
Abstract
The aim of the present follow-up study was to describe staff perceptions of enabling and inhibitory factors that influenced implementation of evidence-based practice (EBP) for urinary incontinence in a nursing home. Focus-group interviews were carried out and the text was deductively analyzed using the PARIHS framework and qualitative content analysis. Factors believed to be most enabling for implementation were EBP being considered as relevant and as a social process, and visiting the lavatory being considered as a right for all. One determinant of successful implementation was having clear and involved leaders who had a continuous positive attitude toward EBP and demanded results. Staff members who were given the role of continence agents were important facilitators. The factor believed to inhibit implementation most was staff having to carry out pad-weight tests before prescribing individual incontinence aids. Evidence-based practice offers a successful concept for caring for older people with urinary incontinence in nursing homes. Evidence-based practice should be spread, both local and more widely.
Background
Many nursing home residents do not receive the available evidence-based assessment and treatment of urinary incontinence (UI) they need. 1 In Sweden, there are about 1.8 million people 65 years of age or older, and 30–40% of them experience UI.1,2 In nursing homes, more than half of residents may be incontinent. 1 The International Continence Society defines UI ‘as any involuntary leakage of urine’ (p. 117). 3
The implementation of evidenced-based practice (EBP) for UI began in spring 2013, in a nursing home in Sweden with physically and cognitively impaired residents. The reason for implementing EBP for UI was to increase quality of life among nursing-home residents through quality assurance of assessment, treatment and nursing interventions, in cases where prescribed individual incontinence aids were needed, and to ensure increased frequency of lavatory visits among residents. The EBP included basic investigation of UI and different behavioral interventions, for example, toilet assistance around the clock. Furthermore, pad-weight tests were carried out before prescribing individual incontinence aids.4–6 The basic assessment and investigation of UI in older people included underlying causes, history of urinary symptoms, history of urination and pad-weight test, in accordance with the provincial guidelines on UI among older people, 4 the national quality assurance program Nikola 5 and the national procedure of prescribing incontinence aids. 6 These policies and guidelines have varying degrees of evidence-based knowledge. Toilet assistance is a nursing intervention in helping older people to regain continence or contain incontinence. Toilet assistance includes prompted voiding, habit training and timed voiding. Prompted voiding means that verbal prompts are used to ask the older people whether they are wet or dry, and whether they need toilet assistance. If such needs arise, then the member of staff helps them to the lavatory. Habit training means identifying the elderly person’s natural voiding pattern and creating an individualized toileting schedule. Timed voiding is based on pre-determined intervals between toiletings.1,2 There is limited scientific evidence suggesting fewer UI episodes in nursing-home residents who have undergone habit training or prompted voiding in combination with physical training, according to the National guidelines for care in cases of dementia 2 and the Evidence-based treatment of urinary incontinence in older persons and frail older persons. 1 The staff received training in EBP for UI, conducting pad-weight tests, fastening incontinence aids, and prescribing and monitoring toilet assistance and incontinence aids.
Promoting Action on Research Implementation in Health Services (PARIHS) is a model intended to put evidence into practice. Rycroft-Malone argued that there are three interacting cornerstones of importance before, during and after implementation when evidence is put into practice: evidence (research, clinical experience and patient experience), context (receptive context, culture, leadership and evaluation) and facilitation (roles, skills and attributes). 7 The PARIHS model can be used as a practical instrument to evaluate implementation of EBP.7,8
Implementation of evidence-based knowledge in practice is a complex process influenced by factors at the organizational and individual levels. 9 Many older people would receive appropriate evidence-based assessment and treatment of UI if compliance with EBP were higher. 1 Studies are needed that deepen our understanding of how evidence-based knowledge in UI is implemented in elderly care. In the present follow-up study, evaluation of implementation of EBP for UI in a nursing home can increase our understanding of staff perceptions of which factors enable and hinder implementation. This knowledge can be used in continued implementation of EBP for UI in nursing homes.
The aim of the present follow-up study was to describe staff perceptions of which enabling and inhibitory factors influenced implementation of EBP for UI in a nursing home.
Method
This is a qualitative, follow-up study that was conducted in a nursing home in Sweden during spring 2014, one year after implementation of EBP for UI. The facility included a dementia ward and a short-term ward and had 46 accommodations in total. A purposive sampling was used, where all informants had experience of EBP for UI and illuminated the questions under study. 10 In total, 14 people accepted the invitation to participate in this study: six auxiliary nurses (including two that were continence agents), four nurses (including one night-shift nurse) and four people in managerial positions. The auxiliary nurses were between 42 and 64 years of age and had worked in the nursing home for between 20 and 32 years. Corresponding figures for nurses were 29–51 years of age and 3–14 years of work experience, and for managers 51–62 years of age and 1–6 years of work experience in their current position.
Three focus-group interviews and two individual interviews (due to inability to attend the focus-group interviews), were conducted in a conference room at the workplace. The focus-group participants had similar educational backgrounds and levels of experience, which was intended to make them more willing to compare notes, evaluations, thoughts and ideas with each other. 11 The authors, including one moderator and one assistant, carried out the focus-group interviews. The moderator used a semi-structured interview guide, containing ten questions, based on the three cornerstones: evidence, context and facilitation, as suggested in the PARIHS framework.7,8 The interviews began with two open-ended questions: ‘What enabling factors did you perceive regarding implementation of the EBP for UI?’, ‘What inhibitory factors did you perceive regarding implementation of the EBP for UI?’ Each interview lasted around 60 minutes. The interviews were audio-recorded and transcribed verbatim by an independent person.
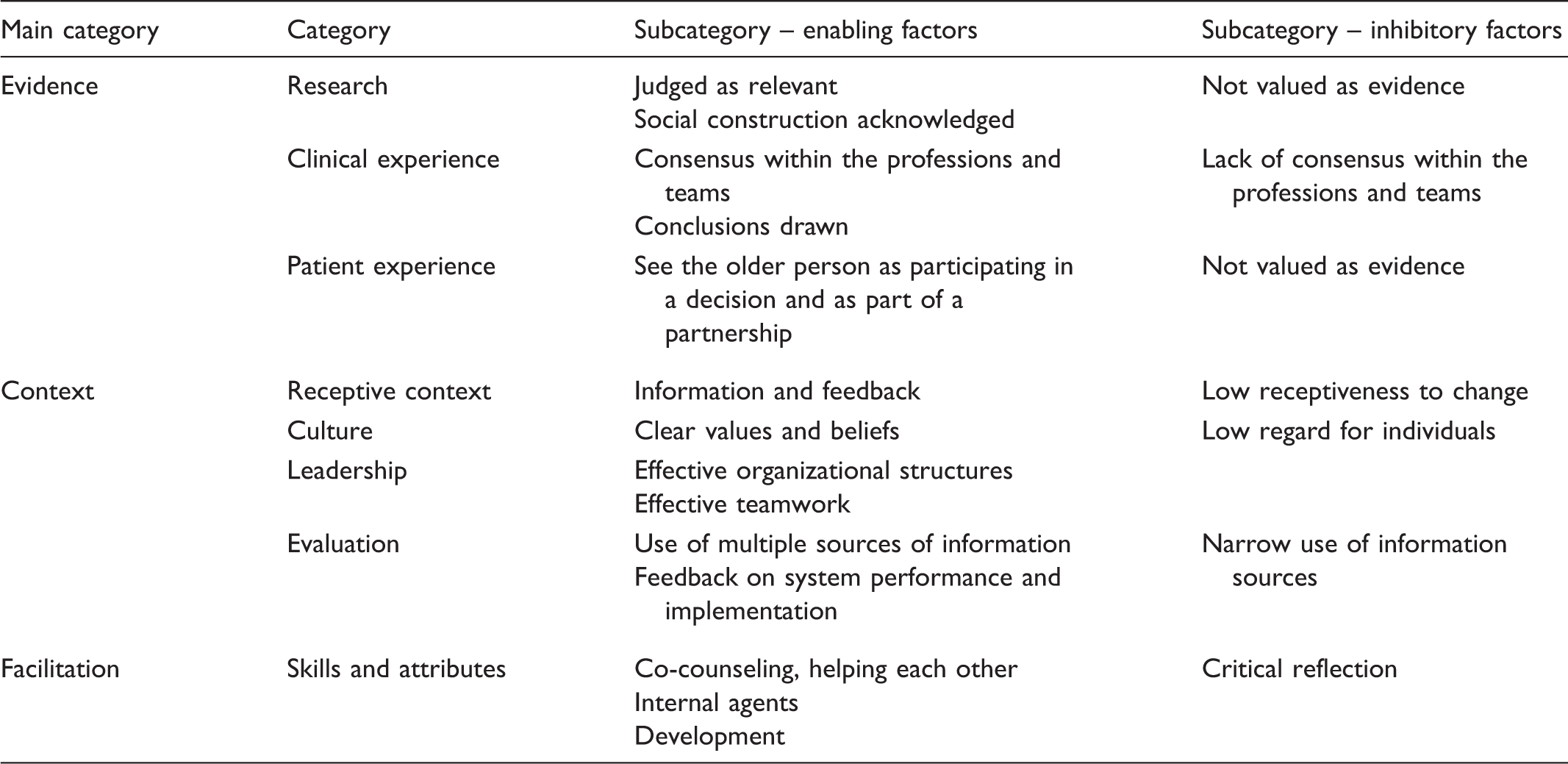
A summary of main categories, categories and subcategories interpreted using the PARIHS framework to describe staff perceptions of enabling and inhibitory factors that influenced implementation of an EBP for UI in a nursing home.
Ethical considerations
Staff members were informed about the study both orally and in writing. Informed consent was obtained from all participants. They were also informed that participation was voluntary and that they had the right to discontinue participation without explanation. All information was treated confidentially. The Research Ethics Committee at Dalarna University approved the study (reg. no. DUC 2014/698/90).
Findings
Findings are presented using the PARIHS framework cornerstones evidence (research, clinical experience and patient experience), context (receptive context, culture, leadership and evaluation) and facilitation (skills and attributes) and using predefined subcategories distributed across enabling and inhibitory factors affecting implementation of the EBP for UI in a nursing home (see Table 1).7,8
Evidence
Research – enabling factors
The staff felt the common ground for the EBP for UI was judged as relevant and gave knowledge and understanding concerning problems associated with older people not visiting the lavatory. The intention of the EBP was to promote the older person’s right to visit the lavatory. A person’s right to visit the lavatory was connected with a dignified life and with the values of the ward. … this is part of a life of dignity and well-being. Being able to use the toilet when I want to – and need to. (Manager)
Toilet assistance and possible prescription of incontinence aids with pad-weight tests were conducted during physical encounters between the older person and staff. The EBP for UI was acknowledged as a social construction and the staff and the older people felt that they were a team and helped each other; close cooperation was essential.
Research – inhibitory factor
From the beginning, EBP for UI was not valued as evidence by nurses and general practitioners at the primary healthcare clinic. Staff at the nursing home did not see the utility of pad-weight tests and documentation. All incontinence aids had to be prescribed individually, but this was not clear to everyone from the beginning. Now it’s individual prescription of aids that applies, before we just took a diaper from the cupboard. (Auxiliary nurse)
Clinical experience – enabling factors
To achieve consensus within the professions and teams, regular team meetings were important. The staff felt that team cooperation and information handover between the day- and night-shift staff concerning older people’s toilet assistance and incontinence aids had improved.
Conclusions drawn
The EBP for UI had influenced the staff to change focus and consider how they want to live when they are older people. Older people need time for toilet visits, and this should not be controlled by staff routines. Several staff could note early signs of a person needing to use the lavatory. Well, you learn to read the situation, for each of them. Some become fidgety and anxious and start rambling, talking too much and … (Auxiliary nurse)
Clinical experience – inhibitory factor
Lack of consensus within the professions and teams
The process of implementing EBP for UI has mainly been experienced as a concern for day staff. The night staff said that the older people were unsteady on their feet at nighttime and that they would not wake anyone. The night staff were included in the process from the beginning, but due to meeting times they declined continued participation. Staff had varying opinions on fastening incontinence aids and whether the process resulted in increased workload or saved time. They said that new staff thought the older people could urinate in the incontinence aid. Sometimes, it was difficult to encourage staff to work with toilet assistance. Toilet assistance is highly specific to who is working. I think people see it from different perspectives too, some think you save a little time and can do something else and others maybe think it’s more work and that it takes more time than … Well. (Nurse)
Patient experience – enabling factor
The staff felt it was important to see the older person as participating in a decision and as part of a partnership. Many older people took for granted that staff would help them with lavatory visits. The staff need to ask each older person about urination habits at admission. Some older people had experienced toilet assistance and pad-weight tests as an opportunity to talk about UI.
Patient experience – inhibitory factor
Not valued as evidence
The staff stated that some older people wanted incontinence aids to be on the safe side, and others wanted incontinence aids instead of toilet assistance. Well, if a person is sharp mentally and still doesn’t want to use the toilet, then you can’t carry them there. (Auxiliary nurse)
Context
Receptive context – enabling factor
Information and feedback
The nurse is responsible for the entire prescription process. The nurses trained continence agents in pad-weight test methods and they received feedback on individual performance. The continence agents passed their knowledge of pad-weight testing on to all day- and night-shift staff. They wanted the time required for work with incontinence aids, to check and refill the supply of aids.
Receptive context – inhibitory factor
Low receptiveness to change
Continence agents and nurses met resistance to implementation of EBP for UI. Not all staff were included in the process from the beginning, which resulted in an emergency meeting. For example, initially the older people’s beds were often wet, which was due to inadequate fastening of incontinence aids; the staff took these comments personally. They’re not fastened right, these incontinence aids. And when this was brought up they, the staff, took it very personally. They didn’t think: Oh! Is this maybe one of the reasons for all the leakage, but instead took it more like: I’ve worked for 20 years and I know how you put incontinence aids on. (Manager)
Culture – enabling factor.
Clear values and beliefs
The continence agents have achieved greater insight into the prescription process, which has affected their jobs. The continence agents initiated pad-weight tests, thus taking on another role. They helped each other and ordered incontinence aids after individual testing. They realized that improved fastening technique enabled older people to sleep with fewer disturbances at night.
The staff experienced that the incontinence work had become easier. Their persistent work toward change had at last led to development. When it finally turned, then it was substantial, we just had to get over the hump. And that was hard for everybody. (Manager)
Culture – inhibitory factor
Low regard for individuals
The intention is that toilet assistance is to be offered based on individual needs. At the beginning of the process, the staff felt that toilet assistance should suit their routines. Well, should residents use the toilet when it suits staff routines or should it be based on individual needs? That’s not how it is. They use the toilet when the staff have time, when it suits how work is organized. (Nurse)
Leadership – enabling factors.
Effective organizational structures
When EBP for UI was anchored among top management, staff members’ work was undisturbed. Support and demands from the managers ensured that the process continued. … knowledge is lacking at all levels and I actually think one of the key things … is that we’ve started at the management level and then gotten everyone with us. Because if it’s not anchored among top management either, then you can’t work with it. Because then people just think: Well really, changing a diaper isn’t difficult. (Manager)
Effective teamwork
It was determined that auxiliary nurses and nurses should cooperate in teams. The unit head encouraged auxiliary nurses to inform and cooperate with nurses around pad-weight tests and prescriptions. The workplace meetings held every fourth week were mandatory, and allowed staff to ask questions so that everyone felt they were participating in the work toward change. And I still feel that those of us in the continence group are very close, we cooperate really well and we know the auxiliary nurses think so too, we’ve talked a lot about this. We’ve developed a fine collaboration. (Nurse)
Evaluation – enabling factors
Use of multiple sources of information
The staff needed access to both regional (www.ltdalarna.se/inkontinens) and national incontinence portals (http://nikola.nu and http://plus.rjl.se/senioralert). The staff used Nikola’s 5 and Senior Alert’s 14 national quality improvement program for UI.
Feedback on system performance and implementation
The staff felt encouraged and continued their work toward change when they received feedback. And then it was great fun when we got to see the lists and how efficient we’ve been … How much better it was for the old person, it was really fun to see that it gave results. Immediately, after a short time. (Auxiliary nurse)
Evaluation – inhibitory factor
Narrow use of information sources
Nurses and auxiliary nurses had different possibilities to keep up to date with new findings and guidelines. Auxiliary nurses were not used to seeking information and had no time to seek evidence. But – the auxiliary nurses don’t have the same – well, development. How should I put it? The same demands aren’t placed on them, to stay informed. No. They don’t have the same opportunities either; they don’t get any external training. When we’re supposed to save, they don’t get anything. (Nurse)
Facilitation
Skills and attributes – enabling factors
Co-counseling, helping each other
The staff felt they helped each other and now worked more as a team, thanks to the nurses. Work toward change requires proactive and knowledgeable nurses with the right competence and training. The prescribing nurses had attended a course on incontinence and prescription of incontinence aids (7.5 credits). It is also of crucial importance for co-counseling, helping each other that managers, on different levels, continue to support the program.
The continence agents worked as internal agents, and it was important that they were interested in the task. Having two agents on each ward was a factor for success. … two on each ward, I think it’s really important. You should never have to be alone in a situation where you’re exposed to some aggression and irritation in the staff group, so a person should never have to be alone … and they have each other’s support. (Manager)
The continence agents have developed with the task and come to understand how they can engage their colleagues. The agents ended up leading their colleagues in the change process. And I think they’ve been given a new role, because now they can, for instance, initiate a pad-weight testing. They come to me and say, now we think this should be done on this person, and then I applaud them. (Nurse)
Skills and attributes – inhibitory factor
Critical reflection
Concerns emerged about additional costs in conjunction with implementation of EBP for UI. Initially, the staff found it difficult to see the future gains, for example reduced costs for laundry and incontinence aids. In hindsight, the management had to acknowledge that it would have been better to start the EBP for UI earlier and make more time for the staff to realize the program.
Discussion
The factors that emerged as being most enabling for implementation were: that the EBP for UI was understood as relevant, that it was regarded as a social process and that visiting the lavatory was considered a right for all people which promoted dignity and well-being. One determinant of successful implementation was having clear, involved leaders who had a continued positive attitude toward the program and who demanded results. The members of staff who were given the role of continence agents were important facilitators; they led realization of the program among their colleagues.
The factor that most inhibited implementation was the staff having to carry out pad-weight tests in order to prescribe correct, individual incontinence aids. At first, the staff felt motivated to carry out EBP, but they lost this feeling early on. Some staff showed aggression, which is a natural part of a change process.
Evidence
The overall purpose of putting evidence into practice is to improve patient care, which also helps relatives. 15 The aim of implementing EBP for UI was to improve nursing-home residents’ quality of life by ensuring the quality of assessment, treatment and nursing interventions, when necessary also prescribing individual incontinence aids and increasing the frequency of residents’ lavatory visits. The EBP for UI was judged to be relevant and was acknowledged as a social construction. In the case of judged to be relevant the residents’ right to visit the lavatory, regardless of time of day, was associated with leading a dignified life and regarded as a matter of course. Care should build on respect for people’s self-determination, integrity and participation.16,17 The subcategory acknowledged as a social construction described that assessments, toilet assistance and prescribing incontinence aids were carried out during physical encounters between the older person and staff. The staff and the older people felt more interactively involved. They helped each other and thus a situation resembling co-counseling between and within professions and older people was developed that constituted the basis for successful change management. Successful implementation is more likely to occur when evidence is well conceived and conducted.7,8
The EBP for UI, above all pad-weight tests, came to imply change, as compared with existing routines. The staff showed resistance, sometimes aggression, which was probably caused by lack of knowledge about individually prescribed incontinence aids – an approach that was not clear to everyone from the beginning. Research results need to be translated into useful routines before they are introduced in healthcare practice. 18 The staff received training in EBP for UI, training in pad-weight tests, fastening of incontinence aids, prescribing and monitoring toilet assistance and incontinence aids. The staff felt that Nikola’s 5 and Senior Alert’s 14 national quality programs for investigation of UI should be used. New routines were created, the change propensity shifted, and some staff took criticism personally, which is a natural part of the change process. Rycroft-Malone et al. reported that thoughts, attitudes, education and the possibility to seek information are individual factors that affect implementation of research findings in healthcare. 19
Early studies on implementing evidence-based nursing in practice have shown that nurses felt the research was of inadequate quality and lacked relevance. 20 Nurses need to see a clear link between research results and clinical significance. 19 Findings from systematic reviews of good quality would help to guarantee evidence-based care. 18 In the present study, EBP for UI was based on the Evidence-based treatment of urinary incontinence in older persons and frail older persons, 1 the National guidelines for care in cases of dementia 2 and the provincial guidelines on UI among the elderly, which have varying degrees of evidence-based knowledge. 4 The nurses were at the forefront and developed good teamwork with the auxiliary nurses. Furthermore, the nurses trained the continence agents in pad-weight tests and wanted staff to see nursing interventions as an alternative to incontinence aids.
Context
Leadership is an important factor for successful implementation of research in healthcare. Effective leadership results in clear roles and effective teamwork. 21 In our study, it was important that EBP for UI was first anchored among top management and then in the rest of the organization. It was when the senior manager in the municipality clearly expressed that EBP for UI should continue that the process took off. The managers indicated, through their words and actions, the need to improve incontinence care and that the change process was a priority. Having clear, involved leaders, who had a continued positive attitude toward the program and who demanded results, was of crucial importance to successful implementation. To succeed with implementation, it is important that managers create a culture which highlights the importance of evidence-based work and that managers follow up on the outcomes. 22
There is a need for organizational support and a favorable culture that promotes implementation of research findings – a culture where, for example, ideas, education and courses reinforce work toward change. 23 Nurses play a key role in preventing and treating UI within elderly care. 24 Keeping up to date on new knowledge is part of the nursing profession. The nurses were trained in incontinence care. The present study showed that nurses and auxiliary nurses had different opportunities to follow new developments in knowledge and guidelines. The auxiliary nurses were not used to seeking information and do not have time to seek evidence. They are not given the same opportunities as nurses have to improve their knowledge, and in times of savings auxiliary nurses’ possibilities are limited. There are valuable web-based training programs (e.g. Nikola 5 ) that could be used to increase staff knowledge.
Facilitation
To support implementation of EBP for UI in nursing homes, facilitators are needed. 25 Factors that have shown positive effects on implementation of evidence in healthcare are local multipliers, teaching meetings, computer-based reminder systems as well as evaluation and feedback. 18 In the present study, the continence agents played an important role in facilitating attitude change and an approach to EBP for UI that entailed introducing new routines. The continence agents had support from the team. Having two designated incontinence agents on each ward was a key to success. Regarding the prescription process, the continence agents need a clear mission, time and knowledge about pad-weight tests. The nurse is responsible for the entire prescription process and plays an important role in teaching pad-weight testing. Moreover, the nurse is also responsible for supporting dissemination and use of national and local guidelines. 26
Method discussion
To assess the trustworthiness of findings, Lincoln and Guba mentioned four criteria for achieving high quality: credibility, dependability, confirmability and transferability. 27 Credibility can be ensured by carefully reporting on sampling and data analysis. Purposive sampling was used here, and all informants had experiences of the EBP for UI. However, only one person from the night shift participated, which may have affected the findings. The participants in each focus group had similar educational backgrounds and levels of experience, the intention being that this would make them more willing to compare notes, evaluations, thoughts and ideas with each other. 11 Furthermore, use of focus groups created openness, in that the participants posed questions to each other, made suggestions and encouraged each other to narrate. 28 However, two individual interviews were conducted due to participants being unable to attend the focus-groups interviews, which may have affected the findings. Examples from the data analysis have been described in the findings, and the subcategory presentations end with quotations, which showed a variety of perceptions from all three groups: auxiliary nurses, nurses and managers. For implementation to be successful there needs to be clarity concerning the nature of the evidence being used, the characteristics of the context and the type of facilitation needed to ensure change. 7 The present data were deductively analyzed using the cornerstones of evidence, context and facilitation according to the PARIHS framework. 7 However, new information could have been lost in the analysis by using predefined categories and subcategories.
Dependability was ensured by using a semi-structured interview guide with questions inspired by the PARIHS framework.7,8 DH led the focus-group interviews, assisted by LO; the interviews were audio-recorded. Some interview texts were difficult to interpret, in that they fell into several subcategories. Repeated analyses were conducted until the subcategories were mutually exclusive 27 and achieved consistency. In our study, there were data that did not fit into the PARIHS framework and we did not find meaning units for all subcategories according to the PARIHS framework. Further studies are needed to increase the understanding of staff perceptions of which factors enable and hinder implementation of EBP for UI in nursing homes. DH conducts research in UI, is an urotherapist and has worked as a district primary nurse. LO conducts research in elderly-care nursing and works as a healthcare developer and elderly strategist in a county. Our different experiences and preconceptions concerning EBP for UI have increased our understanding, and we have critically discussed the data to ensure that they remained original and not simply what we wished to see. 27
Confirmability refers to the degree to which analyzed data truly represent information that participants provided. 27 To allow evaluation of this criterion, original quotations have been presented in the results section.
Transferability concerns the degree to which the findings can be transferred to other settings and groups. We believe our findings on the factors that enabled and inhibited implementation of EBP for UI can be transferred to nursing homes. The study’s credibility, dependability and confirmability have been demonstrated, and the reader can follow how the interpretations and conclusions emerged from the findings. 27
Conclusions and clinical implications
The EBP for UI studied here offers a successful concept for caring for older nursing home residents with UI. The EBP should be spread, both local and more widely. However, the implementers should pay attention to teaching pad-weight testing in order to prescribe correct individual incontinence aids.
For older people, the clinical implications of EBP for UI can be increased quality of life and improved conditions for continued lavatory visits. For the healthcare system, experiences from EBP for UI can hopefully lead to better incontinence care and be used as the sole basis for a county-wide process. For society, EBP for UI can be used as an approach for counteracting the development of UI among older people. Ethical aspects such as the feasibility of assessing and treating UI, facilitating lavatory visits as well as individually prescribing incontinence aids should be considered in collaboration with the older person and his/her relatives.
Footnotes
Acknowledgements
We would like to thank the study participants.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.