
Abstract
Objectives:
Spirituality and spiritual care are the critical components of patient care. In recent years, spirituality has been indicated as a crucial but often overlooked component of patient health. Despite their benefits, several factors prevent nurses from providing spiritual care. Hence, the purpose of this study was to evaluate the current state of spiritual care perception of nurses in Southwest Ethiopia as well as the factors influencing it.
Methods:
From 1 August to 2 September 2021, an institution-based cross-sectional study was performed on nurses at five government hospitals in Southwest Ethiopia. Study participants were selected using a simple random sampling method. Data were collected using the Spirituality and Spiritual Care Rating Scale (SSCRS). The collected data were recorded into EpiData 4.1 and SPSS version 25. Simple and multivariable linear regression analyses were used to identify factors associated with spiritual care perception. Statistical significance was set at p < 0.05.
Results:
A total of 390 nurses were enrolled in the study, yielding a response rate of 96.8%. The mean score for nurses’ perception of spiritual care for patients was moderate, that is, 3.11 ± 0.78. Age (p < 0.05), clinical experience (p < 0.05), educational status (p < 0.05), and religion (p < 0.05) were significantly associated with spiritual care perceptions.
Conclusion:
Nurses’ perception of spiritual care was moderate. It is affected by nurses’ age, clinical experience, educational level, and religion. This expanding body of data should be used to notify nurse managers and nursing management personnel to provide spiritual care training, planning, and services.
Introduction
The World Health Organization (WHO) 1 states that, “health is a state of complete physical, mental, and social well-being, not merely the absence of disease and infirmity.” To improve psychosocial well-being, the definition of health includes not only physical illness but also spiritual health. 2 Despite the importance of spirituality in healthcare services, it is frequently overlooked and misunderstood. 3 Although nurses believe that spiritual care is indeed a vital aspect of nursing care, perceptions and their awareness of spirituality differ, which might hinder their competence in providing appropriate care. 4
A holy spirit, feelings of togetherness, intention and meaning in life, relationships, and spirituality are all aspects of “spiritual nursing care.” 5 Meeting the spiritual needs of patients is a truly rewarding experience for both nurses and patients, and it can hasten the development of a therapeutic relationship. 6 However, ethnicity, religious affiliation, educational status, working environment, and professional experience of nurses influence their understanding of “spirituality and spiritual care.”7–9
Various investigations have demonstrated that “spirituality and spiritual care” help reduce the symptoms of anxiety, worry, and feelings of hopelessness that an individual may experience during a disease, leading to increased hope, coping mechanisms, and better quality of life.10–12 Patients’ well-being appears to be negatively affected by unmet social and emotional demands. 13 Researchers have recently discovered that being sensitive to patients’ spiritual needs enables them to provide true and comprehensive healthcare. 14 Although spirituality is an important aspect, its approach to patient care has often been overlooked. 15
Numerous nurse practitioners believed that spiritual care was not their task, but rather the task of clergy or religious leaders and this could be attributed to a misunderstanding of the difference between “spirituality and religion.” 16 To appreciate the spiritual needs of others, nurse practitioners must first recognize their spirituality and be cognizant of their overall views and beliefs. 17
Data on spiritual care perception among Ethiopian nurses, as well as in the research field, are limited. This is Ethiopia’s first study to evaluate nurses’ perceptions of spiritual care. Hence, the purpose of this study was to evaluate the current state of spiritual care perception of nurses in Southwest Ethiopia as well as the factors influencing it.
Methods
Study design, setting, and population
This institution-based multicenter cross-sectional study was conducted at Mizan–Tepi University Teaching Hospital, Agarro General Hospital, Gebretsadik Shawo General Hospital, Shenen Gibe General Hospital, and Jimma Medical Center, Ethiopia, from 1 August to 2 September 2021. These hospitals have different outpatient departments and four wards, namely, medical, surgical, pediatrics, and obstetrics/gynecology wards. There were 1500 nurses with different academic backgrounds in the selected hospitals. These hospitals are expected to serve for more than 18,000,000.00 people. Currently, the Jimma Medical Center is the largest referral hospital in Southwest Ethiopia, providing services for approximately 15 million people in its catchment area.
Nurses working in Mizan–Tepi University Teaching Hospital, Agarro General Hospital, Gebretsadik Shawo General Hospital, Shenen Gibe General Hospital, and Jimma Medical Center were the study’s source population. The study population consisted of nurses working at selected hospitals in Southwest Ethiopia during the data collection period.
Eligibility criteria
Nurses who worked at selected public hospitals in Southwest Ethiopia during the data collection period and those with more than 6 months of experience were included, and nurses who were given free service and seriously ill during the data collection period were excluded.
Sample size and sampling procedure
The representative sample was determined using a single-population proportion formula. The following parameters have been used to determine the sample size: the proportion of perception of spiritual care by nurses was 50%, the margin of error was 0.05, the confidence level was 95%, and the rate of non-response was 5%, resulting in a final sample of 403. The number and list of nurses were obtained from each hospital human resources office. The total of 1032 nurses at the selected hospitals fulfilled the inclusion criteria. Based on this information, the study population was assigned proportionally to each institution. Consequently, the participants in this study were selected using systematic sampling. Every two nurses were recruited from each of the hospitals. The first participant was chosen randomly.
Data collection tools and procedures
The data were collected using self-administered question-naires:
The Spirituality and Spiritual care rating Scale (SSCRS) was used to gather data on nurses’ spiritual care perception. It includes 17 items and four subdivisions: spirituality, spiritual care; religiosity and personalized care scale. The SSCRS is a 5-point Likert scale with 1 indicating “definitely do not agree” and 5 “totally agree.” Four items conversely scored on the scale. The SSCRS has demonstrated satisfactory validity and reliability. It has acceptable internal consistency with a Cronbach’s alpha coefficient of 0.64. When the total point average was close to 5, this indicated that there was a high perception of spirituality and spiritual care.
18
Section two encompasses the participants’ demographic information, including age, sexual identity, religion, marital status, and educational status. In addition, work-related factors included clinical experience, type of ward, weekly working hours, training, and caring experiences of spiritual care. Data were gathered by three BSc nurses and two adult health nurse specialists who served as supervisors.
Operational definition
Perception of spiritual care
Nurses’ perception in spiritual care was measured using 17 items on a 5-point Likert-type scale with value ranging from 17 to 85. The higher the value, the higher the perception of spirituality and spiritual care:
18
The overall mean score was divided by 17, and the nurses had a value ranging from 1 to 5. The perception of spiritual care level was then divided into low, moderate and high based on this score. A low level is a mean score between 1 and 2.33, a moderate level is a mean score between 2.34 and 3.67, and a high level is a mean score between 3.68 and 5.
19
Data quality assurance
Data quality was ensured during collection, entry, and analysis. The tool’s validity was verified using face validity. Data collectors were trained intensively for 2 days on the data collection instruments. Furthermore, close supervision was provided throughout the data collection process. The tool was pretested on 5% (21 nurses) of the actual sample size in the Tepi General Hospital 1 week before the actual data collection period. The results showed that Cronbach’s alpha of the overall Spirituality and Spiritual Care Rating Scale (SSCRS) was 0.73 and each subscale ranged from 0.81 to 0.67, which was reliable.
Statistical analysis
EpiData 4.1 was used to code the data set, and SPSS version 25 was used for the analysis. To summarize the data, frequency, percentage, root-mean square deviation, and mean were used as descriptive statistics. The link between spiritual care perception and the explanatory variables was first investigated using bivariate linear regression. Variables with p < 0.25 in bivariate linear regression were candidates for multiple linear regression. Multiple regression analysis was performed to account for potential confounders. The statistical significance level was set at p < 0.05. The assumptions of multiple linear regression were tested before analyzing the results. The Kolmogorov–Smirnov test validated the normality assumption. The variance inflation factor (VIF) was used to test the collinearity assumption and determine the correlation between the independent variables. According to the findings, all variables had a VIF of less than 5.
Results
Socio-demographic characteristics
Of the 403 invited participants, 390 completed the questionnaire, yielding a response rate of 98.6%. The participants’ average age was 29.01 years (standard deviation (SD) ±4.79 years), and the majority (75.0%) were in the 25–29 years age group. More than half (55.9%) were male and 146 (37.4%) were Muslim. More than 2/3rd (71.8%) of them had BSc degrees in nursing (Table 1).
Socio-demographic characteristics of nurses at selected public hospitals in Southwest Ethiopia, 2021 (n = 390).

SD: standard deviation.
Work-related factors
Two hundred seventy-two (69.7%) participants had less than 5 years of clinical experience. They were distributed into eight wards, of which 68 (17.4%) were in the medical ward. More than 2/3rd (72.3%) of the participants had less than 40 h of weekly working hours. The majority (87.2%) of nurses did not receive any training on spiritual care and 279 (71.5%) had no experience of caring for patients with spiritual needs (Table 2).
Work-related characteristics of nurses at selected public hospitals in Southwest Ethiopia, 2021 (n = 390).

ICU: intensive care unit.
The level of spiritual care perception
The mean value and standard deviation of spiritual care perception levels were calculated. The average SSCRS result was 3.11 (SD ±0.78) out of a possible total of 5 points, indicating a moderate level of spiritual care perception. The mean spiritual care perception scores for knowledge of “Spirituality, Spiritual care, Religiosity, and Personalized care were 2.97 (SD ±0.86), 2.91 (SD ±0.80), 3.28 (SD ±0.88), and 3.27 (SD ±0.97) respectively.” The lowest mean score, 2.91 (SD ±0.80), was for knowledge of “Spiritual care.” The study’s findings showed that the participants rated their spiritual care perception as moderate (Table 3).
The level of spiritual care perception among nurses in Southwest Ethiopia, 2021.
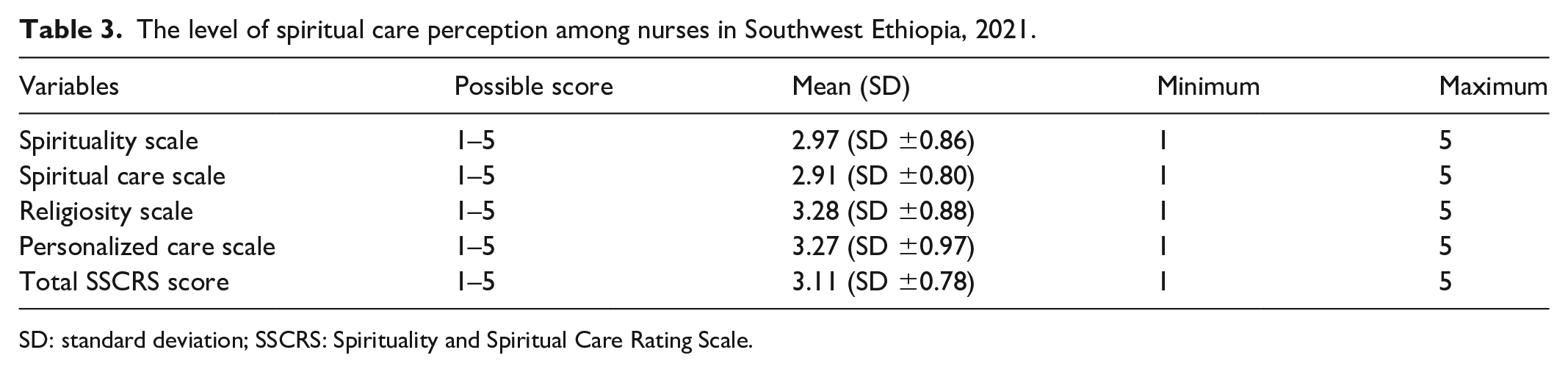
SD: standard deviation; SSCRS: Spirituality and Spiritual Care Rating Scale.
Factors associated with spiritual care perception among nurses
Multivariable linear regression analyses revealed factors associated with spiritual perception among nurses. In bivariate linear regression, age, clinical experience, educational status, marital status, and religion were found to be substantially associated with spiritual care perception among nurses at p < 0.25. To investigate the factors related to spiritual care perception, independent variables with p < 0.25 in the bivariate linear regression analysis were added to the multivariable linear regression analysis. At a significance level of 0.05, the backward elimination approach was used to select the variables for the final model.
The findings revealed that age, clinical experience, educational status, and religion were significantly associated with spiritual care perceptions among nurses. However, marital status was not significantly associated with nurses’ perception of spiritual care. Accordingly, a 1-year increase in age resulted in a −0.043 unit decrease in spiritual care perception (β = −0.043, p = 0.034). A 1-year increase in years of nursing experience resulted in a 0.07 unit increase in nurses’ perceptions of spiritual care (β = 0.07, p = 0.004). Being a bachelor’s degree holder increases spiritual care perception by 0.215 (β = 0.215, p = 0.029) and having a master’s degree increases spiritual care perception by 0.471 (β = 0.471, p = 0.016) than diploma nurses. Being Muslim increased spiritual care perception by 0.269 (β = 0.269, p = 0.03) and being a Protestant increased spiritual care perception by 0.337 (β = 0.337, p = 0.002) compared to Orthodox religion (Table 4).
Multivariable linear regression analysis of spiritual care perception among nurses at selected public hospitals in Southwest Ethiopia, 2021.

CI: confidence interval; SE: standard error.
Discussion
This study assessed the current state of spiritual care perception and associated factors among nurses. According to the findings, the mean score for a nurse’s spiritual care perception was 3.11. This indicates that there is a moderate level of spiritual care perception among nurses in Southwest Ethiopia.
The evidence was lower than that of a cross-sectional study on spiritual care perception among Muslim nurses conducted in Indonesia, which had a total mean of 4.13. 20 This may be because Indonesian nurses received spiritual care training and had previous spiritual care experiences. The current findings, however, were higher when compared to a cross-sectional study on “Spirituality and Spiritual Care among 259 Nurses at Qazvin University of Medical Sciences, Iran,” which reported that the overall average score for spirituality and spiritual care was 2.84. 21 The main barriers to providing spiritual support were heavy workload, a lack of awareness about spiritual care, a lack of interest, the variability of clients’ spiritual needs, as well as a sense of being “incompetent” to give spiritual care.
Another notable element of this study is the identification of spiritual perception-related characteristics. Personal variables such as age, sex, professional experience, and personal spiritual views may influence spiritual care competence, resulting in variations in their ability to provide spiritual care. 22 In this study, age, clinical experience, educational status, and religion were significantly related to spiritual care perception.
According to the findings of this study, old age predicted a lower perception of spiritual care. This is consistent with the findings of a Turkish study that found that the youngest age group had higher scale scores. 4 In contrast, a study conducted in Turkey revealed that older nurses demonstrated higher spiritual care perception scores. 23 This disparity could be attributed to differences in lifestyles, socioeconomic characteristics, and study settings.
This study’s findings also show that longer clinical experience predicts a higher perception of spiritual care. This finding is consistent with the findings of a study conducted in Riyadh, Saudi Arabia, on “Nurses’ Perceptions of Spirituality and Spiritual Care” among 978 nurses, which found statistically significant differences between nurses’ perceptions of spirituality and spiritual care and their nursing experience duration. 4 One possible explanation is that nurses learn to value “spirituality and spiritual care” and become more comfortable with their spirituality over time.
In this study, as nurses’ education levels increased, their mean SSCRS scores increased significantly, which was consistent with previous findings at Qazvin University of Medical Sciences in Iran, which showed that spiritual care perception was significantly associated with nurses’ educational level. 21 One possible explanation is that nurse practitioners with better educational attainment have a wider scope of nursing skillsets to tackle problems and provide proficient spiritual support.
The findings of this study’s findings also showed that religious affiliation increases perceptions of spiritual care. This is consistent with the findings of a Hong Kong study, which found a significant difference between spiritual care perception and religious affiliation. 24 Possible explanations include that subjects with religious affiliations have a more favorable viewpoint on spiritual practice and appear to be more perceptive of clients’ spiritual needs. 25
Mean scores obtained by nurses from the SSCRS and subscales as well as sex, type of ward, receiving training, marital status, and spiritual care experience were determined not to affect mean scores for spiritual care perception. Similarly, studies conducted in Turkey revealed that these variables do not affect spiritual care perception and competence.22,26 It also stated that monthly income, monthly number of shifts, and average weekly working hours were significantly associated with spiritual care perception and professional quality of life. This discrepancy might be due to differences in population characteristics, and the tools that they have incorporated. This study has certain limitations. The study used self-reported data from nurses, which could have resulted in social desirability bias. The results may not be generalizable to other Ethiopian hospitals and medical centers because the study was limited to five public hospitals in Southwest Ethiopia. Because the study was cross-sectional, causality could not be determined.
Conclusion
The nurses’ perception of spiritual care was moderate. It is affected by nurses’ age, clinical experience, educational level, and religion. This expanding body of data should be used to notify nurse managers and nursing management personnel to provide spiritual care training, planning, and services. This encourages Ethiopian nursing curriculum developers to include spiritual care in their current curricula, as well as the necessity for spiritual care training for nurses. Future researchers, including nurses working in private clinics, should conduct further studies. A longitudinal study with a large sample size is required to determine cause-and-effect relationships.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221104436 – Supplemental material for Nurse’s spiritual care perception in Ethiopia: A multicenter cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121221104436 for Nurse’s spiritual care perception in Ethiopia: A multicenter cross-sectional study by Kalid Seid and Mekdes Eneyew in SAGE Open Medicine
Footnotes
Acknowledgements
The authors are grateful to Mizan–Tepi University for permission to undertake this study. The authors would like to express our heartfelt appreciation to the hospitals and personnel chosen for their ongoing assistance. Ultimately, the authors would like to apply data collectors to all the participants in the study.
Author contributions
K.S. contributed to the conception, study design, execution, acquisition of data, analysis, and interpretation. M.E. contributed to the conception, study design, and interpretation. The final manuscript has been read and approved by all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Mizan–Tepi University, College of Medicine and Health Sciences ethics committee under reference no. NURS/368/13.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.
Data sharing and data availability statement
Data used for this manuscript are available from corresponding author at
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.