
Abstract
Teaching practical topics is a central part of nursing education. The aim of this study was to describe the teaching of practical topics to nursing students at clinical skills centres (CSCs) in Sweden regarding organisation, structure and content. Data collection consisted of structured and open-ended questions through telephone interviews with responsible educators at all Swedish Universities (n = 25). The analyses consisted of descriptive statistics and compilation. The results showed that teaching of practical topics varied, depending on each university’s pre-requisites, and a lot of resources were needed. Teaching at CSCs enabled integration of practical and theoretical knowledge. Having large student groups and confusion over terms hamper the teaching, and there was lack of a specific education for the educators at CSCs. Teaching practical topics at CSCs is a complex task, and educators need competences in nursing, theoretical knowledge and pedagogy.
Introduction
Teaching nursing students at clinical skills centres (CSCs) has become an important element in nursing education, both nationally and internationally. 1 During nursing education, students should be taught practical topics at CSCs or in clinical practice or both. However, there are no national guidelines for teaching practical topics in Sweden; thus, each university usually decides independently, based on the curriculum, syllabuses and the university’s resources.
In Sweden, nursing education is governed by the Higher education ordinance, 2 and the Higher education law. 3 Furthermore, nursing students engage in nursing studies at universities. Sweden also has national examination objectives for nursing education 4 pertaining to the European Union directives 2005/36/EC and 2013/55/EU. 5 , 6 European Union directives are related to the competence description for registered nurses, specifically stating that the objectives in nursing education should be achieved with numerous hours of clinical practice. The education is also governed by the university’s subject description, nursing ethical codes 4 and competence description for registered nurses. 7 Nursing education takes a total of six semesters, and the education has objectives for the bachelor of science degree in nursing/caring and the professional qualification for registered nurses. In Sweden, a national handbook can be used as a guideline in healthcare and in education. The purpose of the handbook is to provide overall guidelines for current evidence of clinical knowledge, related to instructions and working methods for healthcare. 8
Teaching at CSCs is a pre-requisite for healthcare students’ learning of practical topics. 9 , 10 Therefore, several universities use teaching at CSCs as a source of support and supplement to the learning, which includes different forms of simulation. 11 The CSCs can be situated either at a university or in a hospital. Additionally, some universities replace clinical practice time with CSC hours. 12 There are positive outcomes for using simulation in teaching practical topics; however, it cannot replace the hands-on patient care work with real patients in clinical practice. 13 Simulation teaching is not unique for nursing education; for example, it is also used in military and maritime education. 14 , 15 Teaching and learning at CSCs are complex, 16 where practical and theoretical knowledge are supposed to be integrated, 9 offering students the opportunity to develop professional identity. 13 Further, the practical topic plays a role in nursing education 13 as it is part of the profession; inability to perform these tasks can have impact on patient care. 17 Therefore, it is required that educators teaching at CSCs have extensive knowledge about practical topics and pedagogical ability. 18
Definitions that will be used in the article.
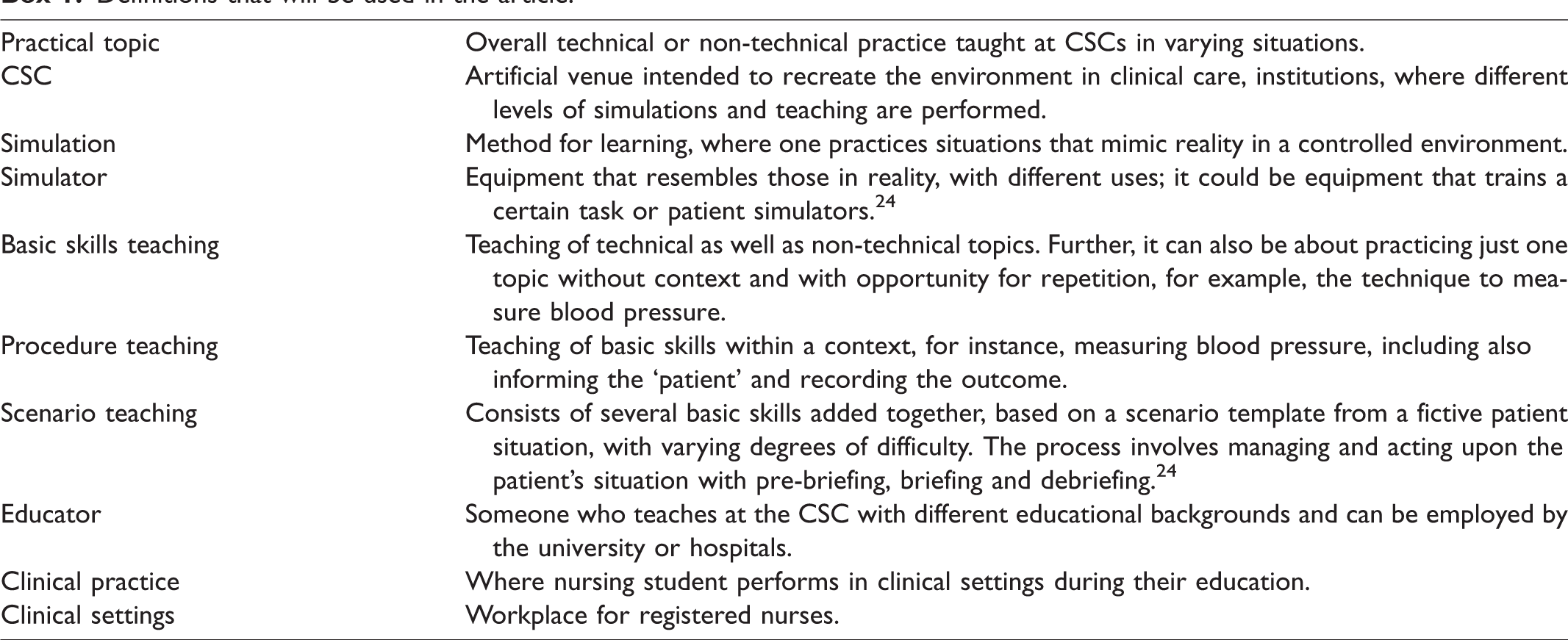
The teaching and learning process for practical topics in nursing education can be performed in different ways, and there are varying pedagogical frameworks, for example, implicit/tacit knowledge, 21 novice to expert 25 and experiential knowledge. 26
Nursing students are expected to become aware of and manage practical topics in their clinical practice and to be prepared to work as novice nurses. 27 Therefore, students are taught practical topics at CSCs to be prepared and to ensure patient safety. Previous studies have focused on one or few teaching topics or criteria at CSCs, 28 , 29 but a description of general teaching at CSCs is missing. Therefore, investigating teaching at CSCs can be useful for educators at CSCs and for clinical settings where nursing students develop their practical knowledge and profession. To the best of our knowledge, there is a gap in existing research literature about what is generally taught at CSCs, with regard to practical topics. Therefore, the aim of this study was to describe the teaching of practical topics to nursing students at clinical skills centres (CSCs) in Sweden regarding organisation, structure and content.
Methods
Design
The study has a descriptive design based on a total mapping with a questionnaire-based telephone interview.
Samples and settings
All 25 universities providing nursing education in Sweden were invited and agreed to participate. The participants were responsible educators at Swedish CSCs, they were between the ages of 29 and 63 years and their experience of teaching at CSCs was between 1 and 15 years.
Data collection
Programme managers at each university received an email with information about the study and a request for responsible educators at CSCs. Two reminders were sent. Information about the study and the questionnaire were sent by email to the responsible educators at CSCs, chosen by the programme manager. A time was scheduled for the telephone interview. Data were collected by the first author (MT), based on a questionnaire with structured and open-ended questions during the interview. The participants answered verbally and had the ability to speak freely during the recorded telephone interview. The interviews, conducted during September 2017–February 2018, were audio-recorded and lasted between 35 and 55 minutes. One responsible educator preferred to respond with written responses.
Questionnaire
The research group developed a questionnaire based on clinical experience and content in existing syllabuses. The questionnaire was pilot tested with two responsible educators at two campuses, and minor adjustments were made. The final version of the questionnaire consisted of 35 questions, including open-ended questions, with the ability to make comments during the interview. The questionnaire had six background questions as well as questions in three main domains according to practical topics. The three domains (organisation, structure and content) emerged during construction of the questionnaire; thereafter, the findings were described according to these domains. There were 12 questions about organisation at the CSC (structured, n = 8; open-ended, n = 4), and 14 questions related to the structure of the CSC (structured, n = 14). Finally, three questions referred to the content in the CSC (open-ended, n = 3). The questionnaire also contained questions about examinations, which will be presented in a forthcoming study.
Analysis
The quantitative data were analysed with descriptive statistics, using the statistical programme Statistical Product and Service Solutions (IBM SPSS Statistics) version 24.0, regarding the frequency and median, which were used to summarise the data. The open-ended questions and comments were transcribed by professional transcriptionists and the first author (MT) and then verified by co-workers. With reference to Patton, 30 the text was read through several times, and compiled according to identified similar content and then organised together.
Ethics
The study was approved by the Regional Ethical Board of Linköping (Dnr 2017/379-31). Participants received verbal and written information about the study’s purpose, arrangement, and presentation of the results and gave their verbal consent before the interview. Participation was voluntary, and participants could withdraw at any time without giving any reasons. The data were handled confidentially; the responses were presented at group level and could not be attributed to any specific person and/or university.
Findings
This section begins with general information about the participants, followed by the results of the data analysis separated into three parts: organisation, structure, and content, from all Swedish universities (n = 25).
Two men and 23 women, aged 29–63 years (median 50 years) participated. Their professional titles were lecturers (n = 15), senior lecturers (n = 6), associate professor (n = 1), CSC coordinator (n = 2) and other title (n = 1). The academic degrees were bachelor’s (n = 1), master’s (n = 16) and PhD (n = 8). Twenty-two of the participants had passed the compulsory higher education teacher training in Sweden. They had between 1 and 15 years (median 6 years) of experience teaching at the university or CSCs.
Organisation
Universities formation
The number of students admitted at each university was between 88 and 250. There were several educators involved in teaching at the CSCs, and the majority of the educators were registered nurses. Furthermore, they had different affiliations such as university (n = 25), hospital (n = 8), and university and hospital (n = 7). The appellations of the CSCs were: CSC (n = 17), Clinicum (n = 1), Competence Centre (n = 1), Method exercise room (n = 2) and other (n = 4). The CSCs were situated at the university (n = 13), hospital (n = 5) or both university and hospital (n = 7). The teaching at the CSCs was performed during all semesters (S); S1 (n = 22), S2 (n = 21), S3 (n = 23), S4 (n = 14), S5 (n = 18) and S6 (n = 21). Sixteen universities out of 25 conducted specific evaluations about teaching at the CSC.
Education for educators at CSCs
There was a lack of specific education for the educator to teach at CSCs. At 17 universities, educators received some type of education. In the open-ended questions, the participants described that the education they received was based on compulsory higher education teacher training; problem-based learning (PBL); and a model for practical skills performance, Research in Nursing Skills (RiNS). The most common was internal education, for example, involvement in networks and conferences. Some attend national conferences. There are a few things like that. Otherwise, I would say that it is collegial continuing education. (Participant 20)
Pedagogic discussion
In the open-ended questions, participants emphasised that the educators’ pedagogic discussions were about teaching at the CSC, and the arrangement of the discussions differed. Some universities had formalised meetings for CSC educators, but there were also informal discussions among CSC educators. However, the following common issues were highlighted: The teaching strategies and administration of courses related to discussions about distribution of resources, for example, materials and educators. It also related to priority about which practical topics should be taught at CSCs versus during clinical practice. What lessons learned should we convey to those in clinical practice and how much do they need to train at the CSC. (Participant 14)
A common issue regarding teaching strategies was how to construct the teaching ‘in the best and similar way’, using the same terms and in accordance with guidelines. We talk a lot about this thing with consensus, that we do the same and we say the same thing. It is something we get in the evaluations from the students, ‘yes, but you don't say the same thing’. (Participant 19)
Advantages, disadvantages and challenges in teaching at CSCs
In this section, the responses were from open-ended questions. The participants reported that teaching at CSCs enabled the integration of practical and theoretical knowledge and also developed the students’ knowledge in order to increase patient safety. As such, the teaching was based on allowing safe and structured proceedings by, for example, permitting students to make mistakes without injuring a real patient, rehearsing the practical topics and getting constructive feedback. Further, participants advocated that teaching in small student groups is a pre-requisite for learning. Disadvantages were large student groups, teaching in several campuses, distance education, having many educators involved, lack of realism and fidelity of the materials and the simulation. These disadvantages could result in difficulties, e.g. by hampering the teaching quality. It was a challenge to have a general structure of the teaching at CSCs as well as distinct progression over the semesters related to the objectives of the course. Another challenge was that teaching at CSCs requires a great amount of resources. Educators perceived teaching at CSCs as having positive effects, and they wanted more teaching time for the students at the CSC. One reason for this was that students had limited time in clinical practice. An additional challenge was the lack of evaluation tools and relevant research about best teaching methods for use at CSCs. We do not use any measurements, we have nothing to build improvements on because there are different opinions and no basis for them. (Participant 2)
Structure
Pedagogic methods and educators
Among the overall pedagogical strategies at the universities, the most common strategies were mixed with elements of various pedagogic methods, for example, combination of case-method and traditional lecture (n = 11), case-method (n = 4) and problem-based learning (n = 3). Seven universities had no specific strategy. The teaching at the CSCs was performed in different courses, integrated into clinical practice (n = 11), caring/nursing sciences (n = 24), medicine sciences (13) and/or a specific CSC course (n = 4).
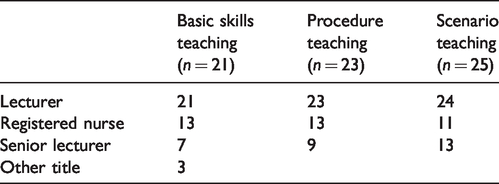
There were several educators involved in teaching at each CSC. All 25 universities had scenario teaching, and educators had a high-level academic degree, compared to basic skills teaching where educators were registered nurses or lectures (see Table 1). Teaching assistants, i.e. nursing students, were also used as source of support when the students practiced on their own at the CSC. Some universities (n = 6) also provided interprofessional learning.
The educators’ titles, related to the university’s type of clinical skills centre teaching, at the universities (n = 25).
Learning activities
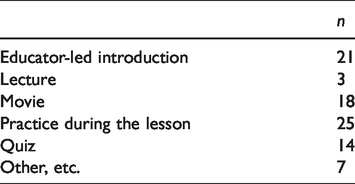
Table 2 displays the learning activities. At all universities, the common denominator was students’ opportunities to practice during the lesson.
Learning activities.
Teaching and practicing time
Total hours of teaching per student at the CSC, at each university during the education, varied between 0 to 40 hours plus, and are displayed in Figure 1.
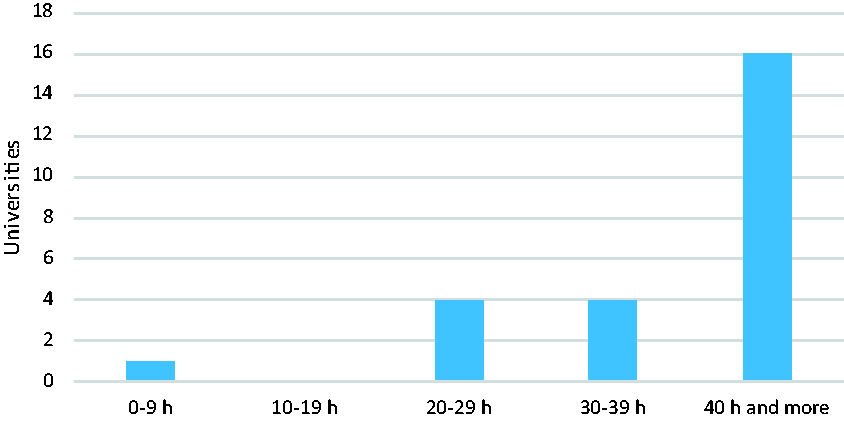
Total hours of teaching per student at clinical skills centres.
Students at 19 CSCs had the opportunity to practice on their own at the CSC. However, there were different pre-requisites before one could do this, for example, students must have undergone teaching in the practical topic beforehand; other requirements were attending during the specified opening hours and the need to have an employee at CSC present.
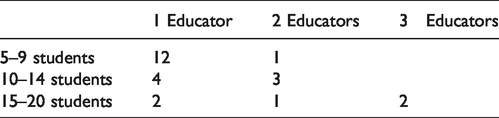
Group teaching was used at all CSCs (see Table 3). It was also mentioned that some of the teaching at the CSCs required more educator capacity, depending on the practical topic.
Number of students per group and educator quantity.
Content
Teaching of practical topics
Table 4 provides a description of the topics taught. The most unusual topics were ostomy care and removing sutures, and the most common topics were, for example, injections, blood pressure and venous sampling.
Teaching topics.
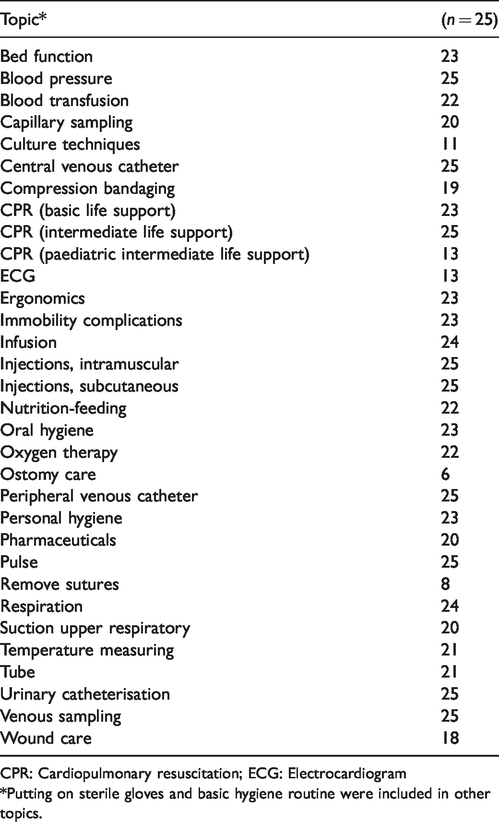
CPR: Cardiopulmonary resuscitation; ECG: Electrocardiogram
*Putting on sterile gloves and basic hygiene routine were included in other topics.
Objectives of the teaching at CSCs
The participants pointed out the objectives by answering the open-ended questions. The objectives of teaching basic skills included that teaching be performed in a safe environment with a focus on learning regarding content, guidelines and sequence, relating to the topics. Another aim was to get acquainted with the material used in the specific practical topics. The teaching and practice at CSCs gave the opportunity to repeat the practical topic before performing on a real patient.
The objectives of teaching skills in procedure included basic skills teaching, which progressed within a context. For example, to put things together by combining practice and theoretical teaching and getting an understanding of the topic. Teaching skills in procedure also meant gathering information on the specific patient’s situation, for example, to communicate, observe and record.
The objectives of teaching about scenarios included teaching basic skills and procedure, aiming to develop progression in preparing students to handle various situations. This required students to focus on leading, being able to delegate, systematically reporting relevant data, immersing oneself in the practical topics and being a team player.
The overall focus of teaching was to combine learning how to perform an examination and objectives with the goal of a progression. There was also a focus on the general teaching process including, for example, the nursing process, documentation and basic hygiene routines. Each teaching session included patient safety and focused on preparing students to be able to succeed in clinical practice in their future profession.
Discussion
The findings reflect a summary of the teaching on practical topics at CSCs. Specifically, the aim of this study was to describe the teaching of practical topics to nursing students at clinical skills centres (CSCs) in Sweden regarding organisation, structure and content. However, there were some discussions about what practical topics ought to be taught and whether they should be taught at CSCs or in clinical practice. Nonetheless, the teaching of practical topics at CSCs varied. Furthermore, educators at CSCs had different educational backgrounds, but most of them were nurses with academic degrees. To provide structure for the discussion the results are discussed based on what, by whom and how the teaching was performed at CSCs.
The results showed that all universities mostly offered similar practical topics, even though there are no national guidelines regulating what practical topics students should be taught. There was an ongoing discussion among educators about whether the practical topics should be taught at CSCs or in clinical practice. Teaching at CSCs has several benefits; for example, it prepares students in practical aspects before clinical practice, allows for repetition, reconciles practice with theory and takes place in a safe environment. 9 , 28 The findings in the earlier studies are in accordance with our own results. Further advantages are that students get the opportunity to practice on less known and/or complex practical topics, which may reduce patient injury. Disadvantages of teaching in clinical practice are the growing number of students 31 and the stressful situation of the clinical setting; in this context, caring for the patient has precedence. 32 Nevertheless, teaching at CSCs cannot completely replace all the learning of practical topics in clinical practice. 13 Combining teaching at CSCs and in clinical practice may increase the learning pre-conditions. However, an earlier study showed that students experienced a disconnect in the teaching between the CSC and clinical practice. 33 Hence, cooperation and teamwork between educators from CSCs and tutors from clinical setting are required. This could be a considerable challenge as there are several organisations and many people involved in nursing education. Another challenge nowadays is the presence of virtual simulations and artificial intelligence, which could be used for educational purposes.
There were differences regarding who performed the teaching at the CSCs. The educators had different educational backgrounds, but most of them were nurses with academic degrees. Apart from this, there is no pronounced competence requirement for educators who teach at CSCs. The CSC educator’s role is not the same as the educator’s role in a regular classroom 16 or in clinical setting. 34 Topping et al. 18 describe that the educator’s role at CSCs includes several aspects, e.g. the educators had an awareness of teaching in an artificial venue with simulators. They would also perform and show practical topics integrated with theoretical knowledge. This implies that educators at CSCs need to have competence in performing nursing tasks as well as pedagogical knowledge. This study indicates that educators partially achieved pedagogical education, but this was limited for teaching at CSCs. Nevertheless, the educators expressed that teaching should be based on evidence, both in pedagogy and in the practical topic, which is congruent with findings from an earlier study. 18 It seems as though the pedagogical element has not been prioritised in teaching at CSCs; moreover, a literature review showed that pedagogical theories were not always explicitly described in studies about teaching at CSCs. 35 As a result, teaching at CSCs and pedagogy can be interpreted as two parallel tracks that do not always intersect. There are pedagogical frameworks that can be used in teaching at CSCs, for example, Waldner and Olson 36 describe that Benner’s nursing skill acquisition theory 25 and Kolb’s experiential learning theory 26 could be applicable. The results showed that educators discussed pedagogical issues with teaching at CSCs in varied forums. However, further structured discussions are needed, both regarding pedagogy and the topics, to develop the teaching. To be an educator who possesses different areas of knowledge requires that the university creates pre-requisites and learning environments. Collaboration in teams and exchanging experiences are also needed, thus allowing educators with different backgrounds to learn from each other. Elmgren and Henriksson 37 require that the management provide a certain structure for discussions as well as the framework for teaching. More research and knowledge are needed on how and in which form this should be organised. 38
The results also showed considerable similarities on how to propose teaching at the CSC on practical topics, e.g. having a progression during the education period and connecting the teaching to the syllabus. These findings are congruent with those of an earlier study. 34 However, teaching at CSCs is dependent on each university’s possibilities to structure the education, for example, how the syllabus is formed. Moreover, access to resources has an impact. One similarity between the CSCs was that students could practice during the lesson. The handbook for healthcare 8 is used as a guideline, but does not describe how the teaching should be performed. This resulted in differences, not only between universities but also within the same university. Participants described that students expressed that educators used different terms, which made it confusing for them. This can be due to teaching embracing many different concepts and parts, e.g. it integrates both specific and alternate contexts and in different degrees, with integration of practical and theoretical knowledge. 22 Another difference was the hours of teaching at the CSC: 16 universities had 40 hours or more for each student, and the others had fewer hours. The results point out that teaching at CSCs is small part of the total 4,600 hours of nursing education. 5 Nevertheless, it is not possible to draw any general conclusions on the hours of teaching at CSCs. However, the pre-requisites for teaching practical topics differ; therefore, it is difficult to have a national consensus. Although developing tools, support and guidelines for teaching at CSCs is an ongoing process, the question arises as to whether they are facilitating or limiting. To have guidelines that can be followed for the teaching is beneficial. It can also be limiting when the focus of the teaching may be on a checklist or imitation. This shows that teaching is challenging and complex and emphasises that educators need educational support to teach practical topics at CSCs.
Methodological considerations
A strength in this study was that all universities providing nursing education in Sweden participated. The data were collected via telephone interviews based on a questionnaire with structured and open-ended questions, where participants could make comments during the interview. Questionnaires with a telephone interview are considered as a strength, for example, motivating participants to answer all questions and also clarifying the questions to avoid misunderstandings, thus reducing the drop out. 39 In this study, participants had the opportunity to ask for and receive clarifications on the questions. They were interested and motivated to participate and thereby created a basis for rich data. The interview and the open-ended questions were chosen to give the participants the opportunity to elaborate on their responses. Participants were responsible educators at CSCs. One limitation could be that only one participant represented each university. However, the participants claimed that each university used the same syllabuses or teaching at the CSC. It was challenging to develop a questionnaire related to all the different concepts in the area, but at the same time, this was one of the reasons why the interest in studying this area came up. Further, the participants’ interpretation of the concepts could have an impact on the results, but they were aware of the descriptions of the content for each question. The structured questions were at a descriptive level; hence, descriptive statistics was chosen for the analysis. The open-ended questions and comments were compiled with similar content and were identified and organised together, which seemed to be suitable for this study.
Conclusion
Teaching of practical topics at CSCs is complex, and many factors affect performance. Universities in Sweden have different pre-requisites for teaching, and there is no national consensus about teaching at CSCs, which can be a challenge. Nonetheless, universities strive for optimal teaching performance. However, this issue may open up for national discussion on which practical topics should be taught at CSCs, educators’ competence, and also where and how the teaching should best be performed, in relation to the constant development and changes in healthcare and education. Nonetheless, the study was conducted within nursing education in Sweden; however, there ought to be an interest in nursing education for other countries related to European Union directives 2005/36/EC and 2013/55/EU. The findings could be transferable to other countries that have similar nursing education, for example, European countries. Collaboration in teams and exchanging experiences are also needed. This study has begun to explore the teaching and learning at CSCs; however, more research is needed. One area that needs to be illuminated is examination and compulsory education related to teaching and learning at CSCs.