
Abstract
The aim of this study was to explore child health care nurses’ experiences of conducting health dialogues with non-native-speaking parents. In Sweden, it is not routine that all non-native-speaking parents are invited to a health dialogue. Regardless of language and cultural background, it is important that all parents have the same opportunities to participate. The data were obtained through two focus-group interviews and analysed using qualitative content analysis. The results revealed one theme Need for cultural awareness in the health dialogue and two categories: Overcoming feelings of uncertainty, with a need for more transcultural knowledge regarding what health and health promotion mean in other cultures; and Adapting the process of the health dialogue, whereby interpreters need knowledge about the intention of health dialogues and the content of the tool used in the encounter. Transcultural competence is needed in encounters with parents from other cultures.
Introduction
In Sweden, child health care (CHC) is one part of the health-care system, with the purpose of promoting children’s health but also strengthening parents’ opportunities to improve the health of the family. 1 One way to support families’ health and lifestyle at an early stage is to invite parents to meet a CHC nurse for a health dialogue based on the parents’ health situation. 2
A health dialogue consists of a mutual encounter intended to address lifestyle choices. The health dialogue is a complex communicative activity to create a caring relationship. 3 Different views on health can result in different reactions depending on cultural background, 4 which require cultural competence and awareness of the transcultural context. 5 To be able to create a caring relationship when encountering parents, CHC nurses need to understand the cultural context of families.
However, when the CHC services started to invite parents for health dialogues a limited number of non-native-speaking parents were invited. Therefore, it is of importance to explore the CHC nurses’ experiences when conducting health dialogues with non-native-speaking parents to improve clinical practice, and to ensure that all parents, including non-native-speaking parents, are invited to a health dialogue.
Background
According to the United Nations (UN) all people have the right, without discrimination, to reach their highest level of health. Health promotion is one way in which people can achieve and take responsibility for their health and lifestyle. 6 Structural, long-term information on lifestyle issues like alcohol, tobacco, food and physical activity can reduce a person’s risk of cancer by 30%, 7 of type II diabetes by 90%, 8 and of cerebral insult and heart disease by 80%. 9 A healthy lifestyle results on average in a 14-year-longer life expectancy compared to an unhealthy lifestyle. Within the Swedish population, immigrants have a higher risk of developing an unhealthy lifestyle. 10
Communication is built on relationships between people, 11 and inadequate communication might lower a person’s self-esteem, and ability to cope with stress, which could lead to a poorer outcome of a health dialogue. 12 Bridging the language barrier is important if a nurse is to offer an equitable encounter with a parent who does not speak the same language, 13 as language is strongly influenced by the transcultural context. 14
To provide culturally responsive health care to ethnically, and culturally diverse people, Campinha-Bacote’s model 15 for cultural competence, based on Leininger’s transcultural theory, 16 can be used. The model states that cultural competence is an ongoing process involving awareness of one’s own culture, knowledge about cultural, and ethnic groups, skill to understand other cultural values, encounters involving mutual learning and a desire to meet people from other cultures. 15 Transcultural theory is based on the cultural context and codes people live by, taking into account a person’s philosophy of life, religion, politics, economy, values, social structure, cultural history and family ties. 16 A person’s cultural background also affects the relationship he or she has with the health-care system and caregivers. 17 Regardless of language and cultural background, it is important that all parents have the same opportunities to attend a health dialogue, according to the principle of equality. 18
Earlier research has shown that health dialogues with native-speaking parents enable CHC nurses to understand the families’ health situation and therefore improve their support to the child and their family. 2 However, to the best of our knowledge there is no study exploring CHC nurses’ health dialogues with non-native-speaking parents.
Aim
To explore CHC nurses’ experiences of conducting health dialogues with non-native-speaking parents.
Methods
Design
A qualitative approach was chosen for exploring CHC nurses’ experiences. Focus-group interviews were used for data collection. 19
Settings and participants
Child health care in Sweden is based on a national monitoring programme, including health supervision, screening examinations, vaccinations and parental support. Child health care has a long tradition in Sweden, and is free of charge and voluntary to attend. 20 In one county council in Sweden, since 2007, CHC nurses have conducted health dialogues with parents, based on the health of the parents, with the purpose of promoting good health for the entire family. 2 During the health dialogue the CHC nurses use a pedagogical tool, the Health Curve, comprising three questionnaires about exercise and eating habits, alcohol and smoking habits, life situation, psychological health and a health profile. 2
Characteristics of participants.
Data collection
An interview guide was used, after confirmation by an experienced research nurse, based on questions about the nurses’ experiences of conducting health dialogues with non-native-speaking parents. Follow-up questions regarded the use of an interpreter as well as challenges in their work.19,21 A moderator led the interview, and an assistant took notes without interacting in the interview. To allow the participants to reflect and confirm, the assistant presented a brief summary at the end of the interview. The interviews were audio-recorded.
Data analysis
The interviews were transcribed verbatim, 19 and the principle of qualitative content analysis described by Graneheim and Lundman guided the data analysis. 22 The text was first read several times to obtain an overview of the content. Second, based on the aim, meaning units were marked; and third, these were condensed into codes. Fourth, codes with similar meanings were grouped into six subcategories and similar subcategories were grouped into two categories. In the fifth stage, an overall theme emerged from the content of the text.
To enhance the rigor and trustworthiness of the analysis, the coding procedure was done by the first author (LJ) and a colleague (AH) separately, and disagreements were discussed until consensus was reached. During the analysis process, the authors (LJ, MG, BH) enhanced credibility by performing the analysis until consensus was established. 22
Ethical considerations
The study has been conducted according to Swedish law concerning ethical regulations when interviewing medical staff. 23 The study was performed according to the guidelines of the Declaration of Helsinki; 18 i.e. the CHC services managers gave written permission to conduct the study, and the participants received verbal and written information about the study. Participation was voluntary, and participants could withdraw at any time.
Results
Child health care nurses’ experiences of conducting health dialogues with non-native-speaking parents.
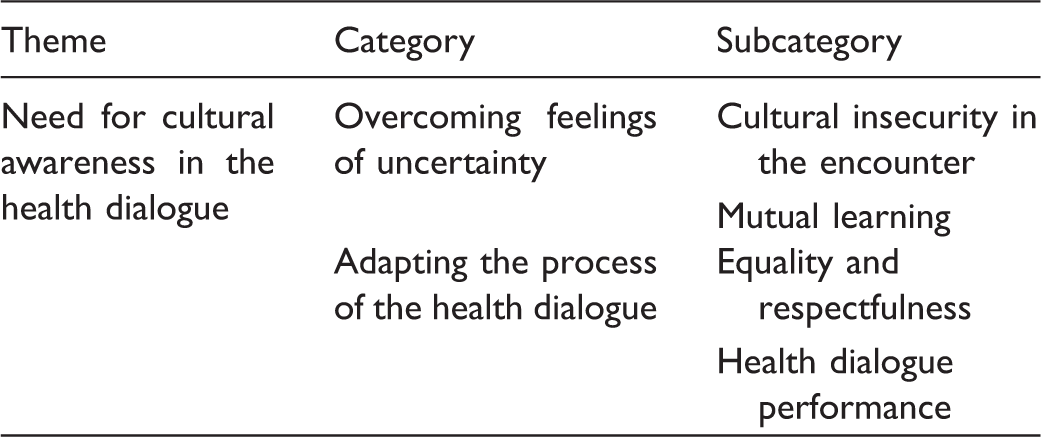
Need for cultural awareness in the health dialogue
The results consisted of an overall theme of a need for cultural awareness in work with health dialogues, to fulfil the need of adapting the work culturally in various ways, to allow nurses to feel secure in the encounter with parents and in performing the health dialogue.
Overcoming feelings of uncertainty
The nurses described a need to (as well as ways to) deal with their feelings of uncertainty. In the encounter, cultural insecurity among the nurses concerned how the dialogue was perceived by parents, when cultural differences might appear. Through interactions between nurses and parents, the nurses’ knowledge was enriched, and they gained inspiration in their work. Through the health dialogue nurses and parents gain knowledge about each other’s cultural context through mutual learning.
Cultural insecurity in the encounter
Before the nurses started to conduct health dialogues their feelings were mixed, with concerns about how they would be culturally perceived by the parents. At the same time, they experienced the encounter as challenging. They feared the advice they might give the parents could be misinterpreted as conflicting with their ideals for a healthy lifestyle, or that it would affect their future relationship with the parents. This was expressed as: I wasn’t that positive about this at all … now we’ll accept this challenge and test it, and see and feel, and I thought it was great; I think it felt really good. (FG1)
It emerged that a deficiency of cultural knowledge created insecurity regarding how the parents perceived the health dialogue and how they related to concepts such as health. It was hard for the nurses to understand a parent’s cultural food habits. Another fear was how it would be perceived if, during the health dialogue, it was discovered that the parent had a disease that needed medical consultation. The nurses experienced that when the parents’ answer had gone through the interpreter, it was sometimes perceived as irrelevant. They did not know what had gone wrong – whether the interpreter had translated incorrectly or if it involved something lying deeper in the parents’ culture, meaning something different in their language. The nurses mentioned health as an example of a word that could be hard to translate, since it can have different meanings in different languages. There seemed to be different perceptions within various cultures regarding what health was, and the nurses perceived that it sometimes seemed as if the word did not really exist. Much of this created insecurity among the nurses: You can wonder whether the interpreter is unprofessional, or if it’s a cultural issue so that you don’t understand each other even with an interpreter, because that way of thinking and those expressions don’t exist in their reality. (FG2)
Mutual learning
The nurses expressed they gained more knowledge about the families through the health dialogue. The knowledge was useful for their continuing supporting work promoting children’s and families’ health. The Health Curve tool, with its health questionnaire, helped them understand the parents. One experience that was highlighted as enriching concerned how the health dialogue offered knowledge not only about the family’s life, food and culture in their homeland, but also how they were getting on in Sweden: For us, I think, it is fun to have a bit of knowledge about their culture and their diet; I think that’s very interesting. (FG2)
When parents verbally expressed that they appreciated the dialogue this enriched and inspired the nurses in their future work, and it served as a confirmation when the health dialogue yielded good results, for instance when the nurse saw a mother at the street walking with her child. Confirmation from the parents gave the nurses a response to the encounter and the health dialogue. It was apparent that the nurses wanted to encourage their colleagues who had not yet conducted this kind of health dialogue to start doing so, because it was inspiring: Whoever hasn’t dared to do it, you encourage them to try because you get so much back … they’re positive meetings, even for us nurses. (FG1)
At the family’s next visit with the nurse, it was important to follow up the health dialogue with a question about how the parents had perceived it and whether they had any questions, to avoid misunderstanding: Then the next time I also bring up a bit about how you felt, what did you think, is there something you’re wondering about now that it’s been a while. (FG1)
Adapting the process of the health dialogue
The nurses described a need to adapt the process around the health dialogue. The nurses experienced the importance of respect for the equality of all parents in their right to a respectfully conducted health dialogue. The nurses described difficulties they experienced when trying to fulfil performing the dialogue; how they, in a creative and flexible way, adapted the dialogue to the parents’ wishes and needs. When the interpreter is an intermediary the nurses described the risk of miscommunication between themselves and the parent.
Equality and respectfulness
It was obvious to the nurses that everyone should have the same right to a health dialogue, regardless of background or language: Even considering fairness and all that, everybody should have the same care regardless of where you come from or what background you have and all that. (FG2)
They perceived that non-native-speaking families were interested in, and had the same need to talk about their health situation as did native-speaking families. They pointed out the importance of conducting the health dialogue while showing respect and humility for the parents’ culture and way of thinking, using the trust capital they had gained through knowing the family to help the parents perceive the dialogue in a positive way. In the interaction with the interpreter, questions should be translated so that the respectfulness was conveyed to the parents, or to acknowledge cultural aspects, e.g. using a female interpreter for a Muslim Somalian woman. When there was mutual respect in the encounter between nurse and parents, the next visit would be easier.
Health dialogue performance
The family perspective was important to the nurses, because the parents’ lifestyle habits also might affect the child’s future lifestyle habits. It was easier to perform the health dialogue in a positive way when the parents had already received information about it. The health dialogue is not like the other visits within CHC services; therefore, the nurses felt it was important to know the interpreter and whether he or she had some knowledge about the health dialogue and the Health Curve: If it were possible to have interpreters who’d worked a bit with this, more or less, and had also been a bit prepared beforehand … not health interpreters, but who know, who are familiar with the questions a bit beforehand and know what we’re going to ask about … just some basic knowledge of it. (FG2)
One experience the nurses had regarding marketing was that people who had taken part in health dialogues told their friends, who were then inspired and wanted a health dialogue themselves. However, the nurses’ experiences in marketing were different. Parents invited by an interpreter when their baby was ten months old had a high response rate, according to the nurses. Other parents were contacted through invitations sent in window envelopes; responses here were mixed. Some parents attended to quite an extensive degree when they received the invitation from their nurse, even if they did not always know why they had been invited, while others came to a small degree: A lot of it’s the marketing; is the idea to get them to us? It’s like we say, sending window envelopes isn’t good marketing. I take my bike down to deliver the letter, and then they come. (FG2)
The nurses experienced that the health dialogues took a long time and that parents could have difficulty filling in the health questionnaire. If the forms were translated into other languages it could be easier, but translating verbatim could cause problems as certain words could have different meanings. They tried angling the conversation to encourage the parents to see the positive side, and also invented creative ways to bridge the difficulties with the forms; for instance, instead of listing all the answer alternatives to a question in the health questionnaire they asked an open question: I think that the more Health Curves you do the better you get at rephrasing the questions … you ask ‘Do you eat bread’ … that you ask that way instead of rattling off all the alternatives, so you can tell what’s best for you … then double-check … so you know that what you write down will be as correct as possible. (FG2)
The interpreter was seen as an intermediary between parent and nurse. The nurses’ experiences diverged as to whether using a telephone interpreter or someone physically present was best during the health dialogues. A telephone interpreter could reduce the risk of miscommunication between nurse and parent, for example due to the interpreter’s body language. I always have just an interpreter over the telephone, because I don’t want to have anyone else with us who in any way shows what they feel or think. (FG1)
It sometimes gave the nurses the feeling they and the parents were speaking to each other, forgetting that it was going through an interpreter. It emerged that the interaction could be disturbed due to eye contact or body language; or, if the parent knew the interpreter, the fact that they could meet each other in their daily life could affect what was said. The presence of another person in the room could impede the conversation. For the health questionnaire and more personal questions, an interpreter being physically present was helpful. The interpreter could also explain different cultural aspects. Verbatim translations were expected so that the communication could be kept between nurse and parent. The language barrier, with different codes and nuances, was sometimes too difficult to overcome: We’d never had an interpreter, but when I tried to have this health dialogue with her it didn’t work; then it was so clear, so there we could’ve used an interpreter because she couldn’t interpret these things. It’s a bit a case of nuances, but if somebody had said these words and explained in her own language what I meant, I think we would’ve pulled it off. (FG1)
Discussion
The nurses in this study experienced the health dialogue with non-native-speaking parents in a positive way, and encouraged colleagues who had not yet conducted these health dialogues to do so. The nurses claimed it was important for all parents to be offered health dialogues no matter their cultural background. People with language difficulties are already in a vulnerable situation, and previous studies have shown that they participate in CHC parental groups to a lesser extent. 24
The nurses in this study claimed that they got to know the family in a better way through the health dialogue, and this facilitated offering future support to the family. This has also been previously confirmed in health dialogues with native-speaking parents. 2 The family perspective was important to the nurses in the present study, who stated that the parents’ lifestyle habits also might affect the child’s future lifestyle habits. 25 Nurse-led health promotion is desirable in early childhood for preventing cardiovascular disease, and needs to be directed at the whole family. 26 When nurses encounter parents who want to improve their lifestyle habits, it is important to be supportive and create a sense of wellbeing. 27 The difficulties the CHC nurses experienced in their encounters with non-native-speaking parents and their children created a concern that the health risks of these children would not be detected. 28
Regarding how health care and health promotion were perceived, both linguistically and culturally, it was important for the encounter to be interactive. In this study, the results showed a deficiency in cultural competence on the part of the nurses; they were concerned about how the parents perceived the dialogue. The results also indicated insecurity about different cultures. It is important to be aware of the influence of one’s own culture, to have knowledge about other cultures, and to discover the interaction between cultures. 29 According to Campinha-Bacote’s model, cultural awareness is the first step and a vital part of the ongoing process of becoming culturally competent. 15 Previous research shows that nurses desire guidelines and education in order to become culturally aware and culturally competent in encountering and supporting these families.29,30 Through education and continual training in cultural competence based on Campinha-Bacote’s model, nurses describe more security in encounters with parents from different cultures. 31 The nurses’ concerns and feeling of insecurity in this study indicate a need for transcultural nursing knowledge. When they adapt transcultural nursing, it has provided them with tools for reaching their goal to appropriately encounter parents in their particular situation. The parents’ self-esteem, self-respect and cultural security increase when elements of transcultural nursing are adapted. 32
The results of the present study revealed a concern over how the interpreter translated concepts such as health, what the words meant to parents from a cultural perspective, and whether the translation was delivered with similar content. As one way of ensuring that a parent has understood the concept, the nurse is advised to ask the parent to retell what has been said. 33 In this study, nurses felt it could be useful if the interpreter had had some introduction to the health dialogue, and how the encounter is usually performed. This is confirmed in another study, where it was desirable for the interpreter to have some knowledge about the subject, manuals and checklists before the visit to support a successful translation. 34
The present study shows that the nurses performed health dialogues in a creative way based on the parents’ circumstances. They asked open questions, and by using the parents’ answers they could more easily fill in the questionnaires in the Health Curve. This also facilitated the dialogue for the nurse, parent and interpreter. Flexibility was important for promoting an interactive dialogue and encounter with the parents. Previous research shows that survey questionnaires in combination with open questions and transcultural nursing provide richer data. 34 Transcultural nursing increases the possibility that the health dialogue will be useful 15 and will have a positive impact on the family’s future health. 35
The limitations of this study are that only data from one county with one pedagogic tool were included. The low number of participants was surprising considering how many could have participated if they had been following the regional statements. Although participation was limited to nine nurses, the data from the two focus groups gave a rich amount of information. 19 However, one limitation might be the positive approach by those nine CHC nurses participating in the focus group interviews. Qualitative content analysis was assessed as an appropriate method when describing an area of limited knowledge. The results have been discussed with nurses working in CHC, which could strengthen conformability and trustworthiness. 22
Practice implications
Although the study has its methodological limitations, the findings indicate that education in transcultural theory may improve transcultural communication. A combined and integrated educative intervention for interpreters and CHC nurses could also provide new knowledge and better interaction in cultural encounters. Moreover, a manual describing alternative ways of phrasing specific questions contained in the health questionnaire could be of value in clinical practice. A future expectation is that nurses will invite all non-native-speaking parents to a health dialogue, and be strengthened in these encounters. A future research area is investigating the experience of non-native-speaking parents of participating in the health dialogue.
Conclusions
In order to prevent situations where nurses become worried and insecure as to whether the parents they meet have understood the message communicated in their dialogue, transcultural competence should be integrated in their professional work. The nurses in this study experienced that in health dialogues they became acquainted with the families in a better way. To improve the communicative encounter nurses need to use a more open way to ask relevant questions that show an understanding of the cultural context of the individual parent.
Footnotes
Acknowledgements
We wish to thank Anna Hildingsson, who participated at the beginning of this work, the CHC managers in the county, and the nurses who participated in the study.
Funding
The study was funded by the Unit for Research and Development in Primary Care, Futurum – Academy for Health and Care, Region Jönköping County, Sweden.
Conflict of interest
The authors declare that there is no conflict of interest.