
Abstract
The diabetic complication macular oedema (DME) is a growing problem worldwide because of the increasing number of patients suffering from diabetes mellitus (DM). DME is treated with injections of anti-vascular endothelial growth factor (anti-VEGF) in the eye. This real-world study aimed to describe patients’ experiences before they received their first injection in the eye. Twenty-one men and women aged 49 to 86 years were interviewed. The interviews were analysed using qualitative content analysis. Two categories and an overall theme ‘to be at a crossroads and a crucial phase in life with an uncertain outcome’ were found. The participants expressed thoughts and concerns at different levels, practical concerns about the treatment procedure, and other existential thoughts regarding hope for improved visual acuity or fear of deterioration. Cooperation between eye clinics and diabetes clinics should be strengthened to clarify who is responsible for providing the information and support required by patients.
Background
Diabetes mellitus (DM) is a lifelong disease 1 and can lead to late complications.2,3 Diabetic macular oedema (DME) is a common late complication that affects the eye and can lead to vision loss.4–7 An increasing number of people are suffering from DM worldwide. 1 Therefore, a large number of people are at risk of suffering vision loss. Vision loss is regarded as the most feared complication by patients 8 and is associated with anxiety and distress. 9 Living with DME and the burden it may cause for the patient can lead to a need for social support. 10 Previous studies have shown that people living with DM and visual impairment have a relatively low level of general health.11,12
Anti-vascular endothelial growth factor (anti-VEGF) injections can improve visual acuity in patients with DME13–18 and they have become standard treatment for DME with visual impairment. 19 This treatment form provides patients with the opportunity and hope to be able to achieve improved visual acuity. Large studies have reported a positive effect of anti-VEGF injections on visual acuity at follow-up.20–23 In current clinical practice, laser treatment for DME is rarely used.
Based on clinical and scientific evidence, treatment options that are considered most relevant are usually injection treatment with anti-VEGF or steroids. Anti-VEGF treatment is provided as an intravitreal injection in the eye under local anaesthesia in an operating theatre. This treatment regimen often comprises three initial monthly injections. 24 Thereafter, the patient is frequently seen at the eye clinic for eye examinations and additional injections are provided if necessary. A previous study in patients who received ocular anti-VEGF injections for wet age-related macular degeneration found that patients feared the treatment procedure itself and further vision loss. 25 Whether these findings also apply to patients with diabetes receiving treatment for sight-threatening DME is unknown.
Patients with visual impairment due to DME are a vulnerable group living with a chronic disease. These patients suffer from a complication that threatens sight and provides challenges for managing daily life. Suffering is a complex phenomenon, which can negatively affect a person’s life in many respects. Eriksson et al. explored the concept of suffering and described it as being where ‘hope and despair meet, and where light and darkness break like waves against each other in the distant horizon where the rays of hope illuminate the way’.26(p.108) Therefore, understanding of patients with visual impairment due to DME is important to be able to provide hope by supporting them in their complex life situation. Qualitative research is used to capture expressive information that is not conveyed by quantitative data about beliefs regarding a particular therapy. However, most previous research on this group of patients has been largely quantitative. Therefore, more qualitative research is needed on this issue 27 to determine the patients’ own perspectives of their situation.
This study is part of a real-world study in Sweden where we have followed a cohort of patients who were diagnosed with visual impairment due to DME starting from baseline before they received their first anti-VEGF injection with ranibizumab.12,28 The participants reported a low level of general health according to two patient-reported measures, the vision-specific National Eye Institute Visual Functioning Questionnaire 25 (NEI VFQ-25) and the generic Short-Form Health Survey 36 (SF-36), before starting treatment. 12 One year after starting treatment, the total group showed improved scores for the NEI VFQ-25 subscales of general health, general vision, and near and distance activities.
After one year, 52% of the patients showed improved visual acuity and in the remaining patients, visual acuity was stable or reduced. The macula swelling was significantly reduced in the total group of patients. 28
This present study aimed to qualitatively describe participants’ thoughts and feelings about treatment, knowledge of the relationship between DM and visual impairment, and if and how visual impairment affects daily life.
Method and participants
Demographic data of respondents.
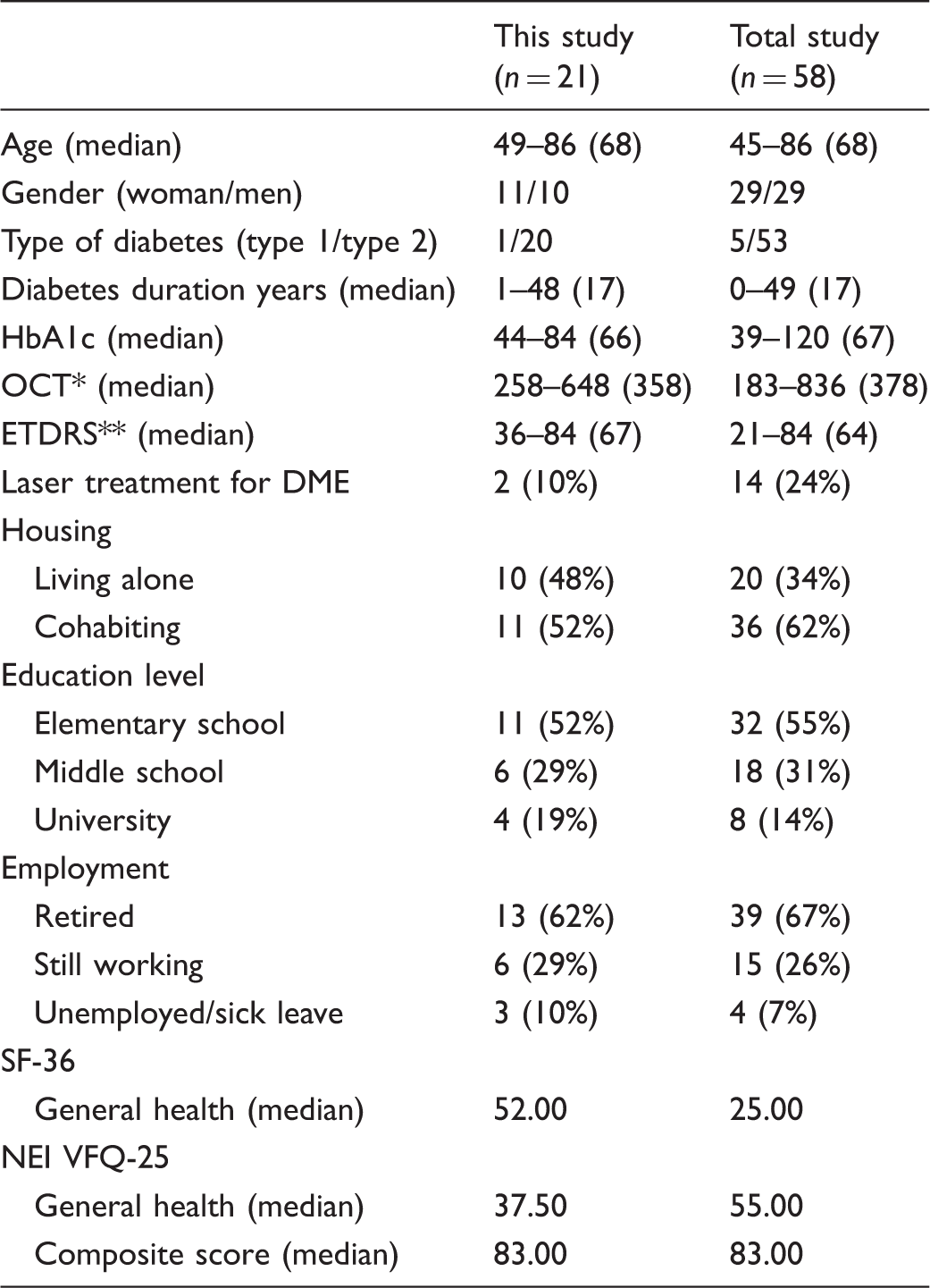
DME = diabetic macular oedema.
OCT = Optical coherence tomography, measures the retinal thickness.
ETDRS = Early treatment diabetic retinopathy study, measures visual acuity.
This study was approved by the Regional Ethical Review Board of Uppsala, Sweden (Dnr 211/264) and was conducted in accordance with the tenets of the Declaration of Helsinki. The participants received written and oral information about the study. All participants gave their written consent before the study began. Participants were informed that they could terminate their participation at any time. The fact that the study was voluntary was emphasized in the information provided to the participants, as well as the fact that non-participation would not affect the standard of care participants received.
Interviews
The interviews were performed at an appointment when medical data and questionnaires were collected, as described elsewhere. 12 The participants were interviewed before they received their first anti-VEGF injection. The interviews were conducted in conjunction with a scheduled appointment in a room at the clinic, where the interviewer and participant had privacy. All interviews were conducted by the first author (TG) and an interview guide with questions was provided. The questions focused on the participants’ experiences, thoughts, and feelings about the treatment, their perception about the connection/relationship between DM and visual impairment, and if and how visual impairment affected their daily life. Examples of questions from the interviews are: ‘What are your thoughts about the treatment you are going to receive?’, ‘Does visual impairment affect you in your daily life?’, and ‘Do you know if there is any connection between your diabetes and your vision problems?’ The participants were asked to share their experiences and the answers were followed up by supplementary questions (e.g. ‘What do you mean?’, ‘Can you explain more?’, ‘Can you give an example?’) The interviews lasted between 10 and 40 minutes, and were recorded and transcribed verbatim.
Data analyses
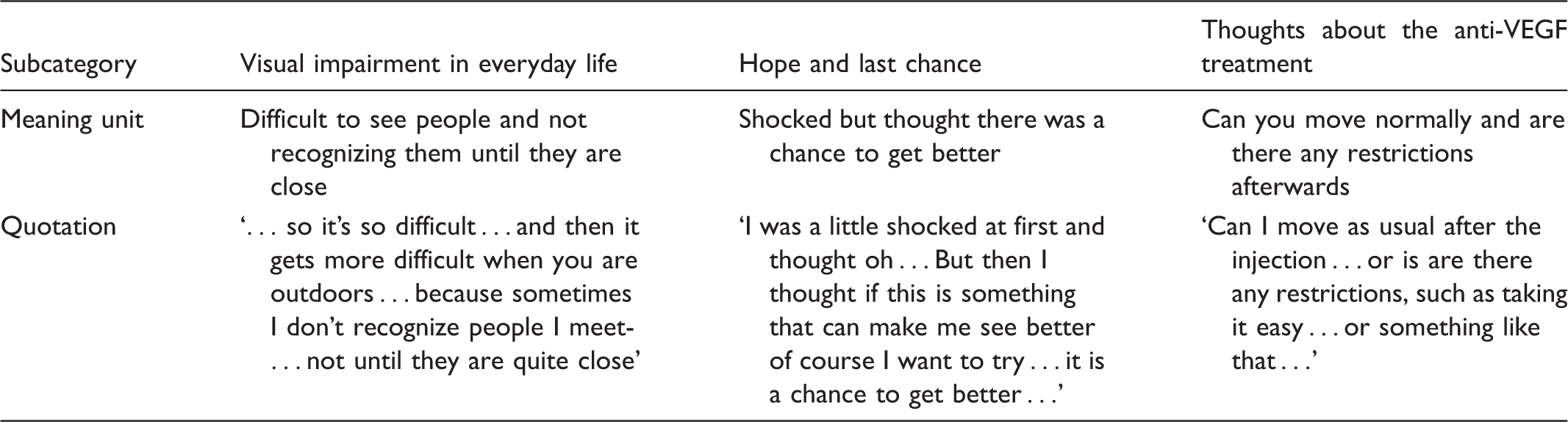
Analysis process examples of citations, meaning units and subcategories.
Findings
Theme, categories, and subcategories.

Perplexity before the treatment
Thoughts about anti-VEGF treatment
Before the first injection, many of the participants expressed concern, uncertainty, or anxiety. They even used the word ‘scared’ to describe their mood. They also expressed an eagerness to start the treatment to be able to finish it as quickly as possible. A further dimension was expressed concerning the emotions of anxiety and fear, and whether negative effects might occur after the injection. The participants tried not to think about this aspect. Some of the participants had been offered anti-VEGF treatment at an earlier time, but had declined because they thought that the injection treatment was frightening. … It’s really hard knowing that someone will do this to my eyes … I must say I find it very, very hard … and I notice that I have been very, very tense the last few days … (F8)
Most of the participants had never heard about the injection treatment for DME. Many participants thought that laser treatment was the only option. When the participants obtained information about the treatment procedure, some of them initially hesitated to receive the treatment because it involved receiving injections in the eye. At the same time they were positive about receiving a different type of treatment. They asked questions about the practicality of the treatment, such as ‘Can you see the needle?’, ‘Does it hurt?’, ‘How long does the treatment take?’, ‘How many times do I have to go to the eye clinic?’, and ‘How long can I be absent from work?’ These issues could be perceived as difficult and time-consuming for the individual.
The participants also had thoughts about possible side effects. They expressed worry and fear that something would go wrong, but said that they tried not to think about it. You get a little scared when you read and it says things about the retina and little things like that … then you get a little worried … (M8)
The participants had various experiences regarding the information given. Some of them felt safe and calm, whereas others were insecure and did not know what the injections would be like. They expressed fear of seeing a needle, as well as fear of pain.
Hope and a last chance
All of the participants felt hope that they might experience improved visual acuity after treatment. However, at the same time, they expressed caution and stated that they could be satisfied if their visual acuity could be stabilized and the deterioration could be stopped at the current level or at least not worsen. They were also thankful that there was a treatment available in addition to traditional laser treatment. I’m just glad there is something more … that you can get treatment for it. (M4) I don’t think it will get worse … I am sure of that … and if I am lucky and it gets better, so be it … and if it stabilizes … it will be good too … so I am positive … (F6)
The participants expressed the hope to be able to maintain current abilities, such as driving and reading, and they had a desire to regain abilities they had lost because of visual impairment.
The participants experienced this treatment as a last chance to stabilize or improve their visual acuity. The thought of an injection was frightening, and at first, they did not want to have any injections in the eye. They finally chose to receive this treatment as a last chance to achieve a positive result for visual acuity. I feel forced to do this because I have no other choice … (F6)
Perception about diabetes and visual impairment
Relationship between diabetes and visual impairment
We found that the participants showed a balance between awareness and unawareness regarding the relationship between diabetes and visual impairment. Some patients had knowledge that diabetes can lead to late complications and that DME can lead to visual impairment. Yes it has … it has to do with diabetes … I am convinced of that … (F4) What I have now is swelling in the macula and rupture of blood vessels. It is a clear connection. (M4)
However, many participants did not understand the association between diabetes and visual impairment or that diabetes could lead to late complications. This situation became a reality when they were affected by DME. I did not understand what it was … but I saw some pictures and I could see a dark spot, but I didn’t understand what it was … (M2)
Experience of disease progression
Several experiences of the situation of having DME were expressed in the interviews. Disease progression with decreased visual acuity could develop over a short time, within a few weeks or months, and patients experienced worry and discomfort. Some participants noticed a sudden decrease in visual acuity. For other participants, visual impairment developed slowly over time and they noticed a small difference over time. Well when I noticed … this … something was not right … it was not like this before … I was able to do crosswords without glasses … but suddenly now I could not … it was just blurry … (F10) It might actually be last year that I noticed it. (M3)
Fear of deterioration or blindness
The fear of becoming blind occupied many of the participants’ thoughts. One participant even used the word ‘horror’ about the thought of becoming blind. One of the participants described a feeling of emotional shock when it became clear that visual impairment was a reality. A feeling of being handicapped if visual acuity deteriorated further was expressed and the participants also expressed concern for the future. Participants who were still gainfully employed had thoughts about how visual impairment would affect their work situation. Work could also already have become difficult in terms of performing their duties and they experienced fear of not being able to continue working until retirement. There was the perception of a burden to live with visual impairment and a fear of it becoming worse. I don’t want to lose my vision, which is my worst fear … (F6)
Visual impairment in everyday life
There were different experiences of visual impairment in everyday life. The participants had varying degrees of visual impairment and experienced daily life in different ways. Generally, the participants could manage their daily lives when they were in their own homes. Some of them were dependent on their husband or wife or needed to ask someone else for help.
The participants talked about different ways to adapt and compensate in their everyday lives. They used various aids for visual impairment. They had refurnished at home, bought more lamps, or asked someone for help. A consequence of visual impairment could be that a person had to completely finish hobby activities, although he/she wanted to continue these activities. The participants also described how they adapted to their visual acuity, and how they were resigned and had lower expectations of their visual acuity over time. I have bought a large television and moved it closer to the couch so that I can see … (M9)
Many of the participants experienced a feeling of limitation in their daily life. Anything that required good visual acuity became difficult to perform and this affected their daily life. It is difficult … sometimes it is difficult to write and that depends on the light … I like to write in daylight … when it is brightest, and if I need light, I turn on the ceiling light so I can see … it depends, and sometimes it is difficult to solve crosswords; for example, I have to sit with a magnifying glass … (F9)
However, some of the participants did not have trouble with tasks, such as reading. Participants felt that not being able to see faces or people who they met when they were out could be embarrassing. So it is hard … and it is harder when you are outside … because sometimes I don’t recognize people … when you meet them … until they are right up close … only then I can see who it is and then I maybe don’t have time to say hello … (M6)
Discussion
This study showed that participants’ thoughts and feelings associated with anti-VEGF treatment included the relationship between diabetes and visual impairment, and the progression of disease and fear of becoming blind. The latent theme of ‘to be at a crossroads and a crucial phase in life with an uncertain outcome’ emerged.
The participants in our study described a feeling of uncertainty before the first injection, such as concern, uncertainty, or anxiety. This result is in accordance with the findings of another study, 25 which showed that fear and discomfort could appear related to treatment procedure and visual loss. Additionally, the patients in our study suffered from a lifelong systemic disease, diabetes, which adds to the burden of this treatment, and entails higher demands at an optimal attention and treatment. During the interviews, the participants discovered that they had not been aware of the relationship between diabetes and late complications, such as retinopathy and/or macula oedema. They recognized or understood the association between late complications and diabetes only when they were diagnosed with DME. This finding is noteworthy and shows that there is a knowledge gap about how to inform people with diabetes regarding the association between diabetes and late complications. This knowledge gap has been well studied, but the solutions appear difficult to implement in everyday practice.31–33 Ophthalmic surgical procedures generally arouse anxiety 34 and uncertainty about practical issues, such as a long distance to travel and many hours spent at the eye clinic. In our study, working professionals expressed concern about absence from work. These concerns could be addressed with clear information from the eye clinic. There could also be uncertainty about the treatment procedure, as shown in other studies.25,35–37 Gomez et al. 38 have described practical steps that can be performed at the eye clinic in order to improve the patients’ experiences, for example using pillows or holding hands. Additionally, ensuring that the information that is provided is understood by the patients is important.
At the same time, the participants in our study expressed gratitude for the treatment and were grateful that they had another chance that could hopefully save their visual acuity. Sometimes, the participants thought that the opportunity to receive injections was their last chance to save their visual acuity and that they had no other choice. Gomez et al. 38 pointed out practical strategies for alleviating discomfort during the injection, which is important. However, participants in our study experienced a type of existential burden, such as thoughts about losing their vision and how to cope with everyday life.
A fear of deterioration or blindness was expressed by the participants in the current study. Other studies have shown that this can lead to anxiety,39,40 negatively affecting people’s lives and perceived situations. 41 Adapting to vision loss is an ongoing process where a person may experience suffering and hope. 42 In view of the suffering experienced in relation to the threat of vision according to Eriksson et al., 26 injection treatment can be seen as a source of hope that can relieve suffering in this situation. Patients with visual impairment due to DME are a vulnerable group of patients and meeting their needs regarding individual support and information is important.
Both the diabetes and ophthalmological healthcare professionals play an important role for patients about to undergo anti-VEGF injection treatment. It is important to open up a dialogue between the eye clinics and the diabetes clinics as a means both to strengthen the cooperation and also to clarify who is responsible for providing the information and support that the patient needs.
The capacity of the individual patient to cope with the situation and the provision of individual support need to be considered; in addition, the type of support that the patient requires to cope with his/her ‘suffering’ needs to be addressed (in our case, thoughts and feelings related to complications with sight-threatening diabetes).
To create opportunities to manage the suffering associated with diabetes and sight-threatening complications, a didactic model called ‘The Challenge to Take Charge of Life with Life-Long Illness’ 42 could be used. This model implies that patients – together with a nurse – have time to reflect on their life and situation in a structured way so as to be able to set goals that let them manage their diabetes and late complications.
Methodological considerations
The interviews in our study were conducted at the eye clinic, which was a familiar environment for the participants. Some of the participants were going to receive their first injection the same day and may subsequently have experienced stress. However, the interviewer (TG) believed that the participants felt that it was positive to talk about their thoughts about the treatment. The participants were encouraged to talk about their experiences and provide examples of situations or feelings. These people were scheduled for regular appointments once a month and had the opportunity to ask questions about the treatment if needed. This study was conducted in a Swedish context, which can limit its transferability to other countries, because the guidelines for anti-VEGF treatment can differ between countries. The analysis process was continuously discussed by the authors. This process frequently involved reflection by moving back and forth between the transcribed interviews, meaning units, codes, subcategories, and categories. The underlying meaning of the categories was expressed as a latent theme. We described the analysis process with examples to achieve transparency and trustworthiness.
Ethical considerations
The interviews could have aroused feelings and thoughts in the participants about their diabetic complications and their situation. All of the participants obtained information that the treating eye doctor, one of the authors, was available to talk to if required. In this study, there was no possibility of involving an interpreter or competence to allow inclusion of patients with cognitive impairment or non-Swedish speaking patients. However, these patients should be included in further studies.
Conclusion
People with DME who are about to start anti-VEGF injection treatment are a vulnerable group of patients with various requirements for information and support in different areas. There appears to be a need for personalized information and also an opportunity for reflection about the situation of patients. Cooperation between various caregivers could be improved to take advantage of available knowledge and resources.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.