
Abstract
The aim was to investigate experiences of mealtimes and related tasks among people with Parkinson’s disease (PD) and to link these conceptually to the International Classification of Functioning, Disability and Health (ICF). Data were collected by use of semi-structured interviews of 19 people with PD. Inductive content analysis resulted in five categories: 1) Managing mealtime preparations and related tasks, 2) Compromised physical control, 3) Difficulties enjoying meals, 4) Difficulties eating together with others, and 5) Strategies to maintain conventional norms and independence. Deductive content analysis linked the categories to the ICF categories: body functions (mental, sensory, neuromusculoskeletal and movement-related functions); activities (self-determination and chores); participation (interpersonal interactions and relationships); and environmental factors (conventional norms, attitudes of friends and strangers). Emotional and involuntary movement functions were represented in all five inductively derived categories. Eating difficulties may have negative consequences on participation and the emotional wellbeing of people with Parkinson’s disease.
Background
In Parkinson’s disease (PD), motor symptoms are primarily due to loss of dopaminergic cells in the substantia nigra and nigrostriatal tract causing impaired dopaminergic neurotransmission. 1 This in turn disrupts the ability to produce complex, purposeful, and skilful movements 2 which require both intact cognitive pathways for strategy and task formation as well as intact motor pathways for execution of activities 3 such as eating. The basal ganglia coordinate the competing motor mechanisms that would otherwise interfere with the intended movement.2,4 Cognitive impairments seen in people with PD include attention, concentration, memory, executive function, visual perceptual spatial/processing and language. 4 Common motor symptoms in PD include hypokinesia (reduced movements), bradykinesia (slowness of movement), rigidity, resting tremor and, as a consequence of dopaminergic drug therapy, dyskinesia (involuntary movements). 5 All these symptoms can affect mealtimes and related tasks.
In 1817 when James Parkinson first characterized PD, he described eating difficulties as a disabling consequence of the disease. 6 More recently, it has been found that persons with PD may experience problems with mealtime-related tasks such as shopping, preparation, clearing up and socializing. 7 Some of the problems that people with PD may experience during eating are drooling, swallowing difficulties (dysphagia), and problems with limb control that affect their ability to handle cups and cutlery.4,7–13 Eating is also slowed due to reduced rate and strength of chewing, problems manipulating the bolus and difficulty clearing food from the throat. 13 In addition, decreased olfaction (sense of smell), appetite, and gustation (sense of taste) has been described. 7
The understanding of the complexity of shopping, cooking and eating in PD could increase by linking such problems to the International Classification of Functioning, Disability and Health (ICF). 14 The ICF was developed as a standardized common language; a conceptualization and classification of various interacting perspectives of health including biological, individual and social perspectives. The ICF encompasses the components Body Functions and Structures, Activity and Participation as well as contextual (Environmental and Personal) factors. 14 Body structures include anatomical parts. Body functions include physiological and psychological functions. Activity is the execution of a task by an individual, whereas participation refers to involvement in life situations (social perspective). 14 The ICF has previously been used for understanding some of the consequences of PD.15,16 In addition a theoretical model was published in 1987, 11 based on literature on eating difficulties in people with PD which was linked to the International Classification of Impairment, Disability and Handicap (ICIDH), 17 the precursor to ICF. However, to the best of our knowledge, eating and mealtime-related tasks have not been linked to the ICF based on findings from qualitative interviews. Such knowledge may possibly reveal new insights to our understanding of the complexity of this area.
This study is part of a larger project (not yet published) that explores the impact of PD on everyday life, in which aspects associated with mealtimes and related tasks were forwarded by participants. Interestingly this subject was brought up in several situations and contexts. We therefore considered it valuable to analyse these data separately, and to present these findings in a single study. The aim of this study was thus to investigate experiences of mealtimes and related tasks among people with PD and to conceptually link these to the ICF model to get a broader understanding of the meaning of mealtimes and related tasks.
Methods
This study used a qualitative design with inductive,18–20 and deductive content analysis.19,20
Sample
Thirty Swedish-speaking people with neurologist-diagnosed PD were strategically selected 20 by a PD specialized nurse from a south-Swedish university hospital. Exclusion criteria were ongoing psychiatric drug adverse reactions and clinically significant comorbidities including depression and dementia, as determined by patients’ PD specialized nurse at the time of inclusion in the study. Nineteen patients were able to participate and signed informed consent. The sample included 11 women and eight men aged 55–84 years (median [q1–q3] age, 66 [61–73] years) who had been diagnosed with PD 3–27 years previously (median [q1–q3] PD duration, 11 [7–14] years). No data were collected from those who declined participation. The study was conducted in accordance with the Declaration of Helsinki and was approved by the local research ethics committee. All participants provided signed informed consent.
Interviews
Interviews were conducted in the participants’ own homes. None of the participants needed support during interviews from their spouse/partner. Data were collected by means of 60 to 90-minute semi-structured interviews, which were tape-recorded. The interviewer started each interview with the phrase: ‘We are interested in knowing more about how you have experienced the impact and the consequences of Parkinson’s disease, both at present and in the past’. Only open-ended questions related to the impact and the consequences were used, based on an interview guide in the form of a checklist of areas, such as the home situation, occupation, social life, personal care, leisure activities, sleep and rest. When needed, prompts were also used to encourage respondents to expand and explore statements in greater depth. Although the interview guide did not cover mealtimes and related tasks specifically, these areas were spontaneously brought up by the respondents.
Analysis
The recorded interviews were transcribed verbatim. The data were then processed according to inductive content analysis, which included both manifest (describing apparent and perceptible aspects) and latent (interpreting abstract purports) analyses as described by Graneheim and Lundman 18 and Patton 20 according to the following steps: 1) All interviews were read separately by three authors (AW, PH and CSH) several times in order to get an understanding of the essence of each interview and to identify and categorize the primary patterns in the data. The inductive analysis was then mainly conducted by the first and last authors (AW and CSH). 2) Meaning units that caught the essence and meaning of the statements were independently formulated and coded. 3) Clusters of different aspects that emerged in the coded data were organized in subcategories independently by the two authors. 4) The meaning units and the subcategories were then entered into the freeware OpenCode program.21,22 5) Next, the subcategories were sorted jointly by two authors (AW and CSH), with respect to their conceptual representation, and a second coding determining the meaning and the properties of the subcategories was carried out to reach a deeper and increased abstract level of understanding. 6) Subcategories were then organized jointly by the two authors into categories before the latent content of each category was formulated and discussed among all authors.
Theory triangulation by deductive content analysis
A deductive approach can be introduced in different steps in the research process.19,20 In this study we used deductive content analysis as a final step for theory triangulation 20 by linking categories derived from the inductive content analysis to the ICF framework. By using this approach we strove to obtain a wider perspective and a broader understanding of the meaning of mealtimes and related tasks for patients with PD. In the final step all authors reviewed the entire analysis to validate the categories, the deductive analysis, and to ensure that no important aspects were missed.
Results
Inductive content analysis
The latent content analysis resulted in five categories: 1) Managing mealtime preparations and related tasks, 2) Compromised physical control, 3) Difficulties enjoying meals, 4) Difficulties eating together with others, and 5) Strategies to maintain conventional norms and independence.
Managing mealtime preparations and related tasks
This category involved tasks that are necessary to prepare a meal properly and the cleaning up afterwards. Shopping for food was sometimes difficult as not all shops were accessible due to stairs or similar hindrances. For those who had memory problems it was necessary to write everything down, and to try not to forget to bring the list. To be forgetful also caused problems when cooking and baking. Recipes that the participants used to know by heart could be forgotten. Some had problems planning the different steps of baking or cooking processes, which sometimes also included an inability to measure the proportions of the necessary ingredients. Motor problems could also interfere with the tasks, for example sudden inability to move the arms and/or legs. Problems with food preparation were also related to fatigue and to feelings of a decreased pleasure in cooking. … it’s minor things. It may be that I forget to buy some things when I’m shopping or that I forget my shopping list. (7G) I get so confused … and my daughters tried everything, finally they bought a cake mix to which you only need to add water. Because I couldn’t accomplish anything, I just mixed everything up, how to measure the ingredients and things like that … and in the past I always used to bake without recipes … always … (2B)
Compromised physical control
Tremor and involuntary movements made it difficult to handle cutlery properly, and glasses and cups could be knocked over due to involuntary movements. Drinking from a glass or cup could also result in spilling. The participants also described the disease as energy consuming in relation to mealtimes and those who had cramps described additional difficulties eating, which resulted in considerable weight loss. I spilled a lot and did a lot of other silly things, it was crazy … (3C) … it’s my table manners … well … I easily spill … and when I eat I need to lean over the plate and shove the food into my mouth which doesn’t look very pleasant … but I have to do it if I want to eat … (9I)
Difficulties enjoying meals
Participants’ ability to taste and smell the food was compromised, which resulted in a limited number of choices of things to eat. Even spicy or salty food could be perceived as tasteless. In some cases it was described that tactile sense was lost as well, i.e. the ability to perceive texture. Meals that were previously favourite dishes no longer brought any joy. However, the imagination or memory of how it used to taste helped. Participants felt a decreased pleasure in enjoying meals together with other people, and that it was difficult to be cheerful amongst others when feeling uncomfortable. I lost all ability to taste, sense and smell … Because I can’t feel what I’m eating. For instance, I went to get something that was tasty and spicy that I’ve always loved to eat in my golden days. But it didn’t taste of anything anymore. (9I)
Difficulties eating together with others
Mealtimes took longer due to eating difficulties, and respondents felt uncomfortable keeping people waiting at the table. Linked to the inability to maintain physical control during mealtimes, the prospect of attending dinner parties could cause stress and nervousness. Eating together with other people was found to be a challenge, and these feelings were difficult to overcome. Some therefore preferred to stay at home alone. For others it was better to walk away and eat alone, away from people’s staring eyes, and feelings of being regarded as strange. They described that they chose to decline invitations or not to invite people to their homes to avoid exposing their shortcomings and disabilities, and the discomfort and shame they felt when being observed by the others. When I was about to start eating, the hands were shaking, I could hardly hold the cup and I felt awful when other people looked at me. It felt like everyone was looking at me and thinking ‘what a strange person’. So when I was going to eat – I walked away from the others – to find a place to eat on my own. (12L) When I was eating … I felt nervous and jittery, you know … I didn’t know what was happening … and finally I couldn’t hide it anymore … that I was shaking … well, it was difficult. You feel ashamed because people might think that you’re an alcoholic when you have Parkinson’s … you have the same movements … (4D) … my husband had to go alone, and it feels tough … hmmm. You avoid inviting new acquaintances in evenings and so on … With those whom I know very well, it’s easier … (12L)
Strategies to maintain conventional norms and independence
Participants described how they tried to adapt in different ways to their difficulties and that adaptation worked to a certain extent. Some felt a sense of accomplishment and independence when making a light meal for themselves without any assistance instead of having a full meal. … then I eat … well … I eat lunch … I make myself some porridge, and two sandwiches … and … then I do the dishes … (10J)
They wanted to maintain conventional norms, e.g. when entertaining, and they tried to find strategies to compensate for their deteriorating function. Some needed to make detailed plans to manage mealtime-related tasks. One strategy was to get help from family or friends to shop and/or cook food. Another was to use catering when arranging a fancy dinner or to send someone to run errands. To order catering was described as ‘less fun’ as compared to cooking, as it took away some of the joy of having friends over. … but that is something that I find exhausting … to have guests … but … but … I’m reluctant to invite people, since I have to offer food. I haven’t had visitors since I fell ill. If I have to have guests, then I’ll buy pre-cooked food. (1A) You need to find strategies to make things work out … If you don’t feel well, you can’t be funny or social or anything like that … And then you don’t invite anybody to your home and you’re not going out … You’re really not in the mood for entertaining … you just want to stay at home … you’re not strong enough to take the fight … it’s too difficult to make the effort. (5E)
Deductive content analysis
Examples of how the inductively derived categories were conceptually integrated with the domains of the International Classification of Functioning, Disability and Health (ICF).
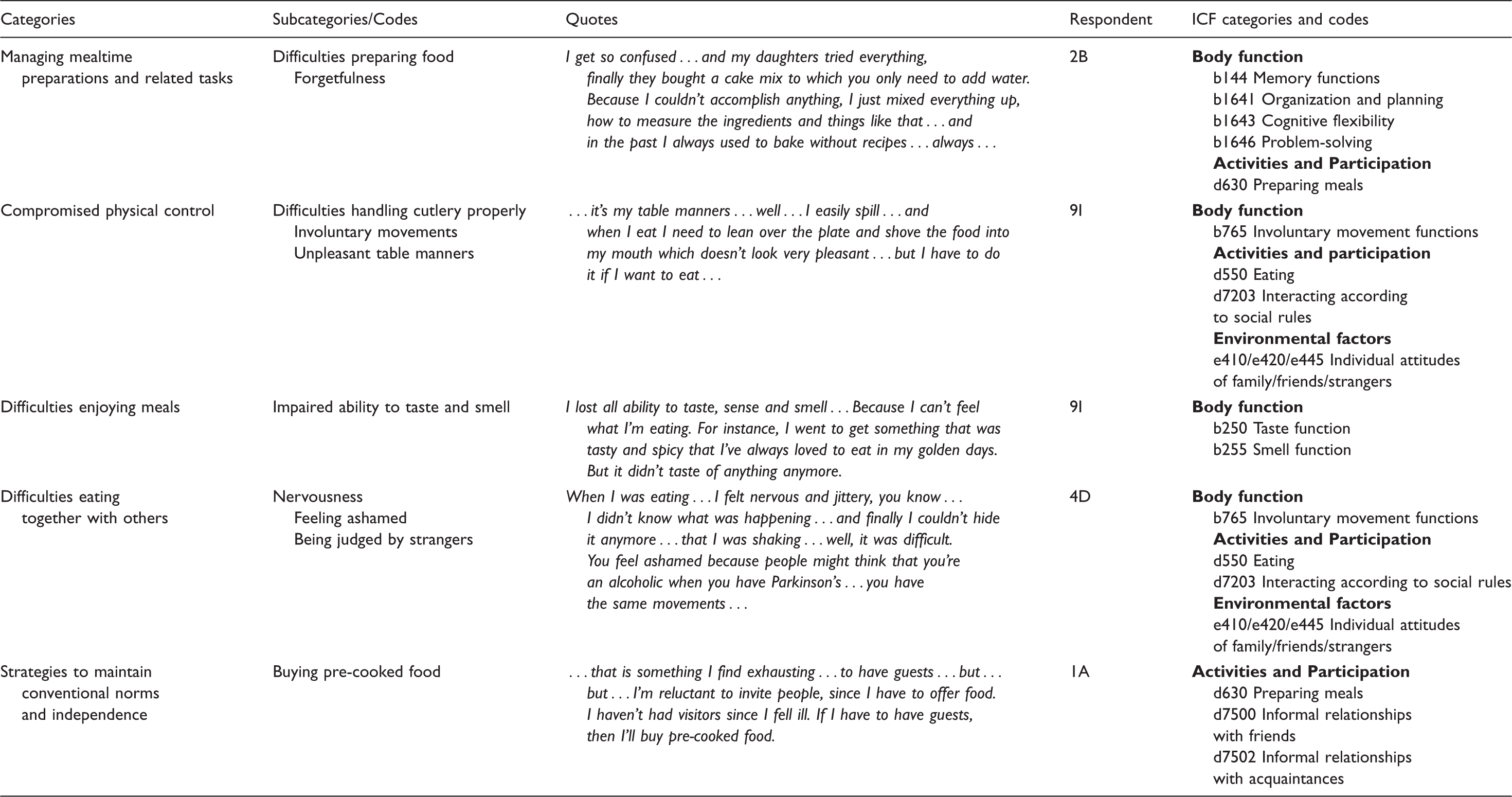
The ICF framework linked to empirically derived inductive categories describing experiences of mealtimes and related tasks.

ICF = The International Classification of Functioning Disability and Health.
X indicates ICF representation within the inductive category.
Discussion
Physical problems during mealtimes and with mealtime-related tasks had a psychosocial impact and negative consequences for the emotional wellbeing of people with PD. This was illustrated by the fact that emotional functions were represented in all five categories when linking ICF to the inductively derived categories. However, it is important to highlight that not everyone experienced all of the problems described in the results. Some faced deteriorating function but were able to compensate and continue to enjoy their mealtimes despite increasing symptomatology.
Broad practical and social activities surrounding mealtimes (e.g. shopping, preparation, clearing up and socializing) were described as impinged by the participants. Eating difficulties affected their self-esteem, enjoyment, family dynamics, and social life. Others have shown that maintaining independence and being able to cook and eat independently were strongly associated with wellbeing and increased self-efficacy.23,24 Self-determination and autonomy were described as important also in relation to buying food, food choices and mealtimes, in line with previous studies.25,26 Persons with eating difficulties expressed a fear of becoming dependent, 24 and common strategies to maintain independence could be to simplify cooking and eating, and to eat cold meals and snacks.7,23,27,28 This was also a strategy described by the participants in our study, who for example described the importance of being able to prepare a light lunch without help. ‘Less elaborate meals’ have been described both as a result of having specific eating difficulties as well as a result of lacking appetite, frailty and loneliness. 28
Precooked frozen dishes and full meals are sometimes chosen by frail elderly people who don’t have enough strength to cook their main meals themselves. 25 Some foods are documented to be problematic for persons with eating difficulties due to impaired motor functioning; for example, bread that has to be cut and buttered. 7 Also the presence of peel, seeds, and other hard and fibrous textures in vegetables 29 may lead to omitting such items from the menu. 30 In addition, elderly persons with PD tend to eat less regularly as well as fewer prepared meals. 30
The deductive analysis linking the categories to the ICF revealed a considerable impact of PD on body functions, activities, participation and environmental factors, which was clearly shown in the categories. Regarding body functions, involuntary movements were represented in all categories, and may be one of the most important factors when it comes to the inability to manage eating in social settings. Especially environmental factors such as the attitude of strangers and the inability to meet norms of conduct at the dinner table brought feelings of shame and avoidance reactions. The feelings of shame and guilt that the participants expressed in our study have also been reported previously.11,31–34 Here, however, the emotional functions were represented in all five inductively derived categories.
The participants felt that lost abilities to taste and smell also negatively influenced the pleasure of mealtimes. Sensory losses may partly be overcome by using distinct flavours and presentations. 35 However, when gustation and olfaction have lost part of their significance in the sensory system it becomes more important to increase the role of other factors in the meal experience such as texture. Some described how the loss of the tactile sense further reduced the pleasure of eating and the selection of dishes. It is well known that texture may surpass taste in importance in perception of food, especially in bland food (e.g. not spicy, low in dietary fibre, cooked rather than raw). 36
A decreased joy in relation to mealtimes also meant a decreased pleasure in enjoying meals together with other persons and sometimes resulted in social withdrawal. The participants did attend social gatherings, but preferably in the company of family and friends. However, avoidance behaviour was more common. One frequently-used strategy in our study was eating alone in order not to expose changes in table manners due to the consequences of PD. To eat together is part of a larger social and cultural context than the food per se. The complexity and co-existence of problems in PD could alter social habits during mealtimes causing cessation of eating out, saying no to invitations to friends or not inviting friends for a meal. Social withdrawal has been described elsewhere as a strategy to handle the eating situation. 24 Also, the frequently-reported strategy of avoiding other people may lead to isolation and feelings of being alienated, which corresponded to ICF aspects of activity and participation. Distinct cultural norms surround mealtimes and having eating difficulties challenges these norms. The mealtime situation thus represents important aspects of the life situation, beyond intake of nutrition. When taking all these aspects into account, the ICF seems to be useful as a framework to evaluate the impact of PD on mealtimes and related tasks, and possibly also in goal settings and needs assessment.
By presenting the complexity of mealtime experiences in relation to the ICF components, we believe that we have shown a rich and realistic picture of the vulnerability caused by the challenges that persons with PD have to manage. Many of these aspects have been addressed earlier 11 but here the understanding is enriched by empirical findings. Further, by adding the deductive approach we deepened understanding about the complexity of mealtimes and related tasks in PD, beyond the inductive findings. The helplessness that participants expressed in relation to the sense of losing control over the situation, facing deteriorating function, and not being able to participate socially was far-reaching and may explain the emotional impact according to ICF in all five inductively developed categories. These aspects need to be taken into account when communicating about eating and mealtime experiences with people with PD. In nursing situations, a person-centred therapeutic approach containing knowledge of all the interrelated aspects presented in this study will facilitate dignified communication to reduce feelings of shame and inferiority, and to enhance empowerment. 37
In our study, the results were structured against the ICF, which presents a positive clinical standpoint classifying functions and disability associated with health. The ICF focuses on functioning and what the person needs in order to overcome activity limitations and participation restrictions. This was a view that the participants in our study were seeking, and which we think is a valid and important perspective in nursing situations.
Conclusion
Inability to control the body and movements due to PD had negative consequences on the ability to manage mealtime situations and mealtime-related tasks. This incapability was linked to all ICF categories, and thus had an impact on body functions, activity and participation. Environmental factors such as the attitudes of friends and strangers, and the inability to meet the norms of conduct at the dinner table brought feelings of shame and avoidance reactions. Physical problems such as loss of involuntary movements, inability to taste and/or smell, and cognitive dysfunction during mealtimes and with mealtime-related tasks thus have a psychosocial impact and negative consequences for the emotional wellbeing of people with PD.
Footnotes
Acknowledgements
The authors wish to especially thank Klas-Göran Sahlén, RN, MPH, PhD, Department of Nursing and Department of Public Health and Clinical Medicine, Umeå University, Umeå, Sweden for valuable advice regarding the OpenCode program. The authors wish to thank Ingrid Åström for assistance with data collection and all participating respondents for their cooperation. Especial thanks to the Swedish house in Kavalla, Greece.
Funding
The study was supported by the Swedish Research Council, The Kamprad Family Foundation for Entrepreneurship and Charity, the Vårdal foundation, BAGADILICO (the Basal Ganglia Disorders Linnaeus Consortium) at Lund University, Sweden, and the School of Health and Society, Kristianstad University, Kristianstad, Sweden, and the Faculty of Medicine at Lund University, Lund, Sweden.
Conflict of interest
The authors declare that there is no conflict of interest.