
Abstract
Introduction
A pulmonary rehabilitation (PR) programme, including exercise training, education, and behaviour change, is highly recommended in treatment guidelines for chronic obstructive pulmonary disease (COPD). A new PR educational material for PR using an interactive three-dimensional (3D) visualisation technique was developed. There is little known regarding using 3D in this setting. The aim was to evaluate, within a PR programme setting, differences between outcomes of education through interactive 3D compared with education by means of 2D visualisation in patients with COPD regarding health-related quality of life (HRQL), physical capacity, exercise self-efficacy, compliance to exercise training, compliance to medication, and the use of health care and to describe learning styles.
Methods
Patients were cluster randomised to PR at the University Hospital clinic, including exercise training, for 10 weeks with education by 3D (n = 27) or education by traditional 2D technique (n = 17). At follow-ups, HRQL, physical capacity, self-efficacy, handgrip strength, compliance to exercise training, compliance to medication and health care utilisation were assessed.
Results
No significant differences were observed in HRQL in relation to COPD between the groups after 10 weeks. Differences were found in handgrip strength at baseline and at 10 weeks (p < 0.01). The 3D group had improved scores in HRQL assessed with the Leicester Cough Questionnaire (LCQ-S) psychological domain (p = 0.022). In the 2D group, the LCQ-S social domain (p = 0.028), psychological domain (p = 0.021) and the St George’s Respiratory Questionnaire total (p = 0.050) were increased. The most common learning mode and learning style in both groups was reflective observation and divergent style.
Conclusion
An interactive education in 3D technique used in a PR programme for patients with COPD yielded no significant differences compared to conventional techniques. Three-dimensional techniques can be used in PR for COPD as an alternative to conventional techniques. ClinicalTrials.gov (identifier:NCT02802618).
Keywords
Background
Chronic obstructive pulmonary disease (COPD) is a growing global health problem, 1 it is now one of the third leading causes of death worldwide. 2 COPD is a heterogeneous lung condition characterised by chronic respiratory symptoms due to abnormalities of the airways and/or alveoli that cause persistent, often progressive, airflow obstruction. Frequent exacerbations and comorbidities add to the overall severity of the disease. 1 These include anxiety and depression and the non-respiratory consequences, for example fatigue, malnutrition, and muscle dysfunction, which add to the reduction in health-related quality of life (HRQL) and physical capacity. 3 Pulmonary rehabilitation (PR) designed to improve the physical and psychological state of patients – including education, exercise training, and behaviour change, all of which are pursued to encourage long-term adherence to health-improving behaviours including self-management strategies – is recommended as one of the most effective interventions in COPD.1,4–7 PR is one of the non-pharmacology therapies shown to reduce mortality. 8 Completion of PR reduces use of health care9,10 – for example by reducing hospital admissions.10,11 Patient education in COPD could reduce costs of health care by decreasing the need for visits to physicians. 12
To emphasise behavioural change, education is seen as a central component in PR, since this provides the patient with the required knowledge. Different factors may reduce learning – for example having low self-efficacy, but also anxiety, depression and fatigue,13,14 all common symptoms in COPD.1,5,15–17 A positive relationship between self-efficacy and HRQL has been shown in COPD. The relationship is stronger for exercise-specific self-efficacy measurements than for measurement of generic self-efficacy. 18 When changing a behaviour within the scope of PR, the assessment of patients’ self-efficacy and their overall psychological condition is of importance in the implementation and understanding of what might influence the effects of PR. 19
There are many ways of learning a new task, and people usually have a preferred way of learning, a so-called learning style. There are several learning styles that learners can be categorised into. 20 Since the idea is that educating someone in accordance with their learning style will result in improved learning, 20 educational situations should be customised to the learners’ individual learning styles. 21 Adapting information and educational materials to patients’ learning style preferences may also play an important role in their ability to obtain an appropriate level of health literacy. 22 This has been shown in a group of patients with diabetes receiving education adapted to their learning styles. 22 It is likely that the adaptation of education to learning styles could improve learning and thereby make PR more efficient. 23 Although there has been suggested to be a need to assess learning styles, there are still few implemented interventions that customise material to match learning style preferences.24–26 Adapted patient education material on heart failure, high blood pressure, and diabetes has been assessed, but to our knowledge, learning styles have not been considered for patients with COPD attending PR.22,27–29 Before education in PR can be adapted to learnings styles, more knowledge is needed about preferred learning styles in people with COPD.
In traditional patients’ education, the anatomical structures’ size and complexity often create obstacles for the understanding of the learners. 30 In computerised three-dimensional (3D) models, the material appears to have width, height, and depth 31 and could make it easier to comprehend, but there is contradictory evidence on how effective it is to use 3D.30,32–34
Some promising results in student education in medical university courses learning about anatomical structures using interactive 3D have been demonstrated.30,33 Since 1995, the evidence-based PR programme for COPD used at Karolinska University Hospital in Stockholm, Sweden, has been continuously revised.5,35 The most recent update used interactive 3D technique in the theoretical part. The 3D technique was used to enable a more customised education and enhance the understanding, and also to increase motivation and engagement for the patients regarding their education in PR for COPD.
In the present study, we hypothesised that education by interactive 3D within a PR programme for COPD would show at least equivalent results to 2D.
Aim
The aim was to evaluate, within a PR programme setting, differences between outcomes of education through interactive 3D compared with education by means of 2D visualisation in patients with COPD regarding HRQL, physical capacity, exercise self-efficacy, compliance to exercise training, compliance to medication and the use of health care and to describe learning styles.
Methods
Study design
A parallel cluster randomised controlled trial design was used. 36 Patients were recruited during 14 months from a waiting list at the Department of Physiotherapy at Karolinska University Hospital in Stockholm, Sweden. The waiting list included patients with COPD, who had been advised by a health care giver to participate in a rehabilitation programme for COPD and who accepted to be informed when it was their turn. This was a convenience sample recruited before the Covid-19 pandemic. Patients on the waiting list were outpatients with referral from primary health care, referral from the Karolinska University's Lung Department, or patients previously attending the physiotherapy department. The patients were randomised in clusters imbalanced [3:2], i.e. when 8–10 patients were consecutively recruited from the waiting list, they formed a group that was randomised 36 into participation in the PR programme with education by interactive 3D or education by 2D. The criteria for inclusion were a COPD diagnosis, in Global Initiative for Chronic Obstructive Lung Disease (GOLD) stages 2–4, 1 and comprehending the Swedish language. Having reading and/or writing difficulties was accepted. Exclusion criteria were not used.
Ethics
The Regional Ethical Review Board in Stockholm approved an ethical application for the study (reg. no. 2013/1276-31/3) before the study was conducted. The study was registered in ClinicalTrials.gov (identifier: NCT02802618). All patients received oral and written information about the study and signed a letter of consent prior to participation. The study was performed according to the Declaration of Helsinki. 37
Intervention
The patients received education and exercise training5,35 at the hospital clinic twice a week for 10 weeks. During the first five weeks, the programme consisted of education and physical exercise training, and in the last five weeks, only of physical exercise training. The education consisted of lectures held by the multidisciplinary COPD team (physiotherapist, nurse, occupational therapist, medical social worker, dietician, and physician). The lectures led by the physiotherapist presented with interactive 3D and included:
anatomy and physiology of the lungs and thorax the COPD disease with pathophysiology and its processes breathing techniques and coughing inhalation techniques physical exercise and physical activities
The other lectures held by the COPD team were presented with traditional 2D techniques, irrespective of group. The content of the education5,35 was identical in both groups.
The interactive 3D visualisation technique used in the study was developed by Sensavis Inc©, 38 in collaboration with two experienced registered physiotherapists from Karolinska University Hospital, Stockholm, Sweden, one of whom was specialised in pulmonary medicine. The 3D technique was displayed by a hardware setup with an Elite book, with Windows 8 and 4GB random access memory on a 50’-screen Hewlett-Packard (HP) 3D TV set, and patients and tutors used active 3D glasses (passive polarised). 31 This programme incorporated possibilities to easily turn the displayed 3D human animated body 360°, to flip, invert, and rotate the presented view from all angles, to zoom in and zoom out and go from macro- to microstructures in the animation, and to watch complex parts of the body interacting instantaneously. The patients could view the spatial relationships between different anatomical structures, such as the diaphragm's movements while the chest was moving, as well as how the heart pumped and how this related to other parts of the body such as the ribs and sternum. The option of turning the image 360° made it possible to view the same aspects of given anatomical relationships, but from different angles. The 3D programme made it possible for the tutors to immediately interact with the patients during the lessons. The 2D educational part was displayed on a large screen and with still pictures and text presented in a PowerPoint presentation view.
The physical exercise training part of the PR programme was supervised and led by an experienced registered physiotherapist specialised in pulmonary medicine 2 times a week for 60 min, following international guidelines for PR. 5 All patients had individualised physical exercise training programmes, including strength training for the lower and the upper limbs, the abdomen, and endurance training. The strength training was performed in weightlifting machines, with resistance training bands, dumbbells, chair standing, and step-up board. The strength training programme consisted of 8–10 individual exercises, 10 repetitions in 3 sets where resistance was gradually increased. The continuous endurance training consisted of cycling for 30 min at a level of dyspnoea 3–6 on the Borg CR-10 scale. 39 Oxygen saturation and heart rate were registered at rest and during endurance training. In accordance with patients’ current health status, the training resistance bands, weights, and the numbers of repetitions were individually adjusted regularly by the physiotherapist during the intervention period. After the 10-week intervention to support self-management, all patients received a personalised exercise programme based on resistance training bands and were encouraged to continue with exercise training at home twice a week, in addition to daily walks of 30 min. Furthermore, the patients were encouraged to present to the physiotherapist how they wanted to continue with their exercise training. 7
Assessments were conducted at inclusion, at 10 weeks and 6 months after the intervention, by a test leader who was not involved in the tutoring or in the physical exercise training. One patient was supported during assessment due to reading and writing difficulties.
Basic characteristics were measured at inclusion. Patient's latest available lung function test (spirometry), with the FEV1/FVC (forced expiratory volume the first second/forced vital capacity) < 0.7 and the FEV1% of predicted, was used to grade their lung function according to the GOLD severity classification system. 1 The emotional status was measured with the Hospital Anxiety and Depression Scale (HAD). 40 The HAD is a 14-item questionnaire with a 4-point Likert scale containing two parts, anxiety (seven items) and depression (seven items). A higher score indicates higher level of psychological distress, 8–10 points indicate borderline abnormal level, and ≤11 suggests abnormal level concerning depression and anxiety, respectively, and the minimum clinically important differences are 1.6 units for HAD depression and for HAD anxiety.40,41
The preferred way of learning was classified with Kolb's classification of Learning Style Inventory System. 42 The scores were calculated in columns for the four ‘learning modes’; concrete experience (CE; feeling), reflective observation (RO; watching), abstract conceptualisation (AC; thinking), and active experimentation (AE; doing). When illustrated in a circle with a cross (Figure 1), lines were drawn to connect the scores for each of the four learning modes into a kite-formed profile. The shape of the kite was used to determine which one of the four learning styles was the most preferred, and how strongly or weakly the other styles were preferred. A person who tended to use the AE (doing) and AC (thinking) modes is said to use a convergent learning style: learns ‘hands-on’ and applies previously attained knowledge; to use the CE (feeling) and RO (watching) modes is said to correspond to a divergent learning style: reflects on a situation from different perspectives at a later stage; to use the AC and RO modes is said to correspond to an assimilation learning style: gathers and organises information to make most sense; and to use the CE and AE modes is said to correspond to an accommodative learning style: learns ‘hands-on’, but wants to find the solution through trial and error.21,43

The learning styles divergent, assimilating, convergent and accommodation by Kolb, including the four ‘learning modes’: concrete experience (CE), reflective observation (RO), abstract conceptualisation (AC) and active experimentation (AE) presented with an example of a person's kite-formed total profile, 20 presented in Kolb's circle modified by authors.
HRQL in relation to COPD was assessed with the COPD Assessment Test (CAT), 44 the Swedish version of the Leicester Cough Questionnaire (LCQ-S),45,46 and the St George's Respiratory Questionnaire (SGRQ) 47 at inclusion and at 10 weeks. The CAT is an eight-item questionnaire, with scores from 0 to 5 and a maximum score of 40. 44 A higher score indicates higher impact, and the minimal important difference (MID) is 2–3 units. 41 The LCQ-S is a 19-item questionnaire with a 7-point Likert scale containing three domains: physical (eight items), psychological (seven items), and social (four items). Each domain can give points from 1 to 7, and the total score varies from 3 to 21. 45 A higher score indicates less impact, and the MID is 1.3 units. 48 The SGRQ is a 50-item questionnaire with scores from 0 to 100, containing three domains: symptoms (8 items), activity (16 items), and impacts (26 items). 47 A higher score indicates higher impact, and the MID is 4 units. 49
Self-efficacy related to exercise was assessed with the SCI Exercise Self-Efficacy Scale (ESES). The ESES is a 10-item questionnaire with a 4-point Likert scale and a maximum score of 40. A higher score indicates higher self-efficacy related to exercise. 50
Physical capacity was assessed with the 6-minute walk test (6MWT) 51 and handgrip strength with a Jamar dynamometer. 52 The 6MWT measures the greatest distance the patient could cover walking in 6 min, on a straight ≥30 m track, and when used in PR programmes, the MID is 25–33 m. 51 The Jamar, an isometrically hand-held dynamometer (Jamar, Preston, MI, USA), was performed while the patients were sitting in the upright position with the elbow flexed 90°, the arm against their side, and the wrist in a neutral position and their thumb up. They were asked to squeeze, for about 3 s, the handle of the Jamar as strongly as they could and while squeezing, they were encouraged. The scale displays isometric grip force from 0 to 90 kg. 53
At six months, follow-up compliance to physical exercise training, compliance to medication and the use of health care (i.e. number of visits to an emergency department and inpatient health care) were assessed. A set of internally developed phrases to measure compliance and use of health care were completed by the patients. A timeline for the assessments and follow-ups of the study is presented in Figure 2.

Timeline showing pulmonary rehabilitation programme and follow-ups including assessments. Photo by Håkan Lindgren.
Statistics
The statistical programme SPSS (IBM SPSS Statistics 24, IBM, New York, USA) was used for all statistical analyses. Patients educated with 3D were conjoined into one group (n = 27) for the data analysis, and patients educated with 2D were analysed as one group (n = 17). To reduce the risk of incorrect entries, the data were checked and read by two persons. All data in the set of internally developed phrases were classified as categorical variables, and all data in the questionnaires and data of learning styles were classified as ordinal data. Data from the Jamar dynamometer, 6MWT, and age were classified as ratio data. Basic characteristics were displayed as n (%), mean ± standard deviation or median, interquartile range (IQR), and range (min–max). The learning styles’ median scores were presented into a Kolb's circle modified by authors. The Kolmogorov–Smirnov test, skewness, and kurtosis values were used to check for normal distribution of the ratio data.
Analyses were conducted on an intention-to-treat basis (n = 44). Missing values were replaced with the previous value. A power analysis or a specific sample size calculation was not performed, given the exploratory nature of the study. Basic characteristics, as well as changes in outcomes between the groups, were analysed with the χ2 test for categorical variables, the Mann–Whitney U test for ordinal variables and for the ratio variables with skewed distribution (6MWT, Jamar dynamometer), and the independent t-test for the ratio data (age). Changes in outcomes within groups were analysed with the χ2 test and with Fisher's exact test for categorical variables, as well as with the Wilcoxon signed-rank test for ordinal variables and for the ratio variables with skewed distribution. Probability values with p ≤ 0.05 were considered statistically significant. If the patient was present for at least 70% of the PR sessions, this was considered to count as participation. 7
Results
Forty-eight patients with COPD were enrolled for participation, and four declined participations. In total, 44 patients were included in the study. Five separate PR programmes were completed during the study period. Five patients failed to complete the study, two in the 3D group and three in the 2D group. Reasons for dropouts at 10-week follow-up were changed employment status (n = 1), private journey (n = 1), having surgery (n = 1), deceased due to other disease (n = 1), other disease (n = 1), and one patient was unreachable at six months follow-up (Figure 3).
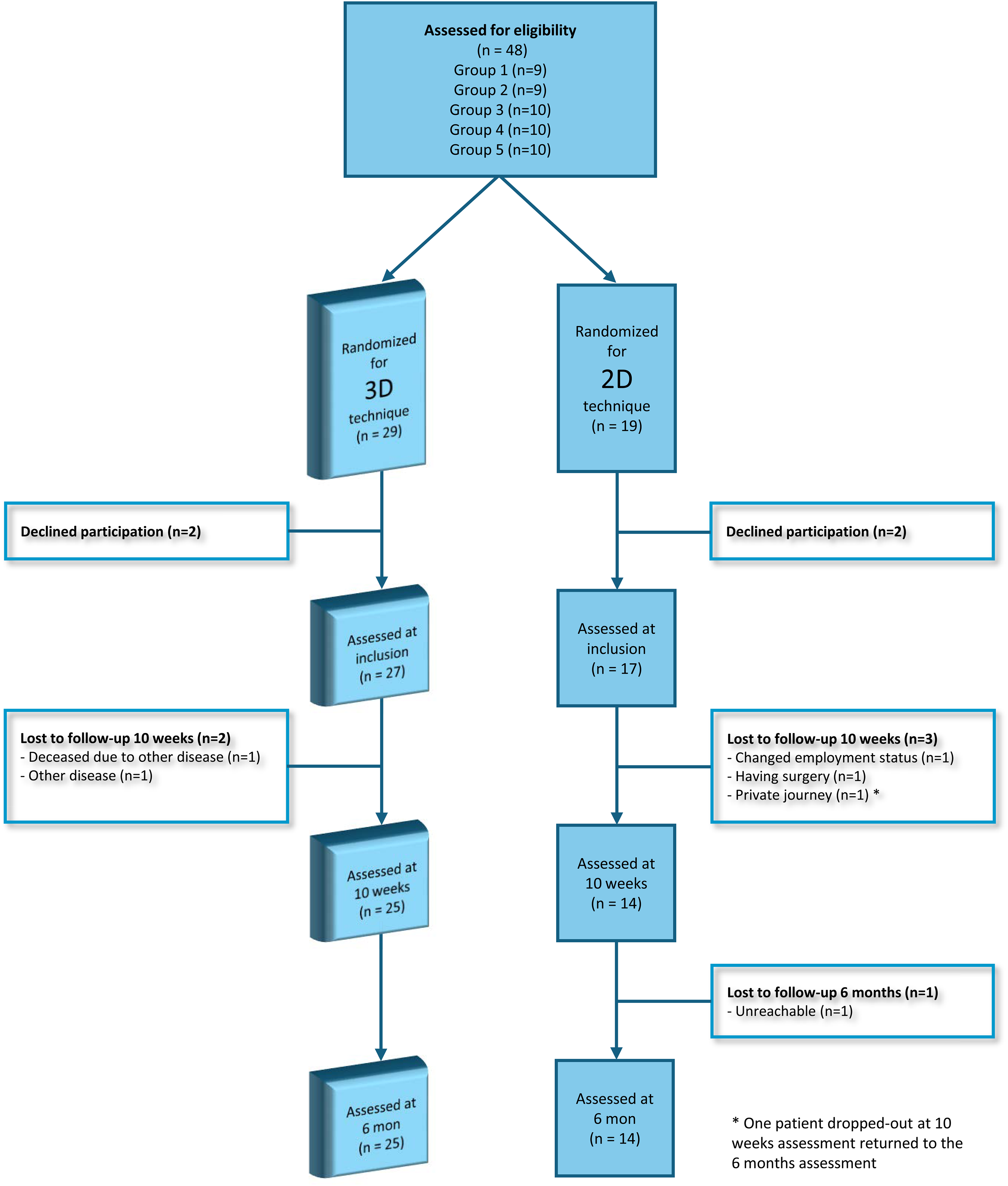
Flow chart of participants randomized for pulmonary rehabilitation for patients with chronic obstructive pulmonary disease using interactive 3D visualisation technique or traditional 2D technique at inclusion and at each follow-up.
The basic characteristics of patients with COPD are presented in Table 1. The mean age was 69 ± 8 years. More than half of the patients were women, and it was a significant difference between groups regarding women in the 3D group (p = 0.036). The patients included were classified as GOLD stages 2–4, and for most of the patients, anxiety and depression were not indicated.
Basic characteristics of the 44 patients with chronic obstructive pulmonary disease divided into the two pulmonary rehabilitation programmes using 2D techniques (2D) or interactive 3D visualisation techniques (3D).

Variables are presented with means, standard deviations (SD), medians, interquartile ranges (IQR), ranges, numbers (n) and percentages (%).
GOLD: Global Initiative for Chronic Obstructive Lung Disease; HAD: Hospital Anxiety and Depression Scale; LSI: Learning Style Inventory System; CE: concrete experience; RO: reflective observation; AC: abstract conceptualisation; AE: active experimentation.
p values from independent t-test.
p values from χ2 test.
n = 43.
n = 41.
n = 14.
p values from Mann–Whitney U test.
n = 16.
Regarding digital literacy, 84% of the patients had access to a computer in their home environment and 77% had used a computer at least once a week during the last three months, while 11% had never used a computer. There were no significant differences between groups.
ixty-six percent of the patients participated at the minimum level of 70% of the 25 sessions. Patients participated in the education sessions with a median of 8, IQR (7–9) of the 10 sessions, and patients participated in the physical exercise training with a median of 11, IQR (8–13) of the 15 sessions. A total share of 84% of the patients participated in at least 70% of the 10 sessions in the educational part of the PR programme, and a total share of 61% of the patients participated in at least 70% of the sessions in the physical exercise part of the PR programme. No significant differences were found regarding participation in PR programme between groups.
No significant differences were shown between groups at 10 weeks regarding HRQL. Significant differences were found between the groups regarding handgrip strength at both inclusion (p < 0.01) and at 10 weeks (p < 0.01) in favour of the 2D group. There were no significant differences between the groups after 10 weeks in physical capacity (6MWT) or in self-efficacy (ESES). In-between group analysis showed that the 3D group increased their psychological domain of the LCQ-S (p = 0.022) and handgrip strength (p = 0.024). In the 2D group, the LCQ-S social domain (p = 0.028), the LCQ-S psychological domain (p = 0.021) and the SGRQ total score (p = 0.050) increased (Table 2).
Results from between-group analyses, presented from the assessment of health-related quality of life, self-efficacy related to exercise, handgrip strength and physical capacity assessments at inclusion and at 10-week follow-up for the 44 patients with chronic obstructive pulmonary disease divided into the two pulmonary rehabilitation programmes using 2D technique (2D) or interactive 3D visualisation technique (3D).

CAT: COPD Assessment Test; IQR: interquartile range; 10 w: 10 weeks follow-up; SGRQ: St George's Respiratory Questionnaire; LCQ-S: Leicester Cough Questionnaire, Swedish version; ESES: SCI Exercise Self-Efficacy Scale; SD: standard deviation; 6MWT: 6-minute walk test.
p values from between-group analyses (Mann–Whitney U test) at 10-week follow-up.
n = 43.
n = 16.
n = 42.
n = 15.
The median scores and IQR for the learning modes are presented in Table 1. Regarding the patients’ learning style scores, the most frequently preferred learning mode, presented according to the kite-formed profile (3D vs. 2D) (see Figure 4), was the RO (median 21 vs. 19.5), followed by the AC (median 18 vs. 19), the CE (median 18 vs. 17), and the AE (median 16 vs. 16.5). The most common learning style was the divergent style, in both groups. In the 3D group, the divergent learning style was preferred followed by the assimilation learning style, the convergent learning style, and the accommodative learning style in descending order. In the 2D group, the order was the same except that they preferred an accommodative learning style before a convergent learning style. Overall, there were no significant differences between the groups.
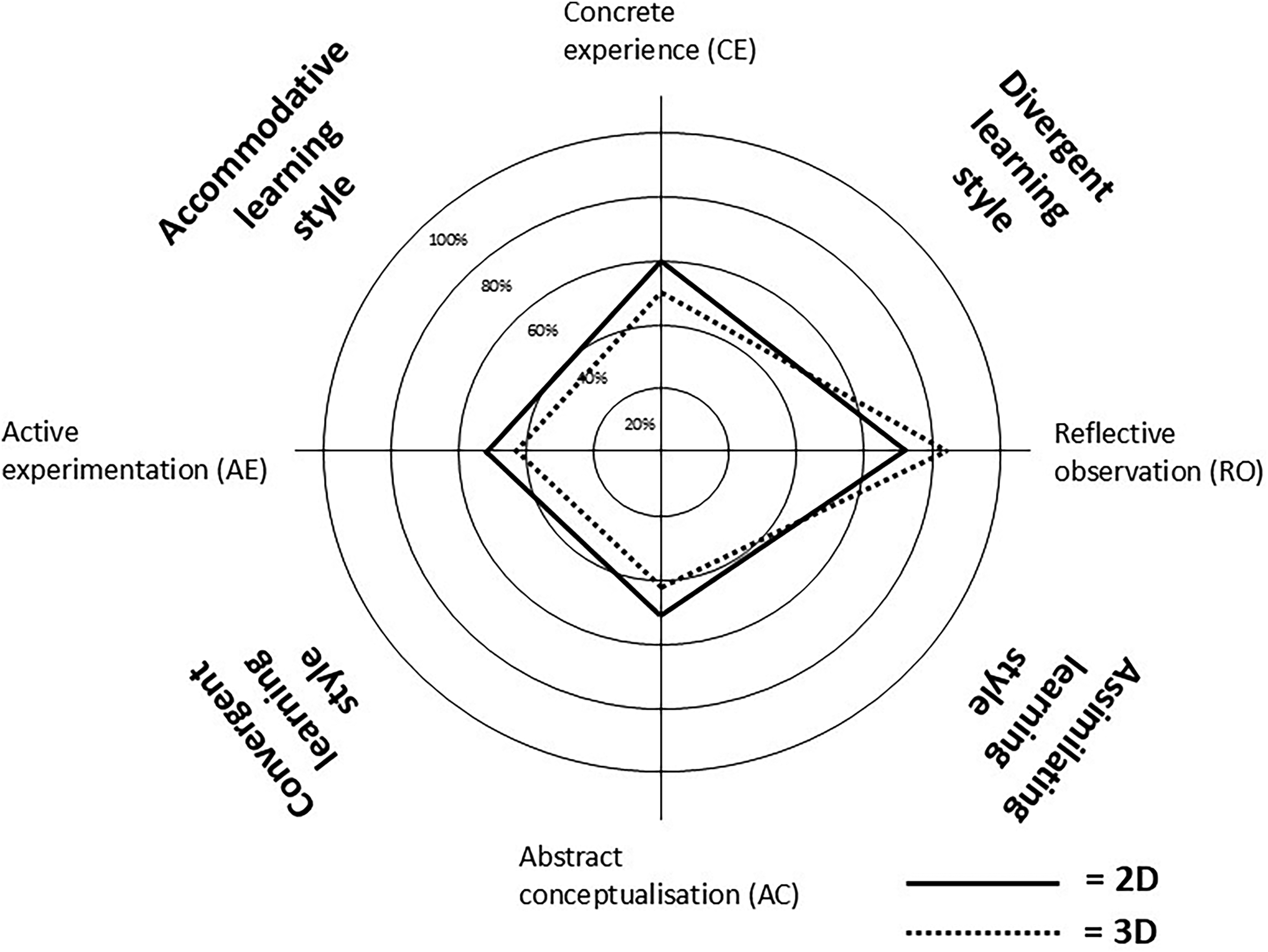
Learning styles and learning modes by Kolb 20 at inclusion presented for the two groups of patients with chronic obstructive pulmonary disease included in pulmonary rehabilitation, the interactive 3D visualisation technique (3D) and the 2D conventional technique group (2D). The result is presented in Kolb's circle modified by authors.
At the six months follow-up, compliance to the recommended exercise was 68% in the 3D group and 51% in the 2D group, and compliance to the recommended medication was 96% and 100%, respectively. In the 3D group, almost one-third of patients (28%) had visited the emergency department versus almost two-thirds of patients (57%) in the 2D group. In addition, 12% of the patients in the 3D group had inpatient health care visits versus one-third in the 2D group (29%), and there were no significant differences (Table 3).
Results from between-group analyses, presented from use of health care, compliance to exercise, and compliance to medication at 6 months follow-up for the 44 patients with chronic obstructive pulmonary disease divided into the two pulmonary rehabilitation programmes using 2D techniques (2D) or interactive 3D visualisation techniques (3D).

n: numbers; %: percentages; IQR: interquartile range.
p values from χ2 test at six months follow-up.
n = 39.
n = 14.
n = 25.
p values from Mann–Whitney U test at six months follow-up.
p values from Fisher's exact test at six months follow-up.
Discussion
There were no significant differences between the groups after 10 weeks regarding HRQL in relation to COPD. Significant differences were found between the groups regarding handgrip strength at both inclusion and after 10 weeks in favour of the 2D group. There were no significant differences between the groups after 10 weeks regarding the 6MWT, ESES, and compliance to exercise, medication, or use of health care. In summary, education through 3D within a PR programme for COPD seems equivalent regarding outcomes to using 2D. The most common learning mode and learning style were RO and divergent style, in both groups.
It has been shown that people with stable COPD achieve clinically important improvements in exercise capacity and HRQL after PR. 9 Consequently, a control group not receiving PR programme was not an alternative due to ethical issues in the present study. Instead, it was hypothesised that the outcomes of education by 3D techniques within a PR programme would at least be equivalent to using 2D techniques. In-between group analysis showed that the HRQL in the 3D group was increased when assessed with the psychological domain of the LCQ-S. In the 2D group, the social domain and psychological domain of the LCQ-S scores as well as the SGRQ total score increased, which support the hypothesis concerning HRQL.
Regarding physical capacity, handgrip strength increased in the 2D group, although the results need to be interpreted with precaution since the groups differed already at inclusion. The differences at inclusion in favour of the 2D group might be explained by the higher proportion of men in the 2D group. 54 Walking less than 350 m in 6MWT has been associated with an increase in mortality, 55 but although the total group of participants (conjoined into one group) reached a mean distance of 360 m at 10-week follow-up, the increase was not significant. In the theoretical part of the programme, 84% of the participants reached an attendance rate of 70%, but in the exercise training part, just about 59% of participants reached this acceptable attendance level. 7 This has also been shown in a systematic review on PR, where the rates of patients not completing the PR varied between 10% to 32%. 56 The lower attendance rate in the exercise part of the programme in this study could be explained by exacerbations or other medical condition also showed previously among the patients with COPD. 57 In addition, having depression and anxiety, and being a woman increase the risk of not completing PR.56–58 Almost half of the patients in this study were living alone, which also could have affected the attendance level, since having a spouse or partner as caregiver has a strong relationship with participation 59 whereas living alone increased the challenges of getting to the PR. 56 Exercise training is a key component of PR and includes the goal of improving or maintaining physical capacity.1,5 In this study, the lower attendance rate for the exercise training part might explain why there were no significant improvements in physical capacity. Physiological changes are relevant to explain the variable improvements of physical performance after PR in patients with COPD 60 ; therefore, another probable explanation might be the incidence of responders and non-responders to exercise training in this study population.
Higher self-efficacy has shown to predict more improvements in 6MWT after PR. 61 In the present study, there were no differences between groups after 10 weeks regarding ESES. The median(IQR) score in the total group of participants (conjoined into one group) was 20 (16–27). These results can be compared with those from a Swedish study on neurological disorders (n = 30), presenting a median score of 26.5 (17–33), 62 and people with spinal cord injuries in the USA (n = 396) scoring a mean of 34 ± 5. 50 This comparison might indicate that patients in this current study had lower self-efficacy, which might have affected the outcomes of PR.
Improving medication adherence is considered critical for optimising patient outcomes63,64 and is also associated with reduced health care utilisation.64,65 By providing adequate information about medications to the patients, the adherence is likely to increase. 63 In the present study, there were no differences between the groups at 10-week follow-up regarding compliance to medication or compliance to exercise. At 6-month follow-up, compliance to medication was extremely high: almost 100% in both groups. This result might be explained by a behavioural change due to the PR programme, although since patients’ compliance before entering the programme is unknown, the result should be interpreted with precaution.
At 6-month follow-up, compliance to exercise was 68% in the 3D group and 51% in the 2D group. Exercise is more time consuming, and a wide range of barriers interfering with exercise behaviours is associated with maintaining exercise programmes. 66 Exercise behaviour has been found to be the first strategy to be ended by patients with COPD when difficulties are confronted, 67 which might explain the lower compliance to exercise compared to medication.
There were no differences between the groups after 10 weeks regarding use of health care, which indicates that both 3D and 2D techniques can be used. Thirty-nine percent of all the participants in the conjoined groups had visited the emergency department six months post-PR, and 18% had had inpatient health care. These results can be interpreted in relation to those from studies in Australia, following patients with COPD during 12 months after PR, where 45% had hospital admissions and/or visits to the emergency department upon 1–10 occasions. 68 Persons with COPD who completed PR have shown to decrease number of emergency department visits and length of stay in hospital compared to levels pre-PR. 69 A study from Norway showed that 4 h of group education for patients followed by individual sessions with a physiotherapist and a nurse reduced costs at 12 months follow-up, as physician visits decreased by 85%. Further research is needed concerning interactive 3D techniques and health care use, since pre-PR programme data were not collected in this study and the follow-up window only extended to six months. 12
In the present study, learning modes and styles were assessed for patients with COPD, and no previous studies regarding these aspects were found. The most common learning mode was RO, and the most common learning style was the divergent style, in both groups.
A divergent style can be described as the ability to interpret a question in many different ways and to see many different answers. 42 This learning style could contribute to being imaginative and having awareness of meaning and values by observing and feeling, 21 and therefore, 3D techniques might be a suitable educational approach, but more research is needed. In the present study, none of the interventions assessed involved adapting either the education or physical exercise part of the programme to the patients’ learning modes and styles. In the few previous studies found on integrating learning-style preferences into the process of communicating health information, patients’ knowledge and compliance increase.22,27 It might be an important factor in future studies to individually, or in a group setting, tailor the educational part in PR in relation to patients’ preferred learning styles.23,28
There were both strengths and some limitations in the present study. Analyses were conducted on an intention-to-treat basis, aiming to mimic a real-life clinic situation. The limited number of patients included was due to the set time frame of the study, and this might have affected the external validity. The fact that the 3D conjoined group was larger than the 2D conjoined group could have led to some limitations. However, to gain more knowledge of new treatments, a higher number of participants could be randomised to the new treatment group. 36 The patients referred to the PR programmes at Karolinska University Hospital clinic generally have more severe COPD symptoms comped to those attending the PR programmes in primary care in Stockholm. In this study, 61% of the included patients were graded GOLD stage > 3, which can limit external validity concerning primary care, but on the other hand, give valuable information on the patients with more severe COPD. Another strength was the collecting of data at follow-up, both at 10 weeks and 6 months, for more than 85% of the initially allocated patients. 70
The tutors were blinded regarding participant’s learning styles and inclusion outcomes, and all participants received the same content in the education and support in their exercise training, which was seen as a strength. 36 However, a limitation of the study was that the patients and tutors could not be blinded 70 to the intervention being in 2D or 3D.
Digital literacy could be an important factor when choosing an appropriate approach for using eHealth in PR.7,71 Despite being novel to education by 3D, participants in this study were using a computer on a regular basis, which could imply a certain level of digital literacy. The development of new models used in eHealth could comprise options to meet patients’ individual preferences and characteristics. 7 If the patients had impaired eye vision or if they had impaired stereopsis, i.e. the ability to use both their eyes, were not addressed and could have been affecting their perception of education by 3D, which was seen as a limitation. eHealth used in PR for COPD has shown some promising results and could be considered even in the most affected patients with long-term oxygen treatment 72 or as a complement to usual PR settings 73 where PR in 3D might be one of the alternatives.
In this study, assessments validated for COPD was used, 1 but self-efficacy was assessed with ESES, 50 not validated for COPD, which was a limitation. It has previously been shown to be a positive relationship between self-efficacy and HRQL, in COPD, and this is stronger for exercise self-efficacy than for general self-efficacy, 18 which is why ESES was used in this study. But, both low exercise-related self-efficacy and general self-efficacy can impact COPD treatment engagement negatively. 74 Therefore, a general self-efficacy measure could have been valuable since low self-efficacy also affects learning, and the current study is limited to results regarding self-efficacy related to exercise. However, as ESES was the only suitable self-efficacy assessment tool available in Swedish, this was used in the present study.
Conclusions
Three-dimensional techniques can be used in PR for COPD as an equivalent alternative to conventional techniques. Interactive 3D visualisation techniques were used in PR for patients with COPD, which resulted in no differences in outcomes regarding HRQL, 6MWT, ESES, and compliance to exercise, compliance to medication, or use of health care when compared to those using conventional 2D techniques. The most common learning mode and learning style were RO and divergent style, but since this was a small study sample, more research is needed before implementing this in PR in COPD. Moreover, knowledge is needed concerning patient's level of satisfaction with the education, factual knowledge of their condition, and motivation to use their knowledge.
Supplemental Material
sj-jpg-1-dhj-10.1177_20552076241308940 - Supplemental material for Interactive 3D visualisation technique used in pulmonary rehabilitation in chronic obstructive pulmonary disease: A randomised controlled study evaluating quality of life, compliance and use of health care
Supplemental material, sj-jpg-1-dhj-10.1177_20552076241308940 for Interactive 3D visualisation technique used in pulmonary rehabilitation in chronic obstructive pulmonary disease: A randomised controlled study evaluating quality of life, compliance and use of health care by Pernilla Sönnerfors, Anna-Karin Nordlin, Maria Nykvist, Ulrika Thunström and Ulrika Einarsson in DIGITAL HEALTH
Supplemental Material
sj-jpg-2-dhj-10.1177_20552076241308940 - Supplemental material for Interactive 3D visualisation technique used in pulmonary rehabilitation in chronic obstructive pulmonary disease: A randomised controlled study evaluating quality of life, compliance and use of health care
Supplemental material, sj-jpg-2-dhj-10.1177_20552076241308940 for Interactive 3D visualisation technique used in pulmonary rehabilitation in chronic obstructive pulmonary disease: A randomised controlled study evaluating quality of life, compliance and use of health care by Pernilla Sönnerfors, Anna-Karin Nordlin, Maria Nykvist, Ulrika Thunström and Ulrika Einarsson in DIGITAL HEALTH
Supplemental Material
sj-jpg-3-dhj-10.1177_20552076241308940 - Supplemental material for Interactive 3D visualisation technique used in pulmonary rehabilitation in chronic obstructive pulmonary disease: A randomised controlled study evaluating quality of life, compliance and use of health care
Supplemental material, sj-jpg-3-dhj-10.1177_20552076241308940 for Interactive 3D visualisation technique used in pulmonary rehabilitation in chronic obstructive pulmonary disease: A randomised controlled study evaluating quality of life, compliance and use of health care by Pernilla Sönnerfors, Anna-Karin Nordlin, Maria Nykvist, Ulrika Thunström and Ulrika Einarsson in DIGITAL HEALTH
Supplemental Material
sj-jpg-4-dhj-10.1177_20552076241308940 - Supplemental material for Interactive 3D visualisation technique used in pulmonary rehabilitation in chronic obstructive pulmonary disease: A randomised controlled study evaluating quality of life, compliance and use of health care
Supplemental material, sj-jpg-4-dhj-10.1177_20552076241308940 for Interactive 3D visualisation technique used in pulmonary rehabilitation in chronic obstructive pulmonary disease: A randomised controlled study evaluating quality of life, compliance and use of health care by Pernilla Sönnerfors, Anna-Karin Nordlin, Maria Nykvist, Ulrika Thunström and Ulrika Einarsson in DIGITAL HEALTH
Supplemental Material
sj-doc-5-dhj-10.1177_20552076241308940 - Supplemental material for Interactive 3D visualisation technique used in pulmonary rehabilitation in chronic obstructive pulmonary disease: A randomised controlled study evaluating quality of life, compliance and use of health care
Supplemental material, sj-doc-5-dhj-10.1177_20552076241308940 for Interactive 3D visualisation technique used in pulmonary rehabilitation in chronic obstructive pulmonary disease: A randomised controlled study evaluating quality of life, compliance and use of health care by Pernilla Sönnerfors, Anna-Karin Nordlin, Maria Nykvist, Ulrika Thunström and Ulrika Einarsson in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank all the patients in the study. Special thanks to Gun Faager, PhD, RPT, and to other colleagues at the Department of Physiotherapy at Karolinska University Hospital in Stockholm for helping with the study.
Consent for publication
Contributorship
All authors have made a substantial, direct, intellectual contribution to the concept or design of the article. A-KN and PS planned, designed, and participated in the development group of the 3D programme. UE planned and designed the study protocol. A-KN and UE contributed to the data collection. A-KN, PS, and UE conducted data analysis and interpretation of data. PS and UE wrote manuscript draft, and all authors revised it critically for important intellectual content of the manuscript and gave their approval to the final version of the manuscript to be published. All authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Data availability
The data generated during the study are not publicly available since the content of sensitive information could compromise the privacy of the participants. Data are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Regional Ethical Review Board in Stockholm approved an ethical application for the study (reg. no. 2013/1276-31/3) before the study was conducted. The study was registered in ClinicalTrials.gov (identifier: NCT02802618).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants through the Swedish Heart and Lung Association (grant numbers: E101/13, E118/14,E144-15), the Schörling Foundation, and the Department of Physiotherapy at Karolinska University Hospital.
Guarantor
UE.
Informed consent
All patients received oral and written information about the study and signed a letter of consent prior to participation. The study was performed according to the Declaration of Helsinki. 37
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.