
Abstract
The rate of requests for autopsies has dropped over the last four decades. In the present study we have investigated the clinical usefulness of autopsies in a university hospital for determining the cause of death and as a source of information for the relatives. The autopsy routines were sufficient to fulfil clinical needs and resulted in essential information. The next of kin were involved in the decision to perform an autopsy in half the cases. In 10% of cases the relatives requested the examination. We believe that a desired increase in autopsies performed could be reached if the relatives of the deceased were informed of their value. We further suggest that nurses be included in a team process informing the relatives of the value of autopsies and their right to share the information gained.
Introduction
The benefits of clinical autopsies in the healthcare system for determining the cause of death, for continuing to educate the medical profession and for informing the next of kin are well known and have been confirmed in a multitude of studies from all over the world. In spite of this, the number of clinical autopsies is rapidly decreasing, while the number of forensic autopsies is not. In the United Kingdom, almost all autopsies are performed after the coroner determines the cause of death, while clinical autopsies are as low as 0.69%. 1 In Sweden, as in other countries around the world, the number of autopsies performed has steadily decreased over the last four decades, from locally nearly 100% and nationally 50% to 10% or lower today in some areas.2–7 This means that the cause of death is determined primarily based on clinical assessments and investigations performed prior to death, although we know from previous studies that autopsy provides additional information about more than 40% of deceased patients.2,8,9 In addition, Pritt et al. identified multiple errors on 82% of death certificates, including major errors on more than 30%. 10
Clinicians are requesting fewer autopsies for many reasons.11,12 Studies have suggested that the low rate of requests for autopsy could be because the process required to obtain permission or consent from the next of kin is cumbersome; relatives are not asked for permission in half of cases; and autopsy reports provided by the pathology department are of poor quality or do not reach the responsible physician in time to be of clinical value.1,5,11 In a high proportion of cases where an autopsy was performed, the relatives were never given the results of the post-mortem examination.11,13 Taking into consideration that the relatives of the deceased are increasingly involved in patient care, and more frequently are asking for autopsies to be performed for the benefit of their own well-being and health, 14 this retrospective study investigated the usefulness of routine autopsies, both for fulfilling the obligations of the medical staff and for informing relatives.
When a person dies at home, whether or not in the healthcare system, the cause of death must be determined according to Swedish law and reported to the authorities through completion of a death certificate. The cause of death is of interest not only to the authorities but also to the relatives and healthcare personnel. The cause of death is determined by the physician responsible for the care of the patient at the hospital, nursing home or outpatient setting. The physician can request a post-mortem examination to support the initial diagnosis after obtaining consent from the next of kin. When persons die from unnatural causes, such as accidents, intoxication or crime, an autopsy is requested by the police and performed in a forensic department. If an unnatural cause of death can be excluded, the post-mortem examination is conducted in the pathology department of a hospital by a clinical pathologist.
Until the end of the 1980s, autopsies were frequent in Sweden. Burton and Underwood reported that in 1984 the autopsy rate in the city of Malmö was 81%, 4 while the national frequency was reported as 38%. 5 Since then, the relative frequency of autopsies has steadily decreased. From a national frequency of 34% in Sweden, the number of autopsies performed is now below 10%: 7% for women and 15% for men, including forensic autopsies. 15 The reason for this decrease has not been investigated, and many causes have been suggested, such as a lack of interest and consent from the relatives; a lack of need because physicians have enough information to determine the cause of death from the clinical investigation; cost; administrative burden; late and low-quality reports from autopsies performed; or insufficient value or quality of autopsies to contribute to the understanding of the cause of death. Another interesting statement is that the frequency of autopsies requested is connected to the earlier experiences of autopsies during education and clinical training.7
The present study aims to investigate the clinical usefulness of autopsies in the healthcare process for determining the cause of death and providing information to relatives and next of kin. In this work, we have addressed the question of the value of autopsy in a university clinical setting. The study is a follow-up to two earlier studies performed in the 1970s by Mona Briton16,17 and in the 1990s by Bela Veress and Irina Alafuzoff, 9 when autopsy rates were significantly higher in Stockholm and at the Huddinge Hospital (now part of Karolinska University Hospital). These studies showed that autopsies contributed significantly to understanding the cause of death and the diseases that led to death. In 25% of cases, the cause of death suggested before autopsy by the physician was incomplete or misleading, and in 15% of cases, autopsy results revealed that the disease at the focus of the treatment effort was incorrectly diagnosed. Fifteen per cent of all cancer cases, half of them fatal, were discovered by a pathologist during post-mortem examination. 9
We performed this study on the value of autopsies in a setting where the autopsy rate is low, and post-mortem examination is an exception rather than a rule, to compare our data with the two earlier studies performed when the autopsy rates were significantly higher in the same university hospital context. This study investigated, for the first time in Sweden, the post-mortem examination procedure from start to finish, that is, from obtaining consent to reporting the cause of death to the authorities and the family of the deceased. This question is of particular interest today, when relatives are increasingly knowledgeable about disease and often participate in patient care. 18
Materials and methods
Design
In this retrospective study, we investigated 54 autopsies performed at a university hospital in Stockholm. Of these, 53 autopsies were complete and included dissection and evaluation of all visceral organs including the brain. One case that was only partially examined was excluded from the study. The patients were cared for at different clinical departments where personnel were accustomed to taking care of patients with terminal diseases and their relatives. We asked the following questions:
When were the autopsies performed? Was the report released prior to issuing the death certificate? Did the autopsies add clinical value for the healthcare personnel and the relatives? Who requested the autopsy? Who was informed of the results of the autopsies?
We also compared death certificates with the cause of death determined after autopsy. The clinical usefulness of the autopsies and the autopsy reports were defined based on whether the above questions were answered or not. We did not include data on the use of the autopsies for educational purposes or research due to the fact that data supporting these useful activities were not reported in the medical records. Thus, in this article, we address clinical autopsies performed during 2008 and 2009 from the end-user perspective, with a special focus on how the relatives participated in the decision to perform the autopsy and how they were informed of its results.
The clinical diagnoses registered, reported or suggested in the medical records were compared to the diagnoses registered in the pathology reports. In this study of the value of the routine clinical autopsy we did not evaluate the quality of the diagnoses described in the autopsy reports.
Materials
Patients registered at the Karolinska University Hospital between 2008 and 2009 who died at the hospital were identified in this study. During these two years, 1588 adult patients died at the hospital, and of these patients 174 (11%) were autopsied. In order to evaluate the routines in the wards where personnel were accustomed to caring for deceased patients and more likely to consider the possibility of an autopsy, we selected three departments – gastroenterological surgery, haematology and geriatrics – from which we studied all of the autopsies requested. These clinics were the same as those selected for a previous questionnaire study on nurses’ and physicians’ attitudes about autopsies. 14 In addition to these cases, we randomly selected 20 cases from other departments that were experienced in caring for dying patients. In sum, we studied 54 autopsies. In each of the 54 cases, the medical record, including the nurse’s record; 19 the request form for autopsy; the autopsy report; and the death certificate were examined and compared. One case was excluded because the autopsy requested was partial and incomplete. In this limited study we have not considered ethnic, cultural or religious differences as possible explanations for the reduced frequency of requested autopsies. These factors as well as socio-economic and geographic differences are included in an ongoing national registry study by the same authors.
Patient age and sex from different clinics and documented times for autopsy request, performance and report.

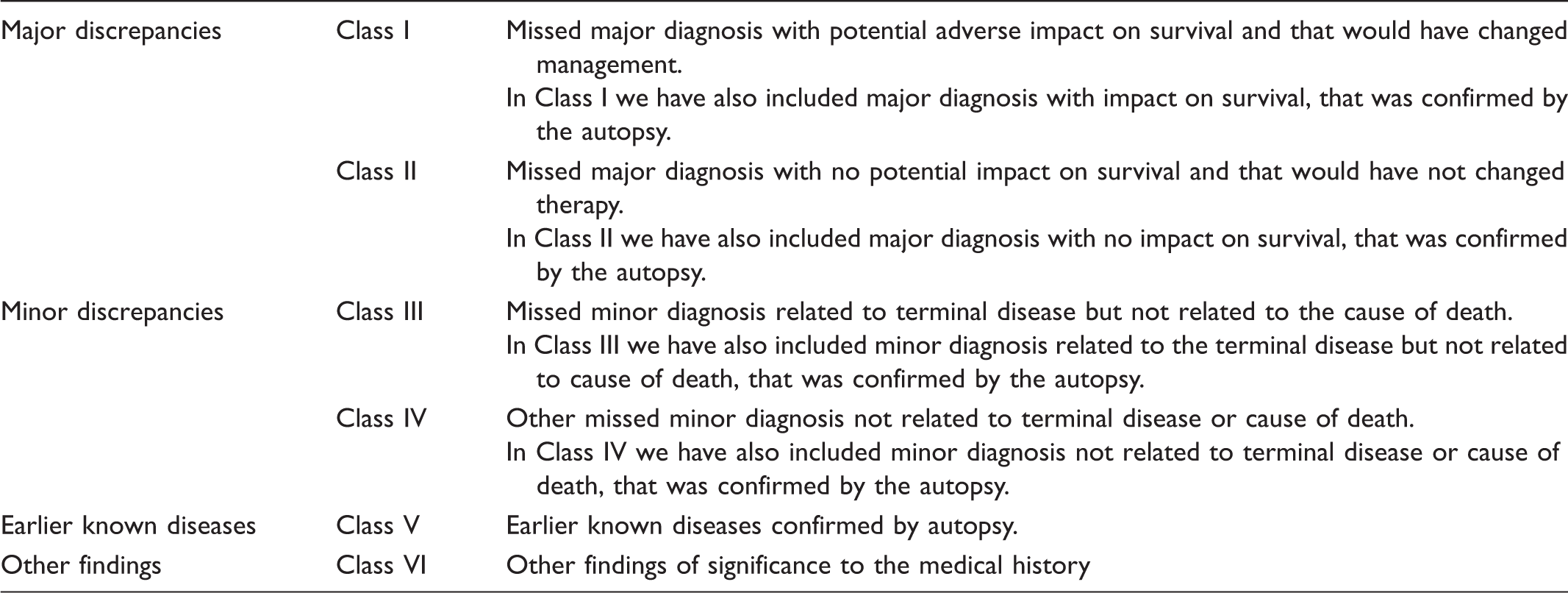
Modified Goldman criteria for autopsy discrepancies.
Each case was classified and categorised by the first author (AR) together with an experienced pathologist (LE). All of the authors discussed the classification and categorisation, and participated in the preparation of the manuscript.
Ethics
This project was approved by the Regional Ethical Review Board in Stockholm (2011/208–31). The patient records were coded to assure the anonymity of the deceased and their next of kin.
Findings
The time of care for the patients in different units varied from 27 days for haematology cases to 8 days for the 20 cases from mixed wards (Table 1). The mean time at the hospital for all cases was 16 days. In the majority of cases from all of the units, the autopsy request was written on the day of, or the day after, the death of the patient, but in five cases the request was written five or more days after the time of death. The request form arrived at the morgue two days after the time of death, and the post-mortem examination was carried out within seven days. However, in five of the 53 cases, the examination was performed two weeks after the time of death for reasons that were not explained in the records. The written autopsy record was registered in the medical record 12 days after the death of the patient. However, in two cases, the registration of the written report in the medical record was more than 100 days after death, with no explanation or obvious reasons. Telephone reports or direct demonstrations to the responsible physician were not registered, but we would expect that they took place. In all cases, tissue samples were taken, fixed, embedded, cut, stained and stored. In 23 of the 53 cases (43%), a microscopic examination was performed and reported.
Party requesting the autopsy and how kin were informed of the autopsy results.

Note. n.d. = not documented
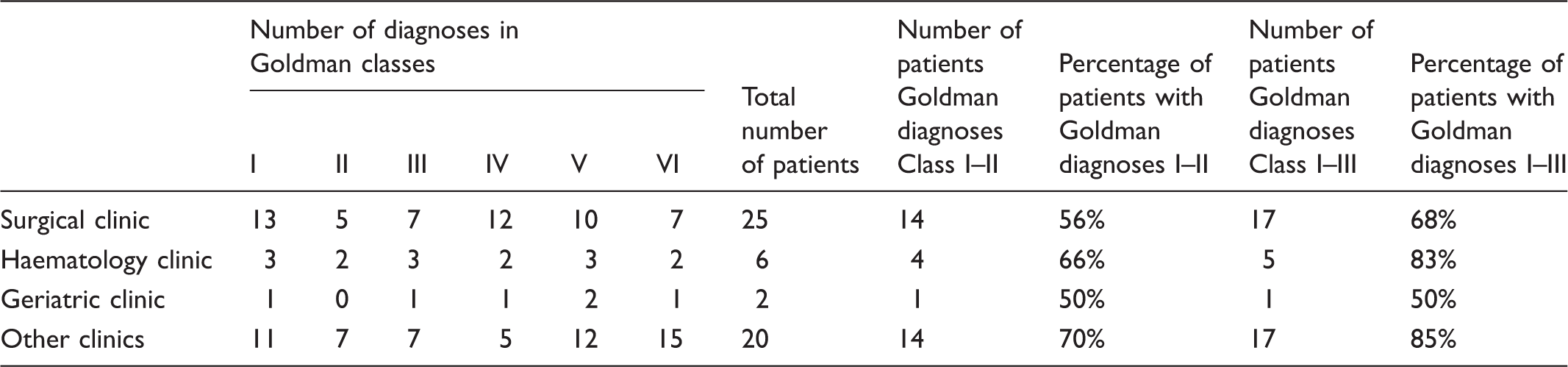
Number of diagnoses in each Goldman class and number of patients with diagnoses in Goldman classes I to III.
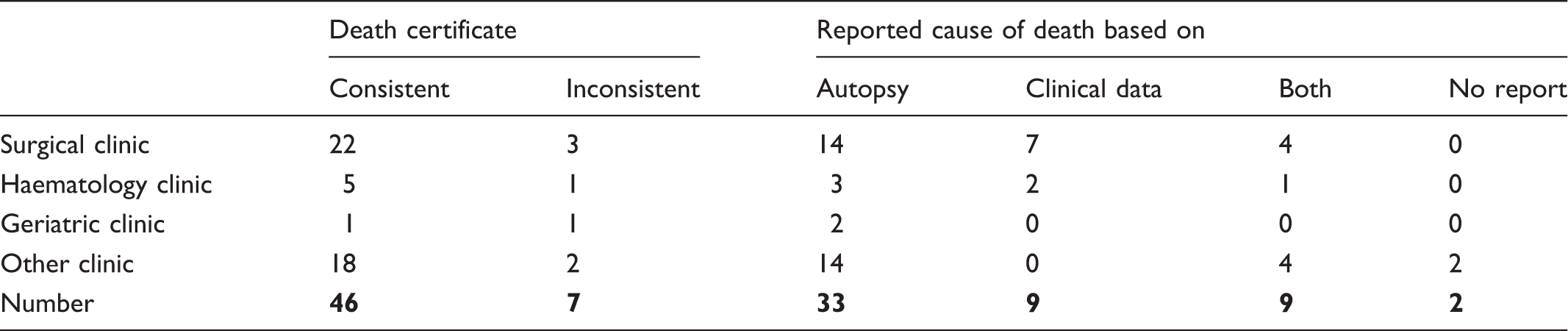
Consistency of the death certificate with the autopsy report.
Discussion
The goal of this study was to determine the clinical value of routine autopsies and to evaluate the value of the information gained at autopsy for the clinical process, for diagnosis before autopsy, for informing relatives and healthcare personnel and for the death certificate. The diagnoses per se were not re-evaluated, confirmed or critiqued. In a clinical situation, where the frequency of autopsies is decreasing rapidly, we addressed whether autopsy today lacks clinical value.25,26 The frequency of forensic autopsy, performed on patients who had died from unnatural causes, including accidents and crime, has not decreased.15,27 Several reports have shown that in a significant number of cases, the next of kin was never contacted or involved in any discussion concerning autopsy, and was not informed of the value or possibility of a post-mortem examination. It is also reported that in many situations where an autopsy was performed, the protocols were delayed, incomplete or unclear, and that the relatives never received the results of the investigation.5,6,11,13,26
We selected departments at the Karolinska University Hospital in Stockholm that were experienced with patients dying on their wards and also which had also been included in an earlier study using questionnaires to evaluate how healthcare personnel used and perceived post-mortem examinations. The departments selected represented different active research departments in the hospital: gastroenterological surgery, haematology and geriatrics. The selected departments had very different rates of post-mortem examinations, ranging from 23% for surgery to 4% for geriatrics. Haematology had a 10% autopsy frequency, which was close to the mean value for the hospital.
By examining data from 53 consecutive autopsies, we concluded that the request for autopsy was generated by the responsible physician within one or two days of death, and that the autopsy was performed and reported within seven to ten days of death, with few exceptions. These routines satisfied the physician’s need for information to write the death certificate and the next of kin’s need to inform relatives in time for the funeral.
We concluded from the documentation in the medical records that two-thirds of the relatives were informed of the results of the autopsy. We also determined that the autopsy results were used to correctly complete the death certificate in just over three-quarters of the cases. However, in more than 20% of the cases, the certificates were completed based only on clinical information. The correlation between the cause of death reported on the death certificate and in the autopsy report was adequate in 85% of the cases, but in 13% of the cases the information was not in agreement with the autopsy report or was missing. It is difficult to find a consistent reason in this limited material for the discrepancies, but in five of seven cases unexpected Goldman class I diagnoses were discovered. It is obvious from our investigation that post-mortem examination supports the clinical process and that it is very important for determining the cause of death. The importance of post-mortem examination is illustrated by studying the diagnoses that were added, confirmed or changed by the autopsy. We classified these diagnoses according to the Goldman protocol to indicate diagnoses that were important factors leading to death or the major disease that led to death (Table 4). We also added findings that were less significant for the cause of death but could have caused symptoms that were obvious to the relatives, or were of epidemiological interest, but that we did not expect to find in the medical record. Diagnoses classified in Goldman class I–III were either missing in the medical record or were suggested but not confirmed while the patient was alive. It is notable that 75% of the patients fulfilled the Goldman I–IIII criteria, and 14% had diagnoses that fit more than one class. Only one-quarter of the patients did not have a diagnosis in Goldman class I–III. The relative number of discrepancies found by our investigation was of the same magnitude as had been previously reported from the same area,9,16,17 and in other countries at hospitals in studies performed 20–40 years ago, when the relative number of autopsies performed was significantly higher.9,11,20,21 It is clear that post-mortem examinations in a clinical setting are of as much value today as they were in the 1970s and 1990s in Stockholm. In a recent report on patients from intensive care units, surgical wards and nursing homes it was stated that the discrepancy in diagnosis before and after autopsy was not dependent on ante-mortem diagnostic evaluation. 28 In recent reports from Fröhlich et al. and Wong et al. the number of missed diagnoses are lower than reported in previous studies and in this work.1,24 These studies of patients in intensive care units are, however, based on Goldman modifications, and included the possibility of successfully treating a patient for the diagnosis reported in the autopsy report before death, or the possibility of actually confirming the diagnosis ante mortem.
We also concluded that the process and flow of information were acceptable for the results to be of value in the clinical routine, although there were exceptions due to delays in reports, microscopic examination and supplying relatives with information. In 40% of cases, a microscopic examination had not been performed, which was not surprising in cases where the macroscopic examination was conclusive. We also observed a significant number of situations in which the relatives asked for the autopsy to be performed. This appears to be an increasing trend, which we view as an indication of relatives’ engagement, and which may indicate that relatives want a confirmation of the diagnosis and of how the patient was treated by the healthcare system.14,26,27,29
One could argue that the findings presented in this work were expected because we examined situations only in which an autopsy was requested by the responsible physician or the relatives, and that these results may not be relevant for deceased patients who are not examined after death. Although we cannot provide data for the deceased who were not autopsied, we believe it reasonable to assume that there are misdiagnoses in these situations as well, likely on the same order of magnitude as seen among the deceased that were examined after death. We base this assumption on the fact that the number of missed or confirmed diagnoses has not changed over the past 50 years and is independent of the autopsy rate. This statement confirms the observations made by Goldman et al. stating that the rate of diagnostic errors has been stable during the last three decades in spite of increased ante-mortem investigations. 20 Scordi-Bello et al. also stated that ante-mortem diagnostic evaluation did not affect the levels diagnostic discrepancies in a study comparing data from patients who had died in intensive care units, surgical wards and nursing homes, respectively. 28 We are concerned about the value of the death certificate register, which among those that had been autopsied contained missed causes of death in 14% of the cases. We suspect that this number is much higher (75% from the Goldman class I–III cases) for the total register of all people who have died in Sweden. Error rates in death certificates were estimated to be around 30% in the United Kingdom. 1
We conclude that the decrease in the autopsy rate in Stockholm cannot be explained by the hypothesis that autopsies are of less value today compared to when the rate was much higher. We also conclude that the validity of the cause of death on the death certificate is dependent on whether an autopsy was performed. Hospital routines have been sufficient to allow the nursing personnel to perform their duties to the government and to relatives. If the autopsy routines from the pathology department have been sufficient, the diagnostic support has been substantial, and the interest shown by the relatives to the deceased has been expressed, why has the autopsy rate been so low and continued to decrease? We 14 and others30,31 believe that the autopsy rate would increase if both healthcare personnel and relatives of the deceased had more information regarding the autopsy process and its value. Hooper and Geller 7 and Liao and Singh 32 also confirm that the propensity of the responsible physician to request autopsy is dependent on the earlier experiences of autopsies during education and clinical training and also on training in the process to collect family consent and to file the request. Liao and Singh 32 and Hooper and Geller 7 also propose automatic routines in the electronic health records to remind physicians to consider autopsy and suggests that nurses and other non-physicians could also have that role.
Autopsy experience in the medical education and training of young physicians is significantly less than 20 years ago. About half of the medical doctors employed in Sweden today were educated in other countries, and many of these doctors have had no or very limited experience in post-mortem examinations. In routine healthcare, where autopsies are rare, the experience of the pathologists has also decreased, threatening the value of the autopsy. We and other authors have noticed that there is a high and growing interest among nurses to be included in the information and consent process with next of kin and other relatives. 30 Nurses often have closer and more frequent contact with family members and can present the possibility of a post-mortem examination, preferably before the death of the patient but when it is clear that the patient is going to die. 14 We suggest that educational programmes for nurses include training in handling cases of terminally ill patients, with an emphasis on understanding the value of autopsies, especially for the next of kin. In the national guidelines for treating strategies in intensive care, where the patients as well as their closest relatives have to consider whether to interrupt treatment or decide not to initiate treatment to prolong life, or to prepare for organ and tissue donation, there are recommendations on how to use information and decide what to do. In this context, the relatives and the next of kin are involved early in the process, and decisions are made by the doctor together with the kin and nursing personnel. We suggest that these recommendations also become guidelines for how to decide on the benefits of post-mortem examination. Hull et al. have suggested that this information should be included in an instructional brochure designed for families to help the next of kin make an informed decision as to whether the deceased should undergo an autopsy. 33
Clinical usefulness
In this work, which is a follow-up study on a recent survey study from the same hospital on the attitudes of nurses and physicians towards autopsy and the decreasing tendency to use post-mortem examination, we confirmed the value of autopsies to gain information about the cause of death for the relevance of the death certificate as well as to inform the next of kin. We believe that the use of autopsies should increase and we discuss the role of information to relatives and education of physicians and nurses to reach this goal.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.