
Abstract
In an intensive care unit (ICU), the environment is highly technological and staff are constantly present. The aim of this study was to describe environmental elements of an ICU room that nurses consider central for their provision of care. Data were collected using photovoice – photographs and in-depth interviews – and analysed using a qualitative content analysis approach. The care environment highly affected ICU nurses, in particular some elements such as medical equipment, work stations and beds. These were considered as an aid, but due to confined space some care was abstained from, maintaining privacy and confidentiality were a challenge, which led to frustration and stress. To provide care in an environment with good lightning, reduced noise and adequate space increases the wellbeing of the nurses, which indicates that an investment in a better care environment would be worthwhile.
Introduction
In an intensive care unit (ICU) gravely ill and injured patients are treated. Close monitoring, a highly technological environment and the constant presence of nurses are required when treating patients with life-threatening conditions in order to ensure bodily functions. The highly technological environment and the numerous staff constantly present can result in a strenuous and complex environment in which both to be cared for and to provide care.1,2 The physical environment in ICUs has been studied objectively,3–5 however, these studies do not provide insights into the subjective experiences of caregivers, nor do they help us to understand whether environmental elements have any impact upon the way care is performed. This study therefore focuses on the ICU nurses' experiences of the physical environment in an intensive care patient room and its impact on the quality of care provided. By physical environment we mean the place and space in the patient room where care is performed.
Design of ICUs
When building a new ICU there are guidelines to follow, which are similar around the world.6–8 The guidelines used in Sweden include free-standing patient beds with access from all sides, 20 m2 per bed in a multiple-patient room, and 25 m2 for a single room as medical equipment requires space. In addition, noise reduction, adequate and natural lighting to support circadian rhythms and ergonomic work stations are recommended as best practice.2,6 Research has shown that ICUs should comprise single patient rooms to reduce the risk of spreading multi-resistant bacteria, to reduce nosocomial infections, medical errors and minimize the risk of delirium.9–11 Delirium increases the risk of a prolonged hospital stay and increases healthcare costs. 12 Single rooms also provide privacy and confidentiality for patients. 9
Architects advocate evidence-based design (EBD) when designing new ICUs or renovating old units where the formation of the unit is based on high-quality research. 13 Forming a multidisciplinary team of architects, engineers and care staff when using EBD is of great importance. 8 Improved construction plan and ergonomic work stations reduce walking distances and work-related injuries, and improve hygiene. Using EBD can therefore reduce sick leave, shorten hospital stays and prevent complications, and is thus cost efficient in the long run. 9
Experiences of the ICU environment
Challenges and substandard environment within the ICU environment have been well investigated. However, most studies have focused on the patients and their families and found that the environmental factor is strongly correlated with increased satisfaction. Aspects such as atmosphere, silence, visiting possibilities and windows are linked with satisfaction.14–17 Research carried out with regard to care providers has typically focused on specific aspects of the care environment, such as light or sound. Sound and windows with natural light affect mood and concentration, and, by extension, the way care is provided.1,13,18 The impact of the care environment as a whole has scarcely been investigated from the care providers' point of view.19,20 The care environment and the ability to provide care is of importance for the recovery process of patients, the wellbeing of their families and work satisfaction of care providers, and should therefore be given priority.15,17,31 However, in spite of the fact that research shows the impact of care environment, it is still substandard. Care providers work in ICU environments every day and therefore bring a unique perspective to the design team when building new ICUs. Hence, the aim of this study was to describe environmental elements of an ICU room that nurses consider central for their provision of care. It is a second analysis of previous material
1
and supplementary data were collected to detect any new tendencies. The research questions guiding the study were:
In what ways do physical environments matter to the nurses? How does the physical environment affect their ability to care?
Method
The study has a qualitative explorative design. Photovoice was employed, a method that combines photographs and in-depth interviews. The purpose of photovoice is to use photographs together with participants' voices and histories in order to elicit data. 21 All data were analysed using deductive content analysis. 22 Categories were formed with the help of the participants' photographs.
Participants and settings
A written invitation and information about the study was published on the homepage of each ICU. Furthermore, a gatekeeper identified potential participants to achieve a purposeful sampling with variation in gender, age and experience, 23 who were then invited to take part in the study by the authors. Out of 17 people asked 16 participated, 11 registered nurses (RNs) and five enrolled nurses. Their ICU experience ranged from 2–32 years. One nurse was male and 15 were female.
The setting for this study was three ICUs, two situated in university hospitals and one in a regional hospital. All the ICUs were renovated or built in the 1990s, with 8–15 m2 per bed space and were staffed by RNs with a post-graduation education in intensive care, enrolled nurses and doctors. One RN and one enrolled nurse had the responsibility for two patients and one of them was always present in the room. Each ICU in the university hospitals had an isolation room, two-bed rooms and a few multi-bed rooms. Each room had windows behind the beds with a view of another building and by the head of the beds monitoring equipment was placed. Curtains or a foldable separated the beds. The rooms at the ICU in the regional hospital accommodated two to three patients. The unit is situated on the ground floor with a garden area outside which one to two bed spaces in each room had a view of and three of the rooms had direct access to the garden area.
Data collection
Fourteen sets of photographs and interviews were initially collected in 2014 for a doctoral thesis, 24 and two years later additional data were collected to identify any new trends. No new information emerged, i.e. saturation after two sets of new data. These additional data were collected at the same ICUs as previously.
After agreeing to participate in the study, a meeting was scheduled for taking digital photos followed by an interview. The interviews where held at the participants' workplaces, and they were asked to photograph physical elements in the ICU environment that affected their provision of care. They decided where and which elements to photograph. The interviews were initiated with the open question ‘Can you tell me how you experience the ICU room?’ and then photographs were used to stimulate the interviews and to maintain focus on the purpose. The interviews, conducted by three persons with experience of working as ICU nurses, lasted 30–90 minutes, were recorded digitally and transcribed verbatim. According to Swedish law 25 ethical approval is only required for research involving intervention or the use of sensitive data. Still, the ethical principles of the Declaration of Helsinki 26 have been considered throughout the process. The participants were given verbal and written information about the purpose of the study, voluntariness and confidentiality prior to the data collection. All the participants and clinic directors involved gave their written consent. Using photovoice can pose a risk of exposing both people and places. 27 The participants were therefore informed that no photographs should be taken of patients, families or other individuals without their consent. The interviewer was present at every photo opportunity to minimize the risk of unethical photographs.
Data analysis
Extract of the analysis process.
Results
This photovoice study sought to understand nurses' experiences of the environmental elements in the ICU patient room. In response to the question ‘Can you tell me how you experience the ICU room?’ the nurses emphasized security, darkness and confined space. By security they referred to having close access to medical devices and monitoring equipment. At the same time, all the different alarms were experienced as time-consuming and a distraction. Everyone mentioned the darkness, many expressed it in terms of walking into a bunker or a cave, and the participants believed that both patients and staff needed daylight. The darkness and the many disturbing alarms made the participants tired by the end of the shift. Rooms were perceived as small and they became even narrower if the patient needed all the medical equipment or if relatives were visiting. A crowded room caused the nurses to sometimes abstain from providing care. In sum, the analysis revealed that nursing staff were highly affected by the care environment.
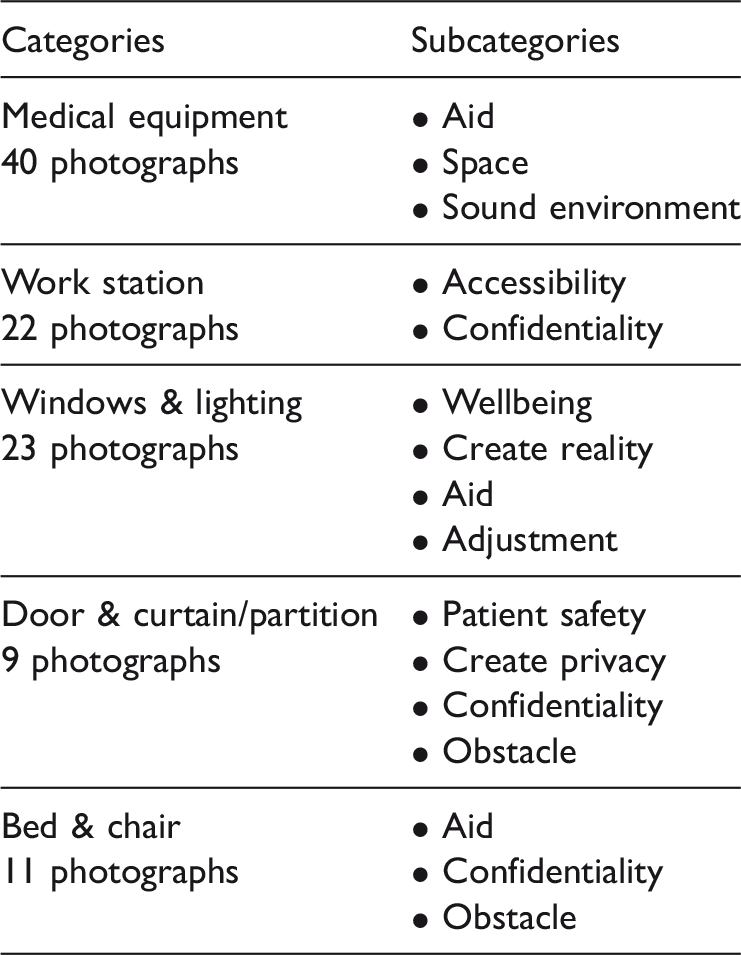
Summary of categories and subcategories.
Medical equipment
The photographs of medical equipment include ventilators, monitoring equipment, drug pumps, wires and hoses (see Figure 1). These items were seen as natural elements in the ICU environment by the nurses, described as helpful, but noisy and taking up space. The equipment alerts nurses if, for example, a parameter goes beyond the guideline values, if the patient has difficulty breathing or if a drug runs out. The warning mechanisms gave a sense of control and security and were described as a lifeline. Many participants described the room as undersized considering the space medical equipment required nowadays. The rooms were also perceived as cramped and dark, and some described a feeling of confinement that affected mood, as well as irritation and frustration that came as a result of not being able to reach the patient. The participants stated that they sometimes abstained from providing care due to lack of space, and mobilization was particularly mentioned in this context despite the fact that this factor was recognized as important. To be able to provide care, the nurses needed to move the heavy equipment, which was experienced as straining. As the space was seen as limited, the devices were in the way and the nurses needed to stretch and stand in uncomfortable positions to provide care. All the energy spent to get close to the patient left the participants stressed and frustrated. The cramped space was also seen as a security risk since it was easy to get entangled in various wires and hoses. It's horrible! I can't access in a simple way, I have to or need to scrape myself, get hurt, slip between or pull in my stomach. (P1)
Medical equipment photographed by P3. To put it bluntly, it can also be a cry-wolf syndrome; you don't react as much or I don't react as much when it beeps so it's also a risk. (P9)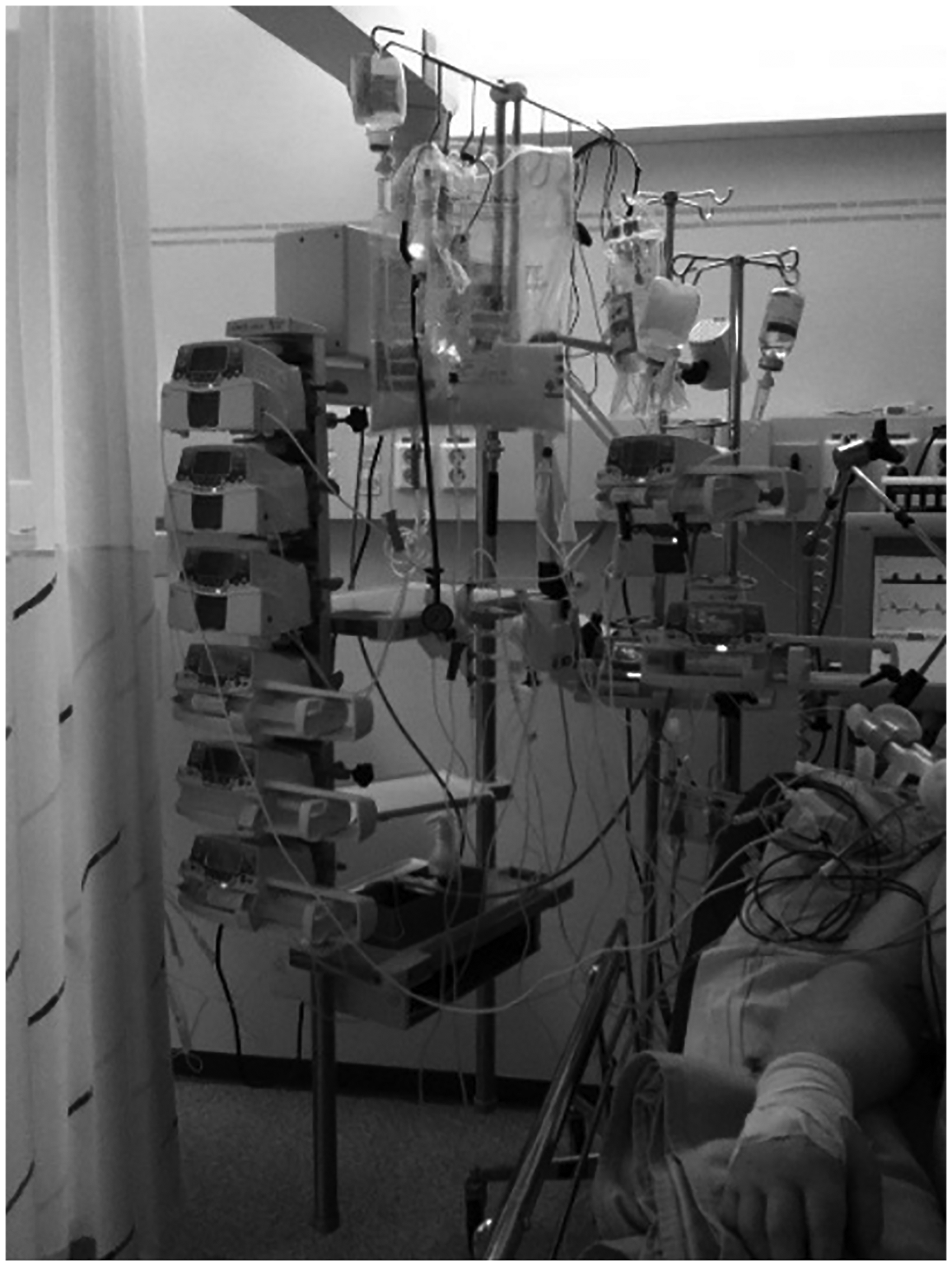
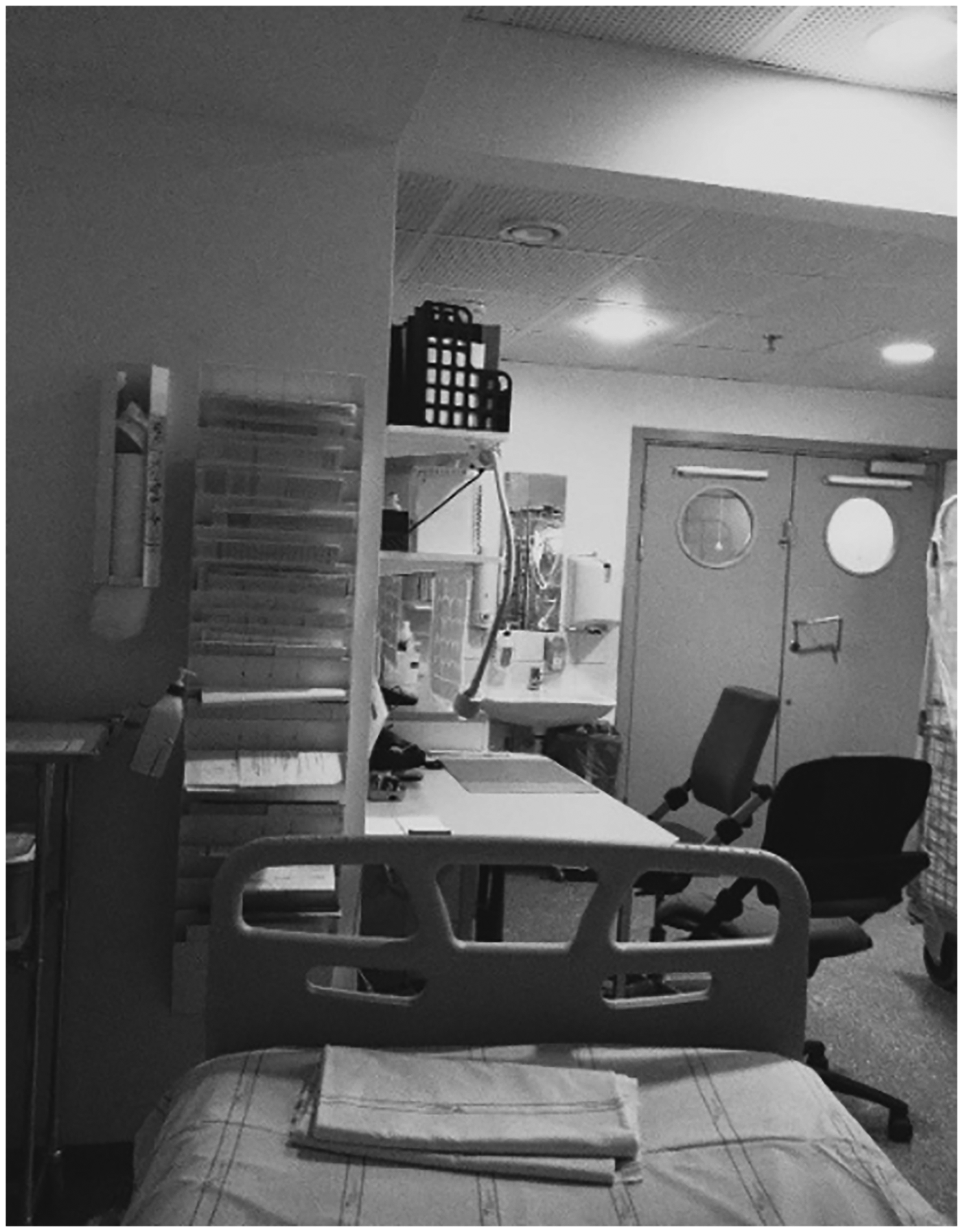
Work station
The work station provides access to working materials, pharmaceuticals, a computer and a preparation bench (for example see Figures 2 and 3). It is a part of the patient room and the nurses observed how it was often cramped. Further, many care providers required and used the computer during the day which made it crowded. Preparing drugs demands focus and there was a risk that patient safety was compromised when this task was carried out in this environment. To reduce stimuli many suggested that the work station should be secluded, preferably behind soundproof glass walls. In a glass cubicle nurses could sit facing the patient and thus have control of the situation, but at the same time be able to work uninterrupted. A glass cubicle could also help maintain confidentiality, which, according to the nurses, was difficult since rounds and reporting were currently held in the patient room. And then maybe doctors and consultants come in and there will be a lot of talk in the room. There is nothing that can, there is nothing that spares, that protects the patient from the talk. (P16)
Work station photographed by P16. Work station photographed by P12.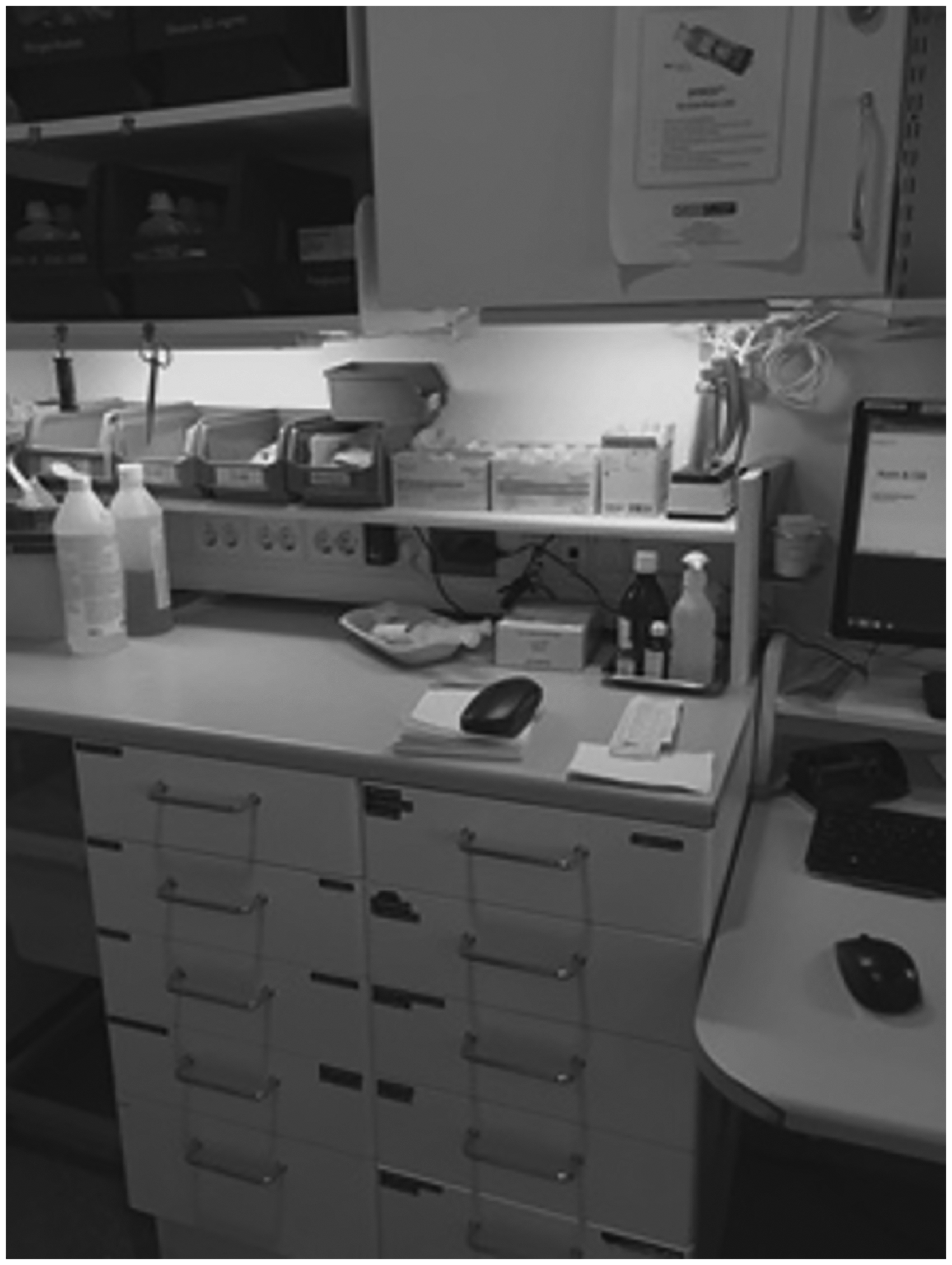
Windows and lighting
The photographs of windows not only represent the window itself but the daylight and the world outside (Figure 4). To see daylight and nature made the participants feel happy and positive, which enabled them to go the extra mile for the patient. Working in rooms with small windows was described as being in constant darkness, and as a consequence nurses became sad and tired during their shift, which affected caregiving in a negative way. Therefore, the lighting in the room was of importance. The participants reflected on lighting as an aid and they needed good lighting to see properly. Some of the light from the lamps shone straight into the patients' eyes, and the nurses therefore tried to adjust it to make them more comfortable, even though it made it harder for them to work securely. Above all, they tried to reduce the lighting at night to support a circadian rhythm. If I, for example, go to another ward I feel a relief that it is so bright and open /../ and then when you come back you feel like you go into a bunker, a cave actually. (P12)
Windows photographed by P1.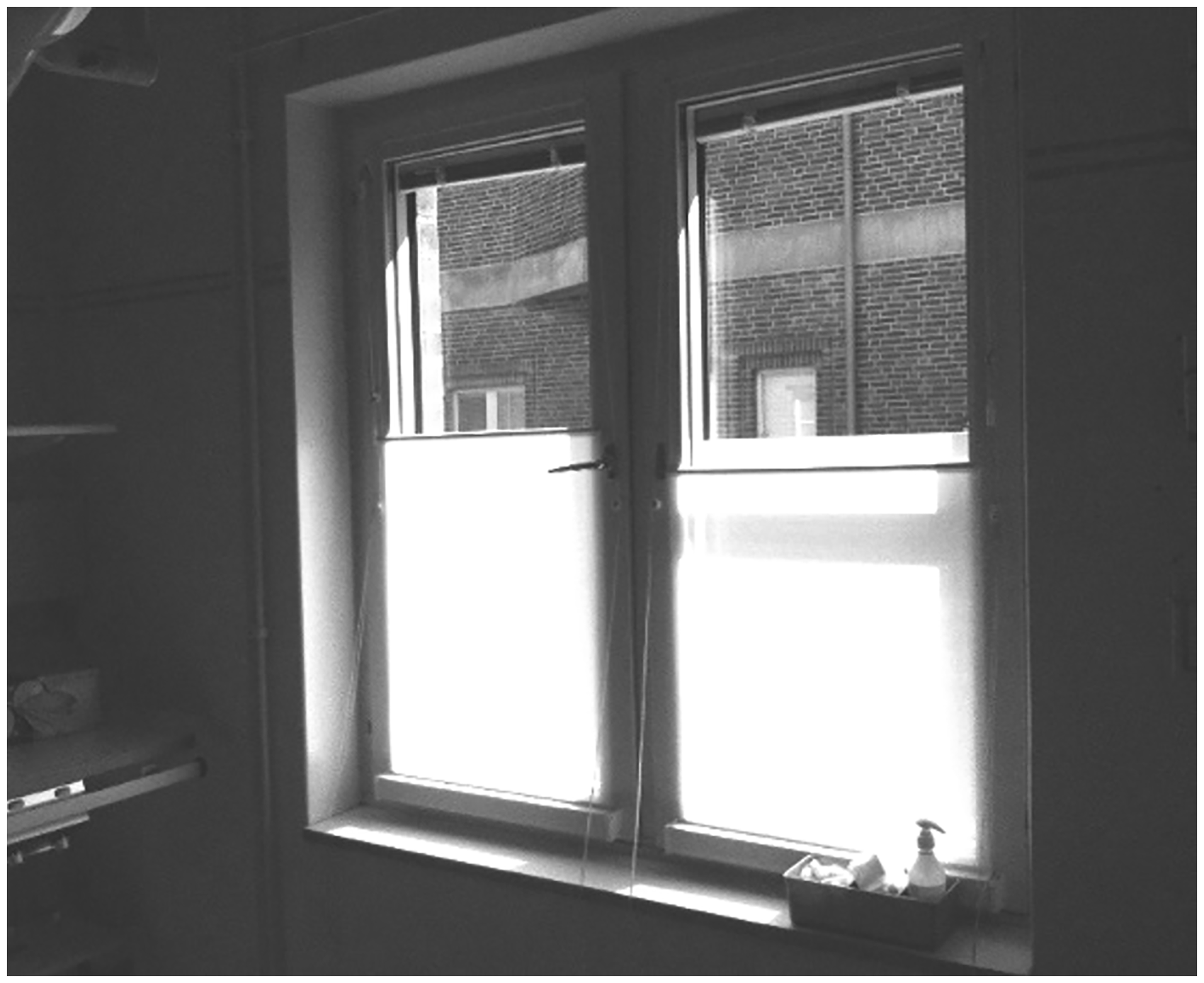
Some of the participants had been involved in a reconstruction process of the ward and described how their suggestions about including large windows with natural light were not taken into consideration. Instead the appearance of the façade was prioritized and small windows were chosen.
Door and curtain/partition
The nurses made an effort to protect privacy, as it was seen to be important that the patient did not feel exposed or stared at. Shutting the door and pulling the curtain was therefore a way of showing respect. It was also a way of shutting sound out, and a signal to colleagues not to disturb, while also protecting patient safety (see Figure 5).
Closed door photographed by P1.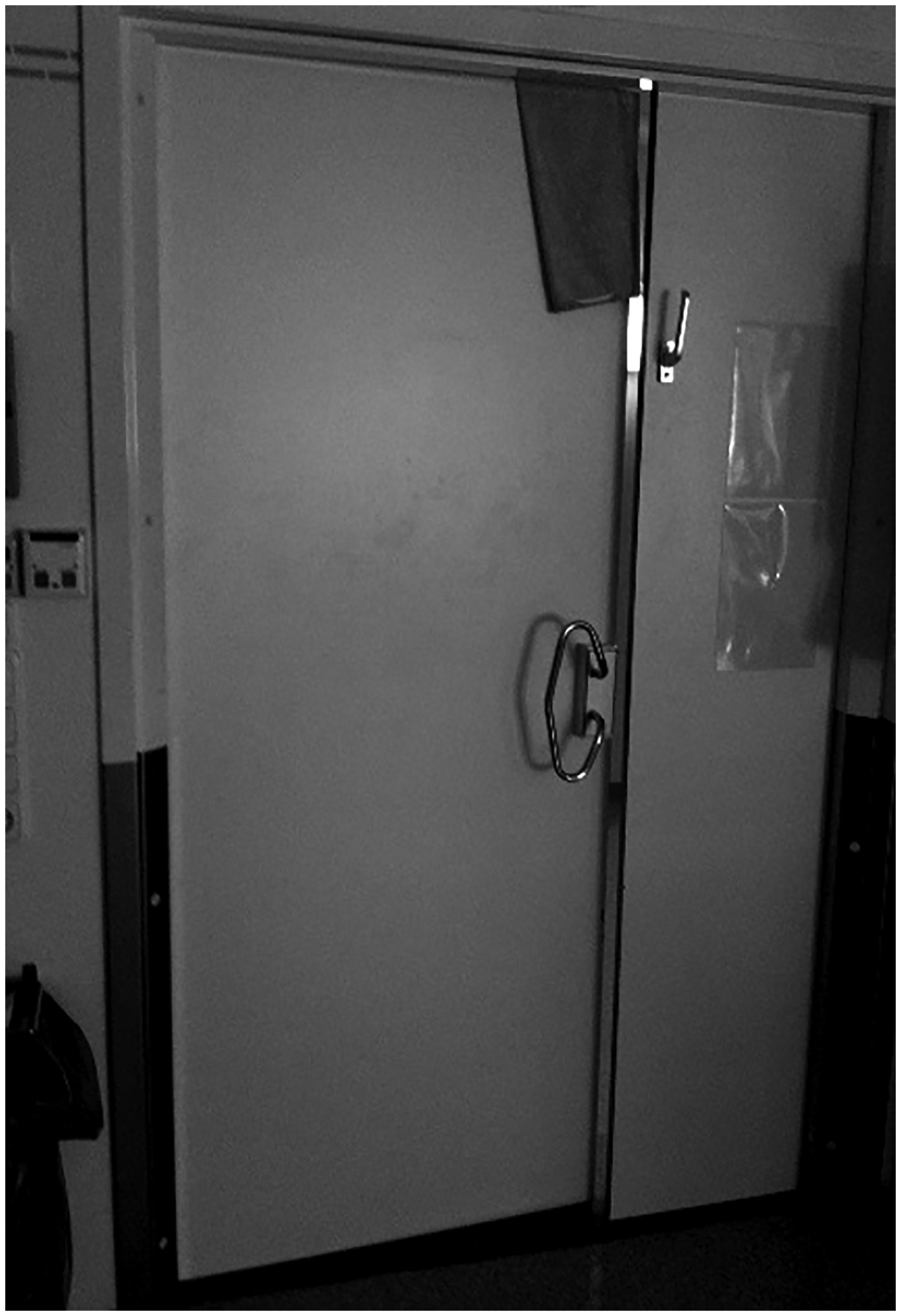
The participants were aware of their responsibility to protect privacy since their patients are unable to express their own will and therefore used curtains and partitions (Figure 6), even if this irritated nurses since it led to them loosing overview of the patients and made the room feel even more cramped. In two-bed rooms sound and smell were difficult to escape, but the curtains and partitions could still protect from transparency and provided a private sphere. Single rooms were seen as optimal for achieving privacy and confidentiality. Maintaining confidentiality was difficult in two-bed rooms since all information to or about the patient was given in the room. They get worried when you talk to the other patient because they don't always know if it concerns themselves or the other patient because they can't know that!! (P12)
Curtain photographed by P1.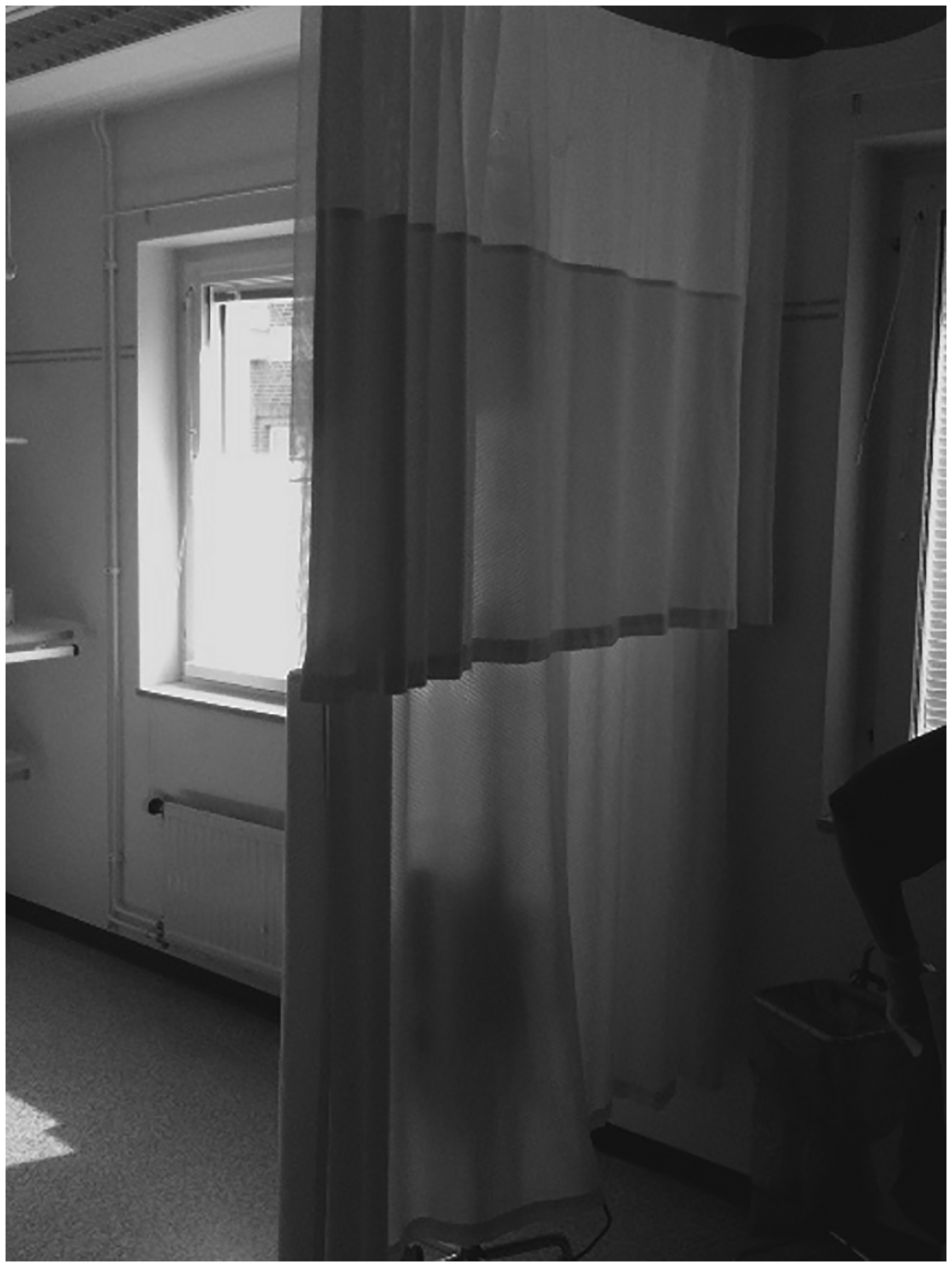
Bed and chair
The bed was described as the patient's place in the room and is therefore a central element and an important aid for nurses' work. The participants mostly had positive comments about the bed, they could weigh, x-ray and mobilize the patients in the bed and believed that a technical bed with an anti-decubitus mattress was comfortable and good for the patients' recovery.
The photographs taken of chairs symbolize next of kin (Figure 7). Participation of next of kin was believed to be important both for caregivers and the patients. Nurses tried to make space in the room, adjusted their work whenever possible, put up chairs and encouraged next of kin to participate in providing care. There was an old couple … the lady said; we have not been apart a single night in all the years we've been married. So she got to be with him and held his hand when he died that last night too, that there is room for that kind of stuff makes me feel good when I go home. (P9)
Next of kin using a chair, photographed by P3. She had heard several conversations about when they would end treatment of the other patient in the room, so when it was time for her family member she said: I guess we start by setting the ventilator on air ‘cause they said so to all the other patients … then you realize that it's quite bad or beneath contempt. (P13)
Discussion
Given the results of the study, lack of space affected the nurses since the rooms were not large enough to accommodate to the demands of today's intensive care, and more and more devices were added without the rooms becoming more spacious. The medical equipment was a central element in the ICU room, and as previous studies also have shown, it was seen as an aid. 30 However, our results also showed that the equipment limits the space even more, and it was perceived as a nuisance when the nurses had to move the equipment to be able to care. They tried to adapt to the cramped space, which led to non-ergonomic working positions and compromised patient safety as hoses and cords became entangled and restricted movement. Space-consuming care, for example showers or mobilization, was not carried out to the extent that the nurses believed was needed. This is serious as early mobilization is increasingly recognized as important in today's intensive care due to having several advantages, such as reduced time in ventilator, less delirium and shortened hospital stays. 31 Non-ergonomic planning also affects care providers, and it has been shown that ICU nurses have back pain to a greater extent than the general population. Better planning, more space and pendulums from the ceiling give more room for manoeuvring, improve patient safety and prevent work-related injuries.32,33 A cramped room creates frustration among the nurses, which may be reflected in the provision of care. A way of improving planning and patient safety is to care for ICU patients in single rooms, 9 which was also seen in our results. The nurses felt that in single rooms, without curtains, they had a better overview of the patient, and relatives also had more space, which was believed to be more welcoming. According to previous studies single rooms and a welcoming environment make family visitors feel safer and more satisfied, 15 and having a relative present reduces the risk of delirium and has a positive impact on patients' recovery. 34 Privacy and confidentiality are more easily maintained in a single room, as information provided belongs to the patient being cared for and no one else.13,14 By law, all health professionals must maintain privacy and confidentiality. 35 In our analysis, the ICU environment made it difficult for the participants to comply with the law.
The nurses wanted to be near the patient and a central element for them in the room was the work station. The constant presence of the nurses inside the room made the work easier but also entailed difficulties as they often were interrupted and lost focus, which may compromise patient safety. The greatest source of error when nurses administer medication is interruption. 36 To improve patient safety the participants tried having the door closed, in order to reduce distractions and stimuli from the outside. However, they were still interrupted by the patients' visitors and various alarms from the medical equipment inside the room. To avoid these disturbances, yet maintain control, a work station behind soundproof glass walls was suggested. This wall would prevent disturbances and the nurses also believed that the patient would be less disturbed by their work. In many wards built according to EBD, the work station is separated from the patient room but still enables monitoring. 33 It has also been shown that staff experience fewer demands, less stress and improved concentration as a consequence of lower sound levels.13,18 The opportunity to get away from noise and its many distractions can reduce brain fatigue among nurses. As earlier described, sound-induced stress among nurses is related to emotional exhaustion and burnout. 9 If rounds and reports are done in these glass boxes confidentiality can be maintained. In the current environment, the participants asked any visitors to leave the room during rounds and reports, but the patients always remained and could not choose which information they wanted to receive.
The highly technological equipment and hygiene requirements that must be maintained made the environment cold and sterile. When the space was too small the rooms felt cramped and dark, the wellbeing of the participants was affected. Feeling a sense of wellbeing and work satisfaction reduces the risk of burnout. 37 The lack of natural light reduced wellbeing, as providing care in rooms with small windows without a view affected mood negatively among the nurses. The nurses described a frustration that their suggestions of large windows were neglected when rebuilding a ward. The participants became more positive when providing care in a bright room with large windows, they became energized and it was easier to go the extra mile for the patient. It has previously been described that health professionals benefit as communication and mood are improved and fatigue is reduced when they have access to natural light. 38 Other studies show that patients also benefit from windows and natural light,4,14,16 although some studies could not find any connection between daylight and lower medical costs, length of hospitalization or mortality.39,40 The nurse participants also used the windows and the view to anchor the patients in reality and establish personal contact by talking about the world outside the hospital. Being personal was a way of creating a pleasant atmosphere in the sterile environment.
The units where the data were collected had been built or renovated in the 1990s and should therefore have been designed according to the same guidelines, but are still different. The fact that data were collected in three units enables different perspectives on the environment. However, all participants, regardless of unit, reasoned along similar paths about the categories that emerged, suggesting that the results are reliable regardless of unit. The use of a gatekeeper can lead to bias when selection is made in order to obtain a specific result, 23 however, using three gatekeepers reduces the risk of bias. The selection is wide as the participants vary in age and work experience, which increases the study's validity. 41 The gender variation was small, as only one man participated; on the other hand this corresponds to the population of the ICUs.
Photographs are easy to take and collect, but difficult to analyse because they contain an abundance of complex data. Using the photographs without the participants' stories would contradict the very essence of photovoice, a method in which the meaning must be explained before the picture can be seen as a whole,21,24 as in this study. Photovoice is suitable for this kind of study since the participants' attention is directed to the object of the study and elicits data. 24 Since three researchers carried out interviews separately and asked different follow-up questions, varying data may have emerged in the interactions with the participants, 42 which can be seen as a disadvantage but also an advantage since more experiences of the phenomenon emerge. As the additional interviews added more nuances but not any new knowledge to the topic, saturation was reached. 29 All researchers were involved in the process of data analysis which increases the reliability of the results. 43 In addition, one of the authors has employed photovoice previously in studying an ICU environment. The analysis process was carried out individually and in a group, subcategories were then formed and overviewed by a controller to increase validity. The participants, settings, data collection and analysis of this study are well described and should allow for transferability to other hospitals and ICUs. The researchers are ICU nurses and therefore have a preconception of the phenomenon examined; however, we have been aware of this during the study and have constantly striven to be open to new knowledge. The awareness of our preconception reduced the risk of interpretations.
The findings of this study shed light on the specific elements in the physical environment that are vital for nurses while caring for critically ill patients. In addition, the way that the physical environment challenges nurses in their everyday clinical practice from a qualitative perspective is presented. To our knowledge such focus in research is sparse.
In conclusion, the nurses are well aware of the challenges in the physical environment and its impact of their daily work. Giving care with these challenges every day left the nurses with a feeling of frustration and inadequacy. To care in an environment with good lighting, reduced noise and adequate space is expected to increase the wellbeing of the participants. Therefore the opinions of health professionals should be taken into account when building and rebuilding wards, as these settings form their everyday work environment, but this is not currently done. The results of this study contain improvement proposals which can be used when designing new ICUs. Using EBD and a multidisciplinary team when planning ICUs would ultimately mean a lower cost to society since length of hospital stay is shortened, sick leave among staff is reduced and their wellbeing is increased. Not to be able to affect the environment can create frustration among nurses. However, the responsibility for the care environment still rests on a leadership, and at organizational level. Further research is needed to show politicians how much the care environment affects nurses physically and mentally. Increased wellbeing will lead to better care, indicating that an investment in a better care environment would be worthwhile and contributes to sustainable development.
Footnotes
Acknowledgements
We would like to thank all ICU staff for their participation.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.