
Abstract
In hospitals, oxygen is the most frequently administered medication to pediatric in-patients. Too much oxygen in arterial blood is not a natural occurrence, consequently hyperoxia can be caused by healthcare providers. The aim of this scoping study was to synthesize evidence that could contribute to safe and appropriate oxygen treatment in children 0–3 years of age. The method was in line with Arksey and O’Malley’s framework, and 11 research articles regarding oxygen treatment were included. The main results are presented as three key findings: 1) overview of assessing the need for oxygen based on the use of pulse oximetry, 2) overview of oxygen treatment, and 3) overview of the need for educational intervention. In conclusion, there is a shortage of research literature to guide nurses in assessment of oxygen requirements, and administration of oxygen treatment in critically ill children. Consensus and guidelines are needed, as there are variations in practice regarding oxygen treatment.
Introduction
Oxygen was discovered in the late 17th century and is considered to be the molecule of greatest importance for human beings. 1 In hospitals, oxygen is the most frequently administered medication to children in-patients2,3 and it is considered a potent and potentially toxic drug.4,5 It is a fact that the toxic nature of oxygen has been a cause for concern for more than 200 years, and that too much oxygen in arterial blood, hyperoxia, is caused by healthcare professionals, as it does not occur in nature. 6 Healthcare professionals need to be aware that too much oxygen supplementation may cause hyperoxia, 7 and that excessive oxygen is the only cause for hyperoxia in critically ill infants. 8 In clinical practice, uncritical usage of supplemental oxygen and limited knowledge regarding hyperoxia have both been observed. Oxygen should be administered according to the patient’s requirements, but this is not always done in practice. 3
Challenges related to hyperoxia
In neonates at birth the normal limit for arterial pressure of oxygen (PaO2) is 8.0–10.7 kPa and in children it is 10.7–13.3 kPa. 9 Thus, hyperoxia is defined as arterial oxygen tension above 10.7 kPa in full-term newborns, 10 and above 13.3 kPa among children.9,11 Oxygen toxicity can result from high levels of the fraction of inspired oxygen (FiO2), which increases the risk of absorption atelectasis 12 and may lead to vasoconstriction, lower heart rate and increased blood pressure.1,13 Hyperoxia leads to free oxygen radicals as a result of more oxygen molecules being added than each hemoglobin molecule can carry.4,14 This may lead to oxidative stress, defined as an imbalance between prooxidant and antioxidant forces in the body. 15 Oxidative stress is associated with both tissue damage and DNA damage, and cell death is a prominent feature of hyperoxia-induced lung injury.4,16,17 Additionally, hyperoxia may lead to the release of a cascade of harmful chemicals in certain parts of the brain, possibly influencing central nervous functions. 13 Research indicates a possible association between administering high levels of FiO2 and increased hospital mortality in critically ill patients. 18 However, there seems to be more awareness about the risk of hyperoxia in premature newborns and less attention is paid to full-term newborns. 19
Assessing the oxygen treatment
Physicians have a legal responsibility for oxygen treatment, 7 but nurses are responsible for titrating oxygen within prescribed limits of oxygen saturation.20,21 Both theoretical and practical knowledge of pulse oximetry are necessary during assessment of oxygen requirements in pediatric patients. 22 In addition, the placement of the oximetry probe is important.23–25 Pulse oximetry alone has its limitations, 22 therefore the best method to both assess oxygen requirements, and detect hyperoxia or hypoxia is by assessing the arterial blood gases. 26 The accuracy even of newer generations of pulse oximeters is poor when used on newborn infants. 27 Clinical conditions such as low perfusion, patient motion artifacts, cardiac arrhythmias and shivering could also result in poor signal quality of the pulse oximeter. 28 In order to assess oxygenation correctly, an understanding of the hemoglobin–oxygen dissociation curve (Hb–O2 curve) and of the relationship between PaO2 and oxygen saturation (SpO2) is required. 21 The dynamic of the Hb–O2 curve will depend on pH, arterial pressure of carbon dioxide (PaCO2), PaO2, temperature, hemoglobin and the enzyme 2,3-diphosphoglycerate. 29 As the Hb–O2 curve refers to the hemoglobin affinity for oxygen, the hemoglobin will bind oxygen more strongly if PaO2 is low, which results in less oxygen released to the tissue. 21 Clinical observations and the patient’s condition may affect the results as well. 30 Nurses also need to be aware that changes to the child’s position could make a difference in the oxygenation status, as children have less ‘surface of gas exchange’ than adults. 31
In addition, if nurses add oxygen without knowing that SpO2 > 95% may lead to high levels of PaO2, the child could be exposed to potential danger. 3 Exposure to pure oxygen, even briefly when SpO2 > 95%, is not recommended, and use of blenders could enable healthcare professionals to achieve FiO2 control and avoid unnecessary use of 100% oxygen. 4 The British National Formulary for Children recommends that SpO2 is maintained at >92% among most critically ill children, but also points out that some clinicians may aim for a target of 94–98%. 32 Appropriate oxygenation in ventilated children could be achieved by titrating FiO2 and regulating the mean airway pressure (MAP). To regulate MAP, the physician may use peak inspiratory pressure (PIP), positive end-expiratory pressure (PEEP) or inspiratory time (TI).7,19 Since physicians have the legal responsibility for decision-making in patient treatment and the opportunity to delegate responsibility to nurses, interprofessional collaboration is a necessity. 7
To summarize, there is a great deal of information available about the significance and risks of using oxygen in premature newborns. We also know that the use of pulse oximetry to assess patients’ need for oxygen has its limitations. In children aged 0–3 years, however, we see that there is uncritical usage of supplemental oxygen and limited knowledge regarding hyperoxia. The aim of this study was therefore to synthesize evidence that could contribute to safe and appropriate oxygen treatment in children 0–3 years of age. The research questions were:
What is known from existing literature about oxygen treatment in children aged 0–3 years receiving supplemental oxygen? What does the evidence tell us about how to improve nurses’ knowledge of assessing children’s need for oxygen?
Method
This article is based on a scoping study of current research literature. A scoping study is used to explore gaps, and map key concepts and types of evidence in research related to a defined field or area by systematically searching for, selecting and synthesizing existing knowledge. 33 This methodology is appropriate to synthesize evidence that can influence guidelines and practice, 33 in this case in pediatric intensive care units (PICUs). Scoping studies also tend to focus on the breadth rather than the depth of literature, 34 and many different study designs might be applicable. 35 When searching for literature, the methodological framework outlined in Arksey and O’Malley was adapted, which means a five-stage approach: 1) identifying the research question, 2) identifying relevant studies, 3) study selection, 4) charting data, 5) collating, summarizing and reporting the results. 35
Eligibility criteria
Articles were included if they contained information about oxygen treatment of children aged 0–3 years, between 2004 and February 2016. Also included were articles with information about how to improve nurses’ knowledge of assessing patients need for oxygen. Studies conducted on premature children were included if they covered nursing assessment in oxygen treatment directly transferable to full-term newborns (0 years of age).
Articles were excluded if they lacked relevance from a nursing perspective, such as manikin, in vitro studies and animal studies. Furthermore, articles that focused on oxygen therapy and different medical conditions such as acute respiratory failure and congenital heart disease, or articles that compared different pulse oximeters, were excluded. The searches were also limited to articles in English or Scandinavian languages.
Literature search to identify relevant studies
Single and combined search terms.
Study selection
The literature search produced a total of 1653 articles. We performed the first-level selection of literature by reading through all the titles, and also abstracts where the title did not clearly state the content of the article. At this step, we excluded comments, letters, conference notes and editorial articles, thus narrowing down the selection of articles to 40. Articles were only included if they addressed any aspect that could contribute to awareness of how nurses may evaluate safe and appropriate oxygen treatment in children. At the second-level selection, we discarded 10 duplicate articles. The remaining 30 articles were then read thoroughly, and after this third-level selection we were left with 11 research articles to include in our scoping study. The included literature was read thoroughly by the first author, judged using standard Norwegian checklists for research articles, following their recommendations regarding aim, research questions, research design and data collection. 36 The checklists have been developed by the national Public Health Institute’s Centre of Knowledge for the Health Service to evaluate the methodological quality and the reliability of results within research articles. 36 The 11 articles were deemed of high enough quality to include in the study.
Collating, summarizing and reporting the results
This stage involved mapping key items of information obtained from research literature as recommended in the scoping study framework. 35 We took a narrative approach during the reading process, to identify key themes. In order to present an overview of existing literature, we needed some thematic categories,35,37 and so we organized the included literature according to their key findings. Subsequently we collated and summarized all information in tables, including author(s), aim, design and methodology, study population, and key findings based on the framework’s approach. 35
Results
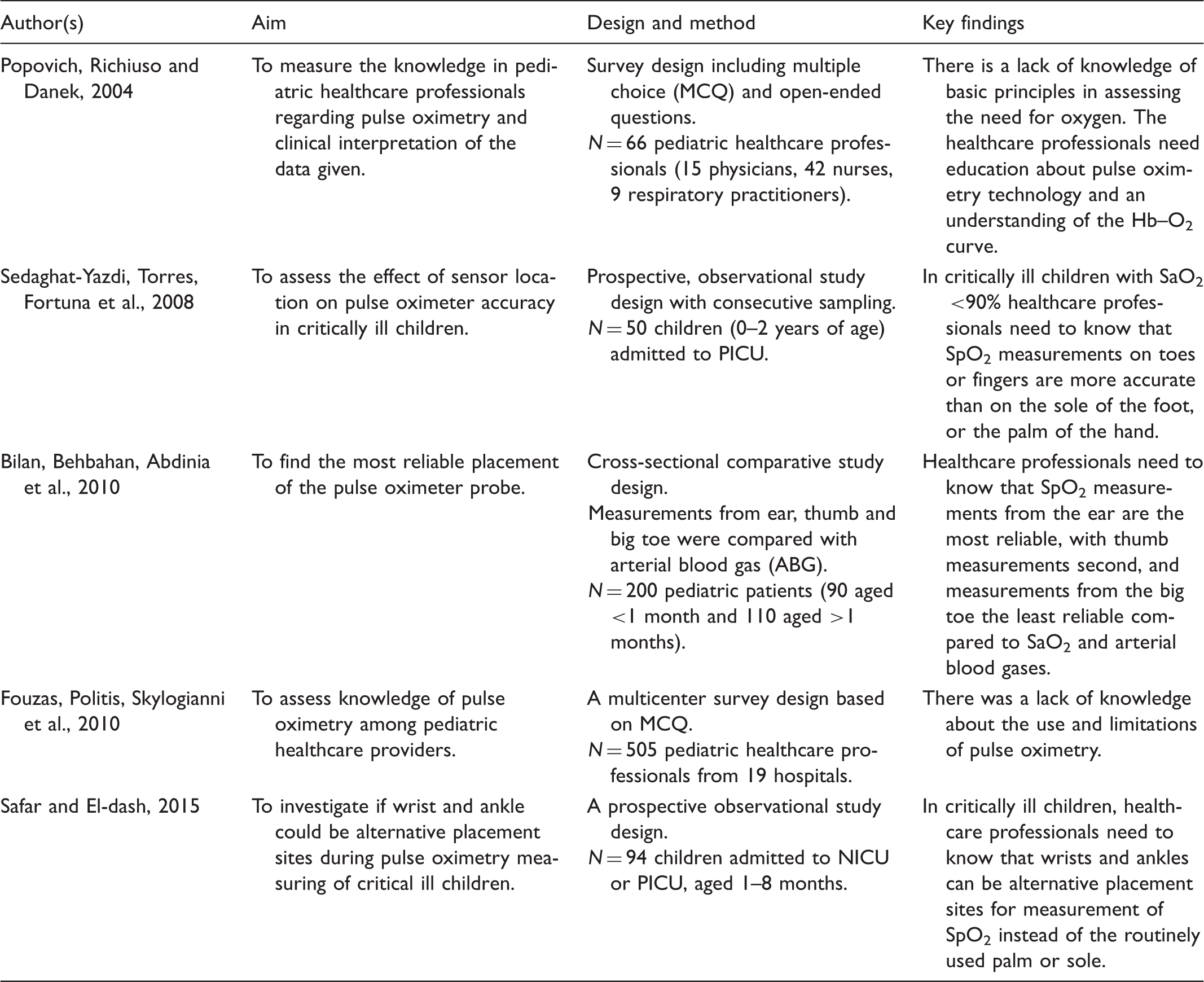
Overview of assessing the need for oxygen based on the use of pulse oximetry.
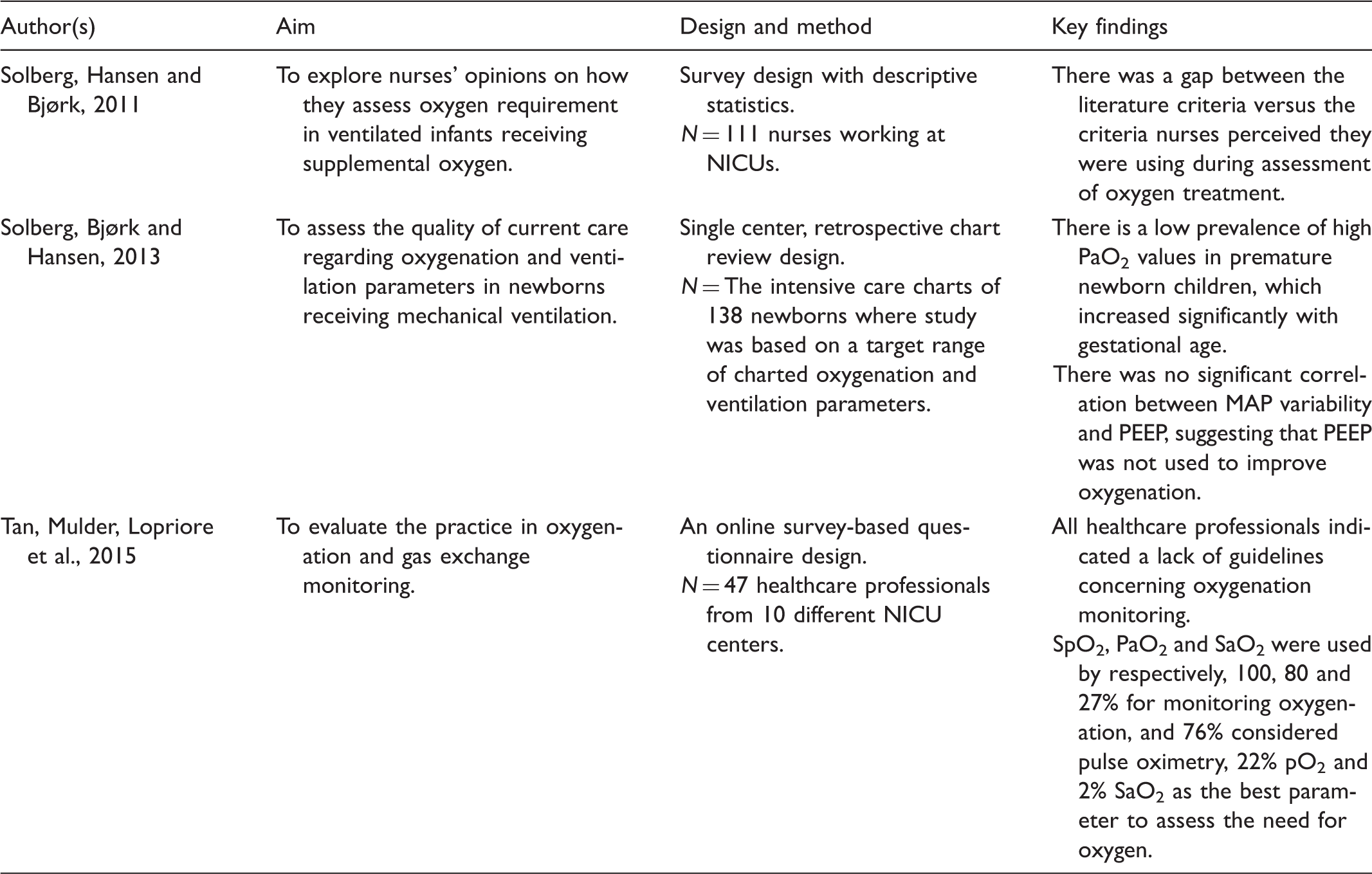
Overview of oxygen treatment.
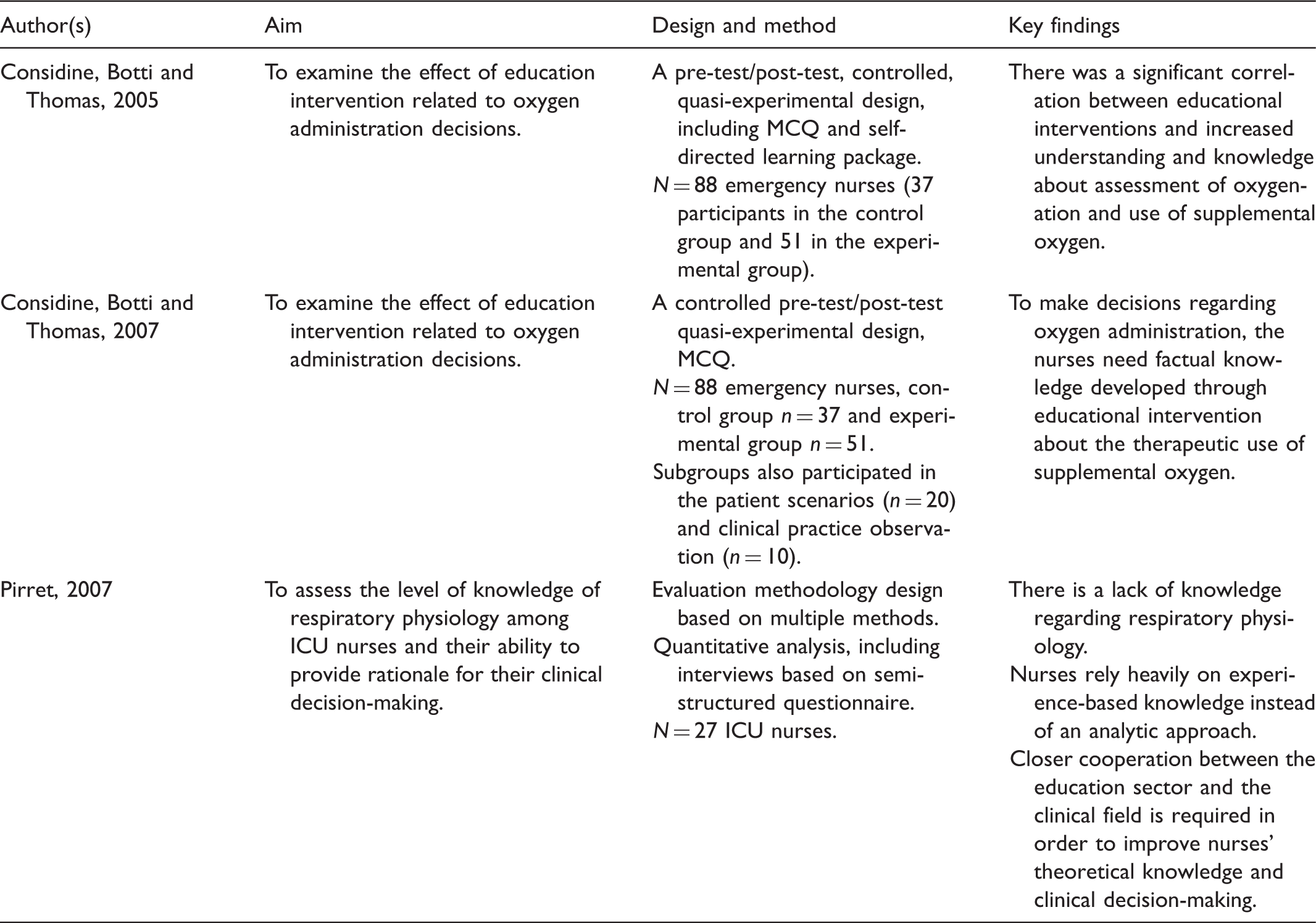
Overview of the need for educational intervention.
The main findings from this scoping study are articles which present pulse oximetry as a noninvasive tool to assess the need for oxygen in children.22–24,38 In order to rely on the monitored saturation, the authors emphasize the impact of correct probe placement.22,23,25 In addition, both theoretical and practical knowledge of pulse oximetry are needed during assessment of oxygenation in pediatric patients.24,38 There seems to be a gap between literature recommendations and existing knowledge among pediatric healthcare professionals regarding the use of pulse oximetry22,38 and correct understanding of the Hb–O2 curve.21,38 This highlights the necessity of an adequate knowledge base for nurses, enabling them to make appropriate assessments during oxygen treatment of critically ill children.
Assessment of oxygen requirement in children is based on insufficient information among nurses. 21 In order to improve oxygenation in newborns, one study found that there was no significant correlation between MAP variability and PEEP, which suggests that changing PEEP was not used as a strategy to adjust MAP. 19 Furthermore, newborns at term were at higher risk for hyperoxia than preterm, as low prevalence of high PaO2 values in premature infants increased significantly with gestational age. 19 This could indicate greater knowledge and awareness of the toxic effect of high oxygen concentrations on the prematurely newborn, with less attention being paid to full-term newborns. But a wide variation in preference in oxygenation monitoring exists both within and between units. 26
The scoping study found that educational interventions contribute to an increased understanding and knowledge of the complexity of the respiratory system.41–43 There is a need for an analytical approach to nurses’ assessment in order to contribute to professionally sound decision-making. 43 In addition, a closer relationship between the clinical field and the education programs in developing nurses in intensive care units (ICUs) is found to be important. 43
Discussion
Assessing oxygenation based on the use of pulse oximetry
We found that one characteristic of assessing oxygenation is a high reliance on the use of pulse oximetry21,26 and that the placement of the probe influences the result (Tables 2 and 3).23-25 Taking SpO2 measurements on toes or fingers might be more accurate than on the sole of the foot, or palm of the hand. 24 Furthermore, SpO2 measurements on the ear appear to be the most reliable, with thumb measurements second, and measurements on the big toe the least reliable compared to saturation in arterial blood gases (SaO2). 23 Nurses also need to be aware that wrists and ankles can be alternative placement sites for measurement of SpO2. 25 When faced with a range of different recommendations, it can be difficult for the nurse to know which results can be relied upon. A study indicates that educated ICU nurses seem to have more basic SpO2 knowledge based on their ability to correctly assess pulse oximetry values within the context of technological limitations. 28 As pulse oximetry alone has its limitations 22 arterial blood gas analysis is the most important and reliable way to assess oxygen requirements in critically ill patients.26,44,45 It is worrying that, despite the known limitations of using pulse oximetry, the majority of the articles we found on children had this as their main focus. This highlights the need for more articles about the more reliable methods of assessing oxygen requirements.
When assessing blood gases together with the SpO2, nurses in PICUs also need to be familiar with the dynamic of the Hb–O2 curve.4,46 For example, if a newborn has no clothes on during procedures and therefore gets cold, there may be metabolic consequences for the child, such as increased oxygen consumption. 47 Since newborns have a lot of fetal hemoglobin, the oxygen will have a stronger binding to the hemoglobin, 48 and when coinciding with hypothermia this leads to a curve tilted leftward, which could lead to quickly reduced SpO2 levels.4,21 In clinical practice, nurses have been observed adding or increasing FiO2 without checking the child’s temperature and the dynamic of the Hb–O2 curve. If oxygen is added without increasing the body temperature, the oxygen treatment may be inappropriate. Thus, the challenge becomes titrating correct FiO2 by considering the Hb–O2 curve together with the clinical condition of the child to prevent hypoxia as well as hyperoxia. It is also necessary to avoid fluctuations of SpO2, therefore titration should be performed with caution 3 and if an increase of 10% is much more than needed, hyperoxia occurs in seconds. 49 According to legislation, nurses should prevent patients being harmed by the treatment provided, 50 and by considering all aspects of respiratory physiology, the child’s position, state of illness and clinical condition, one will practice nursing based on an analytical approach at a high cognitive level.
Oxygen assessment, and the need for educational intervention
We discovered that lack of knowledge was a consistent finding from this scoping study, including of respiratory physiology, 43 basic principles in assessing oxygenation, 38 the use and limitations of pulse oximetry, 22 criteria regarding blood gases sampling, 44 assessing criteria from the literature21,26 and the use of PEEP to improve oxygenation in pediatric patients. 19 We also identified a lack of guidelines concerning oxygenation monitoring, 26 and found that educational interventions that increase knowledge will further improve clinical decision-making regarding oxygenation assessment and use of supplemental oxygen (Table 4).41,42
Knowledge of respiratory physiology and pathophysiology that increases professional expertise contributes to improved patient outcomes. 43 Furthermore, the ability to articulate analytical decision-making processes may enhance the clinical credibility of ICU nurses. 43 The understanding that prolonged oxygen treatment could be harmful to premature infants dates back over 60 years, but recently we have come to realize that even brief exposure to oxygen causes damage to full-term newborns as well. 51 Since few studies have been conducted regarding oxygen requirements in children 0–3 years of age, it is challenging to assess children given supplemental oxygen. Nevertheless, it has been possible to detect the toxic effects of oxygen in adults for over 40 years, 52 and Saugstad has documented the adverse effects of oxygen in premature and sick newborns between the same decade and the present date. 17 Therefore, nurses may be able to assess safe and appropriate oxygen treatment according to need based on literature recommendations and an analytical approach rather than experience-based judgment alone.
Findings from this scoping study indicate a wide variety of preferences in oxygenation monitoring both within and between units, and a lack of guidelines (Table 3). 26 Although clear guidelines combined with the development of clinical judgment are recommended on a general basis, 53 and despite the toxic nature of oxygen, it is a paradox that no consensus exists, nor evidence to guide nurses during administration of oxygen in full-term newborns. 19 Sola et al. argue that if oxygen had been discovered today, national and international drug agencies would have prepared stricter guidelines for the use of supplemental oxygen. 4 Developing guidelines that are evidence-based as well as practical, can contribute to establishing consensus regarding administration and titration of oxygen treatment in critically ill children. 26 In order to ensure the quality of oxygen treatment, established criteria are needed. 54 Additionally, increased knowledge gained through educational interventions seems to be necessary.41,42 Researchers also emphasize that clinical practice should be based on empirical data instead of old traditions. 53
There are limitations to this study. Only the first author has performed the selection of included articles, and gone through checklists in order to judge the included articles’ aim, research questions, research design, and data collection. Nevertheless, tables 2–4 show that the included articles present a specific aim, sample size and important key findings.
Conclusion
Based on the findings of the articles included in this scoping study, nurses need factual knowledge developed through educational intervention in order to safely administer supplemental oxygen. When assessing oxygen treatment, an analytical approach is preferred, using pulse oximetry, arterial blood gases analysis, the dynamic of the Hb–O2 curve, respiratory physiology and the patient’s clinical condition. This study concludes that there is a shortage of research literature to guide nurses in assessment of oxygen requirements, and administration of oxygen treatment in critically ill children. Consensus and guidelines are needed, as there are variations in practice regarding oxygen treatment.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.