
Abstract
There is a lack of studies on ethical responsibility in nursing. Nurses experience ethical responsibility in all settings where patients are exposed and vulnerable. The authors’ interest in public health and intensive care nursing provided a motivation to study these settings. The study aimed to explore how intensive care and public health nurses experience ethical responsibility. A qualitative design was chosen and 10 individual interviews were carried out. The data were analysed using hermeneutic phenomenological analysis. The study is reported in accordance with COREQ. Levinasian ethics provided the theoretical framework. The analysis resulted in four themes: Feeling alone, Feeling worried and uncertain, A sense of satisfaction, A personal commitment. Even though the settings differed, experiences of aspects of ethical responsibility were the same. Further in-depth studies in different settings can enhance an understanding of moral responsibility and facilitate the development of a theory of ethical responsibility in nursing practice.
Introduction
Ethical responsibility is fundamental in all nursing practice. Nursing values and responsibilities are guided by a professional code of ethics. 1 Nursing values become evident when nurses express their moral response to human vulnerability in ethically charged encounters. When a nurse expresses his or her ethical responsibility, it is related to a sense of obligation to respond in an ethically sound manner that is grounded in respect for human dignity. 1
Ethical responsibility is a cornerstone in Levinasian philosophy. 2 , 3 Levinas describes this responsibility as a response to an appeal that comes from the face of another person, i.e. ‘the Other’. 2 The face, in Levinasian terms, is an important metaphor for human vulnerability, a vulnerability that reaches out and demands our response. 4 The face is not necessarily a physical face as we know it; the appeal that demands a response can come from other body parts, such as the nape of the neck or even the untidy hair of a teenage boy. 4 According to Levinas, ethical responsibility for the Other is not something we choose or can explain. It is personal, and we are faced with a demand that we cannot avoid, ignore, or transfer. 2 According to Levinas, we are prisoners in our responsibility for others; we are commanded to respond.2–4 Ethical responsibility is, in this sense, asymmetrical. This is a different understanding of asymmetry than the traditional understanding of asymmetry in power structures in healthcare settings. Ethical responsibility is a fundamental phenomenon and an inherent part of being human. 4
The concept of ethical responsibility as understood by Levinas 2 , 3 and its dimensions in public health nursing were developed further in a study by Clancy and Svensson. 4 The study involved interviews with experienced public health nurses. The nurses shared experiences from their everyday practice. Using the philosophy of Levinas as a framework, an in-depth analysis was carried out. Interrelated aspects of ethical responsibility emerged from the nurses’ narratives. Their analysis of public health nurses’ stories revealed the personal nature of ethical responsibility and how it is connected to boundaries; temporality; worry, fear and uncertainty; being alone; and a sense of satisfaction.
Responsibility is a widely used term in nursing. In this text, its meaning is related to an ethical approach to caregiving. Ethical responsibility concerns our duty to others and our response to their appeal for help. 4 A review of the literature from 2000 to 2020 revealed that there is a limited number of studies on ethical responsibility in nursing practice. Existing research has studied the concept of responsibility in its relation to aspects of ethics within the field of caregiving. Morally laden questions about responsibilities are inherent in all healthcare. Nathaniel developed a theory of moral reckoning based on research into intensive care nurses’ experiences of moral distress. 5 The theory highlighted critical stages in nursing practice related to morally troubling patient-care situations.
Other studies have highlighted responsibility and the importance of reflecting on ethical dilemmas, 6 and the asymmetrical nature of responsibility. 4 , 7 How ethically charged encounters influence professional identity in public health nursing has also been considered. 8 Research related to responsibility and moral distress has revealed emerging ethical issues related to teamwork, end-of-life decision-making, privacy, interaction, and healthcare access.9–11 Relational aspects of moral responsibility as experienced by student nurses revealed their need for a moral space to do good and advance nursing practice. 12
The interrelated aspects of the concept of responsibility, as linked to similar concepts such as courage, have received some research attention. A concept analysis of moral courage in nursing revealed that responsibility was found to be one of the attributes of nurses’ moral courage. 13 Exploring how nurses respond to ethically charged situations can reveal interrelated aspects of ethical responsibility in nursing practice. This study seeks to contribute to the awareness of nurses’ experiences of ethical responsibility in intensive care nursing and public health nursing. Public health nurses work mainly with healthy populations, whereas intensive care nurses work with critically ill patients. The authors have experience as both public health nurses and intensive care nurses, and discussions among the authors on ethically charged encounters in both settings generated an interest in exploring the phenomenon of responsibility in these two nursing groups. The study can contribute to the development of a more comprehensive understanding of what is contingent to each nursing field and what is consistent in both. Consistencies can reveal aspects of the essence of ethical responsibility in nursing practice, while contingencies reveal specific challenges specialist nurses face. The results of this study can contribute to a deeper understanding of ethical responsibility in nursing practice. Therefore, the aim of this study was to explore how ethical responsibility is experienced by public health nurses and intensive care nurses and thus promote an understanding of this, often tacit, dimension of nursing practice. The findings can contribute towards developing a middle-range theory of ethical responsibility in nursing. Nursing is a practical discipline. However, theory development in the field of ethics is important, as it can provide direction for nursing research and guide professional practice. 14
Method and design
This qualitative study has a hermeneutic phenomenological design inspired by van Manen. 15 Data were collected through interviews and analysed using a selective highlighting approach. 15 The design is both descriptive and interpretive. This study is reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ). 16
Context
The study took place in two different regions in the north of Norway. The interviews with public health nurses took place in the communities where they worked, and the interviews with intensive care nurses took place in quiet rooms in a hospital setting.
Recruitment and sample
The sampling strategy was purposeful. 17 Access to the research field was established through verbal and written inquiries to nursing leaders, who then contacted the nurses for possible participation in the study. The researchers then communicated with the nurses, who consented in writing and chose the time and place for the interviews. The inclusion criteria for the purposeful sample were nurses with more than five years’ experience of clinical practice as public health nurses and intensive care nurses. The public health nurses worked in small municipalities (populations < 10,000). The intensive care nurses worked in hospitals in medium-sized municipalities (populations >10,000). The public health nurses had postgraduate education in health promotion and prevention to prepare them to meet the needs of their target population group (children aged 0–20 years and their families). The intensive care nurses were specialised nurses who provided care for critically ill patients in highly specialised units. The participants were between 30 and 60 years of age. Due to issues of confidentiality, we will not provide further details of the sample. One experienced nurse with three years’ experience as an intensive care nurse (ICN 4) wished to participate and was included in the study.
Data collection
Rich descriptions provide the starting point for researching lived experiences, and van Manen 15 recommends the semi-structured conversational interview as a suitable method for gaining access to a deeper and richer understanding of our ‘life worlds’. Data were collected through 10 semi-structured interviews between July and October of 2016. Ten nurses were interviewed: five public health nurses and five intensive care nurses. The researchers informed the participants of their goals and reasons for performing the research. They encouraged the nurses to narrate their experiences of ethical responsibility as freely as possible. If the researchers needed clarification or more in-depth descriptions, they asked the nurses to elaborate further about the experience. The authors had prepared an interview guide (Figure 1).
Interview guide.
The first author, an intensive care nurse, interviewed the intensive care nurses, and the second author, a public health nurse, carried out the interviews with the public health nurses. The researchers decided that having a common background with knowledge of the field could create trust and facilitate follow-up questions. The interviews were recorded and transcribed. The average length of each interview was approximately 1 hour.
Data analysis
Van Manen’s 15 approach was considered relevant for this study as it is discovery orientated and concerned with unique aspects and variations of lived experience. Van Manen suggests that phenomenological interviews produce experiential accounts in narrative form and that philosophical insight can give deeper insight and thoughtful reflection on meaning. 18 In this study, Levinasian ethics provide philosophical insight into ethical responsibility. 4 According to Van Manen, 15 the research process starts before the fieldwork begins and continues throughout the whole process of writing until the work is completed.
The authors chose an open inductive approach to the nurses’ stories in order to remain open to the emergence of new dimensions of ethical responsibility. All 10 interviews were read to gain an understanding of the text as a whole. The collected data were deemed sufficient to develop an understanding of the nurses’ experiences of ethical responsibility. The text was re-read several times and possible interpretations were discussed by the authors before reaching consensus. The selective highlighting approach was used. 15 This entails highlighting significant sentences or phrases that described the participants’ experiences related to ethical responsibility. The highlighted text was then grouped into relevant themes as the researchers developed an understanding of the data. The rigorous process of grouping and re-grouping the selected findings resulted in four main themes: Feeling alone, Feeling worried and uncertain, A sense of satisfaction, and A personal commitment. To ensure transparency, an example of the analytical process of forming a significant sentence into a theme is provided in Table 1, and quotations from the participating nurses are included in the results.
Example from the analysis process: from text to theme.
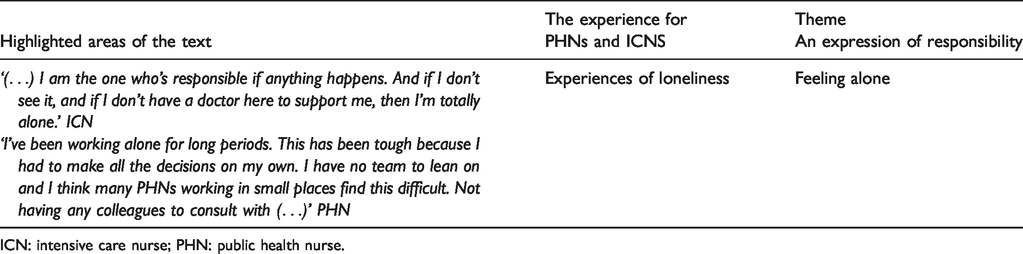
ICN: intensive care nurse; PHN: public health nurse.
Ethical considerations
The declaration of Helsinki 19 and the Convention on human rights and biomedicine 20 provide a basis for ethics in research. The welfare and integrity of the participants in the research project is always prioritised over the interest of science and society. The Norwegian Social Science Data Services and the Regional Ethical Committee reviewed the research protocol. Ethical deliberations were taken into consideration throughout the study. 21 All participants were given written and verbal information and could withdraw from the study at any time. Written consent forms were signed by all the participants. The research team had no previous relationship with the participants. The authors have strived for transparency in writing up the research and discussed how their own personal experiences could influence interpretations of the collected data. Being a researcher in one’s own field requires awareness of the authors’ presuppositions and the challenges they impose. Transparency ensures that the researchers’ reflections are made as visible as possible.
Findings
The participants spoke about ethical issues and responsibilities in their work as public health nurses and intensive care nurses. The nurses were concerned about ethical responsibility. Both nursing groups felt that they lacked a suitable setting for ethical reflection and that they had no formal meeting points to discuss ethical issues with colleagues, leaders, and supervisors. They spoke of the loneliness of their responsibility and a need for greater focus on ethical dilemmas related to interdisciplinary collaboration. Reflection on the nurses’ stories showed the emergence of common themes related to moral responsibility, despite the differences in their remit and working environments. The findings are presented under four main themes: Feeling alone, Feeling worried and uncertain, A sense of satisfaction, and A personal commitment.
Feeling alone
The theme Feeling alone reflected the public health and intensive care nurses’ experiences of being alone with their worries and responsibilities. The public health nurses often worked alone in the community, whereas the intensive care nurses worked in teams and helped each other with practical issues. The intensive care nurses expressed that although they were never physically alone in the unit, they could experience feeling isolated with the responsibility for a critically ill patient, especially when the other nurses were busy. One intensive care nurse stated: I am the one who’s responsible if anything happens. And if I don’t see it, and if I don’t have a doctor here to support me, then I’m totally alone. (ICN 4)
The intensive care nurses spoke about feeling alone in ethical decision-making. They were also concerned about the lack of collaboration with doctors on ethical issues. They could experience that doctors and nurses had no formal meeting points, except for a short stop at the patient’s bedside during the doctors’ rounds. They expressed a dependency on collegial support. As one intensive care nurse said: We have a lot of responsibility. (ICN 3) I’ve been working alone for long periods. This has been tough because I had to make all of the decisions on my own. I have no team to lean on and I think many public health nurses working in small communities find this difficult. (PHN 2) I am only a public health nurse. (PHN 3)
Feeling worried and uncertain
In the theme Feeling worried and uncertain, the respondents spoke about experiencing worries and uncertainties related to having too little time to perform their duties and constantly having to prioritise. One intensive care nurse spoke about the unpredictability of life in the ICU: The work pace here varies greatly. From being very calm and peaceful … to during the course of a few hours, having six patients admitted … You have to be able to adjust at the drop of a hat. (ICN 4) When we start our shift and see the patient lying in a blood-stained, unkempt bed, unshaven, with very poor oral hygiene, and we take over and think … yes, they [the nurses on the other shift] have had other priorities. (ICN 2) It’s unpredictable, but at the same time, this offers a range of possibilities … we can spend more time on the cases that require more time. (PHN 4)
A sense of satisfaction
The theme A sense of satisfaction reflected positive experiences of ethical responsibility and how the nurses felt proud of having the chance to make a difference in people’s lives. A public health nurse said: The majority of people see the value of having us here. We have a status of sorts. (PHN1) It’s often when they’re at their most vulnerable … things they can’t tell anyone else, they share with me. (PHN 3) We had a dying patient; the ICU was full and we had to look after a patient and his relatives (behind screens) in a fully occupied four-bed unit. This was not a desirable situation. The nurses made the best of the situation. The relatives’ only focus was their sick father. (ICN 5) They should be able to leave the ward no matter the outcome and know that we have done our best and feel that they have been looked after in the best possible way. (ICN 5)
A personal commitment
In the final theme, A personal commitment, the participants spoke about the personal nature of their responsibility to others. They had to decide how to deal with and follow up on demanding situations. They spoke of how their personal commitment could intensify their feelings of responsibility. A public health nurse spoke of how her personal involvement with pupils at school evolved over time. She shared a story about a little boy who told her that he had been physically and psychologically abused by his mother and stepfather. She described him sitting in front of her in her school office, restless, with tears in his eyes and facial tics. She said: He was in third grade, a tiny little thing. (PHN 5)
An intensive care nurse (ICN 1) gave an example of experiencing personal involvement in a situation. She suspected that a critically ill postoperative patient was bleeding internally. The nurse called the surgeon who wanted to wait and not re-operate; this resulted in a heated discussion. The surgeon eventually came. The patient collapsed and was rushed to the operating theatre where they discovered that the patient had haemorrhaged. The operation saved his life. The nurse said that her professional values, knowledge, and personal integrity gave her the courage to use her convictions to insist that the surgeon came.
The intensive care nurses in the study spoke about challenges in collaborating with physicians, especially when they had different viewpoints on ethical issues. The intensive care nurses felt that doctors sometimes carried out procedures and treatments that the intensive care nurses felt were unethical. To illustrate this, an intensive care nurse said: I feel that the doctors often want to administer more treatment than the nurses do … I think that, without having any numbers to substantiate this, that they’re prolonging life. They administer additional treatment … non-invasive ventilation, or with older adults and very ill patients, they initiate blood pressure treatment. (ICN 3) We weren’t allowed to remove the mask. So, she had it on when she passed away. (ICN 2)
Discussion
Public health nurses and intensive care nurses experienced ethical responsibility when dealing with a wide range of ethical issues and dilemmas. Interpreting the nurses’ stories shows that both nursing groups experienced ethical responsibility as both rewarding and challenging. The nurses felt a deep personal responsibility for, and connection with, their patients and service users. Intensive care nurses spoke of acute dramatic episodes and short, and intense, relationships with their patients, whereas public health nurses had longer-term relationships. The public health nurses often felt alone in ethically challenging, complex situations that necessitated involvement over time. Although the intensive care nurses did not work alone, they experienced feelings of loneliness in their understanding of the ethical aspects of prolonging treatment.
Feeling alone is a recognised dimension of ethical responsibility in public health nursing. 4 Clancy and Svensson attributed physical and existential loneliness to the very nature of public health nursing. 4 It seems that the public health nurses in this study experienced both physical and existential loneliness, whereas intensive care nurses, although not physically alone, felt alone in their understanding of certain cases and in promoting core nursing values. The nurses expressed a need for support in dealing with difficult cases. The importance of supportive colleagues and having an arena for discussing ethical issues was important for all the participants. Support did not necessarily entail physical presence in dealing with a situation; it could also entail collegial support after an event. Involving colleagues in discussions of ethical issues can increase awareness by viewing a situation from different perspectives. 22
Ethical responsibility can require the courage to define boundaries and say ‘no’. 4 As this study illustrates, it can also require the courage to demand involvement. The intensive care nurses felt a need to discuss ethical aspects of prolonging treatment in end-of-life care with doctors. They were concerned about the discussion of ethical issues in inappropriate settings, and that the knowledge of nurses should be recognised as an important contribution to ethical decision-making. Rapidly changing situations in an ICU setting required qualified and timely support, while dealing with uncertainty in ethical dilemmas was described as a burden. A multicentre study on ethical decision-making illustrates how nurses’ lack of involvement in ethical decision-making can lead to moral distress and burn out. 23 Moral distress is one of intensive care nurses’ major problems and can be experienced due to invasive or inadequate treatment of patients, or even through the uneven distribution of power. 5 , 24 Shared moral work can alleviate negative feelings of responsibility and contribute to sound practice. 9 , 10 , 12 , 25 , 26 Collegial support is also important for community nurses. 27 This study shows the importance of collegial support and a designated time and space for ethical reflection for both nursing groups.
The nurses spoke about the unpredictable nature of their work. Working alone with the responsibility of prioritising cases increased their burden of responsibility. Clancy and Svensson described ‘worry and uncertainty’ as a dimension of ethical responsibility in public health nursing. 4 The intensive care nurses also spoke about the responsibility and uncertainty of monitoring very ill patients. According to Fernandes and Moreira, 9 the ICU is an area of uncertainty, which can lead to dangerous situations and raise ethical concerns amongst professionals. Being alone with worries and uncertainties caused ethical deliberations and added to their experiencing ethical responsibilities.
The intensive care nurses and public health nurses voiced their opinions when they felt that basic moral values and sound nursing practices were endangered. Taking responsibility requires courage. 12 Believing their actions were morally sound gave them confidence. In abuse cases, public health nurses have a responsibility to alert social services; dealing with conflicting values in child abuse cases was a cause for concern for public health nurses. The public health nurses had a strong sense of duty towards service users. In Suzuki et al.’s study on abuse cases, the public health nurses always prioritised the protection of health and life. 28
The public health nurses’ responsibility can be to refer cases, even though they cannot decide the outcome of the referral. When their involvement did not have the desired outcome, they experienced feelings of guilt. Courageous nurses are those who take responsibility and act according to core nursing values. 12 Setting boundaries for medical interventions that prolong the life and suffering of old and very sick patients was a major concern for intensive care nurses. Although treatment and its termination will always be the responsibility of a physician, Cronqvist has noted the importance of nurses’ voices in these matters. 22 Allowing a patient to suffer from unnecessary medical interventions only stalls death, making it morally justified to allow a suffering patient to die. 22 Both nursing groups spoke about the aftermath of living with cases that had not been resolved in a satisfactory way. Tasks can be overwhelming, and courage is needed to limit involvement and define boundaries. 4 Tillich 29 writes that courage is recognised as an ethical concept that affirms self-worth.
The public health nurses in this study felt included and appreciated as professionals. This does not necessarily mean that their ethical responsibility was resolved or clear-cut. In the study by Clancy and Svensson, public health nurses experienced challenges related to worries, uncertainties, and unclear boundaries. 4 The findings in this study also suggest that intensive care nurses and public health nurses experience personal commitment, worry, uncertainty, and self-doubt as dimensions of ethical responsibility. According to Levinas, ethical responsibility is personal; it is only the person who is deeply involved who knows and feels the enormity of the situation. 4 This study has given insight into experiences of ethical responsibility in two nursing settings. Empirical studies on ethical responsibility guided by a philosophical framework can contribute towards development of a middle-range theory in nursing. Theory development is important in nursing practice as it enables analysis of clinical decision-making and creates an understanding of what happens in a complex practice. 14
Strengths and limitations
The scope of this study is limited, but the findings can be transferable to similar settings and provide a starting point for further studies on ethical responsibility. The study was carried out in 2016; no substantial changes have occurred in the study settings and the findings are considered to have continued relevance. The public health nurses in the study worked in small or medium-sized municipalities, and their experiences of loneliness could be related to the small size of municipalities and the small number of nurses. However, public health nurses can also feel isolated in larger municipalities. 30 The authors are aware of the danger of deductive analysis by being too reliant on the findings of former studies. It can also be argued that looking at the dimensions in one nursing group could lead to a focus on similar themes in the other group.
The researchers interviewed nurses from their own field. Being a researcher in one’s own field requires that the researcher is attentive to presuppositions and the challenges they impose. 17 To safeguard against this, the researchers had an open inductive approach to the interviews and the analysis. The authors have strived for transparency and all authors discussed possible interpretations and contributed to the analysis process. Writing up qualitative research is always a creative process of meaning-giving influenced by interpretation. 12 Interpretations must, however, be substantiated, and other interpretations are always possible. Direct citations from the nurses support and validate the findings.
Clinical implications and conclusion
Creating a formal setting for ethical reflection by nurses and their collaborators can help to shed light on difficult issues, heighten ethical responses, alleviate feelings of loneliness, and facilitate support. Although public health nurses and intensive care nurses conduct their everyday work in completely different settings, they experience similar dimensions of ethical responsibility. The findings also promote a more in-depth understanding of interrelated aspects of responsibility and the importance of courage in defining boundaries in both of these nursing groups. The findings can be relevant in nurse education and practice in the development of critical thinking. The study contributes to a deeper theoretical understanding of the concept of ethical responsibility in professional nursing practice. The findings also provide guidance for further research.
Examining the perspectives of doctors and intensive care nurses, as well as public health nurses and their collaborators, in relation to ethical decision-making is an important area for future research. Focus groups and individual interviews within these professions could provide more insight into their perspectives. Nurses need management support and the time and space for interdisciplinary collaboration and ethical reflection. This research has highlighted situations where nurses need support. It is necessary to carry out research on ethical responsibility in other nursing groups, and to study in more detail how nurses can be best supported.
Footnotes
Author contributions
Study design: AST, ABO and AC; data collection: AST and ABO; data analysis: AST, ABO and AC; manuscript preparation: AST, ABO and AC. All the authors have seen the latest version and agreed upon it.
Acknowledgements
The authors would like to thank the nurses who participated in the study and extend a special thanks to Head Librarian, Jan Frode Kjensli, University Hospital of Northern Norway for his rigorous database searches.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.