
Abstract
Discussions on how nursing documentation should be carried out have been ongoing for the last decade. In this study, free-text format for nursing diagnoses was introduced to nursing staff at a university hospital in Norway. The aim of the study was to investigate the impact of an education intervention introducing nursing diagnoses in a free-text format following a problem-etiology-symptom structure. A pretest–posttest design was performed to assess changes in quality and quantity in the nursing documentation using the audit instrument N-Catch II. Several elements in the nursing documentation had statistically significant changes; the largest was found for quantity in nursing diagnoses. Education interventions aimed to improve nurses’ documentation in the electronic health record may have an effect on more complete and accurate nursing documentation. The presented education intervention showed a significant impact of more accurate nursing diagnoses and significant improvements in nursing documentation.
Introduction
The ability to document patients’ responses to illness as well as information on the given care, is cited as a core competence within nursing.1,2 Although nurses have documented their interventions and results for a long time, there is still criticism around low quality and incompleteness in their documentation.2–4 Expectations of higher quality and more complete patient records followed the introduction of electronic health records (EHRs). 5 As the format of these invites a greater use of structured and standardized language, discussions on how nursing documentation should be carried out have followed the introduction of EHRs and have been ongoing for the last decade.4,6,7 However, nursing documentation is still pointed to as being incomplete and inaccurate, implying that the new expectations have not been met.8,9 In addition, recent research displays an apparent correlation between high quality nursing documentation and patient safety, emphasizing the nursing documentation’s significance for high quality care. 10 This is also mirrored in statements about poor documentation causing misunderstandings and misinterpretations leading to unsafe patient situations in addition to longer hospital stays and increased costs.10,11
Although there is no international gold standard for measuring the accuracy of nursing documentation, the stages of the nursing process are acknowledged as having the theoretical elements needed for accurate nursing documentation.12,13 The nursing process allowing nurses to evaluate nursing outcomes as a logical result of nursing diagnoses and interventions, can result in accurate nursing documentation when the elements admission data, nursing diagnoses, interventions, progress and outcome evaluations, are addressed.12,14 Hence, the theoretical framework for accurate and complete nursing documentation is available through the nursing process.
Further, nursing diagnosis has been pointed to as being a central component in the nursing process, acting as foundation for planning, implementing and evaluating nursing care.11,15,16 A nursing diagnosis can be defined as a ‘clinical judgment about an individual, a family or a community’s responses to actual and potential health problems and life process’. 17(p. 94) This makes nursing diagnoses the basis for selecting nursing interventions underlining correlations between accurate nursing diagnoses and given care.11,15 Nursing diagnoses can be used in both paper-based and electronic records, and with or without classification systems. The problem-etiology-symptom structure (PES) is an internationally recognized structure for nursing diagnosis consisting of the elements: problem/health need, etiology, and symptom. The PES structure is independent of existing classification systems and is applicable in free-text format as well as standardized classification use.12,17 Implementation of free-text format nursing diagnoses is pointed to as promoting nurses’ diagnostic process and described as useful for affecting completeness in nursing care plans in addition to increasing focus on nursing documentation in general. 15 Pointing to nursing diagnoses as central in the nursing process makes this element significant to address in education and training in performing nursing documentation.18 Other studies describing education interventions featuring nursing diagnoses have also emphasized the connection between nursing diagnoses and clinical reasoning.19–21
Our intervention followed a PES structure in introducing the concept of nursing diagnoses. This structure is internationally recognized as holding the central elements needed to concentrate the essence of a health problem or need. The element P (problem) describes the identified health need or problem, the E element (etiology) discloses possible factors related to the problem and the S (symptom) gives information on symptoms underlining/emphasizing the problem or what the problem leads to. The aim is to establish an individualized diagnostic statement.12,13,22,23 An example of a nursing diagnosis is described by Ehnfors et al. as: Troubled sleep (P) related to itching (E) leads to tiredness and anxiety during the daytime (S).23(p.105)
The PES structure is independent of any existing classification use.12,17 Implementation of free-text format nursing diagnoses is pointed out as a means of promoting nurses’ diagnostic process. As nursing documentation frequently is described as being of poor quality, there is a need for more knowledge about how to best support nurses translating the theoretical framework into an applicable working tool. Internationally, several studies have addressed the shortcomings in nursing documentation.1,2,19,22,24 The studies involve education interventions emphasizing clinical reasoning to translate the theoretical framework available through the nursing process into the EHRs. Even though the interventions point to improvements in the nursing documentation, there is still a need for more knowledge on easily feasible interventions to be carried out in clinical practice achieving nursing documentation of good quality, in accordance with legislation and nurses’ needs for working tools.18
This was the starting point for collaboration between a nursing faculty and a university hospital in central Norway establishing a research project to implement nursing diagnoses as a common component in nurses’ documentation. The joint research project aimed to explore an education intervention implementing free-text format nursing diagnoses in a medical department due to the importance of nursing diagnoses in documentation. The main intention was to improve the accuracy and completeness in nursing documentation by giving the nurses knowledge of and training in how to formulate applicable and useful nursing diagnoses statements, eventually resulting in better care. This article reports the impact of the intervention expressed as changes in the EHR assessed with a Norwegian version of the audit instrument D-Catch,11,12 namely N-Catch II.22,25
Aim
The aim of the study was to investigate the impact of implementing nursing diagnoses in a free-text format at a medical department by means of an education intervention. The outcomes presented in this article are changes as expressed in quality and quantity of the nursing documentation assessed with the audit instrument, N-Catch II.
Methods
Design
This is a quasi-experimental study using a pretest–posttest design without control group. 26
Setting
The medical department involved in the study consisted of four separate units holding a total of 41 beds. In 2013, the university hospital had 59,016 hospitalizations and 993 beds. The nursing staff of the four units involved in the study consisted of 101 registered nurses and assistant nurses. In the study, 72 members of staff participated in the education intervention teaching sessions – 62 nurses and 10 assistant nurses. All members of staff received peer support from the nurse key personnel in the guidance and follow-up phase. The work experience of the nursing staff ranged from 1 to 41 years, with a median of 8 years. The majority of the participants’ employment percentage was more than 60%.
The education intervention
Hospitals in central Norway had no integrated classification system for nurses in the EHR at the time. Therefore, an education intervention presenting nursing diagnoses in free-text format following a PES structure was initiated.
The education intervention.
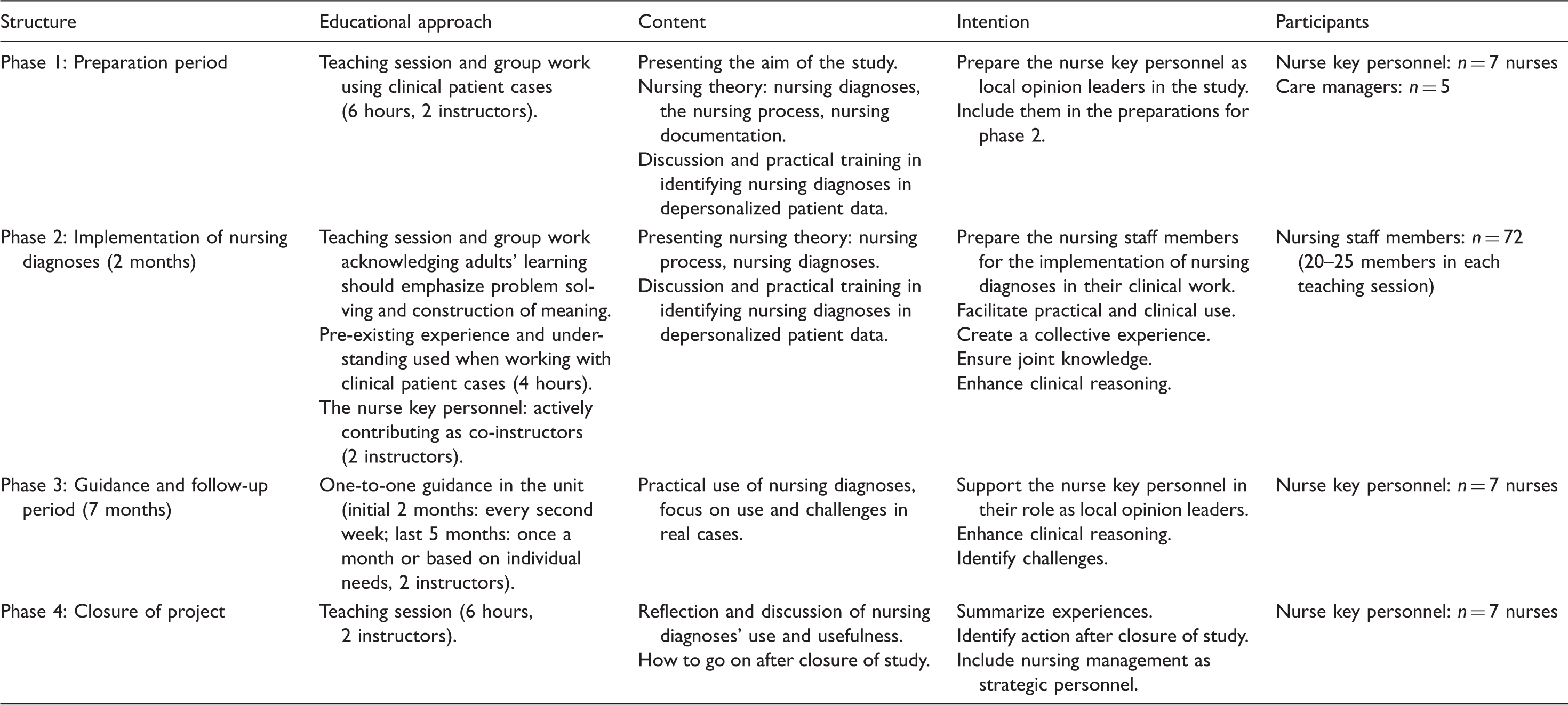
A number of key personnel participated as local opinion leaders in order to promote the implementation process. The concept of EHR-nurse key personnel defines an additional role to the ordinary nursing role, and is described by the hospital itself as a nurse appointed by the nursing management who has completed specific training, with thorough knowledge of nursing documentation and with a special task to instruct and supervise other nurses. These nurses received additional educational measures and training, and acted as resource agents within their department. This is in accordance with current recommendations on implementation concerning health research.27,28 The education intervention lasted nine months. The teaching sessions aiming to cover all staff members were carried out during the two initial months, whereas the continuing guidance and follow-up period targeting the nurse key personnel lasted seven months.
Sample
A sample of nursing documentation extracts from the electronic health records (EHRs) was assessed for performing pretest–posttest statistics investigating the impact of the education intervention. Nursing documentation for the pretest was collected one year prior to the intervention to avoid bias. For the posttest, records were retrieved one month after the intervention ended. Inclusion criteria for the records implied a length of stay of 48 hours or more. Further, that the patient should be both admitted and discharged from the same medical department. With a 5% margin of error (95% confidence interval), the sample size was calculated to be 45 in each group. As the education intervention gathered nurses from all of the four units in the department, our intention was to investigate changes at an organizational level. Therefore, the records were consecutively sampled from the department’s hospitalizations in the chosen period. To allow exclusion of records not meeting the inclusion criteria nursing documentation extracts from 50 records were collected for each measurement giving a total sample size of 100 records.
Audit instrument
In order to identify essential improvement areas of nurses’ documentation, audit instruments are required. 29 In this study, the audit instrument N-Catch II was used to assess quality and quantity in nursing documentation. This is a Norwegian version of the audit instrument Dutch-Catch (D-Catch) that was developed for assessing nursing documentation in hospitals building on the audit instruments Cat-ch-Ing and Scale for Degrees of Accuracy in nursing diagnosis.24,25,29 The instrument is translated and culturally adjusted to Norwegian legislation and practice according to scientific criteria.22,24,25 An early version of the instrument has been used in other studies,9,30 but the updated version has not to our knowledge been applied.
N-Catch II consists of eight items assessing aspects of both quality and quantity. The items correspond with the steps in the nursing process comprising: assessment, nursing care plan with nursing diagnoses, aim and interventions, and evaluation in terms of progress and evaluation notes. The different items are scored on a scale from 0 to 3 (for most items) with 3 points representing the highest score. The patients’ personal data are scored on a scale from 0 to 2 points, making 2 points the highest score for this item.
The N-Catch II implies two different options for assessing nursing diagnoses, namely by emphasizing the International Organization for Standardization (ISO) model and its description for nursing diagnoses, or by using the PES structure when formulating nursing diagnoses. As our education intervention implemented the PES structure, only this option in the N-Catch II was applied. The reviewers used the guideline for the audit instrument N-Catch II through the process of scoring quantity and quality. A set of criteria supported the reviewers in their work. In order to for example achieve a 3-point quantity score for the item ‘nursing diagnoses’, the three elements of a nursing diagnosis must be present along with at least one defined nursing intervention in the nursing care plan. In order to achieve a 3-point quality score, the nursing diagnosis must be relevant, concise/precise, specific and formulated in proper language.
Pretest calculations, records n = 49.
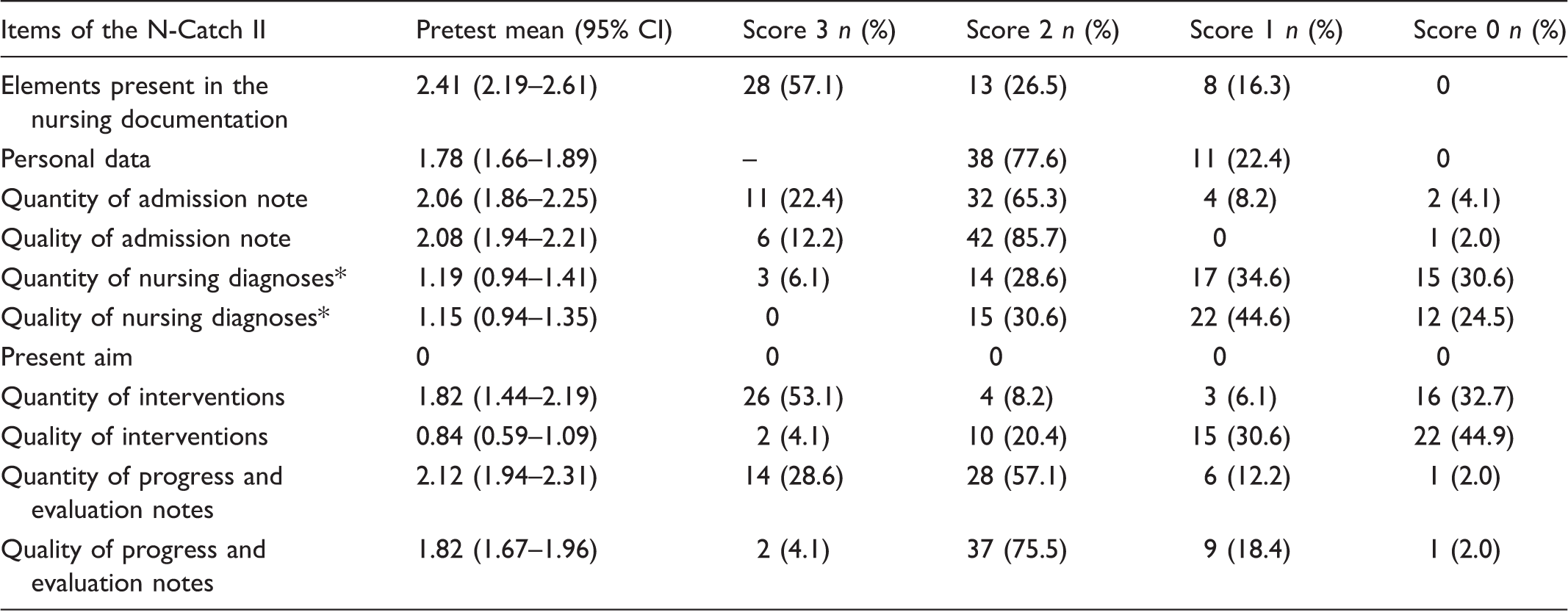
A mean score for all diagnoses present in the assessed patient record was calculated. In the table the following simplifications were made: 0 to 0.5 = 0 p; 1 to 1.99 = 1p; 2 to 2.99 = 2 p; 3 = 3 p.
Data collection
Retrieval of nursing documentation from EHRs was carried out by a nurse from the hospital according to the inclusion criteria, drawing the first record from a given date and moving forward, giving a consecutive sample. The records were collected from the department’s list of hospitalizations, not focusing on a specific number of records from each of the department’s units. This approach was chosen as the aim was to investigate changes in the nursing documentation at an organizational level without considering differences between the units. The nurse scored the patients’ personal details and then removed identifying information before handing over copies to the reviewers.
The two reviewers (first and second author) assessed the nursing documentation using N-Catch II and its guideline. The two reviewers assessed the nursing documentation independently of each other following a number of steps in order to achieve common understanding of the audit instrument and its guideline. Initially, five randomly selected records were assessed separately, compared and discussed until consensus was achieved and the two reviewers were calibrated as suggested in the N-Catch II guideline. The next 45 records were scored separately before comparing scores and achieving consensus. The same procedure was repeated for the last 50 records. In discussion of scores, the guideline was applied and a common understanding of the total audit instrument was established. Both separate scores and consensus scores were registered. The reviewers found one of the records did not meet the inclusion criteria and excluded it from the analysis.
Data analysis
The measurements in the study are treated on an ordinal level. 31 The response data were observations on the same elements in the nursing documentation from two independent reviewers scored in mutually exclusive categories. Frequencies, means with confidence intervals and change in mean values were calculated for all elements addressed in the N-Catch II. Each present nursing diagnosis was individually scored on quantity and quality before calculating a mean of all nursing diagnoses in the specific record. To compare calculations from pretest and posttest, a Wilcoxon Mann–Whitney test was performed.26,32 The cut-off level for statistical significance was taken at p ≤ 0.05 and a 95% confidence interval. For statistical analysis the statistical software IBM SPSS, version 22 was used.
Ethical considerations
The Regional Committees for Medical and Health Research Ethics in central Norway considered the project as a quality study not in need of their approval. Hence, application was laid before the privacy ombudsman acting as local data protection official for research at the university hospital. The study was approved to be carried out without patient consent as only anonymous data were used. In addition, the head of the department authorized the study. Prior to the study, nurses at the department were informed about the project study methods and aims.
Results
Nursing documentation in a total of 99 EHRs, comprising 49 records before and 50 after the education intervention, were assessed using the audit instrument N-Catch II. In the pretest documentation from one year prior to the intervention, the highest score and accuracy was found for the item ‘elements present in the nursing documentation’. The mean score for this item was 2.41 (95% CI 2.19 to 2.61) and 28 of the records were fully accurate (scored with 3 points). None of the records scored 0 points on this element. Admission notes were of both good quantity and quality with the majority of the records scoring 3 or 2 points. The lowest score was found for the item ‘present aim’ as none of the records had this element, giving the mean result 0 points.
The intervention in the study aimed to implement nursing diagnoses in free-text format with PES structure. The pretest assessment of quality and quantity in nursing diagnoses gave a result with the mean 1.19 (95% CI 0.94 to 1.41) for the qualitative aspect and 1.15 (95% CI 0.94 to 1.35) for the quantitative aspect respectively. The nurses did not intentionally apply the PES structure prior to the intervention study, but the N-Catch II guideline made formulations similar to the PES structure possible to assess as partial nursing diagnoses. Three records scored according to complete accuracy on the quantity of nursing diagnoses but none scored 3 points on quality. The majority of the records scored 1 or 0 for both quality and quantity in nursing diagnoses. The following examples illustrate different nursing diagnoses and their scores in the pretest assessment. As these were formulated before the intervention, they are not written in a structured way but more as diagnostic statements: ‘Reduced general condition after falling and becoming dehydrated’ – This statement holds the elements of a nursing diagnosis yielding 3 points for quantity, but is vague in its description giving 2 points for quality. ‘Swollen feet’ – According to the criteria, this does not hold the elements of a nursing diagnosis except for the description of the problem and is therefore given 0 points for quantity, but 1 point for quality as it gives some information about the patient’s problem.
Posttest calculations, records n = 50.
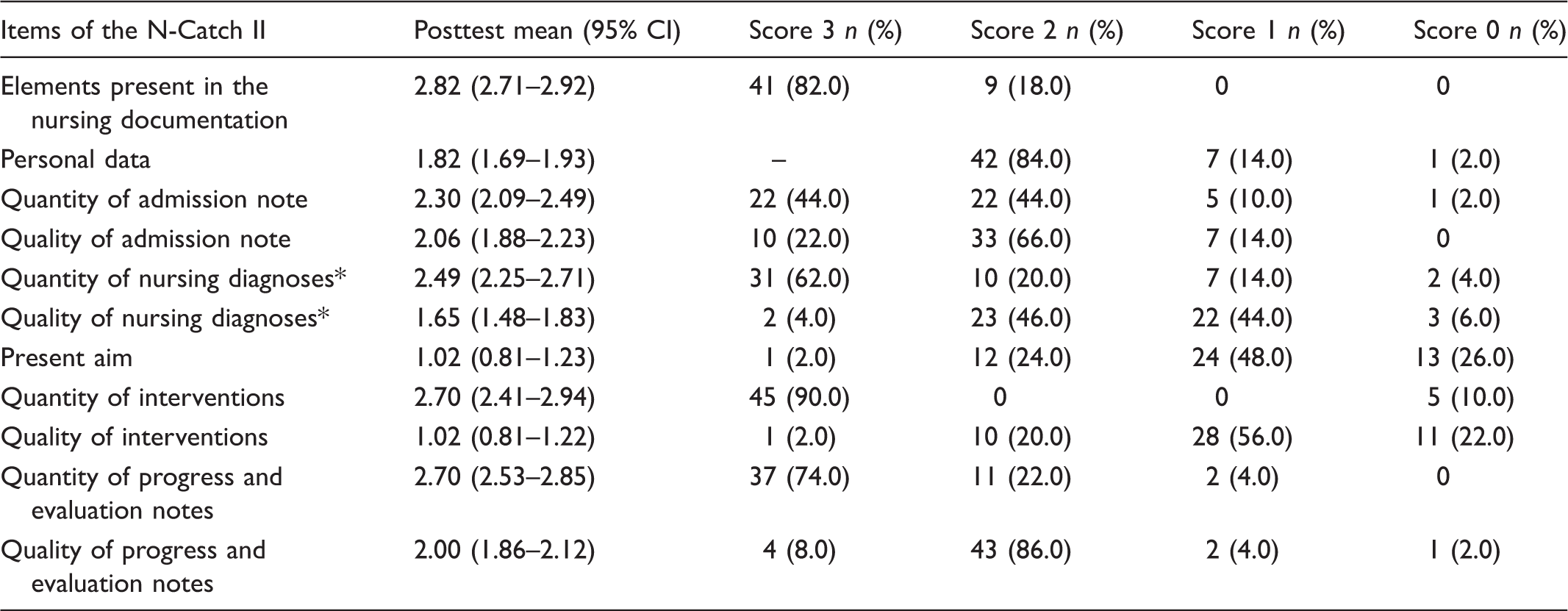
A mean score for all diagnoses present in the assessed patient record was calculated. In the table the following simplifications are made: 0 to 0.5 = 0 p; 1 to 1.99 = 1p; 2 to 2.99 = 2 p; 3 = 3 p.
Posttest calculations on nursing diagnoses disclosed a mean score of 2.49 for the quantitative aspect and 1.65 for the qualitative aspect, respectively. Higher accuracy was found for the quantitative aspect regarding the content described in the actual diagnosis. Complete accuracy on quantity in nursing diagnoses was found in 31 of the records (62%). Accuracy for the item interventions was high for quantity where 90% of the records scored 3 points, but only 2% scored 3 points for quality. The following examples illustrate the posttest assessment and illustrate different nursing diagnoses’ scores. Due to the project’s focus on nursing diagnoses, descriptions of nursing interventions are not included in these examples: ‘Low appetite (P) related to nausea (E) leads to low calorie intake and tiredness’ – This nursing diagnosis contains the three elements in a PES structure giving 3 points for quantity, but is imprecise in terms of patient details and is therefore given 2 points for quality. ‘Pain (P) related to pulmonary cancer (E) leads to low mobility, low appetite, nausea, low quality of life’ – This nursing diagnosis fulfils the criteria of three elements in a PES structure and gets 3 points for the quantity score, but is imprecise in terms of localization and details of the pain and therefore given 2 points for quality. ‘Diarrhea (P) related to AB (antibiotic) treatment? (E) leads to discomfort’ – The lack of a nursing intervention explains the 2-point quantity score. Imprecise PES elements and lack of detail result in a 1-point quality score.
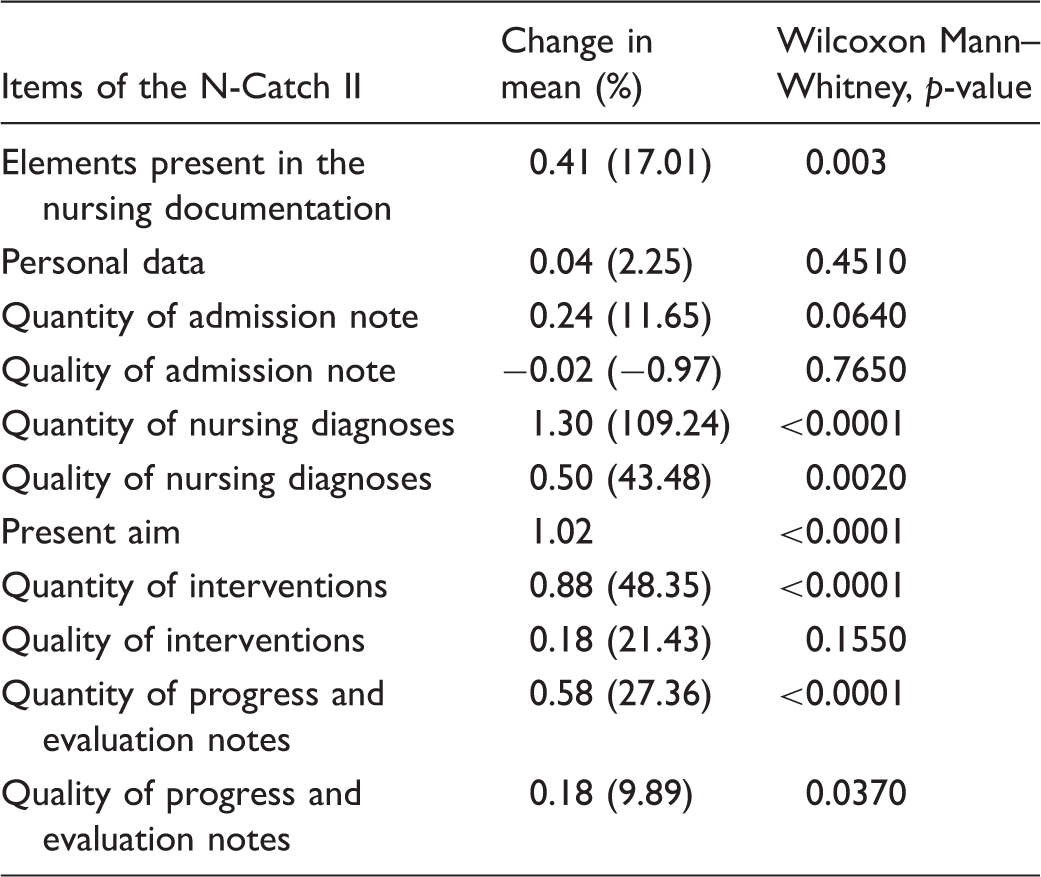
Impact of the intervention was investigated as changes in the nursing documentation by comparing the pretest and the posttest. The largest changes in percentage were found for the items ‘quantity of nursing diagnoses’, and ‘quantity of interventions’. For quantity of nursing diagnoses, the mean value for the item increased by 1.3 points. In addition, for the qualitative aspect of nursing diagnoses there was a positive change with a 0.5 increase in mean points. Several of the elements in the nursing documentation showed significant changes when comparing the pretest and the posttest. In addition to ‘elements present in the nursing documentation’, nursing diagnoses and interventions, the items aims, and progress and evaluation notes showed significantly positive changes after the intervention in relation to the chosen cut-off level.
Changes in the N-Catch II scores in the nursing documentation after the intervention.
Discussion
The aim of the study was to investigate the impact of implementing nursing diagnoses in a free-text format at a medical department by means of an education intervention. Although the intervention emphasized implementation of nursing diagnoses, all elements of the nursing documentation had a distinct focus in the education intervention.
The nursing diagnosis, a core element of nursing documentation
Despite nurses’ long tradition of documenting their practice, the quality and accuracy of this documentation have been discussed for several years.2,4 Nursing diagnoses are pointed to as central in nursing documentation enabling planning of good interventions and individualized patient care.15,16 In addition, it is claimed that improving the use of nursing diagnoses may have an effect on completeness of nursing documentation in general.11,15,21 To formulate accurate and complete nursing diagnoses was therefore chosen as the subject for an education intervention addressing nurses in a hospital setting.
As a pretest, nursing documentation one year prior to the intervention was assessed. The results indicated both elements of satisfying completeness as well as elements of poor practice. N-Catch II’s first item disclosed diverging results. This item in the N-Catch II assesses which elements are present in the nursing documentation. In order to score 3 points, an admission note, personal data, a nursing care plan and a discharge note should be present. The pretest assessment indicated satisfying completeness as 57.1% of the records scored the highest possible score. However, the high score for quantity is not reflected in the quality of the documentation. In fact, all of the elements mentioned above achieved higher scores for quantity than for quality. From this, it could be deduced that the quality of the content needs more attention than the quantitative aspect, e.g. more focus is needed on the ability to express and articulate nursing activities in a qualitatively satisfying manner.
In line with this, an aim for the education intervention was to increase the nurses’ capabilities in clinical reasoning related to the diagnostic process, with a consequence of expressing adequate and useful nursing diagnoses. The pretest indicated a potential for improvement, particularly for the qualitative aspects. Assessment in the posttest indicated that the implemented structure for formulating nursing diagnoses was useful and supportive. The presented structure describing necessary elements to formulate an accurate nursing diagnosis seemed to be applicable in supporting nurses to express their patients’ health problems. However, further support for nurses in terms of classification systems and standardization could be even more fruitful.18
Studies have shown that improving one element of the nursing documentation may have a positive effect on other elements in the documentation.16,33,34 Our results support this. However, the largest changes were found in elements of the nursing care plan, namely nursing diagnoses, aims and interventions closely related to the topics in the education intervention. These findings are in line with the concept of the nursing diagnosis being a core element of the nursing care plan.11,12,15,21 The identification of a nursing diagnosis ensures a beneficial direction for further planning, aims and interventions. The nursing care plan has been a central working tool for nurses over decades. The frequent descriptions of low quality in nursing documentation in addition to insufficient knowledge on the topic could indicate that there is still a need for education on how to document nursing in a way that supports nurses in their working processes.
Impact of education intervention on accuracy in the nursing documentation
The Health Act in Norway describes health professionals’ obligation to document their actions in the EHR. 35 The education intervention presented theory and practical sessions to improve the diagnostic process by enhancing clinical reasoning.18 The changes in the nursing documentation can be interpreted as the intervention having impact on the nursing documentation. This confirms that education interventions on nursing documentation can improve nurses’ documentation in terms of completeness and accuracy.33,36
As previously stated, poor quality in nursing documentation has been reported for several years.2,4 Our study indicates that giving education and an opportunity for training improves nurses’ documentation practice. The interventions’ educational measures were designed in a low-cost manner and therefore were achievable to facilitate within nursing staffs’ own resources. Hence, the education intervention could easily be replicated, both in other departments and for nurses in other parts of the healthcare service. If skills obtained from participating in the intervention are sufficient for applying nursing diagnoses in such a way that quality in nursing documentation is increased, then the results imply that the dissatisfying quality can be addressed with education interventions in a clinical setting. Our findings strongly support the positive consequences of strategic educational measures ensuring nurses’ knowledge on the topic.11,15,18,20,21,33,36
The intervention addressing nursing staff members was delivered as teaching sessions and group work. To make the intervention feasible for the department, members of staff were divided into three groups, and each group attended separate teaching sessions. The participants at each session therefore comprised nurses from all of the department’s four units. This was both convenient for the nursing management and reasonable as the nurses collaborate across the units in their daily work. Therefore, it was also decided not to investigate changes in the nursing documentation on an individual level but rather to focus on changes at an organizational level.
Assessment with the audit instrument N-Catch II
The N-Catch II instrument describes how to assess nursing documentation in an easy manner giving the reviewers an audit instrument and a corresponding guideline.25,29 The reviewers experienced assessment of the qualitative aspects in the documentation as challenging even though the guideline was accessible. It is not always easy to evaluate what is to be considered as precise and relevant when only reading the nursing documentation . Furthermore, the reviewers suggest improvements to the guideline, making it more user friendly by adjusting the amount of text and making the design more applicable. The calculations of reliability in N-Catch II indicate the need for further improvements also suggested by others. 9 Our experience supports their proposal for further developments making the descriptions for assessments of some items less vague and subject to interpretation.
Strengths and limitations
This study was carried out in one department at one hospital. Other departments may have other traditions for documentation and other EHR systems leading to other findings. However, the literature shows shortcomings in and discussions on quality of nursing documentation.1,2,4 Hence, the low-threshold intervention applied in our study could be of interest also for others.
Not all of the nursing staff members attended the sessions in the education intervention. It might be that some of those not attending were part of other phases in the intervention receiving, for example, guidance from nurse key personnel. However, this reflects the practice at the setting where turnover among staff is normal and we believe this to be a strength in the intervention as it will reach nurses at different occasions. Moreover, those not attending the teaching sessions might have contributed to the records that were assessed in the posttest. The documentation of nursing is a joint task and a responsibility for the whole staff. For the nursing management, it was important to create a culture of good nursing documentation. Therefore, we chose an organizational level for investigation of changes in the EHRs.
The study had a pretest–posttest design with no control group. Therefore, there might be additional reasons for improved documentation in the posttest other than the intervention itself. The records for assessment were collected as a consecutive sample and it might be that collecting them randomly would have given other results. Further investigation, preferably with a randomized controlled trial, is recommended.
Conclusion
The study indicates that a low-threshold education intervention may have impact on more complete and accurate nursing documentation, in terms of higher scores for quantity and quality as assessed with the audit instrument N-Catch II. Our study introduced nursing diagnoses in free-text format with PES structure and a significant change was found for nursing diagnoses after the intervention. Furthermore, the intervention seems to have had a positive effect on quantity and quality in the nursing documentation for several of the other elements included in the audit instrument N-Catch II. Consequently, our study confirms that focus on one element in the nursing documentation may lead to improvement in other elements of the documentation. Moreover, the study reveals that skills in nursing documentation can be addressed in an easy and low-cost education intervention.
Calculations of reliability in N-Catch II vary from fair to good. The instrument may be reliable for assessment of nursing documentation in hospitals in a Norwegian context. However, there is a need for further improvements and adjustments in both the audit instrument and its guideline. Further research by reviewers not involved in the translation and adjustment of N-Catch II is needed before concluding on the instrument’s accuracy.
Clinical implications
More focus on the diagnostic process related to clinical reasoning should be emphasized in both education and in clinical practice. The presented education intervention showed a significant impact in terms of more accurate nursing diagnoses and could produce significant improvements in nursing documentation. As this is an intervention which is easy to carry out, it could be of interest for others intending to improve their nursing documentation.
Footnotes
Acknowledgements
We thank St. Olav’s Hospital, University Hospital in Trondheim and the Department of Nursing, NTNU for supporting the study.
Funding
The authors wish to thank the Norwegian Nurse Organization, NNO, for funding to support translation of the N-Catch II audit instrument.
Conflict of interest
The authors declare there is no conflict of interest.