
Abstract
Given the substantial increase in the documentation required of nurses in recent years, this article explores nurses’ perceptions of the value of documentation, and, subsequently, attempts to explain a puzzling tendency, whereby some nurses attach little value to arguably useful forms of documentation. We use data gathered from individual interviews with nursing leaders and focus-group interviews with frontline nurses at two wards in a Danish hospital. Our thematic analysis shows that nurses are divided between a positive view of documentation as something essential, and a negative one of it being a meaningless burden that distracts nurses from their ‘real’ work, contradicts their professional identity, and does not benefit the patient. However, except for some cases where the same information is registered twice (‘double registration’), we find no objective criteria for determining which types of documentation are perceived positively or negatively, as even arguably useful types are sometimes considered meaningless. We interpret this as being because of conflicting concepts of value: utility vs meaning. Using an existential theory of meaning, we argue that documentation’s practical utility alone is not sufficient to provide meaning. We thus suggest the need for finding a balance between: a) adjusting documentation requirements, b) adapting the nursing profession, and c) changing nurses’ perceptions of the value of documentation.
Background
Over the last few decades the specific documentation that nurses are expected to handle has been increasing across the Western world.1–2 Globally relevant research shows that nurses may spend ‘less than half of their working time on direct patient care’3(p.1027) and much of the rest of their time is spent on documentation. According to Danish legislation,4–6 all authorised healthcare professionals must document any professional contact with patients, including all general information regarding observations, diagnoses, and the current or potential problems of the patient. In detail, this includes personal patient data, the condition of the patient, template checklists, screening measurements, as well as all planned and completed interventions, and the evaluations of these interventions, all duly signed with the date and time of completion. 4 Documentation can be quite comprehensive; for example, the initial assessment of the patient upon hospital admission includes 14 points to be documented, 6 which range from screening all patients (over 16 years old) for bedsores, to noting the patient’s spiritual and cultural values.
The importance of nursing documentation in Denmark is acknowledged on numerous grounds. It is typically viewed as a precondition for diligent care and as an important communication tool, with the potential to enhance patient safety.7–9 Furthermore, electronic health records allow the collection, storage and extraction of enormous amounts of information. 10 Digital technologies should reduce paperwork, thereby providing prompt access to patient information. 11 These technologies are thought to increase the speed and quality of documentation, thereby freeing up time for direct patient care. 3 Considering the potential benefits of documentation, studies view it as a necessary part of modern nursing.12,13 Danish authorities have engaged in a digitalisation strategy, which practically eliminates all paper registration, 14 and should ensure systematic, comprehensive and effective documentation. The strategy also aims to create a common and standardised digital documentation system, but this has not yet been achieved at national level.
However, research also indicates that an increase in the amount of documentation is problematic,10,15–17 and can have effects such as reducing direct contact with the patient,3,18 and dehumanising patient care. 16 In one study, the implementation of digital documentation ‘left nurses feeling that they had less time to spend on patient care’19(p.74) – on average, nurses spend ‘more than half [of] their shift time using the computer’.19(p.75) Furthermore, nurses have struggled with digital documentation owing to factors such as a lack of IT experience, frustration with poorly functioning equipment, 16 time constraints, mismatches between staffing resources and workloads, a lack of clear guidelines for completing documentation, and ambivalence. 2 Furthermore, many nurses perceive an apparent lack of value for patients 2 and encounter cases of double documentation. 13 There is also fear of system failure, or struggles with slow programs that delay the documentation process. 11 Moreover, several studies find no significant relationship between the quality of nursing and the use of electronic health records.11,20,21
A Danish report shows that many nurses see documentation as a symptom of ‘externally defined management demands’, which ‘[interfere with] the direct time [spent] with the patient’,22(p.35) which, in short, leaves ‘less time for the core tasks’.22(p.35) Even if it is difficult to determine the exact amount of time nurses spend documenting, this report concluded that ‘the amount of documentation today [in Denmark] is inadequately high’.22(p.6) This contrasts with a positive view of documentation as a ‘precondition’12(p.489) and a ‘necessity’13(p.88),22 for good patient care.
As can be seen, the scientific literature reflects conflicting opinions regarding the value of documentation. However, this discrepancy not only reveals a diversity in documentation’s expected effects, but also in the criteria applied to evaluate it. Objective criteria such as effectivity and utility do not seem to be the only criteria that determine nurses’ experience of the value of documentation. The aim of the present study is to explore nurses’ perceptions of the value of documentation. We first examine and thematise nurses’ perceptions of documentation, but also interpret our results based on an existential theory which allows us to distinguish different forms of value, stressing the difference between utility and meaning.
Method
The data consisted of interviews with registered nurses including nurse leaders and nurses with no management function (who we will refer to simply as ‘nurses’ for the remainder of the article) (n = 27) from two wards of a Danish hospital of the capital region. The material includes individual interviews with leaders (L) (i.e., nine ward nurses and two heads of wards) and three focus-group interviews (FG) with 16 frontline nurses. The interviews and focus groups were recorded, then transcribed and coded in NVivo. Furthermore, testimonies were collected over two days of observing daily work and participating in three staff meetings of one hour each. Ward nurses and nurses were chosen by the head of the ward based on their willingness to participate and their availability. The interviews included open-ended questions about nurses’ professional identities and motivations, recent reforms in the health sector, and leadership participation in these reforms. Documentation work was treated as a fundamental element of the current reforms.
We approached the leaders’ interviews and nurses’ focus groups using a thematic analysis. 23 This method included the identification of all references to documentation work, followed by the coding of the material under different themes that reflected leaders’ and nurses’ experiences with such work, until saturation was achieved. Following discussion, we consolidated the various strands into two main categories. While we do not include any ethnographic or other analyses of the observations and meeting participation, the testimonies given in these situations might have influenced our analysis.
Ethical considerations
This study relied on the support of the hospital authorities and the approval of the Regional Ethical Research Council. All participation was voluntary, and no recording or observations occurred without the participants’ knowledge. We have avoided using quotations or references that might identify the participants.
Theoretical perspective
We interpret our findings using an existential theory of meaning inspired by Viktor Frankl24,25 and Søren Kierkegaard’s philosophy. 26 Such a theory allows us to understand why actions that can achieve practical results are not necessarily considered valuable, as they may lack existential meaning. According to Frankl, to ‘find meaning in one’s life is the primary motivational force’ behind human existence,24(p.99) but mere utility does not necessarily provide meaning. Practical actions are goal oriented and might generate a feeling of purpose, but do not necessarily provide existential meaning. Existential meaning is not achieved by directing our actions towards future goals, but rather by ensuring that the present moment acquires absolute value, what Kierkegaard calls ‘truly to be today’.27(p.39) Present useful actions which are purely means to future goals lack value in the present moment. Meanwhile, existential meaning demands that the present action acquires value in the present, and this can only be done, according to Kierkegaard, if the action has an ethical (or religious) value. ‘Only when life is considered ethically does it acquire beauty, truth, meaning’.28(p.271) In short, a nurse changing a catheter to avoid sepsis as a mere practical action has all its value in the future but changing a catheter to express genuine care for the patient is an ethical and existentially meaningful action, and its value lies in the present. Therefore, Kierkegaard can claim that, in the light of an ‘absolute’ ethical (or religious) value, ‘the means and the end are one and the same’.29(p.141) Shaped by an ethical value, actions become more than mere means, they become meaningful. Based on this theory, we aim to explain why certain forms of documentation are considered meaningless, despite being useful in some sense.
Findings
We identified several themes describing nurse leaders’ and nurses’ experiences of documentation (see Figure 1). We condensed the data into two main categories: the essential task and the meaningless burden. In the former, documentation is viewed as an essential tool for nursing. In the latter, documentation is seen as a meaningless, avoidable burden that keeps nurses and leaders from focusing on what they consider to be their ‘real’ work (i.e. direct contact with the patient). However, it is especially noteworthy that, particularly throughout the latter themes, a tone of indignation and rage against documentation requirements, occasionally mixed with ethical accusations, is prevalent. In these themes documentation is viewed as a burden, not (only) for being unpractical, but also because it works counter to nurses’ and leaders’ perceptions of the meaning and value of their work. Such a critical attitude is even perceived in relation to documentation which arguably has practical usefulness.
Registered nurses’ experiences of documentation.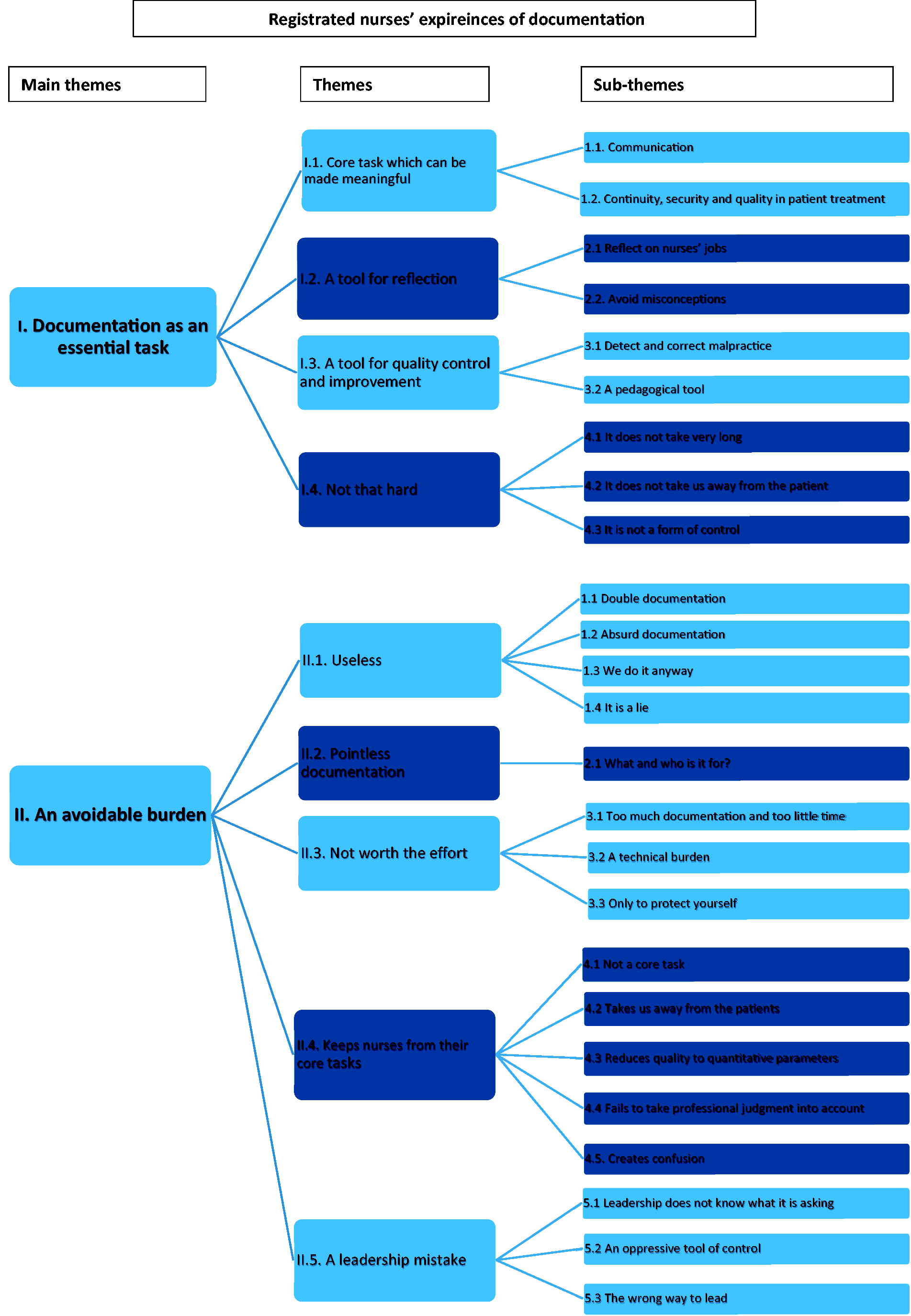
Documentation as an essential task
Core task which can be made meaningful
Numerous respondents, especially among leaders (L), declared that documentation is a core task of nursing staff: ‘Documentation is part of a nurse’s core tasks’ (L1). This is a task that is unlikely to disappear: ‘There are some nurses who think […] that the increase in documentation demands is a chapter that will soon be over, but it is not. It is here to stay’ (L2).
However, leaders tend to be aware that the value of documentation is not always evident, stressing that not all of it has the same value: We should not gather data just to gather data. The aim is to get involved so that the data can be used for something. We need data that is meaningful. (L4)
The following sub-themes cover the main reasons for viewing documentation as a meaningful core task for nurses and nurse leaders.
Communication
Documentation is viewed as essential for communicating with other sectors and colleagues about individual patients, something which is considered particularly meaningful, as expressed by a nurse from one of the focus groups (FGs): Documentation is meaningful if it is oriented towards the patient, and if it is about informing the next colleague about where the patient is in his pathway. (FG2) It has [value] for the next nurse who comes on duty. Therefore, it allows us to help each other as well as the patient. (FG2) I find meaning in documenting for my colleagues’ sake. (FG2) Much of the documentation we do is more for the benefit of the ward than for us. (L6)
Continuity, security and quality in patient treatment
Documentation can be an essential task in nurses’ and leaders’ work, given the perceived effect it has on ensuring continuity, security and quality of treatment. As one leader stated: It is necessary to have everything documented. With medicine, this is super-important – the patients might get double doses or too little if treatment is not documented. (L6) The documentation has to be there. Otherwise, we start from zero every time. Then the patient says: ‘Have you not read anything? Do you not know anything?’ They feel insecure. (FG1) [Documentation] is what we have learned as professionals – to document what we do with the patient. It is … a kind of art – a way of showing that we have an overview of the patient and the patient’s progress. (L3)
A tool for reflection
Reflect on nurses’ jobs
One leader presented documentation as a reflective tool: I think [documentation] is important because it makes nurses think more about what they have done. (L4) Some people with less capacity to think about things in a broader context view [documentation] as just another task … They ask ‘Why should we document so much? We do those things already. It is just about adjusting this practice here and there’. (L5)
Avoid misconceptions
Documentation also helps overcome misconceptions and prejudgment: You might have many conjectures and assumptions. When you examine them a little more closely, they look like a completely different thing – a whole other result in reality. […] It has been so clear there – how important it is to gather data in an area where … we assume something. We find that it is actually something else. (L6)
A tool for quality control and improvement
Documentation is considered a fundamental tool for leaders wishing to control and ensure quality in nurses’ work. The link with quality is unmistakable: ‘[Documentation] is a way to work with quality. This aspect surfaces a lot in relation to documentation’ (L4). Another leader stated: I periodically conduct quality checks. As a result, nurses’ documentation work now scores in the right time interval and their actions lie in the 90–95% range. (L3)
Detect and correct malpractice
Documentation allows nurses and leaders to detect and correct bad practices. This appears to be a relatively obvious benefit of documentation, at least for leaders: [I] say to the employees, ‘Try to look at it this way. Let us take some random patients. Who took this patient? Why did they not record the patient status?’ I also point out that we cannot know the status if we do not write things down. (L7)
A pedagogical tool
Documentation can also be viewed as a way of helping new nurses remember all their professional tasks. Documentation is ‘good for someone completely new who must learn it and remember it’ (L5).
Similarly: I am typically the one who goes to a nurse and says: ‘You have been at work for the last six days, and I can see that you cannot do this or that. Can I help you to learn how to do it?’ I am the one who has some authority to make corrections. (L6)
Not that hard
As discussed below, many nurses have a negative perception of documentation. However, many leaders dismiss some of the common critiques.
It does not take very long
When recounting discussions with nurses who do not complete their documentation work, one leader observed: I tell them: ‘It could be that in the future we will not need it, but right now we do. As you know, it does not take very long, does it?’. ‘No,’ they say, ‘but I forget.’ I tell them, ‘I understand, but try to remember it.’ (L5)
It does not take us away from the patient
Similarly, some leaders present documentation as something that does not need to take the nurse away from close contact with the patient – a common complaint among nurses. In this regard, one leader stated: We have so many laptops, so a nurse can just take one to a table by the bed of ‘Mrs Hansen’ and say: ‘Mrs. Hansen, I have to write a little about what we have done … Should I write this and this? What do you think I should tell my colleagues about you?’ Documentation does not need to happen in the office. It can just as easily happen while the nurse is with the patient. (L7)
It is worth noting that many nurses might disagree with the peaceful representation of documentation work. Notably, during our observations, we asked nurses why they did not carry out their documentation work in the patient’s presence. Some nurses indicated, depending on the circumstances, that it can be an unpleasant experience for both the nurse and the patient. Furthermore, computers are not always available, or they are placed in a way that leaves the nurse standing with his or her back to the patient, which is clearly off-putting.
It is not a form of control
Finally, one leader simply stated, ‘No one experiences documentation as a form of control’ (L8). Interestingly, this contradicts some of the testimonies discussed below.
An avoidable burden
Many nurses and leaders present documentation work as a burden that interrupts the flow of their core tasks. In this regard, documentation is viewed as not being worth the effort. Therefore, it could, and should, be avoided. Tellingly, the critical tone (especially in focus groups, but also among leaders) reflects a deep frustration that goes beyond a mere objective criticism of documentation as something impractical, reflecting a deep feeling of it being meaningless.
Useless
The first sub-themes cover situations in which documentation work is considered to have no use.
Double documentation
A noticeable form of useless documentation is double documentation. One nurse states that it is possible ‘to eliminate a whole lot of documentation because there is so much double, triple and irrelevant documentation’ (FG3). For example, one leader presented a situation in which data on a dementia patient brought to the hospital by ambulance had to be entered again even though it was already in another system: In my world, when a nurse ticks something off, [it is enough]. An authorised nurse has said ‘if the patient is suffering from dementia, it is done in the right way’… In my world, [doing it again] is double registration, which has no meaning! (L9)
Absurd documentation
Nurses and leaders also complained about unnecessary documentation, as expressed by a leader: There is some documentation … unnecessary documentation, for example. Why should I ask a 17-year-old boy who broke his finger, and is walking around and can move, if he has bedsores? That cannot be relevant. (L7)
We do it anyway
Nurses question the goal of documentation, as ‘we do [our work] anyway’ (i.e. without documenting it) (FG3). In other words, nurses question the need to document their activities as a way of ensuring that these activities are carried out, as they claim that they do them regardless of whether or not they are required to document them. This is a contentious point, as those who advocate the need for documentation argue that nurses do not necessarily do all that they should.
It is a lie
Occasionally, the data gathered by documentation are viewed as a ‘lie’. This arises from the fact that certain documentation and quality-control activities are performed when the hospital or the ward knows it is approaching accreditation, with all employees making a concerted effort to get things done correctly. According to the participants in one focus group: When it comes to accreditation, there is a false sense of security. The politicians think ‘Oh, it is going very well. It looks good.’ However, it is just like shooting yourself in the foot because everything is a lie. When it comes to a hygiene control by hygiene nurses, everything is put in place. Then, a week later, everything looks like an exploded toilet again. Therefore, we do not get the help we need because the authorities think that everything is good. I think this is an example of fraud. (FG3)
Pointless documentation
What is it and who is it for?
Nurses and leaders struggle to understand the purpose of the documentation and for whom it is being written. These questions tend to overlap. Nurses and leaders suggested that documentation requirements came from a faceless authority, such as ‘the region’ (L5), ‘society’ (FG3), ‘the management’ (FG3) or ‘the ward’ (FG2). One nurse questioned: Who follows this documentation? Where does it end up? In a pile in a cellar, where it gets burned? Where is it? Who uses it? Why should we do it?! (FG1)
Nurses also questioned whether implementing such documentation requirements really has the nurses’ and patients’ interests at heart: [Documentation] sits with an employee in the quality department, and his job is measured equally regardless of whether I do my job. His interest is not whether the documentation is for my sake or the patient’s. (FG2) Leaders have ambitions that do not necessarily correspond with what we do. That is why I think quality should be initiated from the bottom up. (FG2) We should not have to document our work because there is someone who needs statistics, who then complains to me because I did not do this or that. The documentation should be for my colleagues and for the patient’s sake. (FG2)
Not worth the effort
In this sub-theme, although respondents feel documentation might have a positive side, it is still viewed as imposing too significant a burden. These respondents believe that other tasks should be prioritised.
Too much documentation and too little time
Even though they are not necessarily identical, being busy and lacking time are commonly viewed as being related to the documentation burden. The complaint in this regard is that nurses are already busy with their main tasks and that documentation merely exacerbates their workload: Things take time … Helping a 90-year-old patient with diarrhoea who is dehydrated takes time and basic nursing competence. We can help such a patient, but we also have to document all that we do. That is what is difficult. (FG2)
Ironically, nurses also complained that the sheer amount of required documentation is a hindrance when completing documentation tasks: There are times when we do not manage to document everything because we have to fill out the catheter form, the PVK form … We must also check the oxygen and the drag (whether it is functioning on the first floor) and write it down. There is also the Accelerated Patient Pathway and the Cancer Pathway, which also require us to complete numerous forms. (FG2)
A technical burden
Another factor that might make documentation not worth the effort is the technical challenge it entails. As one nurse stated: ‘There are documentation systems that are slow and demand significant amounts of double documentation’ (FG3). Nurses repeatedly complained about the technical challenges associated with documentation, pointing to ‘a lack of computers’ and ‘slow systems’ (FG3). Computers take too long to start up, sometimes shut themselves down, and, at times, demand restarts. Similarly, certain pieces of equipment, such as barcode scanners, may suddenly lack batteries or fail. Moreover, some software requires too many ‘clicks’ to get to the right place, and various software systems are incompatible.
Deficient technologies, instead of saving time, make documentation burdensome, delay each step, and exponentially increase the amount of work and frustration.
Only to protect yourself
Occasionally, documentation was justified as a way of protecting nurses against patients’ complaints. As one leader stated during an observation: ‘If they do not do their documentation, I cannot defend them’ (L6). This is what one nurse called ‘cover-my-ass documentation’ (FG3). Nurses are aware of the legal problems that might result from poor documentation. In fact, when talking about how to deal with excessive and unnecessary documentation, a nurse described how he saved time by writing ‘Screening not necessary’, to which another nurse replied, ‘I do not think that will up hold in court’ (FG2).
Even though documentation could arguably protect nurses against complaints, it was commonly referred to as a pointless burden. The leaders’ insistence on documenting on these grounds was viewed with suspicion; one nurse ironically stated: ‘Everything we do should be documented. It is as if they expect a complaint to be filed by each of the patients!’ (FG3).
But if this line of argumentation is accepted, the consequence is that every activity should be documented. One nurse jokingly suggested: ‘They should just set up a camera so that everything will be documented automatically’ (FG3). For nurses, the argument itself can be unsettling, as anyone who does not register their actions in such a context comes under suspicion, undermining patient trust.
Keeps nurses from their core tasks
Not a core task
One of the key critiques of documentation requirements is that they get in the way of what nurses and leaders consider to be their core tasks: I can be a good nurse when the fundamental core tasks are in order. This is what frustrates me today … I can tell that the development is moving in another direction. We have to document, we have to write curves, we have to read … we get a pat on our shoulders when the curve goes up and we are notified when it goes down. In the meantime, [everything is a mess] patients’ drinks are dripping down, and the patient lies with the same nappy on for two days. (FG3)
Takes us away from the patients
As mentioned above, documentation is time consuming. However, for nurses and leaders, the truly negative aspect is that this is time taken away from the patient. We have lost the patient. (FG2)
Reduces quality to quantitative parameters
Documentation transforms how nurses’ main tasks are evaluated: Our main tasks are measured differently today. They are measured in terms of numbers and statistics, not in terms of how many letters of thanks we receive or how good the experience is for the patient … That is why the demands are different. (FG3)
Fails to take professional judgement into account
When discussing useless forms of documentation, one leader wished she ‘had a little more freedom of action’ (L6) to decide whether certain forms of documentation or procedures were necessary. As is evident in the previous discussion of the legal consequences of a lack of documentation, the fact that a nurse’s judgement of a screening as unnecessary has no juridical value is perceived as a negation of nurses’ professional ability.
Creates confusion
Respondents were asked if they could see some benefits in the documentation work as a means of ensuring that they remember their daily tasks. Some nurses replied that the amount of documentation ‘creates confusion’ (FG3). In other words, the problem is not remembering what to do, but rather remembering what needs to be documented.
A leadership mistake
When documentation is perceived as being a useless and meaningless burden, it is not surprising that leadership insistence on its importance and implementation is viewed (especially among nurses) as a mistake. However, whether nurses were referring to their immediate leaders or to the higher political authorities in this regard was unclear.
Leadership does not know what it is asking
Some nurses believe that the leadership does not know what it is asking of them. A nurse expressed this frustration as: It is this feeling that [the leaders] have no idea of what is happening out in the ward … We cannot continue to be pressured by these [documentation demands]. (FG3) I would like to see one of the people who is telling us what to do to try to take care of eight to ten patients while simultaneously documenting everything, just like they demand of us. (FG2) You get angry when you experience [leaders] going around looking for things that nurses should document. (FG2)
All of this makes the employees feel that the demands are endless. As one nurse ironically suggested: Are we constantly short on time? ‘Do you just have this? Have you also written those things down there?’ ‘Yes, and I also wrote it over there and I also actually did it … but, oh no, I did not write it down there.’ (FG3)
An oppressive tool of control
Documentation is also perceived as an oppressive tool of control used by leadership: We are constantly checked in terms of what we document. If the data shows that we documented only 60%, we are told off. We hear that it has to be 80% next week. (FG2)
One nurse also stated: ‘I feel that we have to do all of this documentation in order to prove that we have things under control’ (FG3).
The wrong way to lead
Nurses also link documentation to the fact that leadership has stopped working in close collaboration with nurses. Hospital leadership has become an office job, and the leader has become the person who controls the paperwork: My ward nurse, who is sitting in the office, suddenly comes out with some papers and asks ‘How is it going? Have you remembered …?’ (FG3)
Discussion
Beyond showing positive or negative experiences of documentation, what our data show is that nurses and leaders fluctuate between different criteria for determining the value of such work. While, on the one hand, documentation is evaluated according to objective practical results, especially by leaders, on the other hand we notice an evaluation of the meaning of documentation in relation to professional ethical values. Even in the case of positive experiences with documentation, we see that beyond the possible practical benefits, nurses and leaders will only call documentation ‘meaningful’ when they consider it as a way of ‘communicating’ and ‘helping’ their colleagues or the patient. According to our theoretical background,23,25,28 this is because meaning is achieved by the nurses relating documentation to the ethical values of their profession, in this case, helping someone. Similarly, the negative perceptions of documentation conclude that it is meaningless. This is not so much done by pointing to its lack of utility, but rather to the documentation’s perceived disruption of the ethical values of the nursing profession, especially its negative effect on contact with patients. In general, nurses seem to place higher value on meaning than on utility.
Since meaning relates to ethical values, it is not surprising that critical views of documentation are tainted by a tone of frustration, mixed with ethical accusations. The critiques of documentations do not express a mere objective displeasure with the lack of practical results, but rather value-loaded accusations, using words such as ‘cynical’, ‘lie’, or ‘hidden personal interests’. Consequently, even forms of documentation that could arguably be useful, such as, for example, documenting for protection in the case of complaints, are looked upon with suspicion. This is not because it is impractical, but primarily because it seems to betray the fundamental trust that should exist between the nurse and the patient, which again renders this form of documentation meaningless.
However, beyond the many pros and cons, at the core of the nurses’ and leaders’ complaints appears to be that they are forced to prioritise what they see as purely practical administrative tasks, while sacrificing what they consider the existentially meaningful part of their work. Having to prioritise tasks which they see as disrupting or eliminating direct and personal contact with the patient is the source of a fundamental frustration.
Limitations
This study reflects how nurses and leaders perceive the value of documentation, which is not necessarily akin to an objective categorisation of the types of documentation or their purposes. Therefore, there may be other benefits or problems with documentation (for example, administrative advantages or ethical problems) but if we do not address them, it is simply because they were not present in our interviews.
It is important to distinguish nurses’ perceptions of documentation from their explanations of why it is required. If a nurse believes that documentation requirements are the result of cold and cynical interest, we should not necessarily assume that this is the true driver of documentation requirements.
Conclusion
To determine whether documentation is an essential task, or a meaningless burden is not merely an objective discussion. Even ‘objectively’ useful documentation can be experienced as meaningless. Except in cases of double documentation, where almost all respondents agree on its futility, it is difficult to determine which concrete documentation work could or should be eliminated, and why. The perceived value of documentation is determined based on different and occasionally immeasurable criteria. For example, lack of time for basic nursing care triggers a negative evaluation of documentation, which otherwise might be considered useful. Furthermore, the meaning of ‘basic nursing care’ is subjective. While some would stress treatment and medication, others might prioritise service and personal contact.
Therefore, nurses’ and leaders’ negative experiences with documentation are not necessarily a result of not finding any (practical) value in it. However, they might result from an inability to feel that documentation should be prioritised over other (more meaningful) activities, such as patient contact. As such, arguing, for example, that documentation will benefit the patient in the long run, if perceived as a mere practical goal, will not necessarily convince a nurse to prioritise it, as the nurse experiences a loss of meaning in their present actions, which is essential for the general perception of meaning. In short, insisting on documentation utility will not generate engagement among nurses who experience a loss of meaning.
Implications
To enjoy the benefits of documentation while simultaneously alleviating nurses’ negative experiences, our analysis points to at least three elements that could be recommended for change and reflection. First, the amount and forms of documentation should be re-evaluated (taking nurses’ perspectives into account). Second, the nursing professional identity might need to find a better balance between the expected personal contact and administrative work. Finally, nurses’ perceptions of the value of documentation could be influenced by clarifying its worth (utility and meaning). However, this article shows that stressing documentation’s practical utility does not seem to be enough to make nurses find it meaningful; thus other approaches should be found.
These three possible steps are not independent of one another. Any definition of ‘valuable documentation’ relates to the definition of the nursing profession. Any change in the definition of the nursing profession to include documentation work might be accused of prioritising what is useful over what is meaningful. The connections among these elements can be seen from the fact that documentation is already changing nurses’ (and their leaders’) views of the nursing profession. Unfortunately, this shift entails a great deal of negative experiences.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.
Note
This research was approved by the Den Nationale Videnskabsetiske Komité, Region Hovedstaden (The National Science Ethics Committee, Capital Region) -approval number H-15013263 FSP-.