
Abstract
Parental empowerment plays an essential role in maternity and child healthcare. Professionals delivering these services are ideally placed to improve parents' empowerment and well-being. This study aims to describe the supporting factors of parental empowerment from the perspective of self-identified lesbian, gay, bisexual, trans, or queer (LGBTQ) parents in Finland. The study was conducted using a qualitative inductive design, and 22 parents participated. Interviews were conducted between July and September of 2016 and analysed using inductive content analysis. Four categories emerged: 1) Parents' willingness to create socially recognized families, 2) Parenthood support, 3) Respectful partnership with all parents, and 4) Accessible services. Services were more empowering when parents were treated with dignity. This focus requires gender-neutral communication and a clear sense of security for parents. The findings indicate more education on LGBTQ-related issues is still needed.
Introduction
Empowerment is a complex concept. Fundamentally it is about gaining power and ability in a way that increases capacity, self-efficacy, and decision making. Empowerment is associated with many different aspects of everyday parenting1–5 and childbirth.6–10 Used in this context the term has both psychological and social domains. 11 Parental empowerment manifests as attitudes, knowledge, feelings, and behavior 1 and is a collaborative process by which parents access the knowledge, skills, and resources that allow them to gain positive control over their lives. It is a general sense of power that has the ability to influence people, organizations, and environments. It also gives one control over one's life.1–3
Parental empowerment is considered crucial to positive family well-being.12,13 Further, it is considered an important concept for strengthening the position of parents in healthcare delivery. 14 Previous studies indicate that such empowerment plays an important role in how parents manage their everyday lives in the face of unique life changes and different demands. 4 Increased parental empowerment has a positive impact on children's services, environment, and growth.1,5
Strategies to support parents' empowerment have been studied previously. It has been shown that supporting parents' empowerment through family services is a collaborative process where both the professionals and clients are active participants.1,3 Equal relationships, advocacy, focusing on strengths, supporting active participation and decision making, providing information, and developing skills were all found to be relevant and connected.15,16 Trust and reciprocity are two characteristics of an environment that leads to support, cooperation, mutual benefit, and better outcomes for children, especially in lesbian, gay, bisexual, trans, or queer (LGBTQ) families. In contrast, lack of trust in the relationship is likely to have a direct effect on quality of care, especially reciprocity between the parent, child, and health professionals.17,18 Previous studies, however, have focused mainly on specific services, service situations, or groups.19–21 Further, most of these respondents have been mothers 22 and there are no studies that investigate LGBTQ parents' empowerment in particular. Existing research does investigate and define elements connected to supporting factors of parental empowerment. There are, for example, studies about heteronormative communication with lesbian families, 23 attitudes of health professionals towards LGBT persons in a range of healthcare settings24–26 and those held by nursing and medical students,27,28 and attitudes of health professionals working in community early parenting services in two states of Australia. 29 Further, there is also research on LGBTQ families' experiences and needs in those settings.17,18,26,30,31 Typically, those are dominated by studies on same-sex/lesbian motherhood, 31 and studies conducted on the broader group of LGBTQ parents in Nordic countries is still rare.26,30
According to these previous studies, LGBTQ parents still suffer discrimination and may not be fully supported within maternity or child healthcare because of heteronormativity and professionals' attitudes and practices. There is also an identified need for continuing education of health professionals in the practice arena. 32 A lack of LGBTQ education and training amongst health professionals may contribute to negative attitudes or apprehension towards caring for this population and ultimately may lead to persistent mistreatment33–35 and lack of empowerment of these patients in healthcare systems.
Therefore, this current study is focusing on the broader group of LGBTQ parents. Knowledge about different kinds of LGBTQ parents' experiences is necessary, and the results may add the information that can assist clinicians, educators, and hospital management to develop policies and practices that ensure LGBTQ parents and their families will receive equal, non-prejudiced, and holistic healthcare. Moreover, insight into the supporting factors of parental empowerment provides a good opportunity to understand whether implemented care interventions effectively contribute to supporting and strengthening parents.
In Finland, maternity and child healthcare settings are provided as part of the publicly funded national healthcare system there. They are free and reach most families as a part of the country's preventive healthcare system, the responsibility for which rests with the municipalities. Guidance and directions for service provision are laid down in legislation36,37 and national programmes. 38 These services support parents in providing secure, child-focused rearing and assessing the physical, mental and social conditions of children under school age. Expectant mothers normally meet with a nurse and a doctor 10-15 times during pregnancy. Childbirth and parenthood classes are usually also provided to first-time parents.
At the time of the current study, the number of families for the registered couples was 1500 and 1600 families of same-sex married couples in Finland . Of these families, 67% included female couples. 39 Proper estimates for the number of all LGBTQ parents are difficult to obtain since not all forms are registered. Female couples and single women have legal access to assisted reproduction. Self-insemination is not governed by the rule of law. Same-sex couples have had access to equal marriage and joint adoption since March 2017.
Aim of study
To describe the supporting factors for LGBTQ parents' empowerment in maternity and child healthcare from the perspective of self-identified LGBTQ parents in Finland.
Methods
A qualitative inductive design was employed for this research. This design was implemented through open interviews.
Data collection and participants
The data were collected between July and September of 2016. Inclusion criteria were: 1) parents' self-identifying as LGBTQ; 2) parents being at least 18 years in age; 3) being a biological or non-biological parent; and 4) experiencing Finnish maternity or child healthcare during the 2000s. An invitation to participate in the study was published via the internet through an organization whose members identify as LGBTQ families, a sexual political organization (SETA) website, and on Facebook. Participation was voluntary and confirmed by email. Parents opted into the study by responding to advertisements and then received specific information about the study by email.
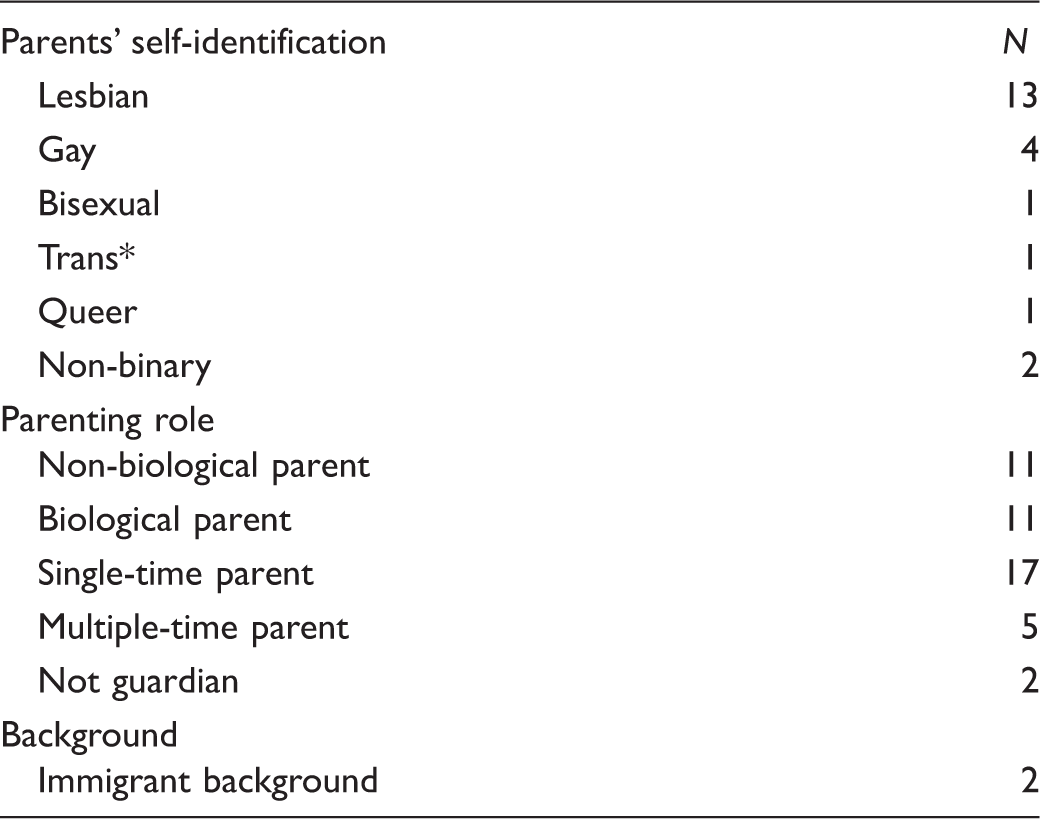
Characteristics of the participants.
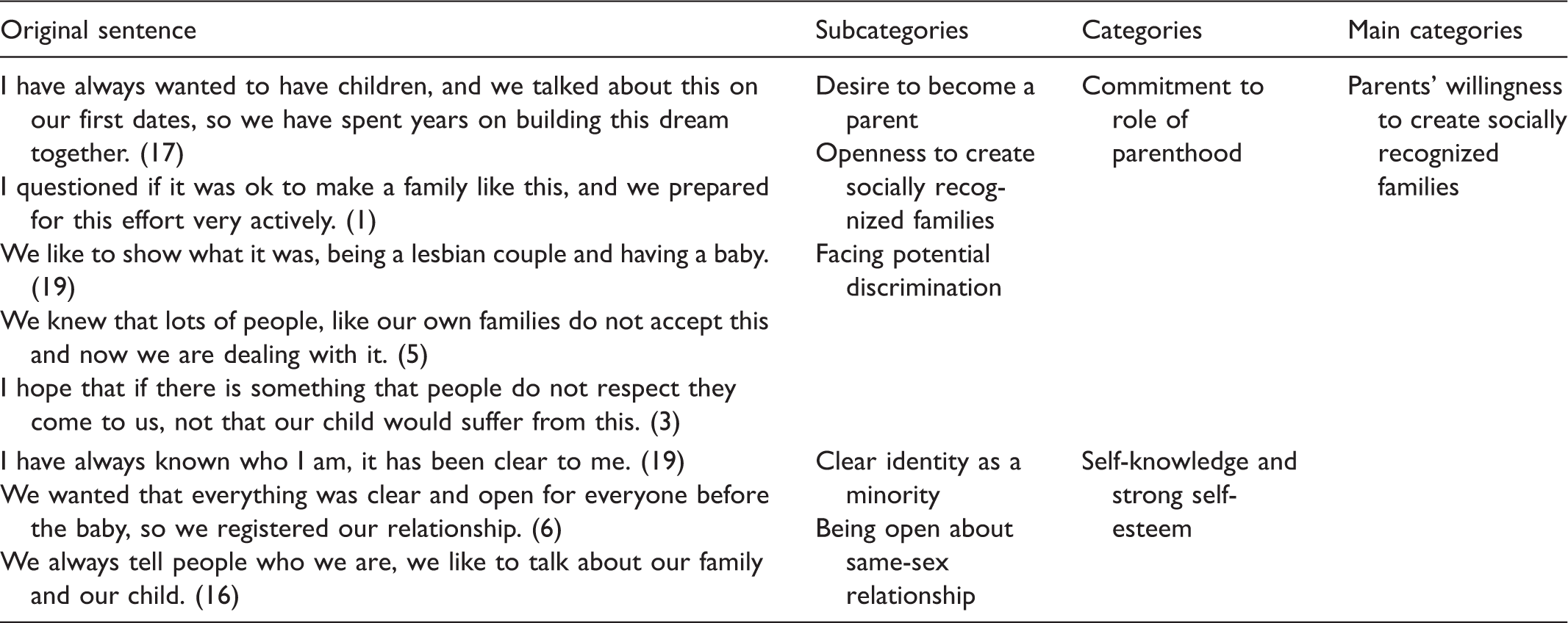
Examples from the data analysis.
All interviews were audio-recorded and lasted between 40 and 90 minutes, with the average interview taking 60 minutes. They were conducted at a time and place convenient to the participants, either during a meeting (n = 8) or over the phone (n = 14). Open interviews were requested to describe participants' own thoughts about supporting factors of parental empowerment in maternity and child healthcare. 40 The effort to gain a deeper understanding about empowerment was highlighted.
The interviews started with, ‘If I say parental empowerment, what are you thinking about?’ and ‘I would like to hear how would you describe supporting factors of parental empowerment in maternal and child healthcare. What would those factors be?’ The natural conversational flow was expanded by asking more specific questions and/or encouraging reflections on statements relevant to the study. Examples of situations such as positive and negative aspects of nursing care were explored, and clarifications and further elaborations were made. To ensure the validity of the data, the researcher tailored the interviewing style to the emotional state of each participant and carefully let them freely express their ideas.
Data analysis
All audiotapes were transcribed verbatim by the first author. The data were then analysed using inductive content analysis in line with Graneheim and Lundman 40 and Elo and Kyngäs. 41 All interviews were included in the analysis. The text was read thoroughly, and central issues related to the research objective were underlined. First, meaning units (e.g. a word, sentence, or a whole paragraph with the same meaning) were identified. Then qualitative data were organized by using open coding, creating categories and abstraction. Next, the texts were abstracted into codes through the process of writing notes and headings in the margins of the transcripts. The codes were then transferred into tables and grouped according to similarities and differences, while focusing on the aim of this study phase. Through the identification and interpretation of similarities and differences, further abstraction continued as far as reasonable and possible. Each category was named using content-characteristic words. The data analysis was conducted by the first author and then discussed in a research group to achieve a common understanding of the findings. An example of that process is provided in Table 2.
Ethical considerations
This study was conducted in compliance with the intentions of the World Medical Association Declaration of Helsinki and standard ethical guidelines and principles.42 Ethical approval was obtained from the UEF Committee on Research Ethics (13/2016). Voluntary, informed, and written consent was obtained from each participant. All participants were aware of the purpose of the study and the structure of their contributions, including audio-taping of their interviews. All tapes were stored in a locked cupboard that was available only to the researcher. Ethical issues included the protection from psychological harm of all participants and researchers and protecting all privacy and confidentiality. The use of critical reflection and rigor in generating the qualitative data was emphasized throughout the effort. 40
Findings
Four main categories emerged: 1) Parents' willingness to create socially recognized families, 2) Parenthood support, 3) Respectful partnership with all parents, 4) Accessible services (see Figure 1).
Supporting factors for lesbian, gay, bisexual, trans, or queer (LGBTQ) parents' empowerment in maternity and child healthcare.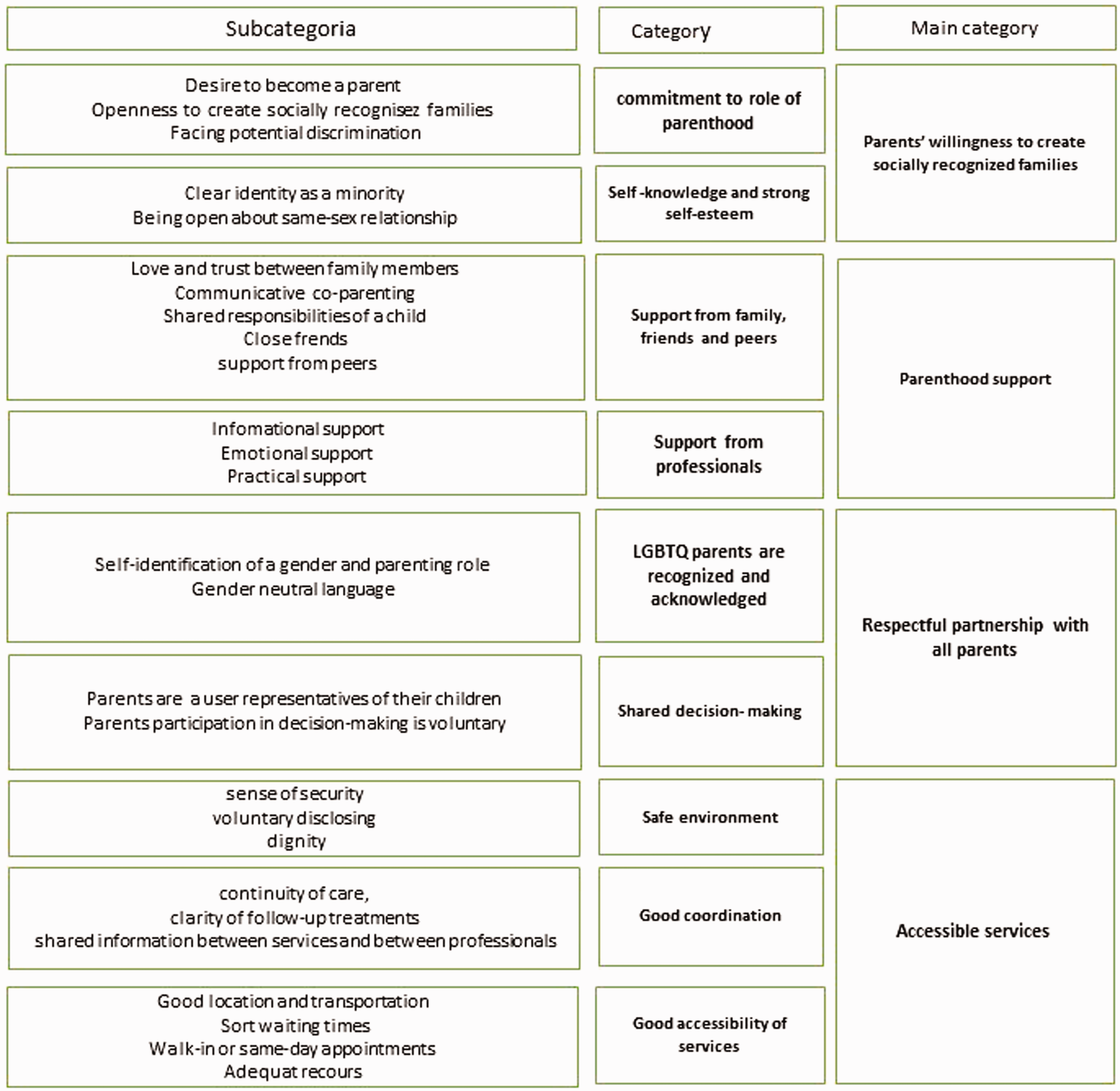
Parents' willingness to create socially recognized families
Commitment to role of parenthood
None of our participants took the decision to become parents lightly. The desire to have a family was usually there for several years, and participants faced different problems compared to “traditional” families. They had to cope with prejudice and discriminatory attitudes toward their sexual orientation, relationships, or family configuration, and they knew that they had to raise their children in the absence of specific laws that protect same-sex couples and families. Participants also expressed a sense of discomfort about potential impact on their children and their social and emotional health by asking: Do we have the right to be parents? (Interviewee 5) I have always wanted to have children, and we talked about this on our first dates, so we have spent years on building this dream together. (Interviewee 17)
Self-knowledge and strong self-esteem
Becoming a parent required good self-knowledge and strong self-esteem, so a clear and open identity noted as a minority was empowering. It's empowering, have a child in a family like this … I mean that I have always known who I am. (Interviewee 19) I need to be my own self and know who I am to get what we want out of the clinical encounter. (Interviewee 6)
Parenthood support
Support from family, friends and peers
Home with love and trust was important and needed especially when planning a family. Making a decision about a sperm donor or biological parenting meant there was the other parenting role that was more vulnerable and not supported by any law. There is always a chance that something goes wrong, and you just have to trust. Well, there is love, but making a family, it is something. (Interviewee 8)
Communicative co-parenting, such as mutual communication, teamwork, and respect for each other as a parent was essential, especially in those families where there were more than two parents and two homes. These arrangements, based on mutual agreement, involve people who are committed to raising a child together, possibly with their respective partners: There are four of us in this, and it's all negotiated. We put it all in a paper, it took time, but it was worth it. (Interviewee 20)
Shared responsibility for a child and shared financial support were important and empowering. Parents stated that their household duties were shared equally and decisions about work or family balance based more on circumstances than on preconceived gender-based ideals. For example, family leaves were taken equally. Shared financial support during the pregnancy was mentioned as extremely important because there was usually only one biological parent during pregnancy, before the adoption. It was mentioned as an important matter that both parents were participating in the costs of fertility treatments. Parents reported an increased understanding of their partner's everyday life after sharing responsibilities and spending time equally with their child. Empowerment was supported when parents trusted each other as parents and they could discuss together and with professionals their concerns about sharing the parenting workload and necessary financial support, parental leave arrangements, and benefits for LGBTQ families with their children.
Parents stated that friends and peers were important parts of their lives. Most of the LGBTQ-specific information was gained from peers and from the Internet, and participants were actively involved in an LGBTQ organization. Supported by peers meant having a sense of connection to a larger LGBTQ community. That view was associated with increased self-esteem and positive social identity development as a parent and as a family. Having support from families of origin was not that common and most parents did not take this for granted. Further, when they had it, they named their family of origin as a resource and a factor that supported their empowerment; it meant that their families were accepting them for themselves. Further, healthcare professionals were helpful when they supported parents in seeing their peers. It was also noted that professionals should be aware that LGBTQ parents are not always supported by their relatives, that friends as “chosen family” might be more important.
Support from professionals
Informational support included suggestions and directives. Further, it suggests that professionals have more knowledge about LGBTQ-specific needs. Parents needed knowledge and discussions about pregnancy as a medical condition, changes in sexual relationships, parenting stress, predictors of postnatal depressed mood and financial pressures as well as parents' return to work. Information was empowering when it was given individually and in an understandable language. Cases where professionals provided something special, were described as empowering. She asked if we were familiar with breastfeeding of non-biological mother, that she was thinking that we might want to do that; it felt so nice, she offered us something, that was just for us. (Interviewee 17) She told us where to go, so there was no need to navigate a complex labyrinth of therapy service referrals and appointments. (Interviewee 15)
Parents described parenthood as being rewarding, isolating and pressured. Feelings of being incomplete as a parent were common, and in the case of LGBTQ parenting, negative attitudes expressed by community, professionals, and others was typical. Many participants described the transition to parenthood as a time of confusion, as they attempted to define their roles within the context of meeting the needs of their partners and the new infants. Throughout the pregnancies and postpartum periods, the participants also experienced grief for the changes in their relationships. Emotional support was needed to develop feelings of attachment to the unborn infant. Professionals were expected to recognize and support their new roles as parents. Also contributing to the sense of parental identity was seen as important. I was wondering if I'm going to be as bonded to these children as the biological mother? (Interviewee 8) She was always willing to hear how we are, are we okay, and was there anything we need, like help or something, and I felt she was interested about our well-being. (Interviewee 22) We need to hear that our child is normal and that everything is normal in our family. (Interviewee 3)
Respectful partnership with all parents
LGBTQ parents are recognized and acknowledged
Being recognized and acknowledged included self-identification of a gender and parenting role that was important with respect to forms and medical records. The choices were ‘man’ or ‘woman’, so I crossed it out and wrote ‘non-binary’ instead. (Interviewee 4) I'm not in those legal documents … No one questions the role of the father in a heterosexual family, but I am not only questioned, but also misunderstood and ignored. (Interviewee 8) They asked us ‘How should we call you?’ or ‘What are your names for the kids?’ and I want to be referred to as mom. (Interviewee 12)
Shared decision making
Parents stated that they should be given the opportunity to be a user representative of their child but also appreciated that they were able to choose when and how they participated in decision making. Empowerment was supported when professionals acknowledged that all parents had an equal say in and responsibility for the healthcare of their child and when parents felt they were able to choose whether or not to participate in decision making.
Accessible services
Safe environment
This involved sense of security, voluntary disclosure and dignity. Being accepted and treated like everyone else, without discrimination or bullying was empowering. Despite these positive experiences, some participants said that they had expressed an internal fear of the reaction of the system to their sexuality or their family situation. Parents hold ‘expectations of prejudice and discrimination’ . Non-biological parents in particular had concerns about how they would be treated. Well, legally we had to be treated, but in reality how would we be treated? I was quite nervous about that. (Interviewee 8) But it turned out to be fine, they made me feel it was okay to be this kind of a family. (Interviewee 16)
Parents stated that they selectively chose to make themselves visible. Nearly all participants in this study wanted to be ‘out’ to their professionals. They usually voluntarily disclosed their sexual identities from the beginning. Parents thought that hiding the family situation was unnecessary. We are loving and caring people, and our child deserves to feel proud of this family. (Interviewee 21)
Supporting empowerment meant creating an environment in which the parents felt confident, relaxed, and comfortable enough to trust the nurse to disclose and discuss their sexual orientation and family configuration to others.
Dignity was part of having a sense of security. In particular, bodily integrity refers to the level of dignity that individuals feel during healthcare procedures that involve the crossing of personal boundaries, such as a gynaecological exam in maternity care. The ability of professionals to enable parents to feel safe during these exams was essential. Further, making a safe environment that supported empowerment required the use of positive space signage and other inclusive signage and professionals' respect for the individual in a vulnerable state.
Good coordination
Parents' empowerment was supported when good coordination, such us continuity of care, clarity of follow-up treatments, and shared information between services and between professionals occurred. Parents having appointments in different units of specialized care felt that it was empowering the professionals to be responsible for their or their child's treatment. Parents needed information about what had been carried out and planned regarding their own or their children's care. However, some parents were told that they had to take responsibility for transferring their follow-up treatment because it was not written down, or the nurse did not have the time to read it. Empowerment was supported when data were available to all those involved in treatment, and parents were informed enough about their responsibilities and appointments. Parents preferred that everything was written in the electronic records, and the professionals were able to access their information directly.
Shared information between the services and professionals included good electronic health information exchanges and effective flow of information between professionals. Parents stated that inter-organizational collaboration and regional cooperation with social workers was working. The flow of information between professionals meant cooperation and communication in the health centres. It was accomplished between nurses and doctors or therapists who worked with the family. According to participants, shared information between professionals helped parents who were disclosing their family configuration. It was mentioned that when professionals had read their files previously, parents did not have to see the reaction and face the possibility of professionals' negative assumptions. So, good electronic health information changes gave professionals time to adjust to the idea of LGBTQ parents and this empowered parents: It's important that the nurse or the doctor could see my family composition straight from the computer. Then they know who we are from the start and they don't have to ask or we don't have to explain … (Interviewee 3)
Good accessibility of services
Good location and transportation, sort waiting times, and walk-in or same-day appointments were all seen as supporting parents' empowerment. Further, Internet and social networking sites and the knowledge that help is available when needed was important, as one mentioned: That someone answers the phone when I need it. (Interviewee 11)
Adequate resources, including minimal exchange with professionals and enough time for the families, were preferred because greater consistency in nurses and care often made it easier for the children, the parents, and the professionals to become really familiar with each other. As a result, the parents did not have to explain the family composition, circumstances, and needs several times to several different nurses. It also seemed to be easier for the parents to ask for help or explain their needs when they knew the nurse.
Discussion
This study provides knowledge and understanding of supporting factors of LBGTQ parents' empowerment in maternity and child healthcare. To our knowledge, it is the first of its kind in Finland. This study addresses many practical ways in which maternal and child healthcare professionals can support parental empowerment and provide better care to LGBTQ parents. This knowledge can also be used in research and education.
Many aspects of supporting the empowerment of these parents are related to human rights, such as dignity, but also healthcare policy and structures, such us LGBTQ parents' recognition and acknowledgment, further parents' own commitment as a desire to be a parent and using services.
Participants in our study did not take the decision to become parents lightly. Interviews reveal that many parents had faced discriminatory attitudes toward their sexual orientation, relationship, or family constellation and encountered a number of stressors associated with their gender identity or sexuality. Further, these parents also reveal how they cope with feelings of otherness or ‘minority stress’ – the stress that accrues to members of socially disadvantaged or stigmatized minority groups and compounds general life stress. 43 Our participants reported feeling guilt, worries about being good enough parents, and concerns about how they would be treated in family services. Our parents told that they were committed to parenting, despite the fact that they would have to raise their children in this atmosphere and in the absence of specific laws that protect same-sex couples and their families. Resisting the negative effects of possible discrimination required good self-esteem and self-knowledge which were seen as empowering. Professionals and the healthcare environment, such as structures and policies, were seen as playing an important role in providing safe, high-quality, supportive, and accessible care that empowers all parents. Having access to at least one professional who values them was both important and empowering. These results emphasize the need to understand how stigma impacts LGBTQ individuals when they become parents. Such understanding will facilitate the development and tailoring of interventions aimed at reaching those most at risk. It also raises a question: how is minority stress related to parental empowerment? Can knowledge gained from research contribute to a better understanding of minority stress and otherness, as a point of departure for health promotion?
LGBTQ parents’ empowerment in maternity and child healthcare was supported when these parents felt that they were ‘part of the system’ . Similarly to several previous studies, parents were willing to participate if they perceived this as a normal and acceptable behaviour, within their control. That happened when they were able to define themselves and their families and be recognized as LGBTQ parents regardless of the parenting role or any biological or legal ties to a child. 44 It was important to be regarded and treated as a parent and seen as a family. Therefore, to design interventions to encourage LGBTQ parents’ participation, understanding parents’ roles, their lifestyle, and special needs is required. Actively giving permission to participate and involving all parents in decision making supported parents’ sense of control. Parents believed that they should be the main decision makers with regard to their own or their children's care. However, when discussing special care, most parents believed it was the professional's duty to make decisions on their behalf. Thus, empowerment was supported when parents were able to choose when and how they participated in decision making. This view may result from the parents generally feeling that they have limited knowledge of special issues in healthcare or what is required when emergency care is needed. If parents find that healthcare providers avoid partnership or leave their concerns unresolved, they lose confidence in professionals and avoid future contact and cooperation. Coming out repeatedly was described as stressful, as it placed parents in a state of emotional vulnerability. Poor past experiences with healthcare, concerns about breach of confidentiality, discrimination, or bullying made them employ certain strategies to shield themselves against such possible negative experiences. 26 This could be explained by the fact that previous experiences of discrimination in healthcare services will decrease willingness to be open about who you are, which in turn may affect the parents’ level of trust in those services or service providers and later, even ongoing parental empowerment in healthcare for their children. Similarly to Malmquist, Nelson, and Zetterqvist, 45 parents in our study reject negative experiences to protect their positive ones, and explain poor treatment as a lack of personal chemistry 23 or lack of education rather than discrimination. Therefore, professionals working with parents should be extra-attentive to LGBTQ parents to ensure they receive respectful and inclusive treatment.
Several studies have concluded that some LGBTQ parents, usually lesbian mothers, find the healthcare systems heteronormative and find professionals hold negative attitudes toward LGBTQ people due to a lack of knowledge of LGBTQ family issues.1,3,16,17 This study supports that finding and included gay, bisexual, trans and queer parents as well. Parents stated that supporting parental empowerment required inclusive and sensitive policies. The language used by professionals was a key indicator. This study also supported the fact that structural exclusions, such as medical records and forms that provided only heteronormative options for families, parents, and genders; heteronormative assumptions; and use of heterosexist language meant that this group is positioned as either invisible or secondary in this system.17,26 Further, a lack of human respect was seen to contribute sometimes to the absence of parent empowerment. The main concerns for the parents included the attitudes of health professionals when one parent was ignored or excluded from their child's care. Parents reported that it is important to take into consideration a parent's life situation as a whole and approve family units and to ensure that all parents feel comfortable by asking open-ended questions, using inclusive and sensitive language, and offering non-judgmental support. Creating a welcoming environment in which parents feel confident and comfortable disclosing their sexual identity and family composition includes acknowledging LGBTQ parents' relationships and different kinds of parenthood, displaying policies that explicitly protect LGBTQ parents from discrimination in waiting areas and in group meetings, and placing LGBTQ health information materials alongside materials intended for other patient groups, such as pregnant women. Most family services have policies and structures in place to prevent discrimination; however, it is necessary that administrators and clinicians ensure these guidelines are applied. In order to support empowerment, it was also judged necessary to have enough time to interact and to create and maintain long-term care relationships with professionals. As known from stigma research in general, factors that could mitigate stigmatizing attitudes are attribution beliefs and knowledge of and experience with a stigmatized condition. 46
Parents in our study reported that feelings of being incomplete as a parent were common. The transition to parenthood was a time of confusion as they attempted to define their roles within the context of meeting the needs of their partners and new infants. Throughout the pregnancies and postpartum periods, the participants experienced grief for the changes in their relationships. Professionals were expected to recognize and support their new roles as parents by giving them information and emotional support. Contributing to the sense of parental identity was also seen as important. Focusing on strengths and giving parents good feedback made them feel empowered. Lack of empowerment emerged when parents were given incorrect information regarding their health concerns and thus felt they had to teach staff about their special needs. Professionals also avoided asking parents about their sexual orientation or gender identity. This finding is important because it require health professionals not only to be willing to engage families from diverse backgrounds but also to ensure that they have the knowledge and skills to demonstrate sensitivity when caring for these families.
Study limitations
The concepts of credibility, dependability and transferability have been used in this study to describe aspects of trustworthiness. The participants lived in both urban and rural areas and identified themselves as mothers, fathers, parents, gay, lesbian, transgender, or bisexual whereas earlier studies focused primarily on lesbian mothers and not gay/bisexual fathers. 41 Further, the study participants' various experiences and parenting roles contributed to the rich data increasing the credibility of the study, as did also the quotations from the participants' original interviews.
Credibility of this study was established by selecting the most appropriate method for data collection. Participants were recruited via the Internet and data were collected using interviews. This choice allowed the use of existing networks to access participants who met the inclusion criteria and had experience with the topic. However, it was limited to those who had ongoing access to the Internet and/or are connected to LGBTQ-focused organizations. So those who chose not to participate may have done so on account of their views of empowerment, maternal or child health services, or LGBTQ issues which could have influenced study findings. Recruitment through a specific organization introduces a risk of skew in regard to education, financial stability and cultural background. However, this type of recruitment is useful when populations are marginalized because individuals might be more willing to participate if they have been referred by another member of their group. 40 The first author collected and analysed the data, after which the other authors evaluated these data to confirm the equivalence of the categories to the original data, which strengthened the dependability of the data.
In total, 22 informants participated in this study. Even though one interviewee's maternity care experience was from the early 2000s, her data were still included because the informants' experiences were similar and consistent across the entire study. Furthermore, the interviewer's pre-understanding of the topic may have affected the additional questions presented during the interviews, selection of the meaning units, and the analysis. To mitigate these limitations, reflection was ongoing, with authors meeting regularly to discuss emerging findings and to examine their own assumptions and bias that could possibly influence the interpretation of data.
Further, the concept of empowerment is multifaceted and diverse 47 and takes different forms in different contexts or settings. 48 Information on context and participants' characteristics was described to enable readers to evaluate whether the findings are transferable to other settings. 41 Because no previous studies on LGBTQ parents' empowerment or factors supporting it were available, these 22 participants are unlikely to be representative of all LGBTQ parents who are regularly involved in maternal and child healthcare. They are, however, able to illustrate many LGBTQ parents' experiences in this dual context. The findings offer a most welcome start toward a better understanding of how LGBTQ parents describe their empowerment in actual maternity and child healthcare settings in Finland now and in the future.
Conclusions
The results of this study indicate that supporting LGBTQ parents' empowerment in maternity and child healthcare requires policies and structures that recognize and acknowledge multiple family structures and parenting roles. To meet the needs of LGBTQ parents in maternal and child healthcare, professionals must develop awareness and understanding of the issues experienced by these parents and their families. Moreover, targeted education is needed to assist in sensitivity training related to the challenges faced by LGBTQ parents in their sexual and family relationships and parenting roles. LGBTQ parents require support and an environment in which they feel confident and comfortable disclosing their sexual identity and family composition. Most family services have policies and structures in place to prevent discrimination; however, it is necessary that administrators and clinicians ensure these guidelines are applied. In the future, greater ability to identify LGBTQ people in national, population-based datasets would help create national benchmarks for key aspects related to positive and effective LGBTQ parenting.
Footnotes
Ethical approval
Ethical approval was obtained from the UEF Committee on Research Ethics (13/2016).
Author contributions
Study design: JK, NH, MLP, AMP, data collection: JK, data analysis: JK, manuscript preparation: JK, NH, MLP, AMP and final approval: JK, NH, MLP, AMP.
Acknowledgments
Our grateful thanks go to these parents for sharing their thoughts and personal experiences.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.