
Abstract
An illness or injury sustained by a family member affects all family members. It is consequently important that a child’s need to be involved in a family member’s care is clearly recognized by healthcare professionals. The aim of this study was to describe healthcare professionals’ approaches to children as relatives of a parent being cared for in a clinical setting. A web-based study-specific questionnaire was sent and responded to by 1052 healthcare professionals in Sweden. Data were analysed using descriptive statistics and qualitative analysis. The results show that guidelines and routines are often lacking regarding involving children in the care of a parent. Compared to other areas, psychiatric units seem to have enacted routines and guidelines to a greater extent than other units. The results indicate that structured approaches based on an awareness of the children’s needs as well as a child-friendly environment are vital in family-focused care. These aspects need to be prioritized by managers in order to support children’s needs and promote health and wellbeing for the whole family.
Introduction
In Sweden, several thousand children (0–18 years old) live with parents affected by a serious physical or mental illness, and approximately 4000 children lose a parent each year as a result. 1 Several studies have found that children of parents with different diseases, or who die, experience psychosocial impact including anxiety and emotional and behavioural problems.2–4 Research has shown that being involved and knowing what is happening to the parent is crucial to the child’s health, wellbeing and relationships.5,6 If children feel that they are left out and not involved in the ill parent’s situation this may lead to suffering such as being sad and worried. 7 The results of a study by Wong et al. show that children have experienced a need for: support, listening and understanding, encouragement and reassurance, tangible assistance, communication about the disease, and engagement in normal life experiences. 8 Children want to be involved in order to feel important, content and reassured when visiting their parent. 5 To be able to visit is an important means of receiving information and becoming involved. 9
Family-focused care (FFC) is based on an attention to the perspectives and needs of the entire family as well as how the nurse experiences, perceives and deals with the caring relationship between them. A fundamental concept of FFC is that illness of a family member affects all the other family members individually, but also the entire family and vice versa. 10 In order to secure children’s rights, an addendum to the Health and Medical Services Act (HMSA) was launched in Sweden in 2010, stating the responsibility of healthcare policy to consider the child’s need for information, advice and support when his/her parent has a physical or mental illness, or dies unexpectedly.11,12 Moreover, parents may feel ambivalent about their children’s involvement in their situation and worry or be insecure about the type of information the child can handle. 13 In addition, parents may experience a lack of knowledge and ability in communicating with their child especially about their illness, 14 which indicates that they need support and guidance from professionals. 15 Parents who have been open to their child visiting them, have expressed that the visit was good for the child since it especially helped the child to feel involved. 16
Healthcare professionals (HCPs) are positive, in principle, to children’s involvement in their parents’ care, although children in most clinical areas are restricted from visiting for various reasons and few departments encourage it.17,18 Nurses have also reported being anxious and insecure in meeting children as relatives. Some reasons for this may be their lack of knowledge about meeting with children of patients, time constraints, absence of guidelines and routines; in other words, a non-child-friendly environment.19,20 Previous research indicates that children, regardless of age or family situation, should be involved in their ill parent’s situation 7 and receive information that affects them about changes or prognosis. 21 However, this must be done individually and consideration must be given to the unique needs of every single child. 7 Psychiatric units have been at the forefront in working with children as relatives, compared to units for patients with somatic diseases 22 where children’s needs seem to be neglected.18,23
By now, the addendum to the HMSA11,12 should have been enacted by all healthcare services and adapted to each unit in Sweden. However, we find that there is a clear gap in research-based knowledge on the enactment of the legislation in terms of implementing structured approaches to give information, advice and support to children as relatives in healthcare settings in order to meet their needs and promote health and wellbeing.
Aim
The aim was to describe healthcare professionals’ approaches to children as relatives of a sick parent being cared for in a clinical setting.
Research questions:
By whom are children as relatives identified? To what extent do the units have routines and guidelines for providing information, advice and support to children as relatives? ^ Are there any differences between psychiatric and somatic units? What are the healthcare professionals’ approaches to children as relatives?
Method
Design
A cross-sectional study, including a study-specific questionnaire with nine closed questions with the possibility to provide comments and three open-ended questions was carried out. 24 The closed questions have been analysed with a quantitative design. The comments and the open-ended questions have been analysed qualitatively using content analysis. 25
Participants
The participants, HCPs (nurses, social workers and unit managers), in one county council in southern Sweden were sent a web-based questionnaire. Inclusion criteria were: HCPs working at a somatic or psychiatric unit located in the county council. Paediatric units were excluded. The questionnaire was sent to 2839 HCPs, and the email containing the web questionnaire was opened by 1549 (54%) of recipients. Of these, 68% answered the questionnaire (see Figure 1).
Study sample.
Procedure
Valid workplace email addresses for all eligible participants were acquired from the hospital’s IT department at the county council. In February 2014, the web-based questionnaire was sent to these addresses. Two reminders were sent to non-responders.
The questionnaire
Frequency and comparison between the psychiatric and somatic units.
Analysis
Descriptive statistics were used to analyse data from the closed questions, and the chi-square test was used to analyse between-group differences. The data from the three open-ended questions and the comments were analysed using qualitative analysis. 25 First, the researchers read all the data to get an overview of the content. Thereafter one of the researchers (SK) made a preliminary categorization based on differences and similarities. The preliminary categories were then discussed and revised by the researchers and rearranged into two categories, with a total of 10 subcategories based on differences and similarities.
Ethical considerations
Ethical issues were considered using the principles of the Declaration of Helsinki. 28 Prior to the study, written information was sent to the heads of the healthcare administrations in the area. The HCPs received an introductory letter along with the emailed questionnaire, describing the study’s aim, voluntariness and confidentiality.
Results
A total of 1052 HCPs participated in the study. The mean age was 44.6 years (median = 45 years). The majority were female (n = 875; 83%), and the most common profession was registered nurse (n = 809; 81%). Of the participants, 120 (11%) were working at psychiatric units and 932 (89%) at different in- and out-patient somatic units.
Results from the statistical analysis
Identification of children as relatives
The results show that at the different units children were identified as relatives mostly by a registered nurse or a combination of different professionals. About six per cent of the HCPs answered that the identification of children as relatives did not occur or that this was not applicable at their unit.
Routines and guidelines for information, advice and support to children as relatives
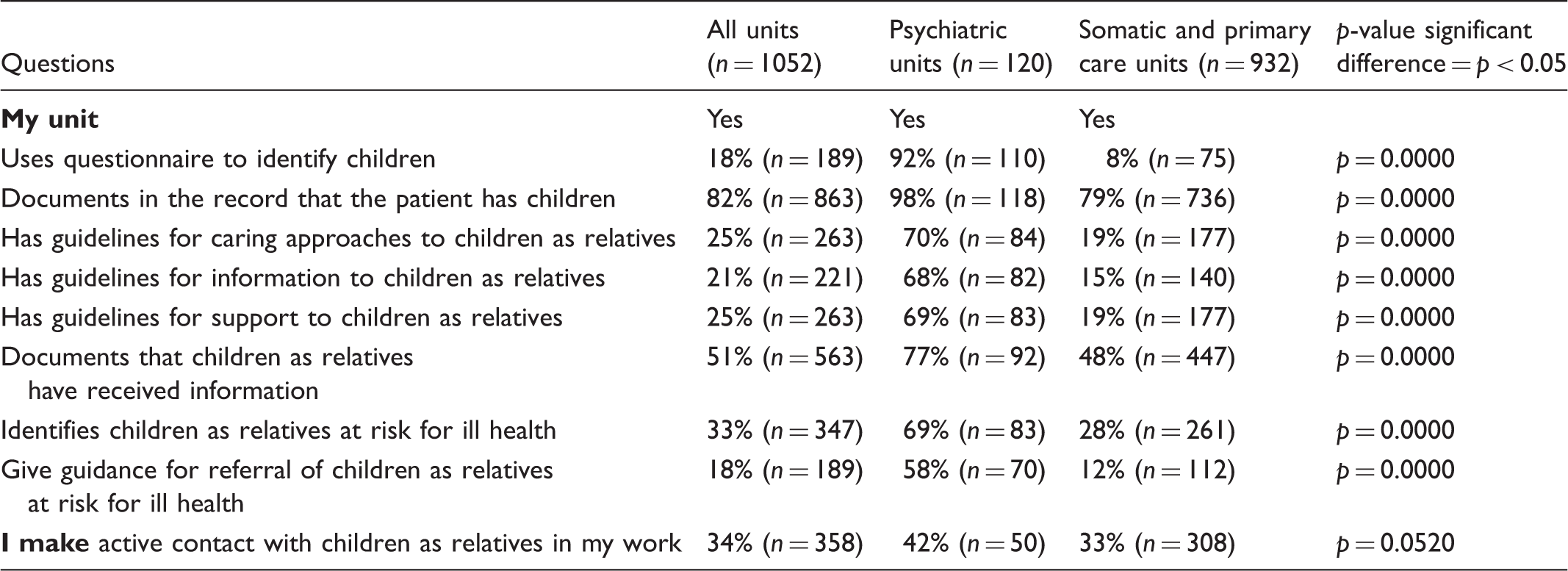
The most commonly reported routines were: documenting in the record that the patient has children (82%); documenting that children as relatives have received information (51%); and of those who identify children, 79% refer to them as relatives at risk for ill-health. Other less frequently reported routines included: using a questionnaire to identify children (18%), and giving guidance for the referral of children as relatives at risk of ill-health (18%).
A fifth of the HCPs reported that their unit has guidelines for caring approaches to children as relatives, for supporting children as relatives, and for providing information to children as relatives. Of the HCPs, 34% reported actively establishing contact with children as relatives, directly with the children or through the parents (Table 1).
Differences between psychiatric and somatic units
The results show that routines and guidelines for approaching, informing and supporting children as relatives are enacted more at psychiatric units compared to other kinds of unit (p = 0.000) (Table 1). Giving guidance for referring children as relatives at risk for ill-health was also more common at the psychiatric units. No differences (p = 0.0520) were seen between the psychiatric units and the others regarding actively establishing contact with children themselves or through their parents in order to invite the child to visit the healthcare unit and ask about his/her need for information and support (Table 1). A similar pattern (p = 0.5600) was also found for those who identify children, when it comes to referring them as relatives at risk for mental ill-health.
Results from the qualitative analysis of the open-ended questions: HPCs’ approaches to children as relatives
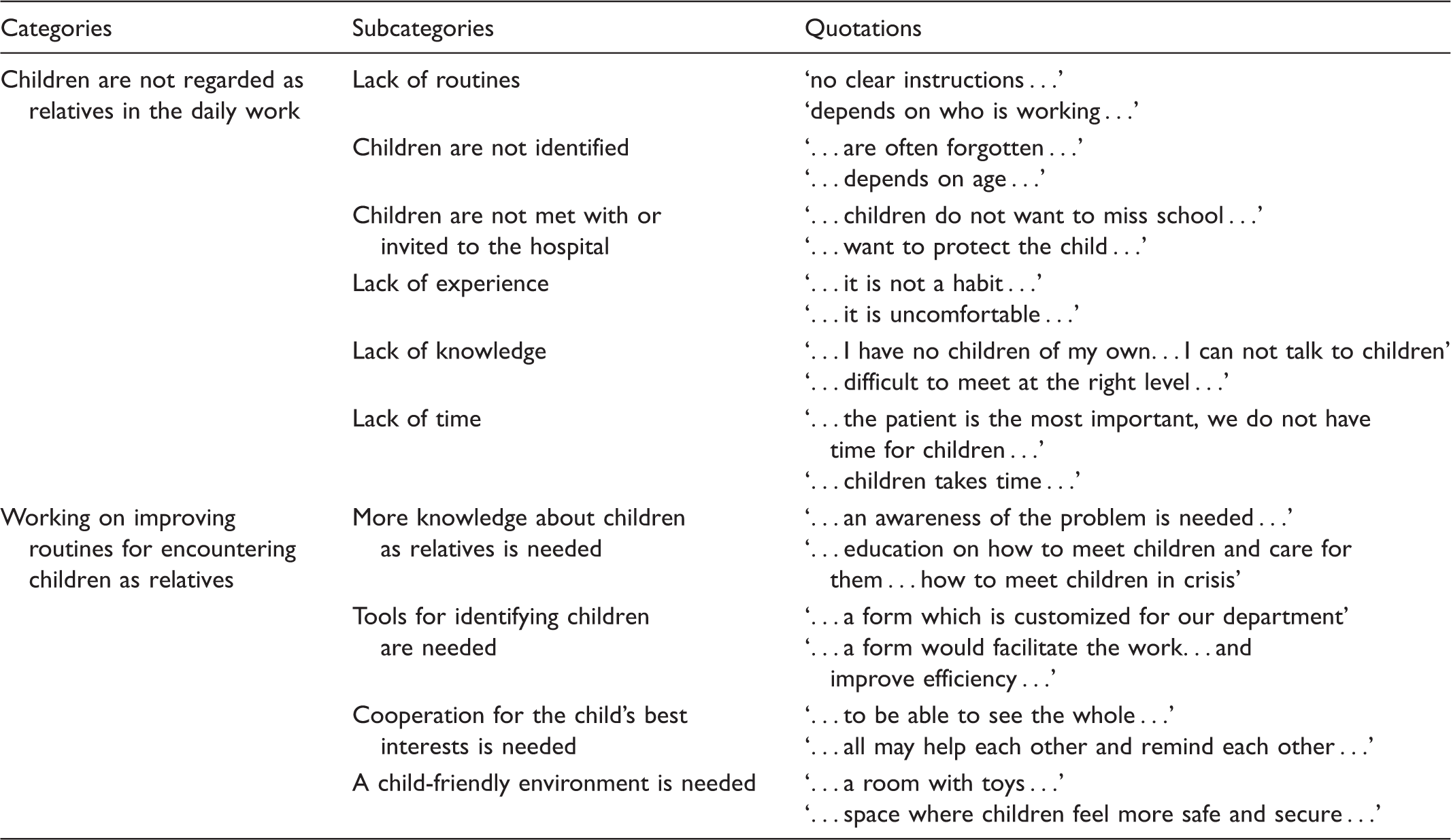
The results presented in categories, subcategories and related quotations.
Children are not regarded as relatives in the daily work
Healthcare professionals experience that children as relatives are seldom part of their daily work. Reasons for this are described as: lack of routines; children are not identified; children are not met with or invited to the hospital; lack of experience, knowledge and time; and a non-child-friendly environment. They state that children are a ‘difficulty’, that it is not ‘our job’ to involve and take care of the patient’s children, and that knowledge about the subject’s importance is lacking.
Lack of routines
HCPs describe a lack of clear procedures for initiating a visit, providing information and giving advice and support as well as of clear procedures for documenting that children have visited or received information. They state that whether or not this is done is very individual, and believe it is up to the parent or the patient to bring the topic up for discussion. The HCPs also describe that there are no clear procedures for identifying children at risk for psychosocial illness. Contact channels and authorities for referring children to other professions do not work smoothly.
Children are not identified
Healthcare professionals find it difficult to always ask if there are any children as relatives in the family. They describe that they are aware that a family form exists but that they do not always use it, or they forget about it. They describe not thinking in terms of involving children; the primary focus is the patient. Historically, children were not to be involved, and this has become a habit. It is described as difficult to reach them or ‘catch’ them, and it is experienced as difficult to dare to ask, to make contact. If the child does not visit the department he/she is not visible and is therefore not an obvious matter, and may therefore be missed. Healthcare professionals describe that they seldom have the children in mind. In the absence of procedures for taking care of children as relatives, they believe the children are forgotten. They also believe that unless HCPs take the initiative to involve the child, he/she will be forgotten.
Children are not met with or invited to the hospital
Healthcare professionals express their ideas about the reasons for not inviting children, including: the child not wanting to receive information or visit; the child feeling ashamed about their parent’s disease; the child not wanting to have responsibility for their sick parent; the child not wanting to miss school; and the child living too far away. The HCPs also describe their ideas related to the parents not wanting their children to get involved. These ideas include: parents not wanting their child to know about their disease and treatment; parents not wanting their child to visit the hospital; and parents feeling ashamed if their disease has caused their child psychosocial problems. Other reasons described by the HCPs include: a difficult family situation, parents being focused on themselves and thereby not having the capacity to bring the child to visit; and parents wanting to ‘protect’ the child from the hospital.
Lack of experience
Healthcare professionals state that they lack experience in taking care of children as family members, and also feel uncomfortable in the situation and therefore prefer to avoid children. They state that it is a ‘hassle’ to take care of children and that it is associated with fear and anxiety if you are not used to it. It is described as being difficult to meet and approach a child ‘in the right way’. There is no continuity, tradition or habit, and there is a reliance on the fact that ‘someone else’ probably takes care of the children. They have not done it before, and therefore do not encourage parents to bring their children. The HCPs describe that they are not used to ‘absorbing’ the situation, and perceived it as difficult to detect that children are in distress when they are not used to this.
Lack of knowledge
Healthcare professionals claim that they lack knowledge about how to communicate with children in relation to their age, experiences and special needs. Since children react differently in different situations, it is described as being difficult to make the situation understandable at a child’s level. Healthcare professionals describe a lack of knowledge about how children should be treated in crisis and about how children react and function in situations of grief and processing.
A lack of knowledge about both the existence of guidelines and laws, as well as how to work according to existing guidelines and laws, was described. Healthcare professionals also describe not really knowing who is responsible for children as relatives, who has the primary responsibility, and which profession has the obligation to take care of the child. Another opinion is that many children are not identified due to ‘common sense’ or ‘feeling’; i.e. the HCPs do what they feel is right, which varies greatly depending on the individual. Knowledge and research evidence are not used as a guiding principle.
Lack of time
Lack of time is a major factor in why children are not met with and informed. Healthcare professionals describe that it is difficult to find time to meet with, inform and engage enough with children, and that there is no space for taking care of children as relatives. They are under pressure to increase production, and have a minimum output to adhere to. They cite time pressure, and say they do not have time to take care of the children as well; the children become an additional source of pressure. A visit from a patient’s child is not included in production, and is therefore not prioritized by managers. Figures and economy become more important than people.
Working on improving routines for encountering children as relatives
Healthcare professionals describe that they need more knowledge, information and training for encountering children as relatives, and also a more child-friendly environment at the hospital. To be able to identify children as relatives, they need tools and to improve cooperation with each other.
More knowledge about children as relatives is needed
Healthcare professionals describe that they need more information and training in the subject. They want a higher awareness of the problem and more regular discussion and reflection on the daily agenda, in order to make the encounter with children more natural. They want more knowledge of the HMSA, and practical tips on how to respond to and talk with children. Knowledge about guidelines, policies and routines is considered necessary.
Tools for identifying children are needed
Healthcare professionals describe that a structured approach is needed to identify children as relatives. They would like to have a special checklist, such as a family form, and other useful tools; and say these tools should be constantly updated and improved. Brochures containing information about children as relatives and their rights can be distributed to parents as a tool for putting the subject on the agenda.
Cooperation for the child’s best interests is needed
Healthcare professionals feel that staff and parents need to cooperate more to facilitate children being involved. When a member of staff first meets the parents, it is important that it be mentioned that there are children in the family and that staff address whether they want to visit as well as what information, advice and support are needed.
Healthcare professionals believe they must have the courage to remind each other and keep each other updated; they must cooperate within the unit. They also describe that a children’s delegate or contact nurse should be introduced in every department; i.e. someone with more responsibility for this cooperation. Healthcare professionals believe a structured cooperation needs to be established with other departments and professions, such as counsellors, hospital church, schools, school nurses, child health nurses and primary care nurses. They also believe that an easy-access telephone number should be established to reach whatever entity has been agreed on within the department for this activity.
A child-friendly environment is needed
Healthcare professionals describe the units as appalling, sterile and filled with technical equipment that beeps and whistles, and argue that children are afraid of this hospital-like environment and of the patient’s appearance. Sometimes the environment is also host to brief meetings or emergency situations, which makes it difficult to go beyond the patient and also take care of his/her children. It is more difficult to establish good contact, trust and security during quick, acute encounters. Healthcare professionals believe that the physical environment for the families to stay in should be improved and adapted more to children’s needs. A room with toys and age-appropriate facilities is needed, as is a room and space where children can feel safe and secure. They describe that if there were children’s delegates in the department to help the HCPs care for the children as relatives, the environment would be more child-friendly. The delegates would update and monitor the rights of children in the department, and help and support staff in issues such as children as relatives, and with informative websites and knowledge banks. The delegates would also have a binder, which they are responsible for keeping up to date. This binder should be kept in the department, easily accessible to all staff. Healthcare professionals describe that the delegate and the binder comprise an asset and a necessity for a child-friendly environment.
Discussion
The results show that there is often a lack of guidelines and routines for structured approaches to identify and give information, advice and support to children as relatives in the healthcare settings. However, the results from the psychiatric units show more routines and guidelines than in other healthcare settings. Work is in progress to improve structured approaches to take care of children as relatives and to adapt the environment in adult units for children. There is a lack of knowledge and experience concerning children as relatives, and cooperation with other authorities and professions could be improved.
Guidelines and routines for structured approaches
The results show that HCPs do not identify children as relatives to any large extent. They describe that children are forgotten by both parents and staff, and they believe that unless HCPs take the initiative to encourage the child’s involvement, the child will be forgotten or will not be invited to participate in the sick parent’s situation. However, 34% of the HCPs in this study reported actively establishing contact with children as relatives. This is an improvement compared to earlier research, 16 which found that only two out of 29 physicians and nurses actively encouraged children’s visits. The consequences of not encouraging visits may be that children do not visit, and are thereby not involved in their sick parent’s situation. This is possibly due to the parent’s own fear and anxiety, a lack of consideration of the importance of involving their child, the belief that children are not allowed to visit, or the belief that involvement would harm them. 16 However, being able to visit is an important means of accessing information. 9
The HCPs in this study described mainly age and time constraints as reasons for not identifying or involving children. Earlier studies confirm this, and also describe age16,18,29 and time constraints19,29 as the most frequently stated reasons for not involving children. Since there are no statistics on children as relatives, there are no data on the actual number of children involved in their sick parent’s situation when they are hospitalized. However, the Swedish Cause of Death Register estimates that several thousand children live with parents affected by a serious physical or mental illness. 1 Research also shows that there are potentially many children who should be involved but are not, and thereby do not receive information, advice or support. 20 Children do need to be involved in their parent’s situation, however, and according to the HMSA,11,12 healthcare has to pay particular attention to this. If the child is involved this may prevent fantasies about the sick relative’s situation, which are often worse than reality. If the child feels involved in the situation, he/she can begin processing what has happened and the prevention of long-term psychological problems can begin. The faster the child’s involvement can take place, including a rapid identification of the child, the better the outcome for his/her psychological health in the long run. 30 Quick identification implies rapidly determining whether there are any children as relatives of patients who are seriously ill or injured. Subsequently, it is of mutual importance to nurses to tell the parents that the unit would happily see the child visit and thereby gain access to information, advice and support. However, support for children seems to depend not on what is best for the patient and child in the long run but instead on more short-term reasons of convenience. 19 To see the child as a family member and practice FFC is of importance. The child will then naturally be involved in the patient’s and the family’s situation and this can prevent future impacts on the child’s psychological health which may result in socio-economic benefits in the long run. 10
The results of this study also show that routines and guidelines are enacted more at psychiatric units. This is likely because since the early 2000s psychiatric units have worked with children’s delegates to involve children as relatives. However, reports have shown that, in reality, children of parents with a mental illness do not always get the help and support they are entitled to. 31 This may indicate that guidelines and routines exist but are not enforced in relation to children’s needs.
The work is in progress
The results of this study show that HCPs are working on implementing routines at healthcare units in order to encounter and take care of children as relatives. This work is proceeding slowly, seeing as the problem had already been identified in the 1980s.32,33 It is up to hospital managers to realize this issue’s significance and speed up the process.
The HCPs also describe that the hospital environment needs to be constructed to be more child-friendly. 34 This may involve both physical space and the atmosphere; i.e. whether time is given to the children and how they are encountered. 5 The HCPs in this study described not having time to take care of children as relatives, which can also be seen in other studies.19,20 They described that their main focus is on the patient, and that time cannot be found to care for both. This lack of time is ‘time that does not relieve’, 35 meaning that children as relatives are missing out on caring time that could alleviate their suffering. Being in an unaccustomed environment means being outside one’s usual context, and may affect health and wellbeing. In their ongoing work, hospitals must meet the demands for a caring environment that is health promoting. It is the relationships between patient, family, children, caregivers, physical space and atmosphere that enable the child to experience their surroundings as caring or not. 36
With its different dimensions, the environment has a great impact on children as relatives, and needs attention when routines are designed. Legislation, knowledge and experience need to be woven into the routines while, at the same time, the routines should not become stiff and completely locked into a method. This would harm creativity. 37
Knowledge and experiences of children as relatives
The results show that HPCs experience a lack of knowledge and experience of children as relatives in healthcare. The focus of the HCPs in this study was more on what they lacked and less on child-related reasons for not involving the child, as research showed some years ago. 27 There may be a shift here in reasons children are not involved. Now that the legislation exists, as well as the knowledge that HCPs need to involve children, the focus may have changed to HCPs’ lack of knowledge and experience regarding encountering children. It is important to make HCPs aware of the legislation, and of the importance of the child being involved through visits or getting information, advice and support in other ways. To succeed in this, knowledge is needed. However, knowledge is a matter of interest. 37 Therefore, it is important that healthcare units create an interest among their employees concerning what needs to be done. It is important to develop curiosity for the subject, because it is when we become curious that we learn. It is also about having opportunities to reflect. Reflection plays a significant role in learning; it is a conscious act with a major place in the understanding process, and has the intention of creating meaning. Reflection may therefore help in encountering and understanding children as relatives. The HCPs would benefit from establishing reflection groups in order to build knowledge and challenge the ethos of the unit. Knowledge can also be obtained through experiences. 37 If children are involved and listened to this increases their chances to understand and thus also the ability to help.10,38 This implies a demand for a more open approach to children’s visits, in which early identification shortly after diagnosis is crucial.
Cooperation with other authorities and professions
The results show that, in HCPs’ experience, cooperation with other authorities and professions could be improved. Structured supportive routines and pliable access to other professions are needed in order to balance time constraints and the needs of children. 27 Units should engage an interdisciplinary team whose members have expertise in the family area of interest. Dialogues and communication with the family are crucial. 39 Family-focused care is a way to connect patients, families and nurses and should be considered and applied more in clinical settings to improve cooperation.10,38 However, children under 18 years of age are very often excluded as family members, 9 and this needs to be considered and changed. Family support programmes for children as relatives and their parents, including meetings with parents and children and age-appropriate information, have been found helpful by children 40 and parents. 41 Other family interventions have shown better communication in the family as an outcome. 42
Methodological reflections
One limitation of this study is the response rate. However, the fact that almost half of the questionnaires were not even opened could be interpreted as indicative of HCPs’ lack of interest in or knowledge of the topic. Another explanation could be that since the email addresses were obtained from the IT department they might also have included HCPs who do not see patients who have children, e.g. working at a geriatric unit, thus making them unable to answer the questions.
Since the topic is considered complex, the questionnaire consisted of three open-ended questions and questions with space for comments to allow the respondents to comment and explain their answers. When using a questionnaire with comments, there is a risk that the answers can be brief or left out. 20 However, many HCPs in this study made comments.
Clinical implications
A structured approach to how to take care of children and their needs should be established and implemented within each specific clinical setting. Early identification should be implemented in order to rapidly determine whether the patient being cared for has children. The nurses could tell the parents that, according to the Act, the unit would happily see the child visit and thereby gain access to information, advice and support. The nurses could work towards creating a child-friendly environment. Reflection groups could be established in order to achieve knowledge and sensitivity to the importance of the issue. Family-focused care should be considered and applied more in clinical settings to improve cooperation with both families and other professionals.
Conclusions
The results show that guidelines and routines for structured approaches to identifying and giving information, advice and support to children as relatives in healthcare settings are lacking. This shows a lack of enactment of the law in accordance with HCPs’ duty to take into account children as relatives in terms of giving information, advice and support. The HCPs describe that they lack knowledge and experience of children as relatives, and that cooperation with other authorities and professions could be improved. Psychiatric units have come a bit further in this work, and it also seems that the work to improve structured approaches is in progress in most clinical settings. However, in order to speed up this work the needs of children as relatives need to be reflected on to make actors aware of their importance. The need for a child-friendly environment, knowledge, experience and the introduction of family-focused care to meet children’s needs is vital, and should be prioritized by managers. Structured interventions are needed in the clinical setting regarding how to approach children in a manner that meets their needs and promotes health and wellbeing, and require further research.
Footnotes
Acknowledgments
We wish to express our sincere gratitude to all the healthcare professionals who participated in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Forte, (Grant/Award Number: ‘Grant number 2013–2082’) School of Health Sciences, Jönköping University, Foundation for clinical cancer research in Jönköping.
Conflict of interest
The authors declare that there is no conflict of interest.