
Abstract
This study is based on an issue in nurses’ meal and nutrition care, relating to nurses’ perceptions of transfer of knowledge between different care settings. Through the notion ‘problems of actuality’, the aim is to identify how and why different methods in care may complicate preventive effort related to undernutrition among older adults. It is a qualitative study that lends itself to ethnography and ethnomethodology, with data collected through the use of semi-structured interviews and insights into patients’ medical charts. Through explications of nurses’ methods in meal and nutrition care, and how this work is accomplished within each setting, the study identifies that the different methods involved in meal and nutrition care (defined respectively as social-bodily care and text-based care), create problems in the transfer of knowledge between different care settings. Due to disconnection between social-bodily care work and text-based care work, there is a lack of transfer of knowledge, through which important parts of meal and nutrition care work become invisible. The study finds a need for noticing the disjuncture between social-bodily care and text-based care and for both methods of care, to be recognized as methods that support a delivery of care.
Introduction
The background for this article is that healthcare studies show that undernutrition is a widespread problem among older adults placed in short-term care facilities such as hospitals and rehabilitation centers. Undernutrition is said to be a significant factor in older adults being re-hospitalized,1–3 which is also due to a nutritional decline often occurring during hospitalization.3–5 In Denmark there has been an increased attention towards preventing re-hospitalizations. The Danish Institute for Quality and Accreditation has included frameworks for specifying relevant nutritional efforts, such as the hospital’s responsibility for ensuring that patients at nutritional risk receive the offer of a relevant effort.6–8 Moreover, the Danish Health Authority specifies the importance of follow-up as part of the discharge letter for patients being discharged before nutritional efforts have ended. 9 In a Danish study on nutritional therapy in the transition between hospital and home, a need for taking responsibility for patients who are at nutritional risk both before and at discharge from the hospital is emphasized, due to nurses generally experiencing a lack of information in the transfer of knowledge across different care settings, specifically at discharge. 10 Another study on ‘Good Nutrition Practice’ has found that having nutrition as part of accreditation efforts has had a positive effect on nurses doing nutritional screening, plans and follow-up. But transfer of knowledge at discharge is still a problem. 11 Whether at admission or at discharge, the primary tool for transfer of knowledge between sectors is computer-based. This (text-based) part of healthcare work is made visible in ethnographies. In an ethnography of front-line work in healthcare, Corman and Melon present the idea that there exist: ‘disjunctures between the actual work of these practitioners (what they do), and how what they do is textually mediated and recorded; there are disconnects between patients, texts, and settings, leading to tensions’.12(p.158) They define this as ‘problems of actuality’ existing in nursing work: ‘The system appears to work smoothly as patients are moved through more “efficiently,” but only because more invisible work is done’.12(p.159)
Problems of actuality can furthermore be identified in works such as Timothy Diamond’s ethnography on nursing home care, in which he can be seen to explicate this disjuncture by saying that the process of getting to know patients through charts is to gain knowledge of medical terms, because care work is invisible and is written out of the charts. 13 Leigh-Star and Strauss’ point to, ‘how nurses, who are very visible as workers in the health care setting, are struggling to construct an arena of voice to make their work visible’,14(p.15) in relation to transferring their knowledge across settings. This transfer calls for visibility, since it involves changes in care hands and settings. Such insights have resulted in different tools for creating continuity of care in healthcare transitions, such as checklists for continuity of care, 15 checklists for patient transition information, 16 a transitional care model, 17 and a discharge checklist. 18 These studies provide detailed and elaborated information on how to successfully transfer patients between sectors in a text-based manner, though often not including a plan for meal and nutrition care (or giving only a cursory plan). Research is attentive towards problems in the transfer of knowledge. What the studies do not fully investigate is the fact that, if knowledge is not shared, it is made invisible and thus knowledge is kept in the single institution. This is referred to in transition theory as practice settings operating as ‘silos’ without knowledge of the problems addressed in the previous setting.17–21
The background knowledge presented shows problems of undernutrition, possible challenges, but also solutions to creating continuity of care for the underweight older adult. Thus, this article works from the assumption that an important part of initiating nutritional efforts when receiving an underweight older adult at a hospital or for rehabilitation, is that the transition involves a transfer of sufficient knowledge about problematics addressed during care treatments. From this the article follows an understanding of knowledge sharing that supports both the formal and the visible parts of care occurring through the use of standard forms in text-based care, and the more informal and narrative, 22 occurring through social-bodily care work, that tend to become the more invisible part of meal and nutrition care. This makes ‘problems of actuality’ 12 the major focus in this article. Taking its starting point in nurses’ perception of transfer of knowledge about meals and nutrition between different care settings (throughout the article the term ‘knowledge’ represents both textual and social-bodily care actions and communication), the aim is to identify how and why social-bodily care versus text-based care, may cause problems of actuality in creating healthy meal and nutrition care transitions.
Methods
The study upon which this article is based is a dataset consisting of data from 22 semi-structured interviews with 20 nurses and nurses’ assistants, two managers, and insights into 50 patients’ medical charts in order to gain insights into the tension between social-bodily care reflections in the interviews and the text-based expression of care in journals.
Sites and informants
The data were collected from two sites: a geriatric department at a hospital and a rehabilitation center in the Region of Copenhagen. Both sites primarily had older adults (65 + years) admitted to the unit. In this study, both sites are considered short-term institutions, based on both institutions having a significant number of patients or residents in transition. The participating nurses were both nurses and assistant nurses, ranging from 35–60 years of age. All nurses had at least three years of experience, but most had more than ten years. Thus, the author considered the nurses to be experienced, knowledgeable and competent members within their field. None of the nurses had any specific training in nutrition other than that during education and one or two one-day seminars within the institution.
Interview and process of transcribing
The interviews were developed with inspiration from James Spradley’s approach to conducting ethnographic interviews, with a specific focus on his notion of using descriptive questions, which is considered especially useful for starting conversations and keeping the informants talking. 23 The interview approach was additionally inspired by ethnomethodology, developing accounts of how knowledge about each patient emerged from the different methods in nurses’ meal and nutrition care work.24–28 The overall themes for the interviews followed the processes regarding meal and nutrition from admission to discharge when caring for underweight older adults. The interviews took place during two periods: November to December 2013 and October to December 2014. No nurses declined to participate in the interviews and permission to do the interviews within the informants’ work schedule was granted by management. The selection of nurses and nurse assistants can be termed coincidental, since there was no pre-structured expectation about the nurses in relation to the topic. The interviews were 45–65 minutes in length. The interviews were audiotaped, with notes on the side. There were not too many notes, but small reminders to return to a subject. The cited data is translated from Danish into English by the researcher, and all names are pseudonyms. The interviews were transcribed using the transcription tool Express Scribe. 29
The transcribed data consist of a combination of meaning condensation and fully transcribed paragraphs. This combination was done with the aim of increasing the possibility both of reporting subjects’ accounts into readable stories30(p.5) and of thematically analyzing 31 the naturally occurring themes that developed from focusing on the paths from admission to discharge in both settings.
Medical charts
The collection of medical charts took place from September to December 2015 in primary healthcare at the rehabilitation center. The researcher personally contacted each resident staying at the facility, bringing an information letter and asking for signed permission to assess nutritional information communicated between sectors. Thus, consent was collected personally at the institution. For this reason, no consent was needed from the National Committee of Health Research Ethics. Fifty permissions were collected, but due to two social security numbers not working and two residents’ charts failing to appear due to technical problems in the system, only 46 charts are included in the study.
Analysis
The overall themes in this article are the outcome of a processual analysis inspired by ethnomethodology,24,25 that aims to exemplify how work is accomplished within the setting in which it was performed, 28 in this case focusing on nurses’ methods in meal and nutrition care. To create a process, data collection and analysis followed the structure of a transition – an entry, a passage and an exit, 32 – which is considered to represent a wholeness in the line of thinking from admission to discharge. The data were read numerous times, following the six steps of thematic analysis by Braun and Clarke: 1) familiarizing yourself with your data, 2) generating initial codes, 3) searching for themes, 4) reviewing themes, 5) defining and naming themes, and 6) producing a report, consisting of analytical narratives that go beyond purely descriptions of the data. 33
Thus, the processual approach created reports of narratives that follow the structure of a transition, through assembling elements in the interviews and medical charts. The reports of narratives created a basis for analyzing ‘problems of actuality’ as a documentary subject, 26 in which issues regarding transferring knowledge between different care sites are documented. Two key concepts from ethnomethodology – accounts and membership 25 – inspired the analysis of ‘problems of actuality’ as the documentary subject. The concepts allow for considering nurses as members of society, 27 who pay attention to the sense-making accomplishments, through accounts of their own and other nurses’ meal and nutrition care actions anywhere. 26 In this process nurses use and rely on a body of practical knowledge, which they assume is shared at least in part with others, 27 and nurses account for themselves as competent members of the category assigned to them and make sense, 26 which in this case is transfer of knowledge related to meal and nutrition care.
The aim of combining thematic analysis and ethnomethodology was to carry out a processual analysis that provided thematic descriptions that depended on the data, reflected the entire dataset, 33 and provided ‘convincing accounts of the methods used by members, to produce and reproduce organization and society’.28(p.134) The medical charts were included to clarify nurses’ experiences of the transfer of knowledge between the different care settings. The charts were schematically mapped based on a search for registrations of weight and nutritional details at admission. Following this, the mapped overview of nutritional information in the medical charts was read numerous times to discover changes in the use of words, abbreviations, and numbers of words. The analysis was supported by notions in institutional ethnography that claim text to be the bridge between the actual and the discursive, 33 in the search for nurses’ accounts and methods in the use of medical charts. All analytical steps aimed at following nurses’ expressions, to create practice-related accounts, more than a theoretically defined account of practice,25,33 with the aim of identifying and discussing problems of actuality.
Results
The results in this article derive from nurses’ perceptions of sharing knowledge of meal and nutrition care from a cross-sector perspective. The findings are recapitulated in two themes, articulating two different perspectives of knowledge: 1) systems creating knowledge, and 2) nurses creating knowledge.
Systems creating knowledge
In healthcare, computer-based systems provide the potential to deliver short and precise text-based care information about nutritional status and to create knowledge, which makes it possible for nurses to follow up on preceding nutritional efforts, due to knowledge being shared between different sites. This exists in both primary healthcare and the hospital. Computer-based systems seem to be a strong tool to ensure nurses’ efficient methods to create knowledge of, for example, existing nutritional issues following a patient. This is a text-based care system that, as part of a medical chart, develops nutritional information for primary healthcare institutions. Figure 1 shows a care plan. This plan provides the basic accounts for the hospital nurses to fill in, which consist of a score on a scale of 1–5 that indicates the severity of a disability.
Example of nurses adding nutrition information in a medical chart; following score.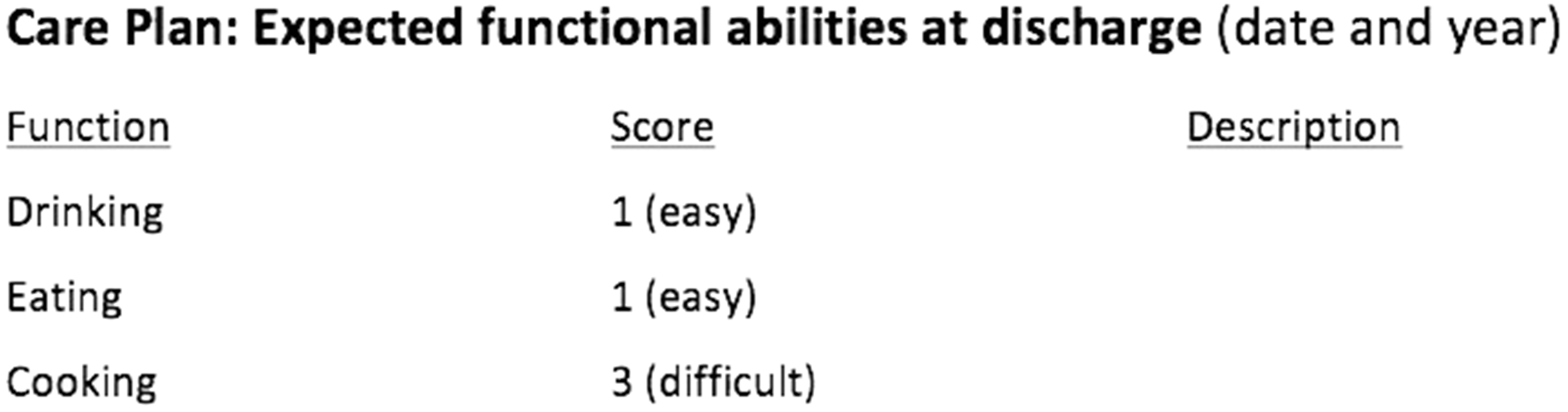
This format is almost identical to the admission report that the hospital receives from primary healthcare. Both are based on a number scale on which 1 to 5 indicates a patient’s functional abilities related to eating, drinking and cooking. The higher the score in the medical chart, the more a nutritional effort is needed. The number on the scale is filled in based on nurses’ assessment of patients’ functional abilities related to drinking, eating and cooking their own meals. As Figure 2 shows, the accounts in the assessment on nutrition in the care plan differ.
Example of nurses adding nutrition information in a medical chart; following score and description.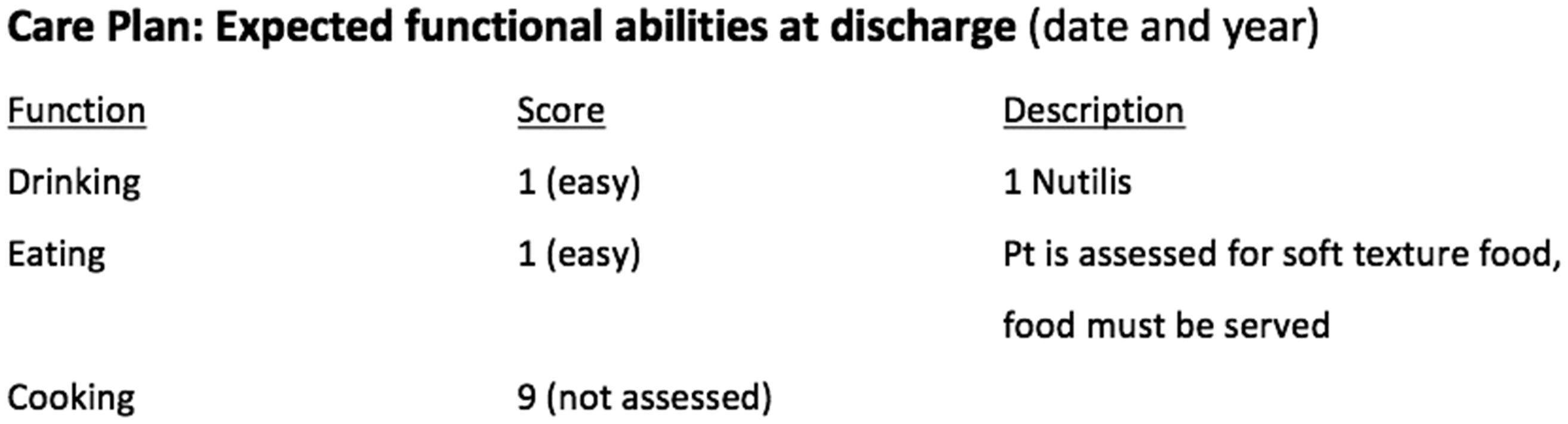
The information passed between sites can be the result of nurses exclusively using the number scale, as shown in Figure 1, or nurses adding elaborated nutritional details, as shown in Figure 2. In both Figure 1 and Figure 2 the accounts of knowledge are based on the same numbers, but in Figure 2, the nurses have considered a need for a written assessment. These written accounts explicate a difference in knowledge between numbers and words. When receiving or sending notions on meals and nutrition, the need for elaborations is based on nurses’ evaluation, and this elaboration furthermore indicates a difference in nurses’ perceptions of what competent membership is, and how practical knowledge is or should be shared, which creates a great amount of inconsistency in meal and nutrition care: … with a brain damage there may be an assessment of chewing-sinking problems. But else no knowledge about nutrition is received. Nothing. I do not experience that. In medical charts there is a number, it says almost nothing … You can say … The electronical documentation form from the hospital. The medical chart. It does not prepare for detailed notions. You are scored, you get some numbers on you. And then we … It is a way of making aware of a problematic, and then we go in and identify what it is. It is a picture. It is a kind of screening. No words necessarily are part of it. (Manager, Rehabilitation center) It is just not always that we receive it [the admission report] before the patient arrives. I think it has something to do with the system, that you cannot always easily talk to each other. But in the admission report it does not say how much they weigh. It does not say how tall they are, and it does not always say something about what they eat. (Nurse, Hospital) It often tells whether they can eat or something. Something with their physical abilities. But sometimes it also says if they lost weight through a shorter period of time (for being able to treat, it cannot be used). Then I use my own observations too. How does the resident look? Usually read the physical ability assessment. What is it that I am going to do? Do they need help to get the food, and what would they want? (Nurse, Rehabilitation center)
Nurses creating knowledge
When adding descriptions and not just a score in the medical chart, more knowledge is shared. Following a score create a lack of information, which is a subject that takes up nurses’ attention. A nurse explains the experience of opening an admission report from primary healthcare in the following way: … then when you open them it is this … a contact for an administrative worker in the municipality, phone numbers for peers, and then there is not much more of relevance for us. Then there is something about ‘receives help an average of 30 minutes each day’, something with medicine doses. It is written a little bit in cues. It is of no use for us. I would ten times rather ask the patient if it is relevant, and get an honest answer. (Nurse, Hospital)
Though nurses at the rehabilitation center express an improvement in the accounts of knowledge through the use of computer-based systems, an admission interview is a necessity on both sites. Due to the Danish accreditation program, it is a nursing responsibility to gather information through an admission interview, and the lack of relevant information and ciphered language also make the admission interview relevant for the nurses to conduct, but in many ways it also makes the use of the system irrelevant: We know we have to do our care plans and we can do that without looking at an admission report. (Nurse, Hospital) In the care plan at discharge there are different sections where you assess functional abilities and there is also nutrition (…) there is no limitations to the amount of information you can write. And I also think that the more we write, the more detailed the care plan is also in relation to nutrition, the more use of it they have in the municipality. And that is also what they say. (Nurse 9, Hospital) We could easily be better, because a lot of times you have talked to the patient, you have their weight, you have a lot of things started, but just not documented. You document whether they can walk or stand and the patient now is fully treated, so now they leave. (Nurse, Hospital)
Discussion
Nurses’ accounts of transfer of knowledge across different care settings related to meal and nutrition care, are seen to confirm that problems of actuality exist, due to a division between the social-bodily care work and the text-based care work that nurses deliver. This will be discussed in what follows.
Social-bodily care work
Nurses follow the methods that allow them to accomplish meal and nutrition activities. 28 In ethnomethodology members are active creators. 25 Thus, by considering nurses as members, the nurses become active creators of meal and nutrition care. Nurses’ methods in meal and nutrition care continuously constitutes and reproduces the practice of sharing knowledge about meals and nutrition within this disjuncture. In repeatedly experiencing a lack of knowledge, and what seems to be a lack of trust in the system-based work, nurses method for handling care is to stick to what they consider as care work. Thus, observation, judgement and social engagement, rather than gaining or transferring knowledge through the medical charts, are nurses’ primary approaches to meal and nutrition care. This in many ways continues to make the computer-based systems an invisible part of care, due to the actual meal and nutrition methods that nurses use and from which they gain patient knowledge substantially differing from the methods that nurses use in text-based care. According to Corman and Melon, these are two distinct and often contradictory ways of getting to know patients – as real people with bodily needs and as text-based objects of professional attention – which represent and result in two kinds of caregiving. 12 One is formal caregiving, written and shared by professionals and administrators, that of a recording task that fits the organizational scheme. The other form of caregiving, which is submerged, unwritten, and shared by the people who live and work on the floors, 13 is that of invisible care work, which is written out of the charts, not considering to whom work should be visible. 14 This also results in nurses performing social-bodily care, which creates knowledge and membership within the single institution.25–28 But considered invisible, knowledge and practice of membership then stay within the institution, due to a lack of sharing. Thus, the performance of competent membership related to transfer of knowledge of meal and nutrition care needs to be both within, and connected with other institutions in healthcare, to be fully competent.
If nurses’ efforts and knowledge in meal and nutrition care are not shared, this points towards a problem in continuity of care that relates to what is referred to in transition theory as ‘working in silos’.18–21 When considering working in silos as part of the problems of actuality, a frame for discussing transfer of knowledge across different care settings is created. It is a frame in which competent membership is more than the passing of a patient from one healthcare setting to another. Thus, a patient is not just discharged when discharged. In his ethnography on nursing home care, Timothy Diamond identifies the older institutionalized adult as moving through a series of situations. 13 If transition is understood as a concept of change, 32 the transition of the undernourished older adult should include sharing the changes that are identified and occur during treatment. This is not always present in nurses’ transfer of knowledge relating to meals and nutrition. In a transition theoretical understanding, patients or residents move from well to sick (and back) until a certain level of stability is reached. 32 The role of the nurse in this process must be to share the level of stability of a patient’s nutritional status. But a stable nutritional status is not a part of a hospitalization completion; therefore, meal and nutrition accomplishments towards improving a negative nutritional status may not be fully completed, and thus become a challenge in text-based care.
Text-based care work
Computer-based systems are a primary way of communicating between sites, and text-based work objects such as medical charts have become a norm in nursing, 22 and a dominating way for nurses to construct and share their knowledge about meals and nutrition.34,35 In institutional ethnography a medical chart could be considered a so-called ‘ruling relation’, which is a kind of textual regulation that stand opposite to what nurses consider care work. 33 In healthcare there is a problem of text-based care producing a high level of extractions of meal and nutrition efforts, rather than a reflection of efforts that have taken place. 13 While nurses can be heard expressing ‘cues’, the extractions can be considered to deliver limited information that nurses seem to consider while creating limited meal and nutrition knowledge upon which to act. Furthermore, there does not seem to exist a common understanding – a membership between sites – that enhances and supports notions of sharing and making visible. Extractions or cues in medical charts conceal as much as they reveal. 13 This is due to filling in a text said to objectify knowledge, and text that appears objective is based on limited information, 12 pushing aside the narrative and more elaborated part of nursing 22 and increasing the invisibility of meal and nutrition care. Problems of actuality exist, in spite of text-based care possessing the potential to improve the transfer of knowledge between actors in different social worlds, 34 due to the possibility of the same words and images presenting different places at different times. 35 Medical charts are transition work objects that possess the potential to share knowledge. But charts moreover have the power to determine what is considered knowledge for caregiving, when a condition is present, and seem to become the protocol of which many nurses think, 12 that also neglects the fact that we know more than we say, due to learning occuring through social processes and not instructions. 34 Another challenge may be that text-based care work may be considered an unskilled task 13 that, even as extractions, is expected to be understood by the receiving party. 34 Nursing skills are based on the social-bodily form of care, not the text-based. Nurses have no or only little training in text-based care, but are expected to know how to do nutrition registration and to have a unified way of doing it, which means that they produce the same kind of knowledge.
Conclusion
The subject matter of this article is not whether nurses do or read medical charts or not, but rather to create awareness of the need for unifying matters of social-bodily care and text-based care forms in healthcare. A disjuncture between nurses’ actual work and the textually mediated (problems of actuality) seem to be accepted as a condition in nursing. Text-based care may follow the rules of the institution, but it is also sharing knowledge between different care settings, for ensuring continuity of care. Nurses’ observations, judgment and social engagement is where knowledge is stored. There is a need for nurses to share their stored social-bodily knowledge in a textual manner. Thus, when developing and introducing text-based care forms, these should meet and include the more informal and narrative methods in social-bodily care forms, and not take for granted that competent membership can be exercised.
Footnotes
Ethical approval
The study was approved by the hospital and the transition care facility. Residents at the transition care facility gave written informed consent for medical charts to be collected.
Author contributions
Study design LHK; data collection LHK; data analysis LHK; drafting of manuscript LHK, MWH and AMB; critical revision MWH, AMB and NHK; supervision MWH, AMB and NHK.
Acknowledgements
The authors wish to thank all of the participants who openly engaged and shared their knowledge and experiences.
Funding
The study was funded by Aalborg University and BDO Consulting. The views expressed are those of the authors and developed independently, with no requirements from BDO Consulting.
Conflict of interest
The authors declare that there is no conflict of interest.