
Abstract
Qualitatively, research has demonstrated the existence of bricolage among healthcare staff, i.e. solving problems on the spot by resources at hand, and its potential to lead to innovation. However, we know little about the spread of bricolage activity and its potential role for innovation in healthcare. The aim of this study was therefore to provide an instrument for measuring bricolage activity among nurses, to test the measure and learn about the spread of bricolage in nursing in Denmark. We used a mixed-method design including a translation–back translation, a pre-test and a pilot test. Primary data were collected during 2015 via interviews and a survey, including 248 nurses. The analysis revealed that the majority of nurses rated themselves and colleagues as having a high level of bricolage activity. This study’s preliminary validations (content and face validation), of the translated Bricolage Measure, confirmed the usability of the instrument to examine bricolage activity in nursing in Denmark.
Introduction
Increasing pressure on public budgets following the recent financial crisis in Europe, as well as demands to address major societal challenges and increased complexity in patient pathways have heightened interest in innovation in health services.1,2 Consequently, a solid understanding of what health services innovation is, and how it is perceived, is vital to research on the characteristics of innovation as well as the development of measurement frameworks.1,2
In this article we refer to bricolage activity as a possible path to innovation in health services – innovation being realization of new ideas in practice. The concept of bricolage activity, as it is used in this study, comes from anthropologist Clade Lévi-Strauss, who compared the savage or untamed mind (not confined to any culture or period in history, however) with the mind of the bricoleur, a handyman acting in a spontaneous way creating structures by means of events contrary to the scientist who creates events by means of structures. 3 Lévi-Strauss thus defined the bricoleur as someone whose rules are ‘to make do with “whatever is at hand”’3(p.17) ‘collected or retained on the principle that “they may always come in handy”’.3(p.18) Baker and Nelson use the concept of ‘resource’ to define bricolage as ‘making do by applying combinations of the resources at hand to new problems and opportunities’.4(p.333)
Bricolage can be seen as small, micro-incremental processes of innovation by resources at hand challenging existing practices. Over time, bricolage activity can add up to larger more visible innovations. 5 Bricolage as a path to innovation differs, however, from classical understandings of innovation as consisting of linear and planned processes. Instead it posits a relational and contingent approach to how resources are used for innovation and value creation. Innovation has traditionally been seen as rooted in research and development, controlled and planned by researchers and managers, and as having relatively well-defined impacts. 6 This notion also comes across in health services. Yet, in health services as in other services, innovations can also be seen as new practices that emerge from interactions between providers and receivers of services (i.e. nurse and patient) and these may sometimes only be recognized retrospectively as innovations. 7 The concept of bricolage is promising because it refers to a specific activity of innovation formed by resources at hand that can be observed and perhaps measured. 8 However, we still know little about how to measure bricolage activity quantitatively in healthcare settings and thus observe its innovation potential.
Background
Case studies in healthcare have shown how bricolage activities can be a path to change and innovation in service organizations characterized by resource constraints. For example Andersen described how resources in the public sector can be mobilized for problem-solving activities by bricolage. 9 Fuglsang and Sørensen 5 showed that bricolage by Danish home-helpers’ day-to-day problem-solving activities was a possible path to innovation in elderly care, and Timmermans and Berg demonstrated how nurses and other healthcare staff tinker with the protocol and thereby act as bricoleurs to make the protocol workable in practice. 10 The concept of bricolage describes dynamic processes of innovation which expand the framework of innovation usually applied to the public sector. 2 The role of bricolage for innovation in the public sector has so far not been measured. Yet, based in a qualitative evaluation of more than 1500 examples of public sector innovations in six countries, Bugge and Bloch suggest that almost a third of the evaluated innovations were bricolage-type innovation. 2
The existing literature examining bricolage, specifically within nursing, revealed only two studies in the databases PubMed, ProQuest, Scopus and Cinahl in January 2016. Our main search terms were: Bricolage, Bricoleur, Innovation, Nursing, Public sector and Healthcare sector. Additionally, the search terms Creative behavior, Creative problem solving, Tinkering and Improvization were used to make sure those processes/concepts similar to bricolage were found and studied. Two case studies used the notion of bricolage to conceptualize nursing practices 11 and understand how nurses act as bricoleurs in fall prevention. 12 The two studies define bricolage with reference to Lévi-Strauss 3 as a problem-oriented behavior and suggest that bricolage is a phenomenon that can incorporate an otherwise unspoken aspect of nursing; a creative behavior where nurses find solutions to everyday problems by using whatever resources are available, such as personal experience, evidence-based knowledge or whatever equipment is usable at a given moment.11,12 The two studies suggest bricolage may allow increased effectiveness on a daily basis in nursing and hold potential for solutions in favor of both patient and staff satisfaction.11,12 However, at this point in time, it is not possible to determine if and to what extent bricolage exists among nurses. Further research within nursing and bricolage is therefore required.
In the search for bricolage literature, a questionnaire called The Bricolage Measure was discovered. The Bricolage Measure was originally developed and tested in Australia by Senyard and colleagues to measure bricolage activity quantitatively in resource-constrained firms.8,13 The measure has not been tested within health services or nursing. Therefore, the aim of this study was to translate and validate the Bricolage Measure so that it could be used to quantitatively measure bricolage activity among nurses in a healthcare setting, to test the measure and learn about the spread of bricolage in nursing in Denmark and thereby contribute to the possible further investigation of bricolage in nursing.
Design and method
To translate, initiate validation analysis and test the Bricolage Measure among nurses in a healthcare setting, we chose a mixed-method design including both qualitative and quantitative methods: A translation–back translation, a pre-test and a pilot test.
The theoretical framework and development of the Bricolage Measure
The Bricolage Measure was developed on the basis of a grounded theory study by Baker and Nelson. 4 This study included fieldwork studies, case studies and descriptions of observed bricolage activity among employees in different resource constraint firms. Baker and Nelson created a theory and a definition of the concept bricolage and argued that bricolage consists of three elements: 1) making do, 2) resources at hand, and 3) combination of resources for new purposes. 4 Together these three elements form the definition of bricolage: ‘Making do by applying combinations of the resources at hand to new problems and opportunities’.4(p.333)
According to Baker and Nelson it is important to understand each of the three elements and the interaction and dependence between them to understand when bricolage is present. 4 The first element making do refers to a way of thinking about problems and challenges and can be experienced as positive or negative depending on whether you and your colleagues think you can solve problems (make do) in general, with whatever resources you have at hand. If bricolage is present in an organization, the staff will have a positive interpretation of making do, a willingness to experiment and not be limited by a potential lack of resources. The second element, resources at hand, refers to existing resources in the forms of materials, equipment, people and their knowledge and experience, or anything else that can be used to get the job done. An organization that exhibits bricolage activity recognizes the use of resources that others would consider useless or unimportant. 4 The third element, combination of resources for new purposes, describes the combination of the previous two elements by connecting these in a creative process. If the organization is willing to see the potential in existing resources then the organization and its employees can create new solutions and possible innovation by thinking creatively and combining resources in untraditional ways. Every element is, according to the definition, inextricably linked to and exists by virtue of each other element, and bricolage thus only exists if all of the elements are present at the same time. 4
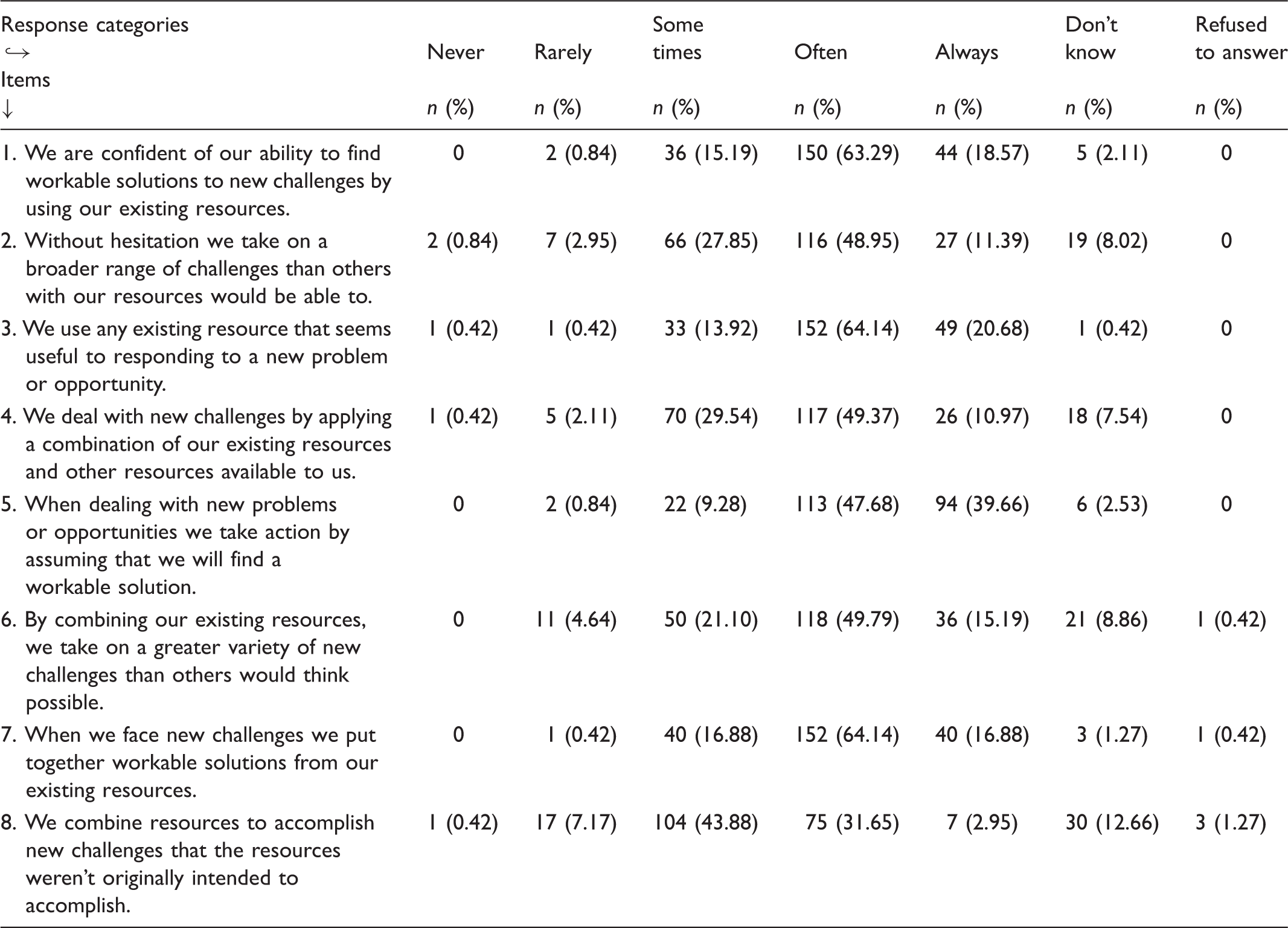
The translated Danish Bricolage Measure presented in English and the distribution of the 237 respondents’ answers to the eight items in the pilot test.
The translation–back translation
The aim of the translation–back translation was to ensure that the Danish version of the questionnaire was clear, precise and equivalent in comparison to the original English version. 16
Data collection and analysis
A translation–back translation method recommended by Behling and Law consisting of four steps 16 was chosen to ensure a high degree of informativness and source-language transparency for the researchers in the translation process.
Firstly, a bilingual translator native in the target language, Danish, from a professional translation firm (TQ translation) was, in January 2015, translating the original Bricolage Measure into Danish. The translator was instructed to focus on the context rather than on a literal translation and note down if the translation could give more than one solution. 16 Consensus about the final wording was reached after discussions between the researchers. Secondly, the Danish version was then back-translated into English by a second bilingual translator native in the source language, English, with no knowledge of the first translation. The translators did not have a background in healthcare but were trained in translating texts related to healthcare, i.e. questionnaires, brochures, pamphlets. Thirdly, the original and back-translated versions were compared to ensure semantic equivalence. If substantial differences existed the fourth step would be to prepare another target-language draft containing modifications designed to eliminate discrepancies. 16
The pre-test
The aim of the pre-test was to produce in-depth qualitative data which are central for analyzing the face and content validity of the translated instrument. The pre-test of the translated Bricolage Measure followed the guidelines from Fayers and Machin 17 and was carried out between 15 January and 3 March 2015. The analyses of validity were used to identify any major challenges with the questionnaire and to help solve these before pilot testing.16,17
Data – sample and collection
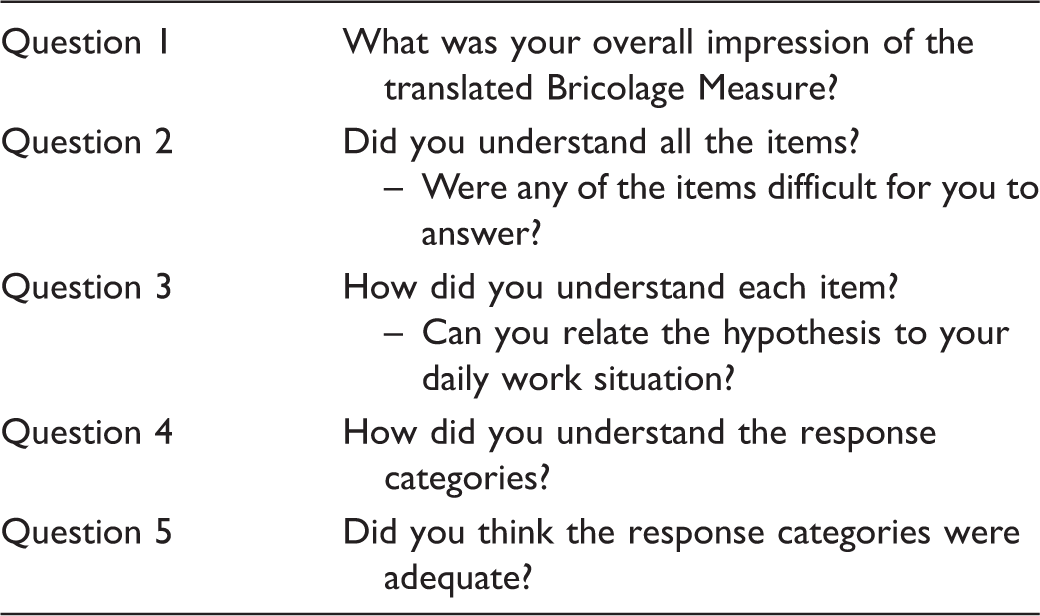
The interview guide used for the pre-test.
Data analysis
A content analysis of the face and content validity was carried out on the basis of the 11 transcribed interviews performed in the pre-test. The analysis of face validity, the overall impression, immediate transparency and understanding of the items, was carried out by examining specifically the nurses’ responses to questions one, two and three in the interview guide (Table 2). The problems emerging about choice of words, sentence construction or alterations were first discussed between the researchers before consulting the makers of the original Bricolage Measure and adjusting the measure in accordance with the findings, without changing the overall meaning of the translation.
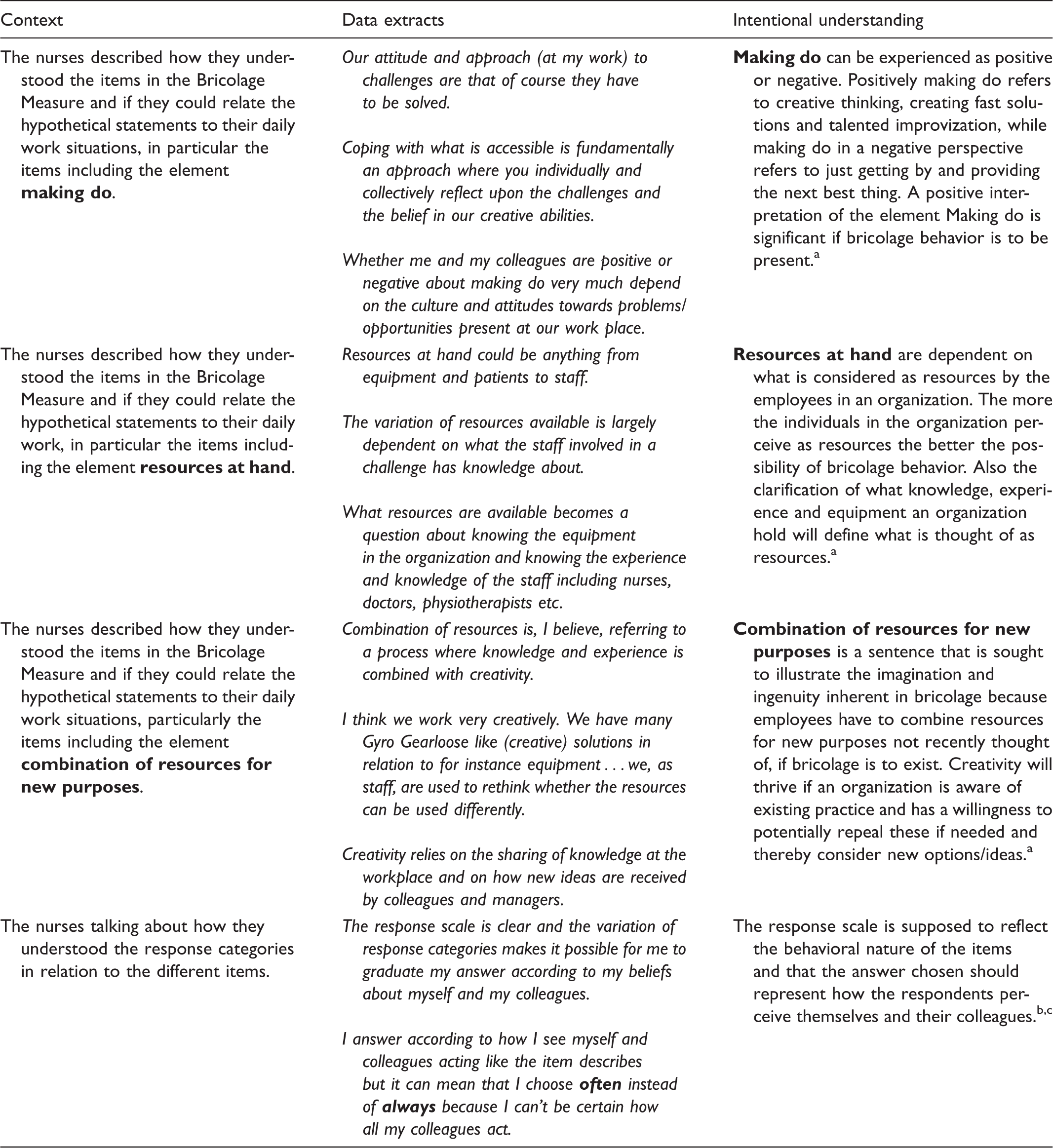
The analysis of content validity, the degree to which items adequately represent the domain of interest, was performed by using the interview data from questions three, four and five in the interview guide (Table 2). Analyses were performed using a comparison of the specific interview data with how the items and response scale were to be understood according to developers of the questionnaire, Senyard and colleagues,8,13 and the original understanding of the bricolage concept found in the grounded theory study by Baker and Nelson. 4 To display the result of the analysis of content validity the nurses’ responses from the pre-test interviews were paired, in a table, with the representative element from the definition of bricolage formulated by Senyard et al.8,13 and Baker and Nelson. 4
The pilot test
The purpose of the pilot test was to determine the proliferation of bricolage among nurses in the Danish healthcare system and thereby to confirm or disprove the usability of the Bricolage Measure and the relevance of continuing the work with validity. The pilot test followed the guidelines of Fayers and Machin 17 and was carried out between 4 March and 4 April 2015.
Data – sample and collection
The participants in the pilot test were found by using a closed group for nurses on Facebook. A random sample was invited by choosing every 20th person on an alphabetically sorted list of 10,125 members of this group on 4 March 2015. Inclusion criteria were similar to participation in the pre-test, meaning that participants worked as a nurse in primary or secondary care in Denmark. If the chosen person did not meet the inclusion criteria, the person figuring to the right was chosen instead. The selected persons received an invitation describing, and informing them about, the study. An invitation to participate in the pilot test and a link to the translated, altered (according to the pre-test) Bricolage Measure was sent out via email to 475 nurses; 237 nurses accepted and completed the translated Bricolage Measure online. To increase the response rate, two reminders were send out with intervals of two weeks.
Data analysis
Firstly, descriptive statistics were used to describe the demographic characteristics of the study population and the respondents’ answers to the eight items. Secondly, we used the responses of the pilot test to determine how the nurses rated their own and colleagues’ bricolage activity, by re-coding the response categories connected to each item and afterwards gathering all the responses from the nurses in a sum index. The response categories ‘never’, ‘rarely’, ‘sometimes’, ‘often’ and ‘always’ carried the points 1, 2, 3, 4 and 5, and the sum index was constructed based on these numbers. ‘Don’t know’ and ‘refused to answer’ were allocated to 0 points and thus were not included in the analysis (n = 108). Additionally, the sum index was gathered in a new variable, where the sums of points were divided into five response categories to illustrate the distribution of all the nurses’ responses. The lowest score possible after answering the eight items in the Bricolage Measure is 8 and the highest score possible is 40 thus the range of scores is 32. The possible 32 points were divided into five equal-sized groups followed by a calculation of how many respondents ended in each group. Thirdly, a Cronbach’s alpha was calculated to evaluate the internal consistency reliability of the measure. All statistics were performed using IBM SPSS statistics 22. 18
Ethical considerations for pre-test and pilot test
The participants in the pre-test were only known by the interviewer and they were promised full anonymity. Also, they could at any point withdraw from the study without giving any reason. In the invitation to the pilot test there was a link to the questionnaire and the participants could therefore not be identified by their responses. Permission from the Danish Data Protection Agency is not required to interview or send out questionnaires as long as informed consent is recieved from all participants. 19
Results
The translation–back translation
The translation from English to Danish did not cause any problems. In a few instances the translator had given some suggestions as to choice of words and the final decisions were made after discussion between the researchers and examination of the literature from Senyard et al.8,13 and Baker and Nelson 4 to ensure coherence with the original Bricolage Measure. The back translation resembled the original English version with only minor differences. The English version of the Bricolage Measure appears in Table 1 and the Danish version can be seen in Appendix 1 (see Supplementary online material).
The pre-test
Face validity
The analysis of face validity after the first six interviews in the pre-test showed that all six nurses missed a definition of the following words: we, resources, challenges, problems and opportunities. Another problem addressed by respectively five and three nurses, was two words placed in two different items that according to the nurses seemed confusing. The first word was ‘gladly’, from item number 2, used in the sentence: ‘We gladly take on a broader range of challenges than others with our resources would be able to’. The second word was ‘surprising’, from item number 6, used in the sentence: ‘By combining our resources we take on a surprising variety of new challenges’. The Bricolage Measure and all eight items can be seen in Table 1.
In order to resolve the missing called-for definitions, an introduction was created after an examination of the original Bricolage Measure introduction. The new introduction was created by making a translation of the original Bricolage Measure introduction and making slight adaptations to specifically address nurses and to incorporate patients as an example of a resource available in the process of solving problems. The second problem with the two words was solved by discussing the words with the creators of the original Bricolage Measure. The first word, ‘gladly’, was changed to ‘without hesitation’. The other word, ‘surprising’, was changed to ‘greater … than others would think possible’. In the second round of the pre-test the definition was subsequently understood and the altered words were not mentioned as problematic by any of the nurses.
Another point mentioned by seven out of the 11 nurses interviewed was the academic wording of the questionnaire. The nurses described that the questionnaire required a great deal of concentration and more time to answer than one would expect of a relatively short questionnaire, but, nevertheless, the measure was understandable and doable because it only consisted of eight items. It was not possible to make the sounding of the questionnaire less academic, because it would mean that the semantic equivalence could not be preserved. Therefore, the academic wording was accepted with reservations as to how the further analysis of content validity would manifest itself.
Content validity
The result from the analysis of content validity of the translated Bricolage Measure.
Baker T and Nelson RE. Creating something from nothing: resource construction through entrepreneurial bricolage. Adm Sci Q 2005; 50(3): 329–366.
Senyard J, Baker T and Davidsson P. Entrepreneurial bricolage: towards systematic empirical testing. Front Entrepreneurship Res 2009; 29(5): 1–14.
Senyard J, Baker T, Steffens P, et al. Bricolage as a path to innovativeness for resource-constrained new firms. J Prod Innovat Manag 2014; 31(2): 211–230.
The pilot test
The pilot test reached a response rate of 49.9% corresponding to 237 replies out of the 475 invitations sent out. The majority of respondents were from the Danish geographical regions Zealand (53.6%) and Jutland (37.5%), with a minority from Funen (8.9%). This geographical dispersion is in line with the number of workplaces and number of people living in these different parts of Denmark. Almost all of the respondents were women (98.7%) and almost half (46%) had more than 10 years of experience as a nurse. The majority of respondents (55.7%) were between 26 and 40 years of age. A minor number of the respondents had management experience (16%) and a few (3%) did not have contact with patients in their daily work.
The Bricolage Measure was answered by 237 nurses who for each of the eight items had chosen one response category they thought relevant, thus we have 1896 answers chosen. In Table 1 it is possible to see the distribution of all the 237 respondents’ 1896 answers. The most common response category chosen was ‘often’, but in items 2, 4 and 8 there were a somewhat greater number of respondents who selected the response category ‘sometimes’ compared to the other items. Of the 1896 answers, only 108 were chosen from the response categories ‘don’t know’ and ‘refused to answer’.
The summed index presenting the distribution of bricolage activity among the nurses participating in the pilot test is illustrated in Figure 1. More than half of the nurses (56.1%) and 15.2% of the nurses respectively reported that bricolage activity occurred ‘often’ or ‘always’ while 1.3%, 3.0% and 24.5%, respectively self-reported bricolage activity as occurring ‘never’, ‘rarely’ or ‘sometimes’.
The self-reported sum index of bricolage activity among 237 Danish nurses.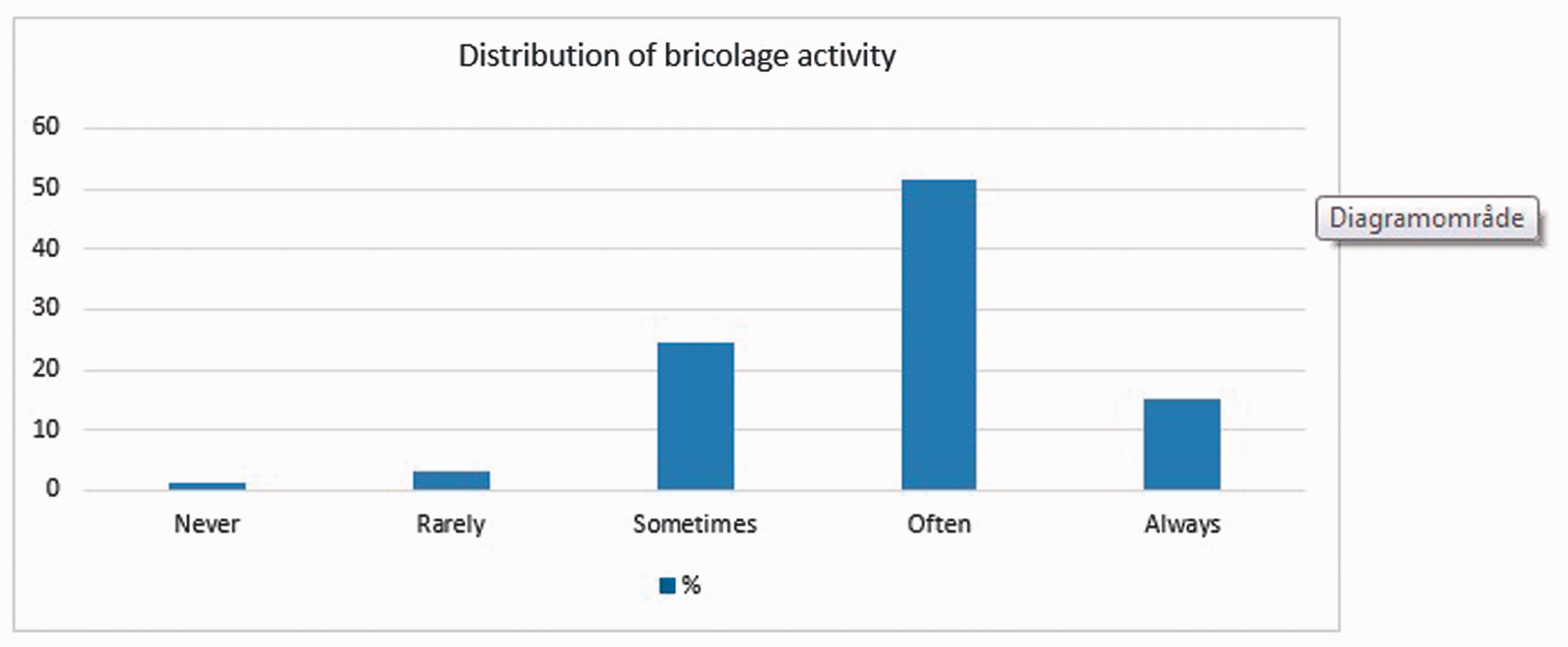
The result of The Cronbach’s alpha was 0.704.
Discussion and limitations
It is important to understand how innovation occurs in health services with limited resources in order to promote innovative ideas and problem-solving activities. Various qualitative studies have shown how bricolage activities can be a path to change and innovation in health services with resource constraints. If these results could be quantitatively confirmed among nurses, it could be an incentive for using bricolage as an approach to promote nursing innovation.
The translated Bricolage Measure showed a high degree of face and content validity when tested in a nursing context in Denmark. Additionally the pilot test revealed that the nurses who completed the translated Bricolage Measure rated themselves and colleagues as displaying high levels of bricolage behavior, underlining the importance of continuing the validity analysis of the Bricolage Measure in order to further validate the tool for use in nursing and to explore bricolage activity among nurses and be able to identify its role in innovation.
The translation–back translation
With the use of the translation–back translation method, the Danish translation of the Bricolage Measure was shown to be equivalent to the original questionnaire. However, it could be considered a limitation that only two translators were involved. Wild et al. suggest the use of a minimum of two translators, 20 preferably more, to obtain a valid translation because as more translators are involved, the margin for error will decrease. Nonetheless, in the present study the original Bricolage Measure was in English, which is fluently spoken by the researchers who could point to any possible mistakes.
The pre-test
The pre-test and subsequent analysis of face validity showed that the problems related to the immediate understanding of words and sentences could be solved in cooperation with the makers of the original Bricolage Measure with the exception of the academic wording. A supplemental calculation to assess the readability of the translated questionnaire by the Flesch-Kincaid Grade Level revealed a text suitable for 11th grade (http://www.readabilityformulas.com/freetests/six-readability-formulas.php) which points to the fact that the questionnaire is relatively demanding to read, thus corresponding to the experience of the nurses interviewed. Even though the academic wording may have made the items more difficult to understand, the analysis of face and content validity indicated that the nurses understood the intended meaning of the questionnaire in accordance with the theory of Baker and Nelson. 4 The nurses’ only reservation was that it was important to have the necessary time to answer the questionnaire. In the future it is therefore essential to keep the setting of when and where in mind when using the translated questionnaire.
The pilot test
The few respondents choosing the categories ‘don’t know’ or ‘refused to answer’ indicated that the nurses understood the items and felt they had appropriate response categories to choose from. Often the lacking responses can be explained by the respondents not understanding the questions or not having relevant response categories available. 21
The Cronbach’s alpha, which was 0.704, is, according to Fayers and Machin, 17 an acceptable result for a measurement with a modest number of items. Even though Cronbach’s alpha preferably are above 0.75 it is important to keep in mind that the higher number of items the higher the Cronbach’s alpha will be and therefor the test of Cronbach’s alpha also must be interpreted with caution. 22 Either way this highlights the importance of further validity measurements to test the construct validity of the measurement when translated and used within nursing.
Using the social media platform Facebook for recruitment of participants meant that the study was not limited by geography and economy. However, Facebook users still belong to a somewhat younger segment of the population, which may have affected the characteristics of study populations in the pilot tests. By choosing every 20th we aimed to achieve a random selection of participants in the pilot test to increase the probability of the study population representing the underlying target population. The comparison of respondents in the pilot test with the general demographic characteristics of nurses in Denmark showed that the study population age was, as expected, younger than thay of the general population of nurses. 23 This means that the validation of the translated Bricolage Measure only may be generalizable to nurses younger than 50 years old.
The study population is reflected in its gender composition with a much larger number of women than men. In the pre-test 90.9% of the participants were women and in the pilot test 98.7% of the respondents were women. This is representative of the general background population of nurses in Denmark of which 96% are women. 24 Considering this, the translation and validations seem to be appropriate for the target population of nurses. On the other hand, if the Bricolage Measure was to be used with other health professionals, i.e. doctors or physiotherapists, with a different representation of gender, new validations might be needed. With 98.7% of the respondents to the questionnaire being women, the pilot test could raise concerns about whether men would also rate themselves high on the Bricolage Measure. More generally, in further research it is pertinent to examine whether there are gender issues in relation to the integration of nurses’ bricolage behavior into innovation activities in the healthcare sector. Previous studies of innovation and bricolage have mostly been gender neutral. 25
Implications for nursing
The proliferation of bricolage among nurses is high according to the nurses’ self-reported responses to the translated Bricolage Measure. This result strengthens the importance of having a measurement like the Bricolage Measure to explore bricolage activity among nurses and to be able to identify its role in innovation. Since responses from the nurses are based on their own perceptions it could be relevant to further confirm these results in e.g. field studies.
This study presented a translated and preliminarily validated Bricolage Measure that if further validated can be used to quantitatively examine the extent of bricolage and therefore provide researchers, managers, policy makers etc. with a unique tool applicable in a population of nurses. The ability to assess the potential of bricolage could be used to plan if and how to use bricolage strategically for legitimate innovation within nursing and to determine where bricolage exists and what characterizes settings with bricolage activity in order to enhance this behavior. Lastly, we also suggest that future research should explore whether there is a solid connection between innovation and bricolage in nursing by using existing innovation measures as well as this preliminarily validated Bricolage Measure.
Conclusion
A translated and preliminarily validated questionnaire available to measure the bricolage activity within nursing in Denmark is now available. The validity analysis consisting of a translation–back translation and a pre-test showed high face and content validity of the translated Danish version among nurses working in primary and secondary sectors in Denmark. Additionally, the pilot test indicated that the Danish nurses rated their own and colleagues’ levels of bricolage activity as being fairly high. This study may be considered as preliminary work in the validation process of the tool to measure bricolage in nursing. Additional construct, criterion, concurrent and divergent validity analyses are needed to make final claims regarding the validity of the tool. However, our study emphasizes the importance of having a tool to uncover bricolage activity in a reliable way and as a possible route to innovation, because there seems to be an unexploited potential.
Footnotes
Acknowledgements
We thank Julienne Senyard, Ted Baker, Paul Steffens and Per Davidson, the makers of the original Bricolage Measure, for ideas and advice during the translation and validation process.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.