
Abstract
Older patients quite often arrive in an emergency department (ED) with a family member, but little is known about the family member’s health evaluated in ED. The aim of this study was to describe family health in EDs evaluated by family members and nurses. Data were collected from Estonian hospital EDs from 111 family members of older patients and from 93 nurses. Family health in EDs was evaluated as being at a moderate level. Family members reported that family health was better when older patients lived with the family. The more time the family spent in the ED, the worse the health-related activities were. Nurses reported that cardiovascular problems in older patients who presented in EDs disturbed the values of family health. We conclude that ED nurses should recognize the level of family health, in order to ensure that the family will be able to cope at home. Family health in EDs should be reviewed over time to help nurses meet the required needs of the family.
Background
Older patients in emergency departments
Older patients (≥65 years) often visit emergency departments (EDs)1,2 due to the following conditions: cardiovascular problems; musculoskeletal conditions; intestinal disorders; adverse drug reactions; neurological, respiratory, and dermatological conditions; accidents; mental-health problems. 3 In 2014, 79,854 patients visited one ED in an Estonian regional hospital, on average about 218 patients per day, and over 60% of them were older. 4 Paavilainen et al. found that nearly half of adult respondents (42%) arrived in the ED with a family member such as spouse/partner, person with whom they lived, or child. 5 In the present study, a family member was defined as someone accompanying an older patient to the ED. Family members may also care for older patients after they have been discharged home. 6 Previous studies describing family health have focused mainly on the children and parents, and especially on the interaction either in parent–child relationships 7 or in respect to mental health and related behaviors.8,9 Any stressful situation can influence human wellbeing and affect the whole family’s life. 10
Family health within healthcare settings
The definition of the term ‘family’ differs; in sociology it denotes ‘groups of people living together’; in psychology it means ‘groups with strong emotional ties’.11(p.7) The term ‘family health’ frequently equates to ‘family functioning’.11(p.5) Family health may be affected by one family member’s health condition. Family perspective denotes the collective view of the family’s health situation over time and through interaction with its members. 12 Here, the term ‘family health’ refers to ordinary family issues such as values, wellbeing, knowledge, ill-being, and activities as main components of family health.13,14
Health-related values consist of family beliefs, rights, atmosphere of peace, personal growth and feelings of safety, feelings of being a whole, humor, a person’s connection to his or her surroundings, and self-knowledge. 14 When healthcare professionals work with families, they need to know a family’s values and its culture; then healthcare staff become a crucial support to the whole family, creating reciprocal trust, friendship, energy, and pleasure in the family. 15
Wellbeing is related to satisfaction, strengths, and alertness. 14 In a neurological setting, family caregivers reported good psychological wellbeing if they provided more assistance to less depressed stroke survivors with better cognitive functioning. 16
Ill-being could refer to feelings. 14 In a study by Hakio et al., respondents reported that they were in quite good health, but experienced having feelings of ill-being. 17
Health-related knowledge involves issues related to one’s own health and that of a close relative/friend, health matters, potential answers with feasible solutions, and where help can be obtained. 14 Visits to the hospital by family members of patients with prostate cancer were associated with health-related knowledge. 18 Adler et al. point out nine categories of family knowledge needs: knowledge about the health condition, related care management, daily care, necessary contribution, future issues, how to explain the illness to others, required devices, facilities, organizational matters, and how the illness affects the family. 19 The family members of older patients who visited EDs noted the need for clear communication, family members’ role in ED care, how older patients were treated in the healthcare system, and the appropriate ability to provide specific care during the ED visit. 20 Furthermore, health-related activities that emerged included functional capability, self-care, significant performance, and a claim that the person is in good health. 14 Family members who took part in associated activities experienced better physical health status and comprehensive knowledge. 17
Only a few studies have been found that describe ED nurses’ points of view with regard to older patients and their family care. In one study, conducted within the home, nurses pointed out that families are important for the patient both physically and mentally, by staying together, being aware of related issues, and hearing each other. 21 Respect for older patients and their families is important. 22 Emergency department nurses claimed that lack of information and poor communication provided insufficient support in decision-making and predicted how well or badly older patients fitted into the hospital environment. 22 Emergency medicine requires professional staff who can see a patient’s bigger clinical picture in order to be prepared for managing critical conditions and situations. 23
There is not enough scientific evidence about family health of older patients experienced in ED settings. However, it is critical to gain a better understanding of family health of those families whose older members are discharged home. Families have great role to play in older patients’ after-care.
Aim of the study
The aim of the study was to describe family health in EDs evaluated by family members and nurses. The following research questions were set out:
How do family members describe family health in the ED? How do nurses describe family health in the ED? How does the family health described by family members differ from that described by nurses?
Methods
Instrument
Family Functioning, Health and Social Support (FAFHES) instrument in an emergency department setting.
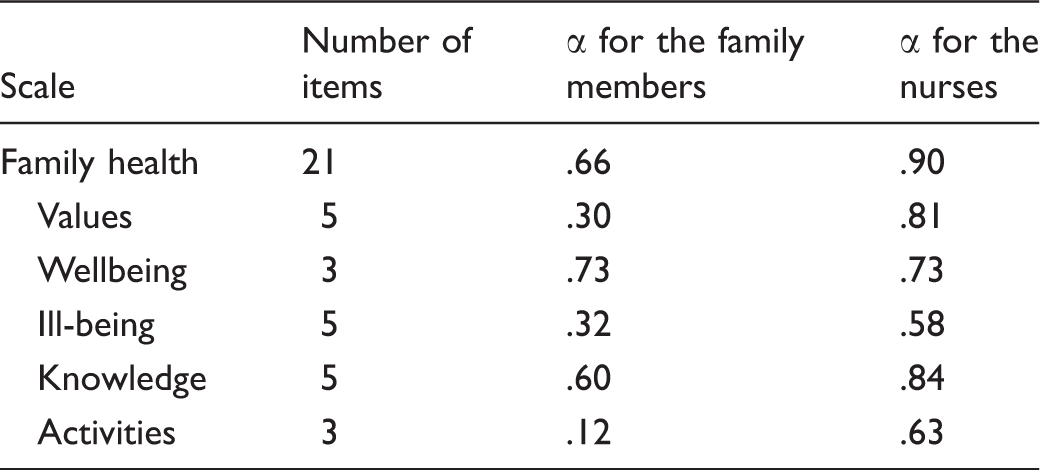
α = Cronbach’s alpha
The background variables of family members included demographic characteristics such as age, gender, marital and social status, level of education, relationship to the older patients (spouse, cohabiting, daughter, son, sister, brother, or other), self-assessment of the health condition at the time of the ED visit, and hours spent in the ED. In addition, family members were asked to describe demographic characteristics of older patients, whether they had needed help in daily life before their ED visit, health problems, week day of the ED visit, type of transportation to ED, and previous visits to the ED because of the same health problem. There were seven items in the demographic part of the questionnaire measuring functional status of older patients at discharge, using a published instrument from Rowland et al. 25 Respondents were asked to circle the appropriate option ‘yes/no’. It was revealed from the pilot study that nurses should have the opportunity to answer also at a neutral level. Family members and nurses were asked to consider whether older patients needed help with their mobility, if they could collect their own pensions or do their own shopping, and whether they received meals on wheels, attended day centers or hospital day units, received home help, and/or could not dress themselves in the ED.
The demographic characteristics of the nurses included age, gender, marital status, highest professional education, and their work experience in healthcare, emergency medicine, and the current ED where the data were collected. Nurses were asked to specify the number of nurses working in their ED and the number of older patients visiting the ED during one shift, the reasons for visits, and the day of the week when most of the older patients came, the time that family members spent in the ED, and the type of transport older patients used to arrive at the ED. To come up with relevant experiences related to family health, each nurse was asked to think about the most recent older patient (and his or her family) the nurse had met and taken care of in the ED.
Sample and data collection
A total of 367 questionnaires for family members and 144 for nurses were distributed to EDs in two regional and two central Estonian hospitals. Regional hospitals are the top main healthcare providers in a country of about 1,325,000 inhabitants. There is extended specialist care, compared with central hospitals, and medical care is offered in all the specialist fields except ophthalmology and obstetrics. In central hospitals fewer specialists and services are provided. In Estonia around 30% of the population speak Russian as their mother tongue.26,27 Most of the Russian-speaking population live in the eastern part of Estonia. One central hospital situated in the eastern part of the country participated in the study.
Data were collected from February to June 2014. First, questionnaires were distributed to family members of older patients who had been discharged home by ED nurses or the researcher. The latter spent 141 hours delivering the questionnaires. In the present study, a family member was defined as someone accompanying an older patient to the ED. The questionnaires were sealed inside envelopes. Family members were asked to send the completed questionnaire back to the researcher by post within 14 days of discharge. They were asked to describe their view on how the family responded to the visit, and their general experience of family health during their ED stay. The family members could choose whether to answer the questionnaire in Estonian or Russian.
After the questionnaires were filled in by family members, nurses were asked to participate in the study. The chief nurse or contact person for each ED informed the researcher of the number of nurses working in the department, as well as the mother tongue of each. Questionnaires were delivered directly to nurses in envelopes by the researcher. Completed questionnaires in sealed envelopes were collected in a special collecting box in the ED. Nurses could choose whether to complete the questionnaire in Estonian or Russian.
A total of 204 responses were returned to the researcher (response rate: family members 30%, nurses 65%). The study sample consisted of family members aged ≥18 years (n = 111) of older patients (≥65 years), who were discharged from the ED to home care, and of nurses (n = 93).
Ethical considerations
Permission to use the FAFHES instrument was received from all its authors. 14 Written permission to conduct the research was obtained from the Tallinn Medical Research Ethics Committee (Nr183) and the administrative staff of the participating hospitals. Family members received both written and verbal information related to voluntary-based participation, data protection issues, and confidentiality, and nurses or the researcher invited them to participate in the study. In addition, posters with information related to the study were hung in the waiting rooms of the EDs throughout the data collection period in both Estonian and Russian. Both nurses and family members were informed that they could contact the researcher if they needed to.28 (p.93),29 Administrative and clinical staff meetings were organized, at which the researcher introduced the study’s aim and data collection process. In every department a contact person had agreed to be available and could be contacted if necessary. Anonymity of respondents was guaranteed.
Data analysis
Descriptive statistics were used for synthesis and summary of the data.28(p.389) Some background factors for both family members and nurses were gathered. The age of family members was grouped as follows: 18–29 years, 30–50 years, 51–64 years, 65–74 years; however, the age of older patients was put into two groups of 65–74 years and ≥75 years. Marital status was either ‘married’ (married, cohabiting) or ‘single’ (not married, divorced, widowed). Education was divided into two groups of university and school. Social status was grouped as ‘working’ and ‘other’ (studying, retired). Relationships to the older patients were modified into three groups: ‘spouse’, ‘child’ (son, daughter), and ‘other’ (brother, sister, friend, friend of the family, relative). Health condition was allocated to one of two groups: poor and rather poor were merged into ‘poor’, and rather good and good were merged into ‘good’. No one answered at a neutral level ‘not good/not poor’. The time spent in the ED, defined as time from patient admission to time the patient leaves the ED, was gathered from four into two groups: ‘<3 hours’ and ‘≥3 hours’.
The day of the week when older patients visited the ED was modified to ‘weekday’ and ‘other’. Transport used by the older person to arrive at the unit was grouped as ‘ambulance service’ and ‘other’ (own transport, taxi, with help of relatives, friends). Reasons older patients visited the ED were divided into eight groups through use of content analysis: musculoskeletal, abdominal, cardiovascular, mental health issues, neurological, adverse drug reactions, dermatological, and respiratory. 3 Also reported were concrete health problems, why older patients sought help in the ED, no poor health, or unspecified conditions.
The age of the nurses was grouped: <35 years and ≥35 years. Among the nurses the group ‘married’ consisted of people who lived together (married, cohabiting) and the other group was designated as ‘single’ (not married, divorced, widowed). The highest professional education was modified to ‘registered nurse’ (RN) and the rest were counted as ‘advanced nursing’ (nurse specialist in emergency medicine or intensive care nursing, master of nursing or social sciences). Work experience in healthcare, emergency medicine, and the current ED was grouped: <5 and ≥5 years.
Reasons for ED visits differed for family members and formed seven groups: musculoskeletal, abdominal, cardiovascular, neurological, poor health, respiratory conditions, 3 and ‘other’ (people know that all possible diagnostics can be performed in the ED; do not have transport to go to the family doctor; have difficulties getting an appointment with the family doctor; experience social problems; and/or any disease). The differences were a result of the health conditions presented by the respondents. The day of the week when older patients mostly visited the ED was coded as ‘weekday’ and ‘other’ (all weekdays/does not matter what day of the week; every day, on holidays/public holidays). Time spent in the ED fell into two groups: <3 and ≥3 hours. The transport used by older patients for arrival at the unit was: ‘ambulance service’ and ‘other’ (own transport, taxi, help of relatives; car of his or her son/daughter; came on own; public transport; other transport).
When analyzing functional status, 25 a patient was at risk of ED admission and discharge if the questions elicited four or more positive answers out of seven. The first question involved the FAFHES score and the second the binary variable that indicates, based on the Rowland et al.’s seven questions evaluating functional status, 25 whether there is a risk for readmission. The answers were used for all the participants, so a new binary variable (0 = no risk, 1 = increased risk) from these individual answers was created.
To compare group means Student’s t-test and one-way analysis of variance (ANOVA) were used for normally distributed variables. For between-group comparisons in post hoc analyses Bonferroni correction was used. As the family-health dimensions of wellbeing and ill-being did not meet the assumption of normality, the Mann–Whitney U-test and the Kruskal–Wallis test were used to discover differences or associations. Spearman’s correlation and linear regression were used to find the relationship within explanatory variables. Mean (M) and standard deviation (SD) were used to present data when answering the research questions. To summarize the relationship between two categorical variables, cross-tabulation was used. To estimate the reliability of the summated variables Cronbach’s α was used.28(p.326) The level of statistical significance was set at p < 0.05. Statistical analysis was carried out using the Statistical Package for the Social Sciences (SPSS) version 24.
Results
Participants
Characteristics of family members and older patients.

Characteristics of nurses.
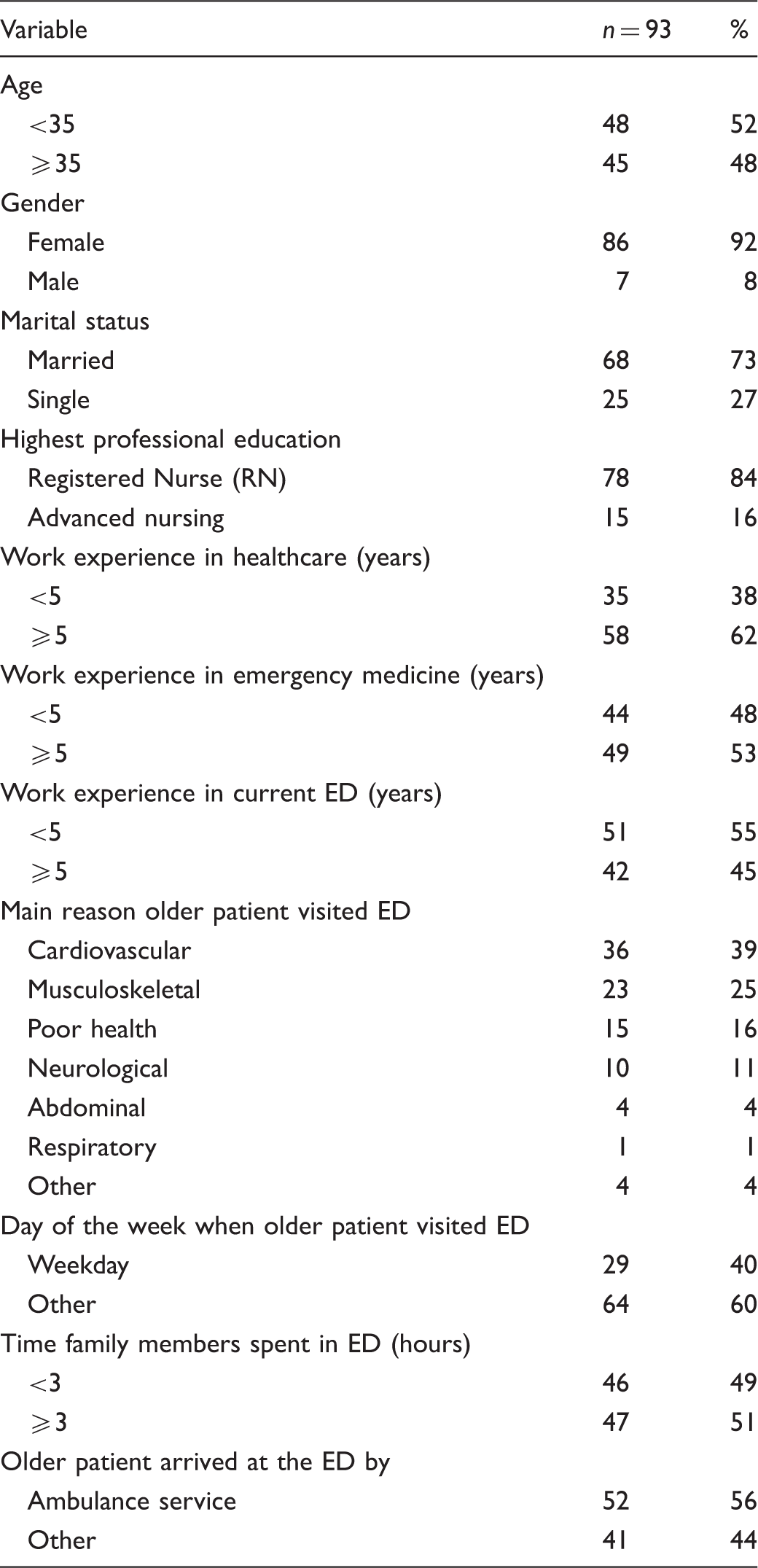
Seventy percent of the family members noted that older patients visited the ED on weekdays, whereas 60% of the nurses reported that there was no preference for any day of the week for these visits, all days being busy. Thirty percent of the family members pointed out that musculoskeletal problems were the reason for seeking help, whereas 39% of the nurses reported that cardiovascular problems were the main presentation in the ED. Forty-one percent of the family members and 27% of nurses found that there was risk of readmission when evaluating functional status at discharge.
Family health described by family members
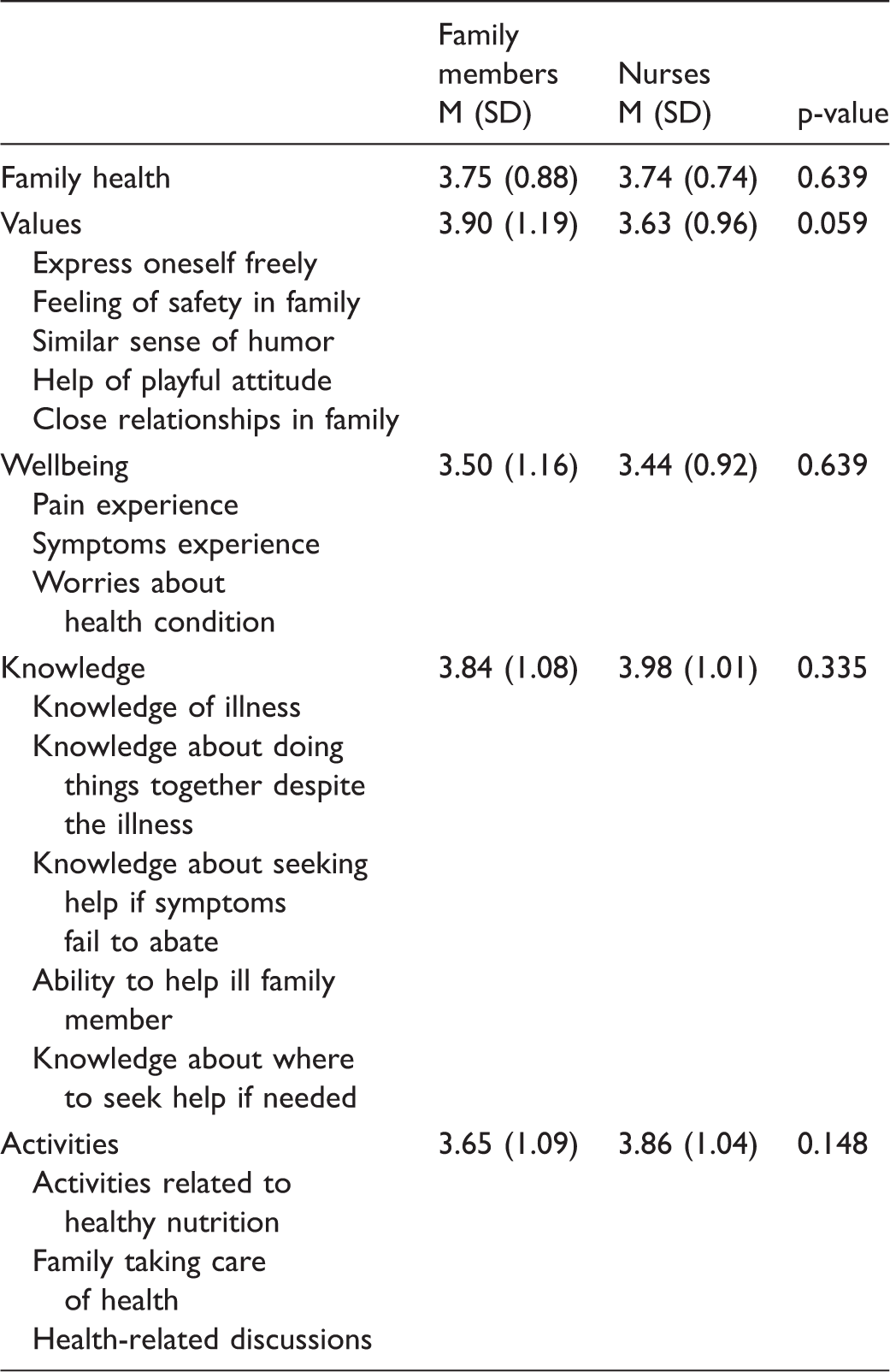
Family health described by family members and nurses.
Background factors of family members and family health.
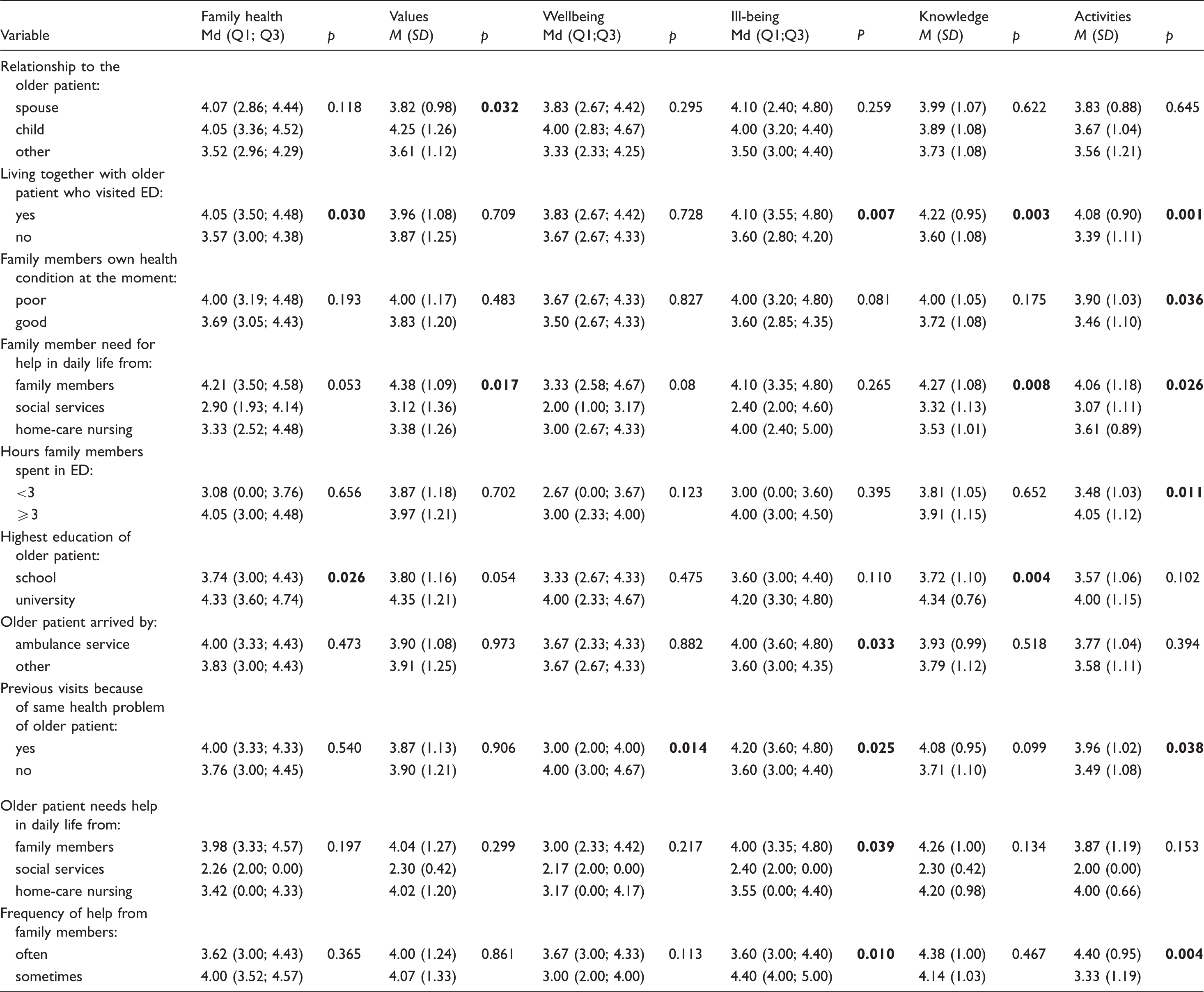
Note. p = p-value. p < 0.05 are shown in bold font.
Health-related knowledge (M = 3.84, SD = 1.08) was reported at the moderate level. There were statistically significant differences between health-related knowledge and living together with the family member (p = 0.007); health-related knowledge and the family member’s need for help in daily life (p = 0.008); health-related knowledge and education of the older patient (p = 0.004) (Table 5).
Health-related activities were at the moderate level (M = 3.65, SD = 1.09). It was found that the time spent by family members in the ED was related to activities within the family. The more time the family members spent in the ED the worse the health-related activities were (p = 0.05). There were differences in health-related activities with regards to living with a family member, poor health condition of a family member, need of a family member for help with daily life, family spending up to three hours in the ED, previous visits to the ED for the same health problem, and frequent need of older patients for help from family members. The variations appear to differ significantly (Table 5).
Family health described by nurses
Nurses reported that family health in EDs was supported at a moderate level (M = 3.74, SD = 0.74). No differences were identified between family health and any background factors. According to the nurses, family values (M = 3.63, SD = 0.96) were supported at a moderate level in EDs. Cardiovascular problems were found to be associated with family values (p = 0.009), which were disrupted when older patients visited an ED with such problems. There were differences between family values and arrival by ambulance of older patients at the ED (p = 0.045).
Wellbeing (M = 3.44, SD = 0.92) was supported by the nurses at a moderate level. The ill-being of the family (M = 3.70, SD = 0.98), health-related knowledge (M = 3.98, SD = 1.01), and activities supported during the ED visit were found to be at a moderate level. Ill-being differed from the need of family members for help with daily life from other family members (p = 0.035), and this difference appeared to be highly significant. No other associations or differences were identified.
According to the opinions of the family members (M = 3.74, SD = 0.74), family health was experienced at the same moderate level as nurses reported. There were no significant differences between the family members’ and the nurses’ ratings (Table 4).
Discussion
This study describes family health evaluated by family members of older patients and rated by nurses in EDs. Of the family members, 58% completed the questionnaire in Russian while only 30% of the Estonian population speak Russian as their mother tongue.26,27 The researcher delivered the questionnaires with no language preference. According to the family members, older patients presented in EDs mostly on weekends or at the start of the week. These findings seem logical because family doctors are unavailable at weekends. It could be problematic to get an appointment with a physician or nurse on the day after the weekend, and older patients tend to have multiple diseases that occasionally get worse for varied reasons. 30 The availability of a family physician and his or her team at weekends and later in the evening on weekdays should be considered when planning primary healthcare.
Families stated that older patients visited EDs because of adverse drug reactions. This may be due to patients not understanding the information given to them by medical staff on discharge or by specialists whom they had visited on the last occasion. Nurses should be convinced that the information shared at discharge is clear enough and acceptable to both the patient and the family. 3 More attention should be paid by nurses to the discharge process, to avoid cyclical readmissions and to prevent the burden of older patients on EDs.
In the present study, 30% of the older patients had visited an ED over the previous 12 months for the same health problem. A literature review shows that unresolved problems in EDs were identified as factors affecting discharge, as well as the social and health problems associated with repeat ED visits. 3 Education at discharge must be improved. 31
Furthermore, family members described family health during an ED stay as being at a moderate level. For older patients who lived with the family, better family health was described. The results confirm statements by sociological scientists, who claim that the family is a group of people living together who depend on each other on the emotional, physical, and economic level.11(p.12) There is evidence that any stressful situation may worsen family health. Close relationships were important for the family. 14
It was found that 84% of the investigated nurses reported their highest education as registered nurse. Only a few had specialized in emergency medicine or critical-care nursing, not to mention master’s studies or an even higher educational level. Educated and trained nursing staff are a valuable resource for quality service in EDs. 32 Callander and Schofield looked at ED workforce models and concluded that senior staffing, matching peak staffing levels with peak patient demand, having appropriately skilled staff mixes, and designing the staff profiles based on individual hospital needs, produce the most effective outcomes. 33
There are about 9000 RNs but only 8% of them are being registered as emergency and critical-care nurses in Estonia. 34 This clearly shows the need for nurses in this area. The admission requirements for specialized training in nursing should be reviewed, allowing more nurses to acquire the necessary competencies.
It appears that both family members and nurses in general described family health as being at the same moderate level. From one perspective it was good that family health was not reported as poor, and families could continue to care for older patients at home. But, from another perspective, to ensure quality of care, a higher level of responses was expected. The FAFHES instrument enabled responses at a higher level. Thus, there is a need for further development of nursing care provided in EDs, to a level where family-health-related issues have more and better support.
It has not been possible to evaluate whether the opinions of family members and nurses matched. Family members who accompanied older patients to EDs, and who are likely to care for the patients after discharge, were involved in the study. Their opinions are important when planning after-care and assessing the readiness of the family to be responsible for older patients.
Methodological considerations
The present study had several strengths. The valid instrument earlier developed was modified for use in ED settings. To the best of our knowledge, the current topic has not been investigated before in the ED context. In the present study we received viewpoints of both family members and ED nurses. However, some limitations were identified. First, data were collected from family members and later from nurses, with no matching of the families. Family members answered from their own points of view, and nurses were asked to think about the most recent older patient and family whom they cared for. Second, data collection in a country where nursing research is not so common is demanding. The researcher involved participants in the study and placed informative posters in the EDs so that all visitors knew about the study being conducted. A larger sample size had been expected. The lowest response rates were found within settings where the researcher was not present when the data were collected.28(p.276),35 In addition to this, the FAFHES instrument had not been used before in ED settings, so further development of the family health scale, especially when used for family members, is needed. There are lower Cronbach’s α values when describing family-related activities of family members; this calls for a modification of the instrument to be more ED specific. Based on the descriptions from the nurses, the family health scale was acceptable at this stage, possibly resulting from the fact that nurses tend to think more largely than family members. In addition, the current findings may result from the fact that most of the nurses who worked in the ED at the moment of data collection were Russian speakers, and for them it was more convenient to communicate with patients and families in their mother tongue when involving families in the study.
It is up to future research to determine whether the questionnaire should undergo additional development to suit ED settings relative to concerned study groups. In addition, more EDs can be involved in the study, not only from regional and central hospitals. There is a lack of literature evaluating family health in EDs and its subareas (values, wellbeing, ill-being, knowledge, activities) related to the present study. Literature from different nursing areas was used in the literature review and possible comparisons, because there are limited numbers of papers describing family health. This complicated the comparison of results.
Knowledge related to family health and support by nurses could improve the quality of nursing care provided in EDs and the discharge process from EDs. It may positively affect further after-care or the environment for coping at home, improve patients’ health outcomes, and reduce costs by preventing unexpected readmissions. Knowledge of family health during an ED stay from the perspective of family members allows more collaboration and exchange of experience across different healthcare teams, which would contribute to ensuring the quality of treatment.
Conclusions
The family members of older patients and ED nurses generally spoke at the same level with regard to family health. The nursing care provided for older patients and their families should be more supportive, by providing all required information to families to enable them to take care of older patients at home. Families have a huge role in continuing the care of older patients after they have been discharged. Emergency department nurses should recognize the level of family health, in order to ensure that the family will cope at home. In addition, attention should be paid to those older patients discharged from the ED after having received medical help, who live alone and need continuing care at home. After-care service providers and the primary healthcare sector should be integrated in this way, to treat this group to a greater extent. It can be assumed that continuity of care and older patients’ health outcomes when they live alone are worse than when living with the family. This may produce readmissions to EDs, overload of ambulance services, and increases in healthcare costs.
Family health and support in EDs need to be reviewed over time. A longitudinal study should be considered to describe the situation in EDs and allow comparison of results over time.
Footnotes
Acknowledgments
We thank the family members and the ED nurses who participated in the present study for their valuable contributions to the research.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors have declared receipt of funding from the following source: University of Tampere, School of Health Sciences.