
Abstract
Nurses in the Swedish child healthcare system can make a difference by offering support to parents of children who are overweight or at risk of becoming so. Still, research concerning these nurses’ clinical practice when encountering parents whose child is overweight is inadequate. The aim of this study was to describe nurses’ clinical practice when encountering parents of an overweight child. Data were collected through interviews with 10 nurses, and a content analysis approach was used. The nurses’ clinical practice is described in relation to Olander’s theory: Individualising actions, Creating a dialogue, Documenting, and Focusing on normality. This study adds knowledge about nurses’ clinical practice in encounters with parents whose child is overweight. Also, it adds information on how an issue in a specific care situation may contribute to further understanding and use of an existing theory in caring science.
Keywords
Introduction
Swedish child healthcare (CHC) is designed to promote children’s (0–5 years of age) health and to support parents. Child healthcare nurses therefore need to identify issues concerning children’s health such as, for example, overweight. 1 The WHO defines overweight and obesity as ‘abnormal or excessive fat accumulation that presents a risk to health’. 2 In the Swedish guidebook for CHC, children’s overweight is defined as weighing too much and obesity as a disease demanding lifelong treatment. 3 Globally, the number of children (<5 years of age) who are overweight is estimated at >41 million. 2 In Sweden, approximately 9.4% children of the age of four are overweight. 4 The percentage of overweight children has increased due to a more calorific diet and less physical activity. 5 The earlier a child suffers from overweight, the greater the risk that the child will remain overweight in later adolescence and adulthood 6 with risk of developing diabetes and cardiovascular disease 7 and dissatisfaction regarding themselves. 8 The focus of this study is not, however, children’s overweight as such but nurses’ clinical practice when encountering parents of children who are overweight. The experience of encountering parents as a CHC nurse has changed over time. 9 Child healthcare nurses need to pay attention to the family’s psychosocial situation, lifestyle and home environment. 1 Still, parents may not want the CHC nurse to intrude in their private lives. 10 Previous research has shown the difficulties nurses face encountering parents regarding issues of breast-feeding, sleep11 and tobacco habits. 10 Research concerning CHC nurses’ clinical practice when encountering parents of a child being overweight is inadequate. Children’s overweight may be an issue not considered by their parents and therefore difficult for CHC nurses to address. In this study, Olander’s theory 12 is used as framework.
Theoretical framework and previous research
Olander’s theory 12 regarding CHC nurses’ clinical practice shows how nurses synthesise their two assignments: the public health assignment including following the national population-based guidelines regarding children’s health and development; and the caring assignment including considering a family’s individual needs. 1 Despite how the nurses synthesise these assignments their actions are described as Individualising actions, Creating a dialogue, Documenting and Focusing on normality.
The importance of Individualising actions in encounters with parents whose children are overweight is clear, as previous research shows that parents’ levels of education, socioeconomic status and weight are significant factors affecting children’s weight. Parents with higher levels of education to a greater extent serve fruit and fish than parents with lower levels of education. 13 Living conditions, lifestyle and knowledge about health vary among families due to socioeconomic status. Children whose parents are obese and have lower socioeconomic status are at higher risk of being overweight.14–15
Actions of Creating a dialogue 12 are part of national guidelines describing nurses’ assignment to offer parents guidance to encourage physical activity and healthy eating. 16 However, the guidelines do not recognise how to encourage the parents. Nevertheless, research shows that informing parents about physical activity and healthy eating influences children’s health 17 as parents do not always seek information about how to offer a healthy lifestyle to their children. 18 Still, they show interest in receiving advice and support to help their children adopt a healthy lifestyle. 19 Research shows that parents receiving information on healthy eating serve vegetables more often than those who do not receive such information. 20
Documenting actions imply that the nurses follow regulatory requirements 17 as children’s weight and height should be measured and documented in the growth curve, as should the iso-BMI. 1 The iso-BMI helps to find out whether children are overweight based on their weight and length but is used sparingly; it is considered easy to misinterpret and difficult to use. 21
The nurses’ actions of Focusing on normality present difficulties when considering children who are overweight as there is a national weight gain and changing attitudes towards body size. 22 Perceiving children who are overweight as normal weight represent a risk since then there are no actions taken. Other difficulties regarding focusing on normality occur when parents do not see their child’s overweight, even though it is determined by objective measures. 23 These parents may be ashamed of their child’s overweight and the nurses’ health promotion is hampered because they do not want to offend the parents.22,24
Olander’s theory 12 is used to describe CHC nurses clinical practice when encountering parents whose child is overweight. There is a need to apply existing theories to specific contexts to determine their sustainability and to further develop them. Also, research concerning CHC nurses’ clinical practice when encountering parents whose child is overweight is inadequate. The collaboration between nurses and parents regarding children’s health in relation to overweight is important as it influences the child’s health. The varying living conditions among families calls for adjustment of national population-based guidelines to fit the individual family. Although nurses find child overweight difficult to deal with, this issue needs to be part of parental support to ensure the child’s right to health.
The aim of the study was to describe CHC nurses’ clinical practice when encountering parents whose child is overweight.
Method
A descriptive design with qualitative interview and deductive content analysis 25 was used.
Participants, setting and data collection
Ten CHC nurses at five different CHC centres participated in an individual semi-structured interview conducted in the nurses’ consulting rooms. The nurses were invited to the study via a telephone call. The nurses had at least one year of work experience to ensure that they had encountered parents whose child was overweight. The recorded interviews lasted between 28 to 39 minutes, and were transcribed verbatim.
Analysis
The theory of child healthcare nurses’ clinical practice as generic categories and subcategories. The concepts used in the categories and subcategories are conformed to mirror the data of this specific study.
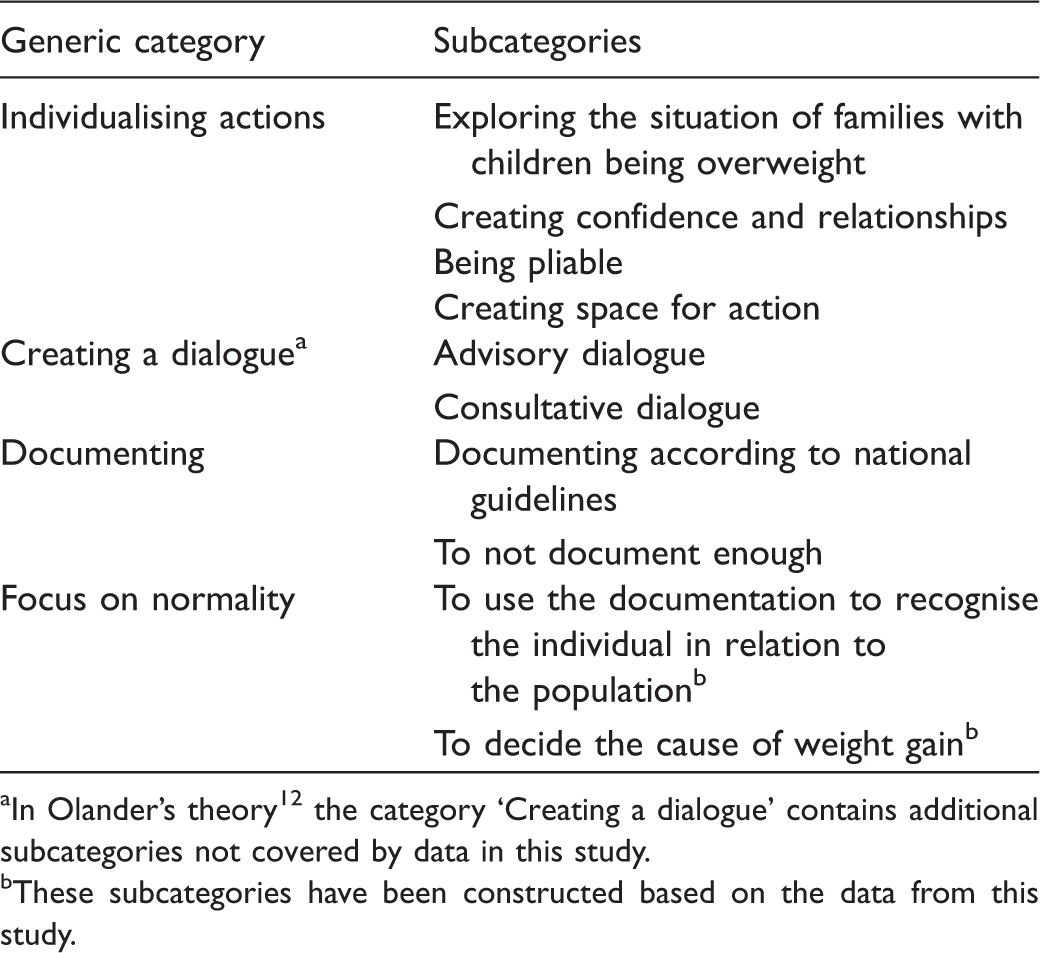
In Olander’s theory 12 the category ‘Creating a dialogue’ contains additional subcategories not covered by data in this study.
These subcategories have been constructed based on the data from this study.
The ethical principles of the World Medical Association 26 were applied in the study. Each CHC nurse was given written and verbal information about the aim of the study, the fact that the data would be treated confidentially 27 and that they had the right to withdraw from the study at any time. The nurses gave their written informed consent to take part in the study prior to the data collection.
Findings
The findings are based on the theoretical framework and the following concepts are used as categories: Individualising actions, Creating a dialogue, Documenting and Focusing on normality.
Individualising actions
In the encounters with parents the nurses try to adjust to the individual family by: Exploring the situation of families with children who are overweight; Creating confidence and relationships; Being pliable and Creating space for action.
Exploring the situation of families with children who are overweight involves paying attention to and being sensitive to the individual family. The nurses describe how they explore the individual family’s needs by listening to what parents say about eating habits and physical activities. They also describe being sensitive to what is not said, and that they observe the child’s physical actions. Furthermore, the nurses recognise the family’s socioeconomic situation, culture and knowledge. They report how families with low socioeconomic status may experience guilt and shame about their child being overweight. They also state that a family’s culture can influence the child’s weight. Being overweight might be an external sign of prosperity and therefore the parents do not understand the importance of changing food habits for their child. Families may lack knowledge about what healthy food is and why physical activity is important. The following quotation shows how the nurses’ exploration of a family has several aspects: It’s about parental responsibility, parental skills, resources. If it’s social, cognitive, or economic or whatever it is. All the pieces are needed and if there are shortcomings it is a concern.
Creating confidence and relationships is based on the nurses’ knowledge about the family. The nurses describe this action as a process beginning at the first encounter. They indicate that parents who have confidence in them can talk about their child being overweight: You try to create a good relationship, they [the parents] should always know that they can call me, or come and knock on my door if they can’t call or if they can’t speak Swedish. You need to be available.
Being pliable means the nurses try to meet parents’ expectations. The action includes paying attention to, and recognising parents’ concerns regarding their child being overweight to be able to encounter their expectations of support, especially as parents’ concerns are not always explicit. The nurses describe their need to be sensitive and use their intuition to support parents in helping their child to do more physical activity and eat less. They also report that parents who find it difficult to set limits for their child can be supported by the nurses setting such limits: You can get a hint from the parents that you should say something. That you must help them along. Then you can tell the child: you cannot eat four buns, one is enough.
The nurses are Creating space for action as they provide the individual family with time and allow the family’s needs to direct the content and pace of the encounter. They report their opportunity to use their time as they see fit. This control over time enables them to determine what to prioritise: The benefit of our work is that we plan all the appointments ourselves. I can take my time. If I know that a child demands a long discussion, then I can dedicate more time.
Creating a dialogue
The nurses report that they encounter parents whose child is overweight by creating a dialogue; a dialogue characterised by questions helping the nurse identify the needs of the family and informing the parents about CHC, the monitoring programme and results from examinations such as height and weight. This dialogue is tailored to fit the individual parent. The nurses’ dialogues can be created as an Advisory dialogue meaning the nurses provide advice from national and local guidelines and/or a Counselling dialogue meaning the parents’ views and concerns are addressed.
An Advisory dialogue contains the nurses’ descriptions of how they inform parents based on how they respond to posed questions. They express clear and straightforward advice about: food, physical activity, and the consequences of being overweight such as health effects on the body and the risk of being bullied. The advice given concerns: that parents need to be involved in their child’s eating habits and take control of them; the importance of good nutrition; portion size; number of servings, snacks, and that the children can start each meal with a glass of water and vegetables. The advisory dialogue implies providing information without giving parents space for questions. The nurses describe that parents who do not listen or do not want information are informed that it is their duty as nurses to inform them about overweight and its consequences. The following quotation describes how a nurse tailors her advice: The information is equal to all families. But it is presented differently depending on the language, the situation. You must tune in to what level of information is possible. Some get more details, others more basic information. It’s all about who it is. If you show them the growth curves so that they can see in black and white, with their own eyes, this is the way it is and then pose the question: have you considered this [the child’s weight gain]? That you use open-ended questions. What do you feel when you see this [the child’s weight gain]?
Documenting
The nurses’ documenting includes: Documenting per national guidelines and To not document enough.
Documenting per national guidelines includes nurses’ documenting the growth curve, complemented with notes. They describe that the documenting allows others to identify the child’s needs. The nurses report that the results of height and weight measurements are documented on the growth curve and as annotations. The annotations are described as being brief and as focusing on: diet, physical activity, advice given, the family’s thoughts about changes and the planned follow-up. The following quotation illustrates how a nurse documents according to the national guidelines: When I document I always record in the height and weight in the curve, then I write down what we talked about and what changes the family should try to make. We don’t use the iso-BMI at all on the CHC. I don’t know why; we haven’t had that discussion.
Focusing on normality
The nurses focusing on normality means that CHC nurses compare the child’s growth over time and with standards for the population to identify deviations from the norm as well as ill-health. This is described as: To use the documentation to recognise the individual in relation to the population and To decide the cause of weight gain.
To use the documentation to recognise the individual in relation to the population shows how the nurses pay attention to their two assignments. The nurses report their use of the growth curve to comprehend the individual child’s weight development in relation to the norm of the population. The growth curve makes it easy to recognise when a child has left the normal curve. The following quotation shows how the individual child’s weight curve is followed: All children are weighed and measured at every visit, and the results are documented in the growth curve. In the weight curve it is easy to observe the child’s weight development, and see if there have been any changes. According to the father there was nothing strange, there were normal meals and all. Then I began to wonder if there was some other problem, something to do with metabolism or hormones.
Discussion
The trustworthiness of this study relies on the theoretical framework being visible throughout the study. The variation of workplaces entails variation in the types of socioeconomic status of the families that the nurses encounter. These variations made it possible to receive nuances in the findings. Using a deductive qualitative approach means the researchers try to understand the data from a specific perspective without forcing the data to fit into a specific category and without trying to find data in the interviews to cover the whole of the theory. To reach findings with substance and sustainability the analysis process has involved cooperation between the researchers.
In Olander’s theory 12 the nurses’ various actions appear in various ways in their clinical practice due to how they synthesise their two assignments. Olander has developed four dimensions of clinical practice: Population-individualisation, Individualised support, Population survey and Routine check-up. The nurses are not necessarily in the same dimension during a health visit, they position themselves differently depending on the situations in an encounter. 12 The position a nurse decides on has consequences for the parents.
Population-individualisation is the ideal dimension as the nurses conduct their two assignments equally: the national guidelines are followed with individual variations. 12 Nurses’ encounters with parents whose children are at risk of, or are overweight are complex as the clinical practice needs to be based on guidelines to reduce the prevalence of overweight. 28 Still, the guidelines are general, unclear and incomplete. 16 Research in school healthcare shows that nurses equipped with action plans regarding children with obesity are confident about how to help families attain a healthier lifestyle. 29 The lack of specific evidence-based guidelines in CHC is made visible in this study. The nurses’ actions are based on their understanding of the individual family needs rather than population-evidence-based interventions formed to fit the individual family. This means that parents of children who are overweight have to meet various prerequisites to receive the support needed to help their child to reach normal weight, depending on the individual nurse’s understanding of the situation.
The dimension Individualised support focuses on the needs of the individual family instead of considering health and development from a population perspective. 12 In relation to the present study this dimension refers to the Individualising actions involving the nurses getting to know the family to decide on the intervention needed. Such an approach seems successful, as previous research shows that children of parents with low socioeconomic status are predisposed to being overweight.13–15,30 Research regarding lifestyle advice in general shows that persons with less education to a greater extent implement the changes suggested by healthcare professionals. 31 Additional research also suggests that nurses need to pay attention to the characteristics of a family to promote a healthy lifestyle for the children. 32 Furthermore, the actions of exploring offer a way to reach parents who are having difficulties in seeing their child’s overweight. 30 In the present study the nurses positioning themselves in this dimension adjust their actions to the individual family, aiming to create a consultative dialogue to promote the parents’ participation. When parents are involved, the nurses can explore their resources and support them in their decisions on lifestyle changes. Parents, after all, have the best knowledge about their child and their family situation 33 but need time to engage in dialogue about their child’s food habits and physical activity. 30 Previous research22,24 describes how nurses find it difficult to talk to parents about their child being overweight. Still, they have the mandate to support parents in their parenthood to promote children’s health 1 and previous research shows that parents are receptive to advice on healthy eating habits. 12 Therefore, nurses need to be aware of the impact of their actions regarding lifestyle advice and not ignore the issue of overweight. 31 Deliberate counselling dialogues with directed interventions can help children avoid suffering from consequences of overweight such as feelings of alienation 13 or chronic diseases such as diabetes. 12 Nurses’ descriptions of creating counselling dialogues from the perspective of the family are given in previous research concerning health dialogues on lifestyle changes, such as guiding, adjusting and inspiring. 34
In the dimension Population survey, the nurses’ approach is based on the national, population-based guidelines. The nurses use their individualising action to a minor extent. 12 They carry out the height and weight check-ups 16 and create an advisory dialogue without inviting parents to participate. The results show that the nurses found it complex to create a dialogue with parents not being open to changes. Still, these parents probably need the dialogue and the interventions the most. In the creation of an advisory dialogue the nurses clarify their obligations. They position themselves as actors in a service for the population rather than actors in a service for the family. The nurses’ advisory dialogue could also be described as directed, pressuring and instilling fear. 34 Furthermore, our study shows that the nurses always document the child’s weight and height, i.e. their population-based assignment. It is also found that their documenting of the cause of weight gain in terms of annotations is brief. This means that incomplete documentation gives the nurses fewer opportunities for individualisation. Previous research regarding children’s health records suggests that more information requested in the standardised part of the record may lead to more comprehensive and informative records. 35
In the dimension Routine check-up, the nurses conduct their assignment as such but their interventions towards the population and towards the family are unclear. 12 The commitment to the assignment is insufficient. Not using the guidelines given and not adjusting them to the family implies there is no individualising, which contributes to dialogue difficulties. Moreover, this dimension implies that children’s right to health is being neglected. 36 Guidelines regarding the promotion of children’s health are the minimum level of requirements to achieve equal quality care. 1 The nurses are assumed to keep themselves updated about the guidelines. Lack of knowledge about the guidelines is made visible in the finding on documenting using the iso-BMI. In the national guidelines 16 it is explicit that the iso-BMI should be documented for all children aged four years and for children from the age of two with identified risk of becoming overweight. The lack of using the iso-BMI found in the present study may be related to the guidelines being hard to understand. 21 To not use this tool indicates that the nurses have positioned themselves in the dimension of a routine check-up. Such an approach implies that children on the verge of becoming overweight are missed and action is taken only when overweight is already observed in the ordinary growth curve in the record. Also, the shifted perception of what is overweight further aggravates these children’s chances of receiving early interventions. 22
Conclusion
Based on the results of this study it is possible to conclude that Olander’s theory 12 of CHC nurses’ clinical practice is applicable in a context such as CHC nurses’ encounters with parents whose children are overweight. In this study, the theory has been modified and further developed. In the discussion, the result of the present study is related to the various dimensions of clinical practice 12 which clarify how the nurses’ encounters may vary due to their actions. The lack of evidence-based guidelines is made visible as the nurses’ actions are based on their understanding of the individual family needs rather than population- and evidence-based interventions adjusted to fit the individual family. Such national guidelines may help the nurses to pay further attention to these parents, contribute to reducing the number of overweight preschool children, and thereby contribute to decreasing the economic burden of overweight and its complications for society.
Footnotes
Acknowledgements
We are grateful to the CHC nurses for taking their time to participate in this study. The authors received no financial support for the research and/or authorship of this study. The authors have no industrial links and affiliations.
Author contributions
The listed authors certify their contribution. MH and SA designed the study and performed the data analysis. SA performed the data collection. MH drafted the manuscript. MG critically reviewed the data analysis and reviewed the manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.