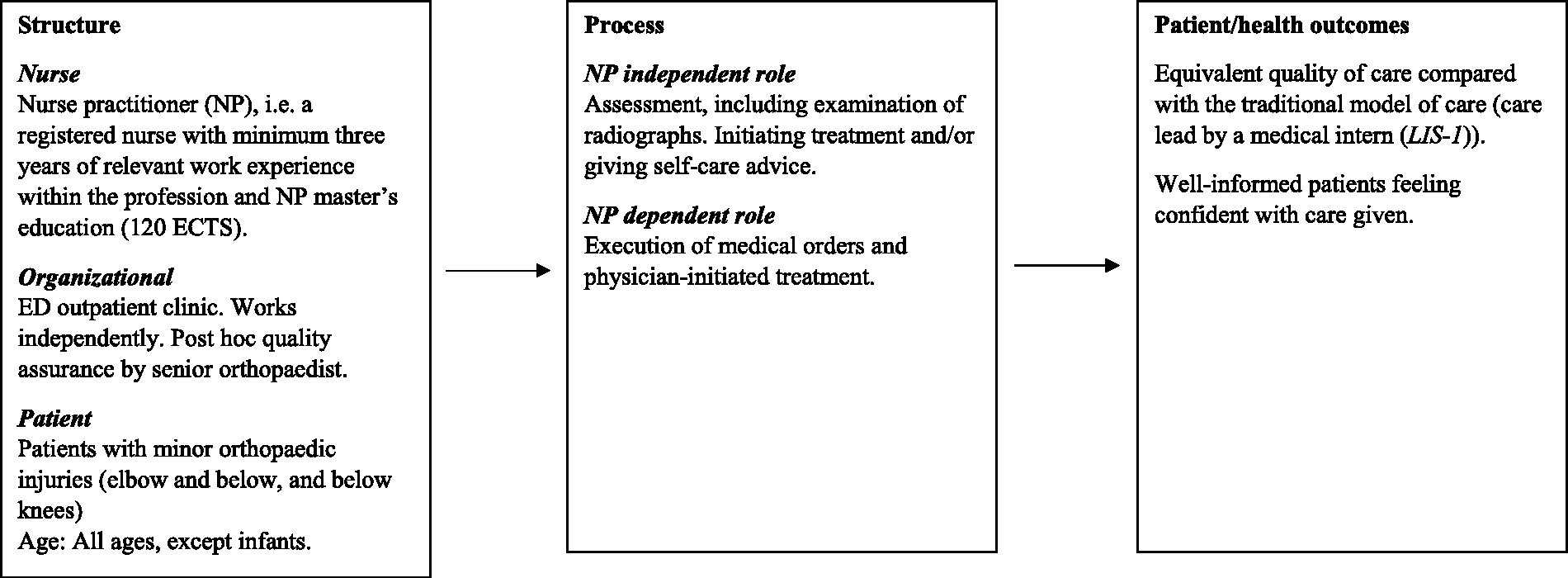
The nursing role effectiveness model for patients with minor orthopaedic injuries.
The orthogeriatric hip fracture patients will be cared for in a NP led fast track unit. The NPs will be working with a team of registered nurses and be supported by a consultant physician. The NPs will independently make a comprehensive assessment, identify medical and nursing problems/needs, optimize the patients’ clinical condition before surgery, and foresee common risks and initiate preventive actions. As NPs in Norway do not have prescriptive authority, prescription of drugs is an NP dependent role, together with other physician-initiated treatment outside NPs’ scope of practice. The nurse interdependent role includes regular preoperative care, and to communicate with and inform patients, significant others and the healthcare team (responsibility shared with the registered nurses). The NPs will also take on a case manager role, as the orthogeriatric patients often are in need of multi-professional care. The model is assumed to result in improved symptom control and reduction of complications, reduction of adverse events and improved team collaboration and person-centred care.
Regarding patients with minor orthopaedic injuries, patients at all ages (except infants) will be cared for by NPs in the ED outpatient clinic. The NP will work independently, including making assessments and initiating treatment and/or self-care advice. The NPs can consult physicians if needed, and a post hoc quality assurance by a senior orthopaedist is included in the model. The model is assumed to result in equivalent (or superior) quality of care compared with the traditional model of care (care lead by a medical intern (LIS-1)), and well-informed patients feeling confident with the given care.
To support the new model, a literature review was undertaken. Having found sufficient evidence, we then sought to answer the question of whether there was evidence that the proposed new model of care would be effective. Based on our findings, we argue that it will be (and is) effective. It is assumed that the model can be evolved gradually. However, it has been considered important that the scope of practice initially is limited so the NPs can grow in confidence in their new roles. They have years of work experience from the emergency field (or similar). In the new model they get to practice core competences in the NP practice, beyond the scope of registered nurses. 1
Conclusion
This is the first project in which the NP role has been implemented in emergency care in Norway. To support the process the PEPPA framework was used. Inspirational ways of developing contextual solutions suitable for a particular workplace are needed, and we maintain that we have undertaken a pioneering path to the development of a new model of care for EDs in Norway. Even though here it is applied in the Norwegian emergency care context, the overall comprehension is that the PEPPA framework is not context bound, and can be recommended to an international audit and beyond emergency care.
By using the PEPPA framework, we claim that a purposive and trustworthy resolution for the concerns relevant to an ED setting has been found, and the process, supported by the framework, will contribute to the improvement of praxis. We have supported the transferability of the process by seeking to document our knowledge and experiences so that others may integrate them into their own inquiry.
In this article, the first five steps of the framework are described and discussed. We initially anticipated that the new model of care would be fully implemented by now, but the last three steps have only just been initiated. This is due to organizational changes outside of our control, economic restraints, tenuous support from the management team and the COVID-19 pandemic. Some pilot tests have been performed, whereafter revisions in the implementation strategy have been made. A protocol for outcome studies has also been set up. 13 While we have demonstrated the applicability of the PEPPA framework, we conclude that the process has not been straightforward. It is noted that to communicate and establish the new role in a setting as demanding as an emergency department takes time.