
Abstract
Diabetic peripheral neuropathy is a diabetes-related complication with vague and progressive symptoms with few available treatments. The aim of this study was to describe the experiences of diabetic peripheral neuropathy among adults living with type 1 diabetes. Twelve interviews were performed and qualitative content analysis was used. The overarching theme ‘living with challenges in the shadow of diabetes’ substantiated by the categories ‘pay attention to changes over time’, ‘frequent needs to facilitate living’ and ‘burdens to manage’ represents a daily awareness of the complication where autodidactic strategies were implemented. The conclusion indicates that it might be beneficial if nurses in diabetes care initiate an open-minded dialogue with adults with diabetic peripheral neuropathy to highlight their experiences and to discuss further strategies to facilitate living.
Background
The purpose of diabetes care is to prevent complications and to provide good and equal care for individuals living with diabetes. 1 Diabetes can be classified into type 1 diabetes (T1D) and late autoimmune diabetes in adults (LADA) and into four clusters of type 2 diabetes (T2D) according to Ahlqvist et al. 2 Type 1 diabetes is most common in Scandinavian populations and in Sardinia and Kuwait, but a global estimation to separate the prevalence of the different classifications does not exist. 3 In Sweden, approximately 50,000 adults are living with T1D, according to the Swedish National Diabetes Register. 4 It is estimated that 10–30% of adults with T1D have also been diagnosed with one of the most common diabetes-related complications, diabetic peripheral neuropathy (DPN). The complication is a result of nerve damage with a multifactorial aetiology; it is primarily related to prolonged hyperglycaemia, vascular complications and a long duration of diabetes.5,6 Genetic factors can also contribute to the complication. 7 DPN can cause loss of sensation from peripheral nerves in the hands, feet and toes; sometimes, it causes a feeling of tingling (from affected small fibres) and numbness (from large fibres), so-called ‘glove and stocking’ sensory loss. 8 For one third of adults with T1D, pain negatively affects daily life, and treatment such as general pain relief, antidepressants and anticonvulsant medications is sometimes ineffective. 5 Moreover, weakness of muscles in the feet can affect movement and can increase the risk of falls, 9 as well as the risk of foot ulcers. DPN can consequently affect individuals’ daily lives in different ways. In summary, the domains assessing quality of life show negative results when living with DPN.10,11
Nurses in diabetes care have the crucial task to support, educate and empower individuals by providing opportunities to improve the management of diabetes. 12 Daily foot care is an essential assessment in diabetes care. It involves inspecting the feet to detect deformities, foot ulcers, fungal infections and dryness as well as using proper footwear and shoe insoles. 13 However, this preventive action may not be feasible for individuals with disabilities, such as impaired mobility or blindness, where a chiropodist may offer regular supporting care.14,15 In Swedish diabetes care, an annual manual foot examination is recommended, which is performed by a diabetes team to diagnose or further evaluate the progress of DPN. The manual examination includes measurement of touch sensations, pressure, temperature, reflexes and vibrations, as well as visual, neurological and vascular measurements.1,16 Grenell and Turner 17 propose an open mind to different diagnoses, and Zang et al. 18 argue that clinical DPN is underdiagnosed and that further diagnostic methods are required. Underdiagnoses could augment the risk of accentual injuries and foot ulcers, and cause unnecessary trouble for individuals. Additionally, Boulton et al. 19 and Chin et al. 20 demonstrate that almost half of the individuals with diabetes experience no symptoms of DPN and the recognition of ulceration can consequently be delayed. One previous study describes a lack of knowledge about DPN among individuals with diabetes, especially about symptoms, which underlines the importance of foot care and its assessment and evaluation. 21 Hence, nurses in diabetes care have a prominent role in the diabetes team; nurses promote a holistic and an individual approach to the care, which is also advised by Gok and Arslan. 22 Moreover, nurses endeavour to create a partnership between patients and healthcare providers, and to strengthen the patients' own participation in their care and, finally, in their own empowerment.
To our knowledge, only two qualitative studies have illuminated the experience of living with DPN. One study performed by Brod et al. 23 includes elderly participants with DPN and T2D, and the results from the telephone and focus-group interviews indicate that half of the informants experienced daily pain. These experiences contribute to negative effects in life such as reduced physical activity and increased general difficulties. Thus, the aim of the present study was to describe the experiences of DPN among adults living with T1D.
Method
Study population and inclusion procedure
Characteristics of the informants.
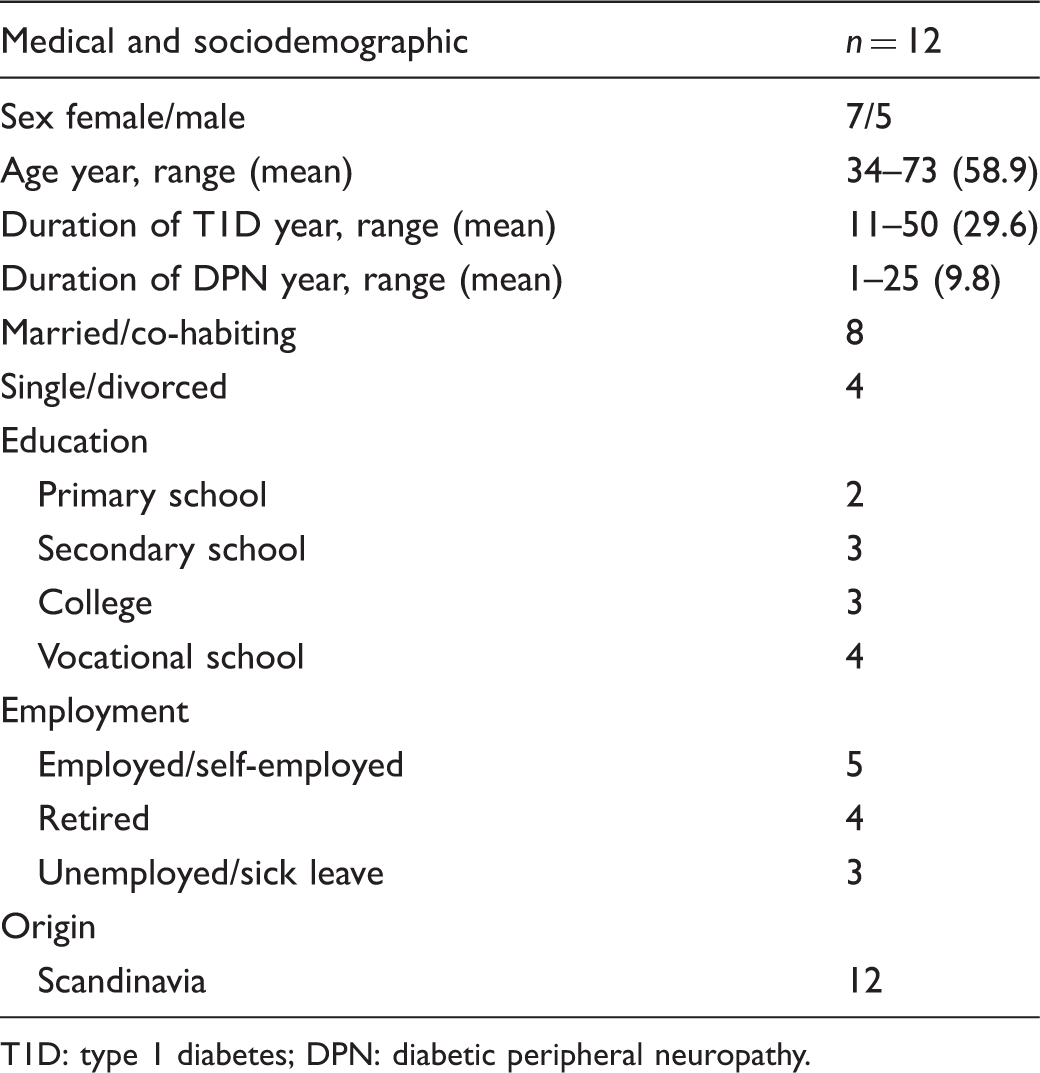
T1D: type 1 diabetes; DPN: diabetic peripheral neuropathy.
Ethical considerations
The study was approved by the Regional Ethical Committee, Lund (Dnr 2016/350) and was performed in accordance with the Declaration of Helsinki. 24 Before the interviews, the informants were informed verbally and in writing about the study design, voluntariness and confidentiality. They were also informed they could withdraw at any time without negative consequences for future care. A signed informed consent was obtained. All informants chose an undisturbed room at the clinic for the interview. To ensure confidentiality, all personal identifiers in the text were removed. The first author performed the interviews and neither of the authors had any previous or any ongoing contact with the informants. Moreover, neither of the authors worked in ordinary diabetes care. The primary author works within a research unit at the selected hospital and the second author works within the university.
Data collection
After collecting medical and sociodemographic characteristics from the informants, the first author performed an individually unstandardized interview by using the open question ‘Could you please tell me about your experiences of living with diabetic peripheral neuropathy?’ This all-embracing question was followed by probes, ‘Could you please tell me more about …?’ and checks ‘Do you mean that …?’ in an attempt to immerse and understand the answers. 25 One pilot interview was performed to assure the interviewer’s technique, but these data have not been included in the study. The interviews lasted between 25 and 75 minutes (the mean time was 40 minutes).
Data analysis
Qualitative content analysis, inspired by Berg, 25 was used to analyse the data, which provided a surface structure meaning (manifest analysis) and a deeper structural meaning (latent analysis). After transcribing the tape-recorded data verbatim, the initial first step of the analysis was an independent reading and rereading of the whole text to apprehend the ‘naïve preunderstanding’. This reading was incorporated before the detection and interpretation of meaning units began, and can be seen as a way to identify and handle each author's preunderstanding. The purpose was to create an open-minded understanding of the text that could be useful as a base for comparative analysis, and to avoid misinterpretations due to irrelevant conduct of the preunderstanding throughout the process of analysis. The first author has a preunderstanding as a trained nurse in diabetes care, and has service experience as a study nurse in diabetes, endocrinology and obesity research; the author has a long clinical experience as a nurse within various disciplines. The second author has experience working as a nurse in emergency hospital care and advanced home care, as well as several years of experiences as a teacher and researcher within a university. The purpose of the following discussions between the authors was to illuminate and to identify the preunderstanding to ensure that neither exaggerations nor understatements existed in the interpretational process.
Examples of the process of analysis.
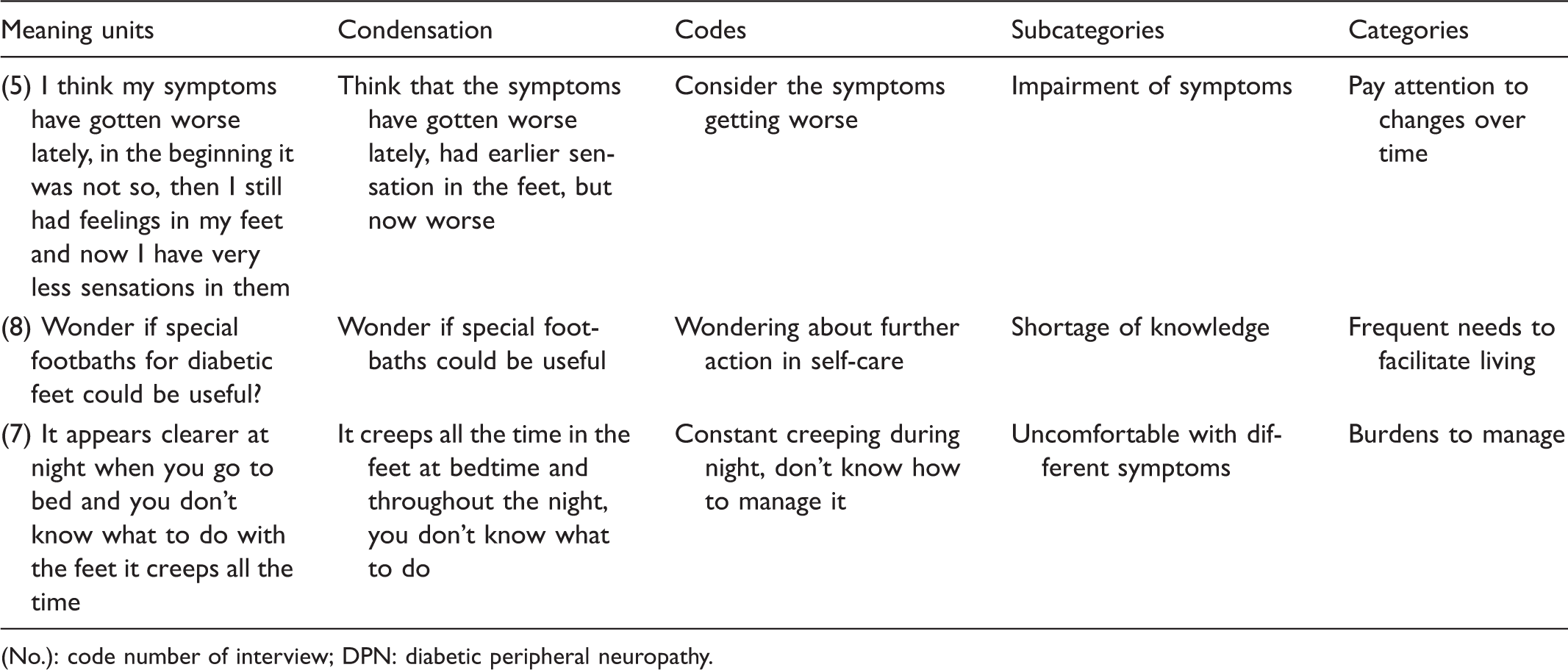
(No.): code number of interview; DPN: diabetic peripheral neuropathy.
Findings
The analysis generated one theme, three categories and 11 subcategories. The overarching theme, ‘living with challenges in the shadow of diabetes’, embraced the informants’ experiences throughout life. Living with DPN was demonstrated as being aware of the impairment of the symptoms from DPN and further, how to manage these challenges, as well as the underlying fear of more serious complications from diabetes. DPN was thereby a daily reminder of the need to continue self-care to prevent comprehensive difficulties, both of an emotional and a practical nature. The overarching theme illuminated the informants’ experiences living with DPN and the challenges they face, including improving their own ability, skills and knowledge concerning the condition. Moreover, three categories emerged: ‘pay attention to changes over time’, ‘frequent needs to facilitate living’ and ‘burdens to manage’. These categories represented the results of the analysis of 11 subcategories and all are shown in Figure 1. In the following section, the subcategories are presented in italics in the text under the associated category. The findings characterized an ongoing process of becoming aware of the changes accompanying DPN, which in turn needed intensive attention and creative interventions. DPN is a frequent reminder of the challenges of living with diabetes, an unpredictable and sometimes threatening disease.
Overview of theme, categories and subcategories.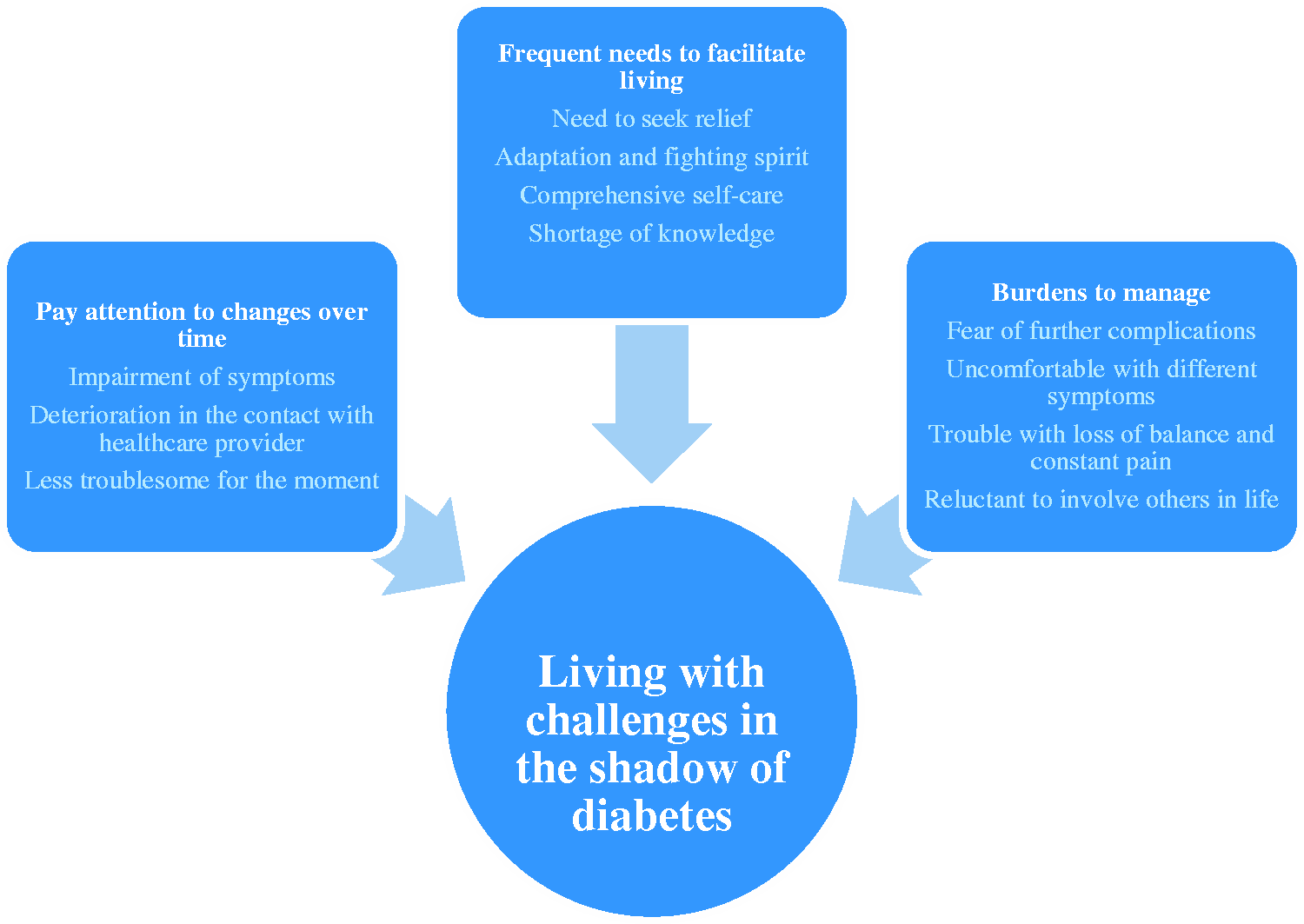
Pay attention to changes over time
In the first category, the informants described their feelings of being on guard in terms of the impairment associated with the vague symptoms of DPN. They became more aware of and paid more attention to the symptoms that could affect their daily lives. They worried about delayed encounters with healthcare providers, and they described their expectations of a dialogue about the current status and the deterioration of DPN. However, DPN could also be experienced as little less troublesome with few uncomfortable symptoms at the current time, although this could change and vary over time.
The experiences within the subcategory impairment of symptoms revealed thoughts and feelings about the worsening of symptoms and how to manage this discomfort. The informants were aware of and deeply concerned about these changes, and they talked about how the present symptoms needed to be addressed every day. Painful DPN was experienced as a major problem which could need further attention from the healthcare provider since this symptom caused suffering that greatly influenced daily life. … it's what it is all about that it hurts and it gets worse and what happens? … that is what it looks like now, it has only gotten worse … and I may have to quit my job? (5) … now the [healthcare provider encounters] are once a year but it will be every second year … if you don't call and say – ‘I must come!’ … so during two years, it has become worse [DPN] … but otherwise, we didn't even talk about it [DPN] during the last encounter. (10) … when they do the tests I react worse on the left leg but I don't think about it daily … my illness should not be a limitation for me and this is how I think about it now. (4)
Frequent needs to facilitate living
This category presented the informants' experiences about how to manage daily life when DPN symptoms were prominent. The informants emphasized the importance of seeking relief and having a fighting spirit, performing comprehensive self-care and acquiring further knowledge of DPN. The informants performed regular foot care and paid attention to their feet when the stealth symptoms of DPN could be observed.
Need to seek relief demonstrated their strategies of handling DPN. They included medication, physical activity, seeking a hotter environment, stress management and technical devices. The interventions were usually inevitable and necessary, and could improve everyday life. … it's the heat that makes me become more alert of course, and then it feels like … well, now I've got the feeling back again … if it's stressful around, it [DPN] can come all the time and then I have to use my technical device and then an hour or five minutes may pass and then I have to use it again. (2) … so it is, so I have to make the best of it … so that's why I don't hang on to that I can't wear those shoes anymore or … anything else. (8) … I go to foot care regularly and then you get control of your feet … and I'm a bit afraid to get sores and stuff at my feet … on beaches and so I've always shoes on and never go barefoot … except for indoors (smiles). (7) … but why I now have these pads [under my feet] – I don't know, and the doctor simply noted that I had impaired sensation … and I could understand when I didn't feel anything at the last check-up. (10)
Burdens to manage
The last category characterized experiences of fear about further complications that could likely be expected after a long life with diabetes. The informants described foot ulcers, amputation and kidney disease as the most frightening side effects of diabetes. Furthermore, the informants experienced dissimilarities in terms of DPN symptoms, when they were expressed and how they affected daily life. Finally, the stories exposed the burden of dependence and how to avoid involvement of family and friends in their own chronic disease.
Fear of further complications was expressed as a frightening experience when the informants realized that DPN was a fact and a consequence of diabetes. The symptoms from DPN could be interpreted as a sign of threat from diabetes itself – perhaps a predictable development of a chronic disease or an internal or external pressure to perform comprehensive self-care. … it's the fear of complications, and I've had diabetes for forty-four years and virtually no complications but I think about this [DPN] … but I've never have any problems with my kidneys. (3) … it's the tingling and mainly at night and tend to be under the sole of the foot and then with a bad feeling … otherwise, I also have a hand that usually goes numb. (6) … and then comes the plague … in the evenings, afternoon and weekends … well then it hurts and then I feel the numbness and if I feel any numbness at work, then you just have to turn it off. (3) … yes everyday life becomes … very influenced … but … you keep it for yourself … it is nothing I let affect others, and no one knows that I have these problems. (11)
Discussion
The main findings represent the informants’ daily experiences of living with the burdensome symptoms of DPN. They describe the numbness and tingling in their hands, feet and toes, and their unstable mobility. The descriptions involve variability of symptoms, and describe a broad range of obstacles associated with impaired sensations in the lower extremities, and a need to develop strategies regarding daily difficulties and a fear of future harm. Respondents practice stress management, increase physical activity, use emotional strategies comprising adaptation and acceptance, use technical devices and search for interventions and knowledge on the internet. In the study by Brod et al., 23 the informants with mainly T2D talked about their painful DPN experience, but they expressed few proposals or strategies. In our study, the informants adopt autodidactic strategies to enable living. We suggest that differences in strategies between the studies may be related to the informants’ recognition of the fluctuations arising from T1D and their need for a creative approach to cope with life's struggles. The informants described that diabetes self-management demands continuous awareness of impairment and decision-making, with or without the presence of DPN. Moreover, they reflected about the progression of DPN, and whether and how it would influence life if the symptoms occurred more rapidly. This expression may relate to their experience of the importance of urgent actions when compared to hypoglycaemia, and, furthermore, it may indicate their distress over how to manage impairment from DPN symptoms. Also, the slow progression of DPN could contribute to a feeling of being vulnerable and losing control of their lives. Delmar et al. 26 showed that self-control and self-responsibility are meaningful values for individuals living with a chronic illness. Individuals could request alternative options to manage the chronic illness, which, in turn, requires a nurse who welcomes and accurately meets an individual's unique needs.
The informants expressed a need for additional knowledge about DPN involving causes, treatment and the progression of DPN. This statement is in line with a study by Hansen Textor and Hedrick, 27 where the informants declared a lack of awareness and knowledge about the increased risk of symptoms related to peripheral neuropathy, a bothersome side effect of immunosuppressant treatment after organ transplants. Our informants with T1D had a shortage of knowledge about one of the most common complications, and this is consistent with results from a questionnaire study among adults with T2D. 20 It is a somewhat unexpected finding, and it may be related to the missing vague symptoms of DPN and even an ambiguity in diagnosing. On the other hand, adults living with T1D may be fully engaged in handling diabetes itself, and, therefore, the presence of DPN can be experienced as a minor burden in daily life, as compared to managing T1D. Perhaps an intervention, such as group sessions, could be valuable in illuminating important DPN knowledge to maintain and improve the present condition and also make it possible to exchange strategies in managing this complication. This suggestion supports Leksell's study, 14 which showed the benefits among individuals living with another diabetes complication, diabetic blindness, when attending group session interventions.
In our study, the informants had a fear of developing additional complications, which was also present in an interview study among adults living with T1D. 28 Symptoms from DPN appeared to elucidate the general risk of further side effects of T1D, but, in contrast, DPN was not considered as a serious complication despite its daily presence, or its potential risk for foot ulcers. Instead, the informants in our study expressed a greater fear of suffering from kidney failure or amputation relating to limitations, dependability and a higher degree of severity. Furthermore, Marks 29 named DPN as a forgotten complication due to lack of interventions, except for pain relief. Marks also mentioned the existing knowledge and clinical experience concerning the nature of DPN among healthcare providers, as an opportunity to improve the care of individuals living with this diabetes-related complication. Finally, despite many common denominators between individuals with T1D and T2D when experiencing symptoms of DPN, individuals with T1D can possibly differ by developing the need of autodidactic strategies to facilitate everyday life with the slow progression of DPN during a long duration of T1D.
Strengths and limitations
One limitation in our study is the cultural distribution of solely Scandinavian informants. A representation of individuals from other cultures might have extended the understanding of everyday life with DPN. Hjelm and Apelqvist 30 described dissimilarities in managing diabetes among individuals from other European countries and the Middle East. Their study incorporated health beliefs, knowledge of self-care and, in some cases, a need to adapt to the present religion. This limitation may affect transferability of our findings to other settings and situations. However, the available variety of informant characteristics may be applicable to other Scandinavian adults living with T1D. 31
Another limitation is that not all of the materials from the interviews are content rich, which may have affected dependability and perhaps the possibility to develop and conclude the names of the categories. Although we would like to point out that the data underpinning each level of category are in line with the chosen name of the respective categories. On the other hand, using focus-group interviews, where individuals with similar interests could have a meaningful exchange, might have increased the material,25,32 as was also considered by Gale et al. 33 Regarding confirmability, the findings are enhanced by quotations from the original material and a table illustrating the process of analysis. To strengthen credibility, the authors had continuing discussions throughout the process of analysis, where the process of analysis was described in detail. 31
Next, we are surprised by the low number of participants in the study: only 8% of the presumptive informants contributed. This may be attributed to the earlier description of experiences of DPN, where the individuals expose less knowledge about the nature of the complication, or a misdiagnosis. But the most important reason is likely a need to improve the dialogue about DPN within diabetes care. Therefore, we suggest that nurses in diabetes care pay attention to symptoms of this vague and progressive complication by using their knowledge and skills within a holistic perspective, where the entire life situation of the individual is of importance. Lewko et al. 34 further proposed paying attention to the dynamic life course and changes from a lifetime perspective. The individual's needs and experiences should be listened to in an order to obtain a holistic description of changes and influences from the entire life situation.
Conclusion
Living with symptoms of diabetic peripheral neuropathy may require a wide range of strategies to empower life. The theme, ‘living with challenges in the shadow of diabetes’, mirrors the informants’ experiences, where the management of diabetes is not negotiable. In an effort to reduce the knowledge gap about diabetic peripheral neuropathy and to augment attention of the symptoms and consequences of the condition, we suggest that nurses in diabetes care initiate an open-minded dialogue about how this forgotten complication can affect everyday life. The primary objective of the dialogue needs to highlight individuals’ own experiences with an opportunity to discuss strategies to improve life. Nurses in diabetes care have an important position in the diabetes team to meet the fluctuating needs among individuals living with this challenging complication. Finally, this open-minded dialogue should emphasize the importance of performing and maintaining self-care and prevention and it may, in turn, create a need to develop further strategies to facilitate living for these patients.
Footnotes
Author contributions
Both authors were responsible for the conception and design of the study and acquisition of data. YW conducted the interviews, analysed the data and drafted the manuscript. CB was responsible for analysing and reviewing drafts of the manuscript. Both authors read and approved the final manuscript.
Acknowledgements
We want to express our sincere gratitude to the informants who participated in this study and made this research possible.
Funding
The authors received financial support from Malmö University, and funding from Swedish Diabetes Association for the application to the Regional Ethical Committee.
Conflict of interest
The authors declare that there is no conflict of interest.