
Abstract
In Norway, more patients are visiting the out-of-hours primary clinic than before, and with a higher urgency level. As the first out-of-hours clinic in Norway, the leader at one medium/large clinic wanted to introduce the role of nurse practitioner (NP) for more effective and safer service for patients. The aim of this study was to explore challenges in the current model of care and whether NPs can perform new tasks in an out-of-hours clinic seen from both care providers’ and patients’ perspectives. All general practitioners and registered nurses who took part in out-of-hours shifts and patients classified as urgent priority during one week were invited to participate in a survey. Descriptive statistics and a chi-square test were used to identify statistically significant differences between groups. Long waiting times in the clinic and lack of patient information during waiting time were identified. General practitioners (GPs) were skeptical about task shifting, while the registered nurses and patients were more positive. All groups agreed that nurse practitioners could perform advanced assessment of patients until a GP took over. Possible new tasks were stitching wounds, referral to X-ray and treating lower urinary tract infections.
Introduction
Access to primary healthcare (PHC) services has become an international challenge. Demand for services has risen as many countries have implemented healthcare reforms resulting in shorter hospital stays, and patients with more complex health conditions are being cared for in a PHC setting. 1 Consequently, the need for advanced practice nursing is greater than ever. 1 The International Council of Nurses defines an advanced practice nurse, or a nurse practitioner (NP), as a registered nurse (RN) who has acquired the expert knowledge base, complex decision-making skills, and clinical competencies for expanded practice. 2 Employing NPs with advanced clinical skills seems to be essential to meet the increased demand for PHC in many countries in Europe, and NPs are a growing workforce.
There are a number of studies on advanced practice nursing in PHC, especially from countries where the expanded nursing role has a long history. Results summarized in reviews show that advanced practice nurses perform as well as or even better than physicians within their scope of practice, and with a higher degree of patient satisfaction. 4 , 5 It has been demonstrated that NPs can take on medical tasks and, in combination with the nursing approach to practice, they can provide person-centered, seamless and integrated service delivery. 6 It has been suggested that NPs are able to provide 67–93% of all primary care services. 3
There are some studies from northern Europe where the NP role is relatively novel. 7 , 8 To the best of our knowledge, there are no studies looking specifically at the NP role in PHC in Norway. The healthcare system in Norway is different from many others because it uses a gatekeeper system. Patients have to pass through a general practitioner (GP) or an out-of-hours primary clinic (OOH clinic) to get access to specialist care unless their condition is life threatening.
In Norway, the municipalities are by law in charge of organizing local emergency medical services for all inhabitants 24 hours a day. This is arranged by offering GP services during the daytime on weekdays and OOH clinics at all times. These clinics are staffed by RNs 24 hours a day, seven days a week. In addition, each municipality has a duty to maintain one specific telephone number (116117) at a local Emergency Medical Communication Centre (LEMCC), which usually is located in an OOH clinic. 9 , 10 The OOH clinics use different triage systems to ensure an appropriate response. The assessment system uses color coding to denote urgency: green for non-urgent situations, yellow for urgent situations, orange for more urgent situations and red for acute situations. 11
In OOH clinics, GPs charge fees for each consultation in addition to submitting reimbursement claims for each patient to the Norwegian Health Economics Administration (Helfo), which is the Directorate of Health’s external agency. 12 During the period from 11 pm to 8 am, a per-hour salary is fixed by regulation (OOH clinics that serve more than one municipality), and different refunds then fall to the municipality. A few OOH clinics have employed physicians during the daytime on weekdays. In Norway, 72% of all patients who visited OOH clinics from 2007 to 2018 were registered as non-urgent admissions, 24.5% as urgent and 3.5% as acute. The contact rate for OOH clinics in Norway in 2018 was 352.9 per 1000 inhabitants. 10 The age groups with the highest rate of contact are the oldest adults and the youngest children. The most frequently used single diagnoses in 2017 were abdominal pain, respiratory infections, skin cuts, lower urinary tract infections and general health problems. 13 One Norwegian study showed that more than a quarter of the observed GP consultations in OOH clinics were partly or totally spent addressing minor ailments. 14
The areas served by OOH clinics in Norway have gradually expanded into larger districts that include several municipalities, 15 and since the 2012 Coordination Reform in Norway, more patients are visiting these clinics and they have a higher urgency level than before. 16 The Norwegian Health Directorate states that a nurse with advanced clinical skills can contribute to the care of vulnerable patient groups. 17 Due to the increases in workload in clinics and in statutory tasks for GPs, waiting times appear to have increased. Therefore, leaders and GPs at one OOH clinic have expressed a need to meet these challenges by introducing a new role for registered nurses with master’s education in advanced practice nursing to provide a service that is both more effective and safer for patients.
In Norway, the master’s degree program in advanced practice nursing was established in 2011 with the goal of providing students with the advanced knowledge, competence, and skills needed for systematic assessment, care, and treatment of patients with minor health problems and follow-up of patients with chronic diseases. 18 The role is new and spread thinly throughout the Norwegian healthcare system and thus not much studied at this point in time. 1
The aim of this study was to explore challenges in the current model of care and whether NPs can perform new tasks in an out-of-hours clinic from both care providers’ and patients’ perspectives.
Methods and design
The study used a cross-sectional study design in which the data were collected via an email survey 19 and analyzed using descriptive and analytical statistics. 20 This study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 21
Setting
The OOH clinic where this study was conducted serves five municipalities with a total of 140,000 inhabitants. Seven RNs from this clinic have been studying part time on the new master’s program in advanced practice nursing at the University of South-Eastern Norway. This OOH clinic is one of the first clinics in Norway so far with a goal to implement new advanced roles for nurses.
Recruitment and sample
Both professionals and patients were invited to participate, allowing us to gain a broad perspective. The population consisted of all the RNs and GPs who took part in out-of-hours shifts in a medium-sized OOH clinic; in June 2018 they were invited to participate in a survey (n = 60 and n = 176, respectively). In addition, all patients who visited the OOH clinic during five weekdays in 2018 and were triaged as urgent priority were asked to participate (n = 17).
Instrument
The content of the questionnaire was developed for purpose of the study as no tested questionnaires were found. For the professionals, the questionnaire included background information regarding years of experience in the OOH clinic and questions about their perceptions of care delivery and waiting times and availability by phone and at reception. In addition, there were questions about possible new tasks that NPs could perform in the OOH clinic informed by international studies showing that NPs can perform tasks related to treating minor illnesses. The questions were ordinal as all the variables were categorized. The patients answered the same questions as the professionals, with the exception of questions regarding profession, work experience, and relevance of expertise in practice. The questionnaire was pilot tested by five RNs at the OOH clinic to check the wording of the questions, the response categories and the content. No changes were needed after the pilot test. Advantages of using a survey include that they are not resource intensive and can be given to large selections of the population, respondents can respond when appropriate and take the time they need, and it is possible for them to remain anonymous, as was the case in our study. The disadvantages are that surveys usually have a low response rate (often below 50%), which may limit generalizability. 22 , 23
Data collection
An electronic version of the questionnaire was set up using Nettskjema (University of Oslo). RNs and GPs were asked in an email to fill in the electronic version of the survey, and one reminder was sent after 14 days. 23 The patients filled out a paper version of the same questionnaire. When patients with urgent concerns (yellow response) came to the clinic they were informed about the study, verbally and in writing, and asked to participate. They were informed by a nurse who was not participating in the study. Once they were filled out, the questionnaires were locked in a cabinet.
Data analysis
We used descriptive and analytical statistics. Data are presented as frequencies and percentages. We used ordinal data with categorical variables. To identify statistically significant differences between groups, we used a chi-square test, and the level of statistical significance was set at p < 0.05. The statistical analyses were performed using SPSS version 26.
Ethical considerations
The Declaration of Helsinki guidelines have been followed. 24 The professionals received information about the study beforehand from the leader of the clinic and one researcher in joint meetings. The email with the questionnaire also included written information. GPs and RNs consented to participate in the study by completing the email questionnaire, which was done anonymously. The patients were informed about the study by the RN on duty and received an information letter and a letter of consent while waiting in the OOH clinic. To ensure that the patients did not feel forced to participate, they left the papers in an anonymous envelope. The study was approved by the Norwegian Centre for Research Data (NSD) with reference number 464505.
Each participant received a letter containing information about the study in addition to participating in a joint meeting where information was given verbally. If the participants filled out the electronic survey, it was understood as consent to participate in the study. The patients were informed by the RNs while visiting the clinic (urgent response).
Results
A total of 71 questionnaires were returned. Of these, 41 were from RNs, 13 from physicians and 17 from patients. The response rates of nurses and physicians were 68% and 7% respectively. From the RN group 34% (n = 14) had more than five years of experience in the OOH clinic, compared to 69% (n = 9) of the physicians. There were no significant differences between RNs regarding work experience and whether they felt they could use their expertise in their work or not. About three quarters of the RNs and the GPs answered that they could use their expertise at work to a large or very large extent, 78% (n = 32) and 76% (n = 10). Twenty percent (n = 8) of the RNs stated that it was unclear who was medically responsible for the tasks the RNs performed in the clinic, compared to 38% (n = 5) of the GPs.
Answers about availability by telephone during weekdays were significantly different between the three groups (p = 0.007) but also between GPs and RNs (p = 0.003). Opinions about telephone waiting times on weekends also differed significantly between the three groups: the nurses and patients reported either some or a large degree of waiting while the GPs reported either some degree of waiting or no waiting (p = 0.010). Most of the GPs had no opinion about the waiting time to see an RN at reception, and the RNs stated either no waiting or some degree of waiting on weekdays and more than half of the RNs reported large or very large degree of waiting. Three patients answered that the waiting time to see a nurse at reception on weekdays and at weekends was long. While the RNs and patients reported some or long waiting times to see a physician, the physicians answered there was some or no waiting time (Table 1).
Registered nurses’, physicians’ and patients’ opinions about challenges in the out-of-hours (OOH) clinic regarding waiting times, information given during the waiting time, and the organization of the OOH clinic (percentages).
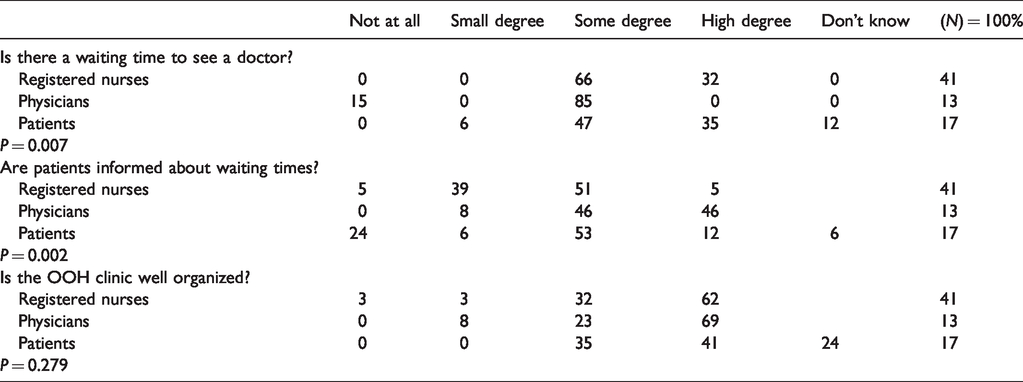
There were also statistically significant differences between the groups regarding whether waiting times to see a GP for yellow (urgent) and orange (more urgent) situations were acceptable. For yellow cases, all the GPs answered that the waiting time was acceptable while all the RNs answered that it was not. For green (non-urgent) cases, the three groups agreed that the waiting time was acceptable. This was also true for red cases (acute situations).
More than half of RNs and GPs felt the OOH clinic was well organized in terms of patient flow, 63% (n = 25) and 62% (n = 8) respectively, while 64% (n = 11) of the patients stated that the clinic was well organized (Table 2).
Registered nurses’, physicians’ and patients’ opinions about new tasks nurse practitioners (NPs) could perform independently at the out-of-hours (OOH) clinic (percentages).
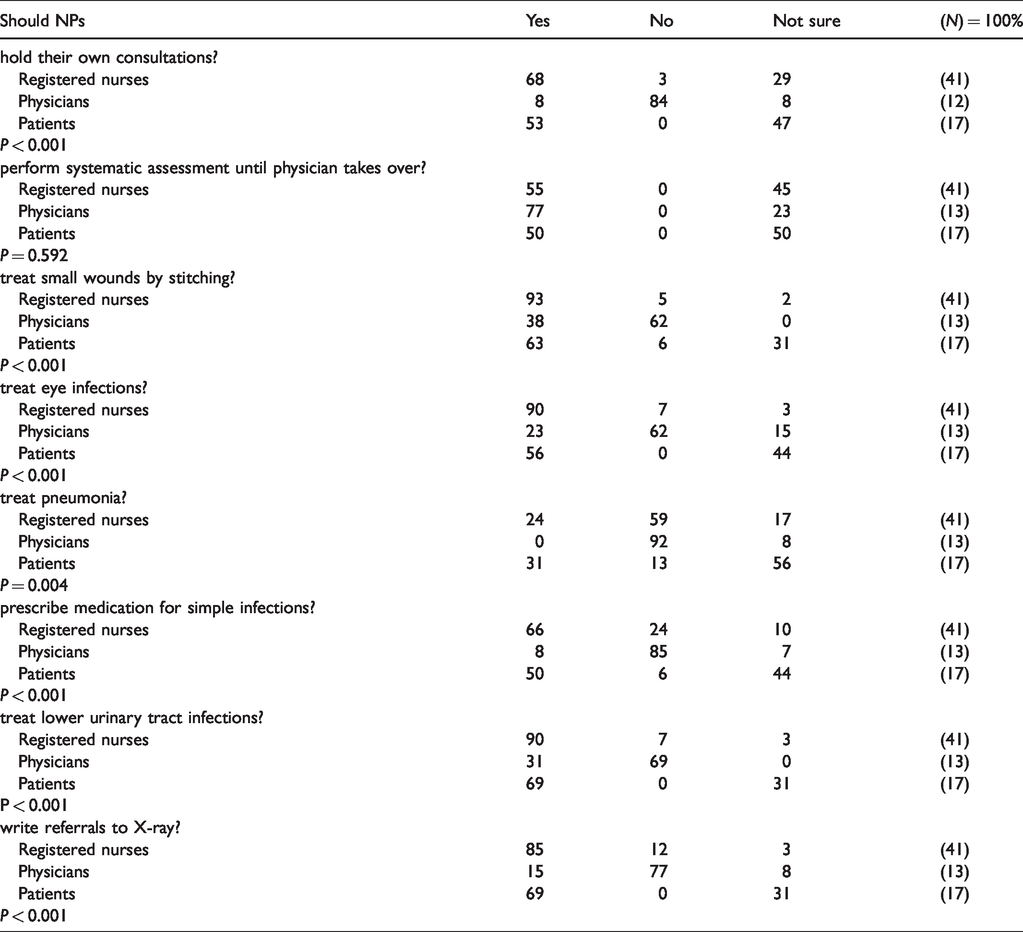
The RNs were more positive about NPs performing new tasks independently in the OOH clinic than the GPs (68% and 8%), while patients were either positive or unsure. A few GPs were positive about NPs referring to X-ray, stitching small wounds and treating lower urinary tract infections (Table 2). For other tasks, fewer than 25% of the GPs answered yes. NPs performing systematic assessment was one task that most of the GPs agreed upon and there were no statistically significant differences between the three groups.
There were significant differences between the nurses and the physicians regarding whether NPs should have their own payment structure for independent consultations: the nurses viewed this more positively than did the GPs (p ≤ 0.001). The RNs with the least experience had a significantly more positive view of NPs doing physicians’ tasks then the more experienced RNs. The patients were more likely than the GPs to think NPs should do new tasks, being either in favor or not sure.
Discussion
The aim of this study was to examine challenges in the current model of care and whether NPs can perform new tasks in an OOH clinic. Both nurses and GPs reported being able to use their professional skills at work. At the same time, more than one third of the GPs answered that it was not clear who was medically responsible for the tasks the RNs performed in the clinic. When implementing new roles, like that of the NP, it is of utmost importance to clarify what each health professional’s role entails. One study suggests three strategies to clarify roles: encourage all team members to sort out who has competence to do what tasks, preserve job motivation and facilitate positive relationships between team members. 25
Availability of RNs at reception was perceived as good by both patients and RNs, but the fact that patients found waiting times to be too long on the phone and to see a GP in person is in line with previous studies showing that unacceptable waiting times and poor general self-perceived health are factors affecting patient satisfaction across all contact types in OOH clinics. In addition, satisfaction depended on the type of contact and on geography, with patients living in urban areas being more dissatisfied than patients living in rural areas.26–28 Other challenges we found in our study were lack of information about waiting time until consultation with a physician; this was a problem from both the patients’ and the RNs’ point of view. One possible solution could be to make NPs responsible for face-to-face triage and performing an advanced assessment for each patient; this would allow them to give specific information about waiting times based on the patient’s condition. Thus, NPs could contribute to making patients feel safer and more secure; not feeling safe is often a reason for dissatisfaction with care. 16
There was significant disagreement as to whether NPs should take over the tasks and duties of GPs. RNs with less experience were generally more positive than more experienced RNs, and the GPs on the whole were more negative than the RNs. This is in accordance with previous studies which show that shifting tasks from physicians to NPs is challenging and often met with skepticism. 8 , 29 , 30 In addition, to successfully shift tasks, it is essential to have knowledge about NPs’ competence before implementing the new role. 8 ,30–32 Other findings from previous studies also showed that when GPs had experience working with an NP they had a more positive view of task shifting. 33 , 34 Based on the general skepticism about NPs handling new tasks, there were also significant differences of opinion between the nurses and the physicians as to whether NPs should submit their own reimbursement claims. In other countries that have implemented new advanced roles for nurses, NPs have the right to both their own reimbursement claims and prescription privileges. 1 Norway is at an early stage of implementing advanced practice nursing in OOH clinics and in pubic healthcare in general, and so far, there has been no change in the legal right of NPs to write prescriptions.
While the physicians, RNs and patients all agreed that there were certain patient conditions at the OOH clinics that could wait or be taken care of by other health professionals, the physicians did not agree about task shifting by letting NPs handle things like treating minor ailments for example. Considering the long waiting times for some patient groups and dissatisfaction among both nurses and patients, one might think that it could be beneficial to implement new roles for NPs performing tasks traditionally handled by GPs. Indeed, one study from Norway showed that consultations with in the OOH clinic were spent wholly or in part addressing minor ailments. 14 Previous studies have shown that implementing a new role for NPs results in better patient safety and more effective healthcare services.35–37 One study from Norway revealed a need for enhanced clinical competence among RNs in primary healthcare, as well as the importance of negotiating professional barriers before implementing the NP role. 34 The same study also showed that the role of NPs, and what competence they were expected to have, was not clear and that physicians did not know what to expect from NPs and therefore lacked trust in their competence. 34
In this study, the GPs agreed that NPs could start assessing patients until a GP became available, but not finish a consultation by themselves or hold their own independent consultations. This is in accordance with a study on implementing a new NP role in Norway which showed that nurses and GPs should not perform one another’s tasks. 34 At the same time, 68% of the GPs in our study had a positive view of NPs’ competence to refer to X-ray, and one third agreed that NPs could treat lower urinary tract infections and eye infections. More than one third of the GPs also agreed that NPs could stitch small wounds. This could mean that the exact role and competence of NPs are still not clear; moreover, the GPs’ lack of experience cooperating with NPs in the clinic may have affected their answers. The NP master’s students had not yet had the chance to work independently and gain trust among the physicians as they were at a clinic that was early in implementing advanced nurse practice.32–34
Methodological considerations
There are several limitations in this study that should be addressed. The total number of participants was relatively low, and the number of participants between the groups was uneven. The unequal distribution may have affected the results and differences between groups and should be read with some caution. The response rates for online surveys in general has an average of 33%. 38 Further, a validated questionnaire developed for the purpose of this study was not to be found. The questionnaire was pilot tested by five RNs. This was carried out to bring attention to ambiguous, complex, or vague questions and eventual inconsistency in definitions, scales, or wordings that could compromise the validity of a survey. 39 In general, developing a de novo survey is not recommended, but is necessary if no instrument exists. 39 To increase trustworthiness, it would have been useful to not only recruit RNs, but also physicians and patients to test the questionnaire. To increase reliability, repeated measures could have been used. Nonetheless, we could identify challenges in the current model of care and gathered indications about whether NPs can perform new tasks in an out-of-hours clinic seen from both care providers’ and patients’ perspectives.
Conclusion
Our study found some challenges with long waiting times on the telephone, which were considered less satisfactory than the waiting time to see a nurse at reception. Despite agreement among patients and nurses about long waiting times for non-urgent patients to see a GP, most of the GPs did not agree about delegating tasks to NPs. Patients were either very positive or not sure about having NPs do the work of the GPs. In addition, the information provided while the patient was waiting was not satisfactory. Our study showed that there is a need for clear descriptions of the tasks and responsibilities of both RNs and NPs in OOH clinics. While NPs’ advanced assessment skills were considered to help patients until GPs took over, only a few GPs were positive about handing over new tasks such as referral to X-ray, stitching small wounds and treating lower urinary tract infections.
Footnotes
Authorship contributions
Study design: EHH, EB, LF. Data collection: EHH, LF. Data analysis: EHH. Study supervision: EHH, LF. Manuscript writing: EHH, EB, LF. Critical revisions for important intellectual content: EHH, EB, LF.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The study was funded by the Oslofjord Foundation regional qualification support.