
Abstract
Different organizational climates and cultures appear within healthcare organizations and vary within their associated subgroups. The healthcare and nursing work environments have been studied from the individualistic perspectives rather than from organizational or nurse managers’ group perspectives. The aim of this cross-sectional study was to examine the differentiation of organizational social contexts in hospitals. The organizational social context (OSC) measurement system was used to assess characteristics of culture, climate and morale. The data have been statistically analyzed using within-group consistency (rwg), ANOVA-based eta-squared values and interclass correlation coefficient (ICC). The results revealed that at the divisional level, the organization’s social context is different.
Introduction
Healthcare organizational culture differs from other institutional cultures because hospitals have their own unique organizational structure and management. 1 Healthcare organizations have a broad primary culture, but also cover the subcultures of different work units and these can vary considerably. 2 There is evidence that organizational cultural value systems positively affect the delivery of care. 3 Healthcare organizations have traditionally been divided into the functional groups of nursing, medical specialties and administration, and medical specialties play an important role in hospital organization. 4
Organizational culture, climate and morale may be viewed as multilevel and multidimensional constructs, 5 which together constitute the organization’s social context, 6 which plays a key role in the organization’s outcomes. 7 The three constructs of the organizational social context have intertwining connections with each other. Culture influences the organizational climate, and individual attitudes, including positive attitudes towards work.8,9 Culture profile determines an organization’s strategic planning and how it functions within its society. 10 There is also evidence that in an organizational change, employees’ perceptions of cultural and climate factors change, but that these can be modified. 11
Organizational culture refers to shared expectations; beliefs and norms that affect employees’ perceptions, behaviors and emotional responses to the workplace,9,12 and is a dominant feature in discussions about modernizing healthcare. 13 Organizational culture guides and shapes behaviors and attitudes. It is also an element of the organization which is malleable and controllable. 14 In this study, culture refers to ‘the way things are done in the organization’.15(p.315) Organizational culture has been found to be partly created by managers. 16 It is vital to identify or assess the organizational culture prior to embarking on a change process because this may help the change leaders to create a positive cultural structure.1,17,18
According to Verbreke et al., 15(p.322) climate is defined as ‘the way how people perceive their work environment’ and may be divided into psychological climate and organizational climate. Psychological climate, at the individual level, consists of the psychological impact of the work environment on the individual worker (for example emotional exhaustion). Organizational climate is understood as the shared perceptions of an organizational unit or division.8,19,20 These team or group climate perceptions provide information about their members’ shared attitudes, performance and outcomes. 21 The perceptions of working and practice circumstances are influenced by managers. 22 According to James and James, 23 the organizational climate in a team may include stress from one’s role and lack of harmony, challenge and autonomy, manager facilitation and support, and work-group cooperation.
In contrast to culture and climate, morale is an individual-level construct which indicates the employee’s commitment to the organization and satisfaction with his or her own work.20,24 It can be described as a positive or motivated employee psychological state. There are several factors that can influence this state; for example, pride in the organization and its goals, the opportunity for professional growth, payment, loyalty to co-workers, and faith in management. 25 Morale is usually identified as an individual’s attitude towards work, but in this study it is evaluated as a collective group-level phenomenon and is used in line with theory previously proposed by Glisson and James, 8 and Glisson et al.19,20
First-line nurse managers are primarily responsible for linking the clinical ward to the rest of the organization. 26 They play a role in establishing and maintaining an organizational culture in their work unit, 27 and thereby promote safe, effective and high-quality patient care. 28 A positive social context helps nurse managers to lead the unit more effectively, and to feel that they can act independently and gain more support. A negative organizational culture, however, may cause nurse managers to feel that they are disrespected and unappreciated in their roles. 29 As Trus et al. 30 mentioned, organizational culture and climate seemed to be connected with nurse manager work-related empowerment but at the same time Trus’s 31 research showed that nurse managers’ structural empowerment is only displayed on a moderate level.
In recent years, research in healthcare has focused on culture and climate from a patient safety perspective,32,33 as well as on the work environment’s attraction factors (forces of magnetism).34,35 The healthcare and nursing work environment has been studied from the individualist perspective rather than from an organizational or nurse managers’ group perspective. 28 Less research has been conducted on healthcare’s organizational social context. This study examines the organizational social context of different divisions, as viewed by first-line nurse managers’ groups in terms of how they see their work environment where they manage nursing care. The present perspective is therefore based on collective perceptions and interpretations.
Aim
The aim of the study was to examine the differentiation of organizational social contexts (organizational culture, organizational climate and morale) at various divisional and organizational levels in hospitals, as perceived by first-line nurse managers.
Methods
Design
A cross-sectional, descriptive survey design was used to analyze how culture and climate vary in teams, by examining within-group consistency and significant between-group differences.
Ethics
Permission to conduct the study was obtained from each target organization. No further permissions from associated ethical committees were deemed to be required (Pirkanmaa Hospital District Ethical Committee, Finland approved this). The participants were informed about the opportunity to participate in the study via their own supervisor through a cover letter created by the researcher. Each respondent consented to participate in the study by completing the research questionnaires, which were completed anonymously.
Sample
A convenience sample of 11 hospitals, with a population base of approximately 250,000 persons was used. This offered consistent types of divisions (surgical, medical and psychiatric) for each participating hospital. In Finland there are five university hospitals and 15 central hospitals that provide public specialized healthcare. A group consensus estimate (rwg) was used and it was required that each group comprised a minimum of six participants.8,36,37
After receiving research permissions participants completed a questionnaire at occasions organized by each of the target organizations in the presence of the researcher. The retrieved data consisted of the responses from 264 first-line nurse managers in 30 different units, including 10 groups of each of the three functional divisions. All organizations have three functional divisions with a group size ranging from 6 to 16 persons (Md = 8.8).
Instrument
The organizational social context (OSC) measurement system was used to assess characteristics of culture, climate and morale, with total of the 105 items.20,37 Social context examined three dimensions: organizational culture, climate and morale. Organizational culture consisted of measures of rigidity (14 items), proficiency (15 items) and resistance (13 items). This was measured as the behavioral expectations reported by members of the group or organization. 20 The organizational climate measure addressed stress (20 items), engagement (11 items) and functionality (15 items). Morale (17 items) measured the first-line nurse managers’ commitment to the organization and their job satisfaction. 38 The survey also contained 15 questions on the respondents’ backgrounds.
Data analysis
Statistical analysis of the survey results was carried out using PASW Statistics for Windows, Version 18.0 (SPSS Inc., Chicago, IL, USA). T-scores were used for each dimension of the OSC, and measured deviations from the group average. These were computed by averaging the dimension scores for each group, subtracting this from the average dimension scores of all groups, and then dividing them by the standard deviation obtained from all groups.37,39 The homogeneity of variances was tested before comparing means (ANOVA). The level of statistical significance was set at p < 0.05.
Three complementary measures of within-group agreement were used to assess group-level agreement. Within-group consistency was assessed with (rwg) which measures the variance that determines the agreement of responses within the group. This was calculated by comparing an observed group variance to an expected random variance. 39 This within-group reliability statistic (rwg) is not dependent on between-group variance and provides a measure of agreement for each group rather than for all of the groups. According to Glisson and James, 8 values of rwg = 0.70 or greater indicate an acceptable agreement among individual responses on a scale. On this basis it can be assumed that there is agreement in a working unit on the culture and climate scales.
Between-group differences were assessed using ANOVA-based eta-squared values and intraclass correlation coefficients (ICC). 39 These were calculated using the between-group and within-group sum squares and mean squares. ANOVA-based eta-squared is useful in describing how variables are behaving within this sample of first-line nursing managers if we can compare effects of grouping variables in related studies. Equal between-group and within-group variance suggest chance similarity among first-line nursing manager group members. The ICC refers to the proportion of total variance that is explained by unit membership with values ranging from –1 to +1.37,38 ICC values are typically less than 0.20 and usually much smaller than eta-squared values. 39
Results
The variation of organizational social context
By ANOVA analysis no significant differences between the 11 organizations were found. However, it is often the case that while there are no significant differences in climate and culture at the organizational level, there may be more variation in OSC scores seen at the subgroup level. For example, one group might have an extremely low average for resistance, whilst another has an extremely high average. Combining these two groups into a higher (organizational) level would therefore result in eliminating the variation in OSC scores.
As shown in Figure 1a, each culture profile type represented a different subgroup or division. Again, variation in responses between subgroups meant that one group’s cultural rigidity may be very high, whilst its cultural proficiency may be seen as low. Correspondingly, Figure 1b provides examples of the best and worst culture profiles in the three divisions.
Examples of culture profiles from three divisions (surgical, medical and psychiatric).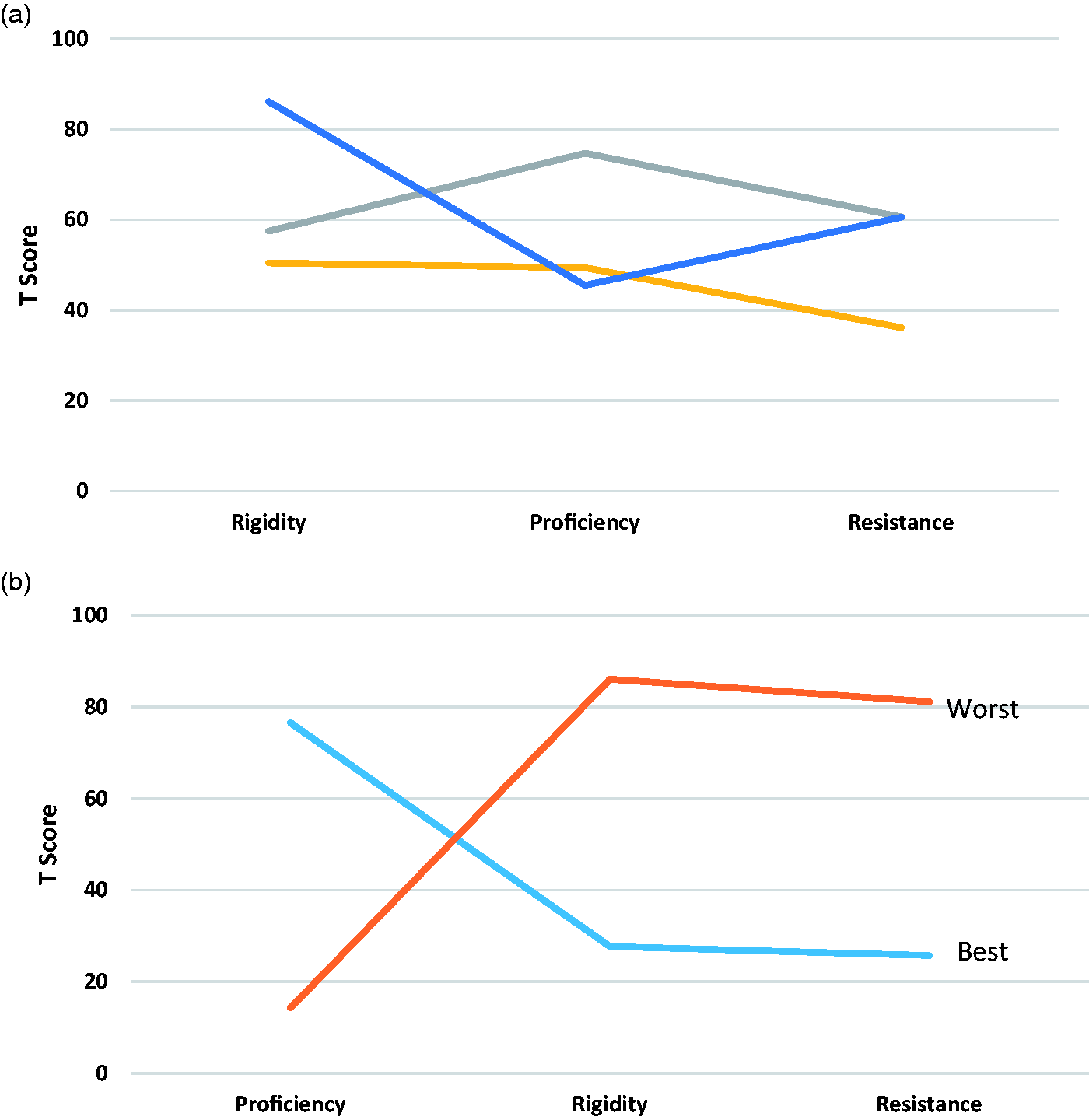
Figures 2a and 2b provide examples of climate profiles in three different divisions. The first-line nurse managers’ profile had scores that were close to the mean on all three climate dimensions (Figure 2a). According to Figure 2b, stress is the predominant factor in climate, but scores as regards engagement and functionality were over 1.5 standard deviations below the stress score. The figures have been picked as one of first-line nursing manager’s group, and results show, that the organizational culture can vary between different parts.
Examples of climate profiles from three divisions (surgical, medical and psychiatric).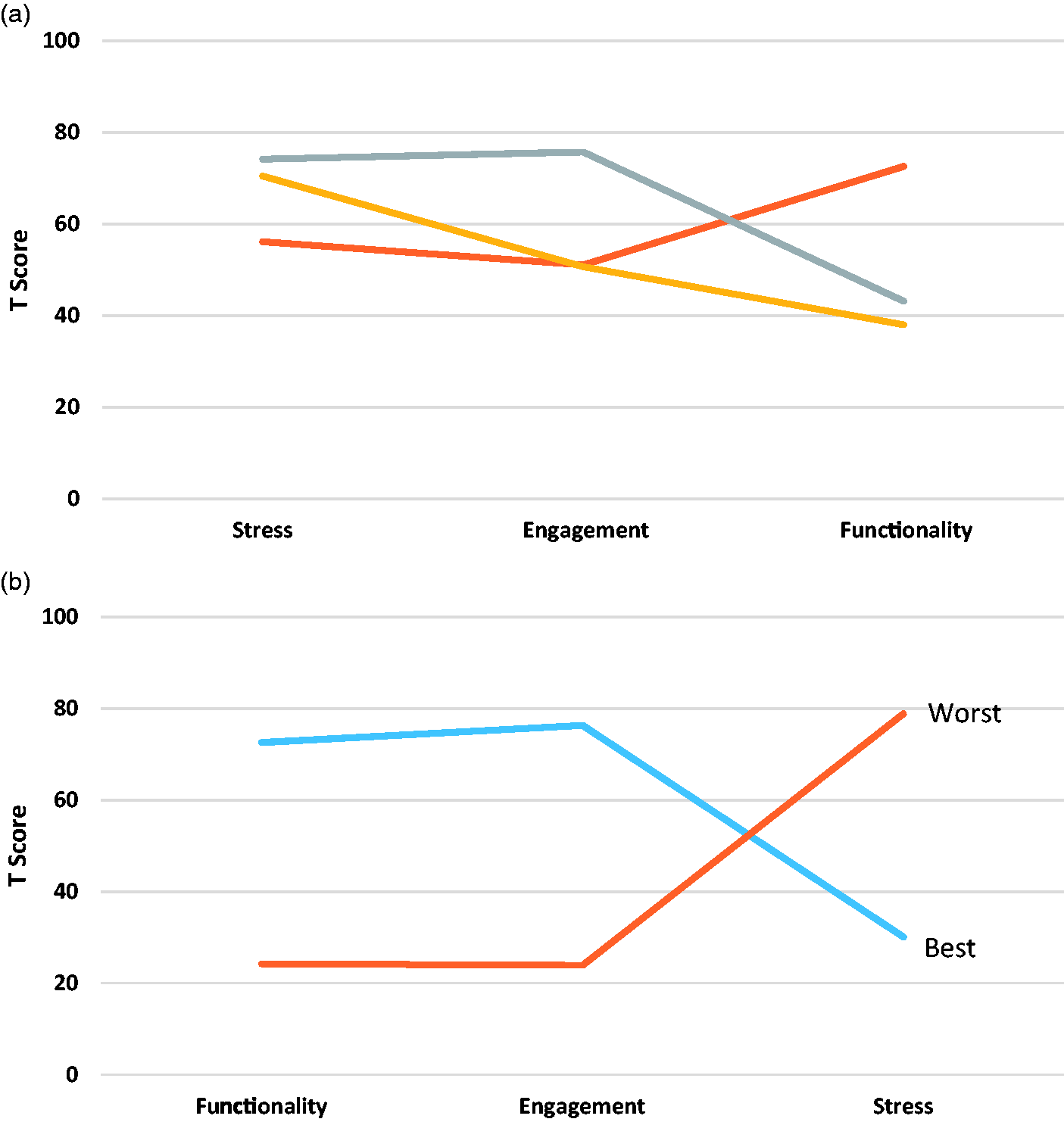
Differences in organizational social contexts and morale among groups and organizations assessed by first-line nursing managers (n = 264). Means, ANOVA-based eta-squared, significance and ICC are indicated.
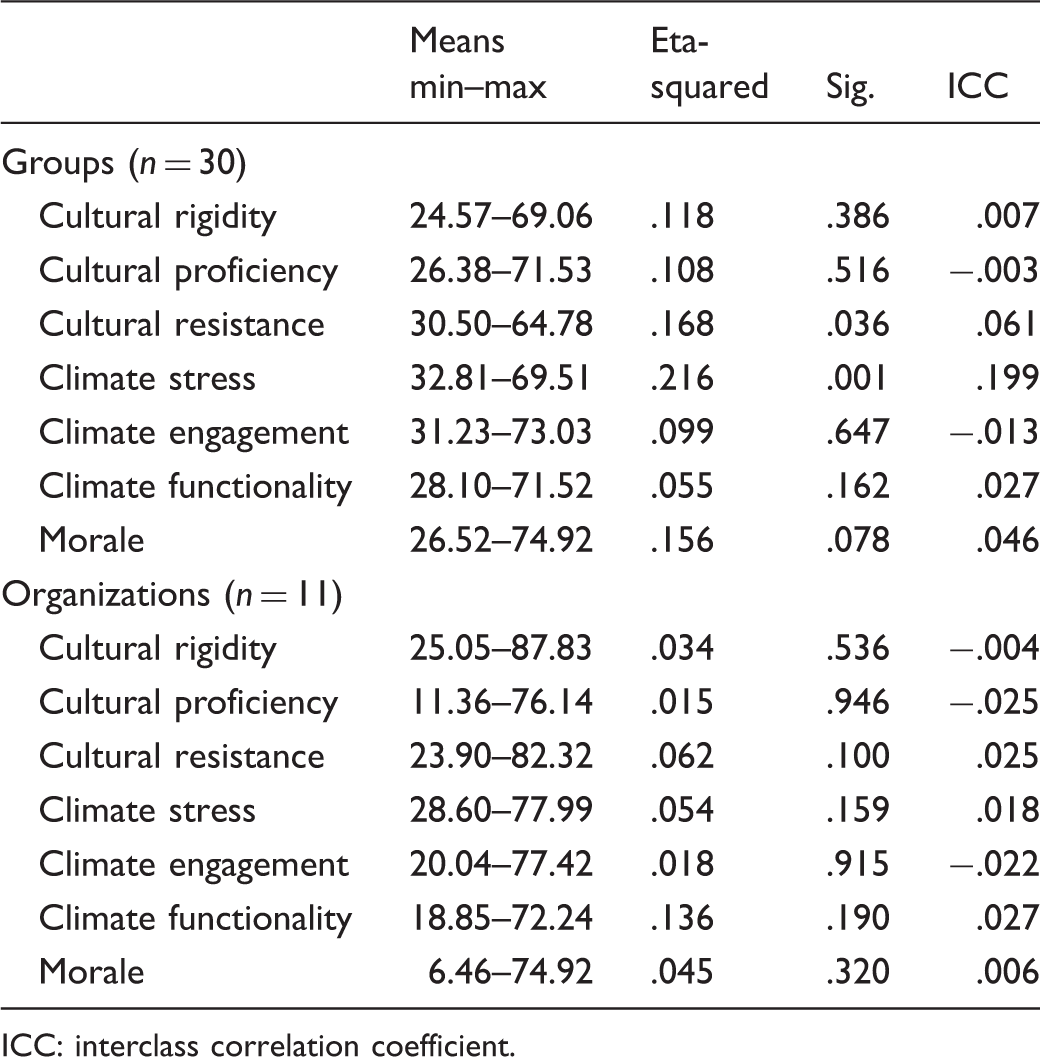
ICC: interclass correlation coefficient.
Differences in organizational social contexts and morale among three different healthcare divisions. Means, ANOVA-based eta-squared, significance of differences (p-value), and ICC.
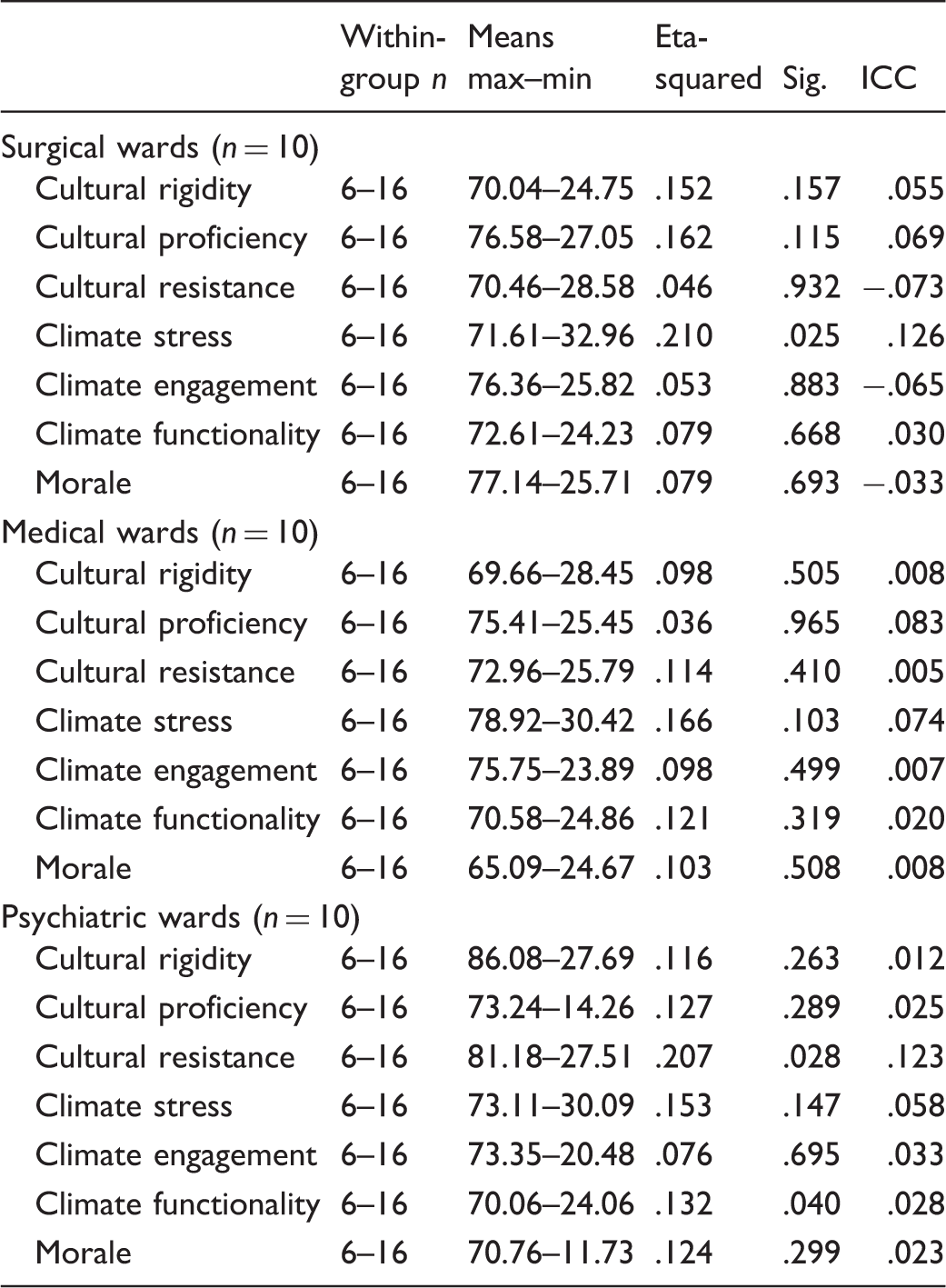
First-line nurse managers in each of the three groups (surgical, medical and psychiatric) showed a remarkable consensus regarding the social context and morale in their divisions. The estimates of within-group reliability (rwg) at the division level were above the critical value of (.70). At the divisional level, the estimates for rigidity and resistance were (.96), and proficiency varied between stress (.97–.98), engagement and functionality (.96–.97) and morale (.96–.97).
Discussion
This study provides a snapshot of the organizational social context in 11 Finnish healthcare organizations, in 30 groups and three divisions as viewed by first-line nurse managers. According to rwg, the organizational social context in the organizations was perceived to be consistent. The organizational social context seems to be associated specifically with differences in the healthcare sector, and not with differences in organizations, groups or divisions as work units.
Based on eta-squared values and ICC analysis, variations between organizations and groups seemed to be more within rather than between the groups.30,40 The extent of negative ICC values both at the organizational and group level differed considerably. Only climate stress and cultural resistance differed significantly at group level. This result is in line with earlier studies by Rostila et al. 37 and Trus et al. 31 However, it was noted that first-line nurse managers were emotionally exhausted, conflicted in their roles and overloaded. If the managers themselves feel the organizational climate is distressing, this will inevitably have a disturbing effect on their staff.29,33 Trus et al. 31 indicate that in a less stressful climate, nurse managers were more structurally empowered.
The results for cultural resistance strengthen this observation, because cultural resistance consists of apathy and the suppression of culture. 20 Maybe the competition between first-line nurse managers regarding both criticism and perceived inflexibility in management also increases the level of climate stress experienced. On the other hand, the results suggest that, especially at the group level, culture requires both active and passive resistance. This affects the organization’s implementation of change, especially if the attitudes and values of the institution begin at the management level. 27 According to an earlier observation,41 first-line nurse managers feel that they cannot achieve a change in the decision-making process and that it is difficult for them to implement change. As such, they risk marginalization if expressing opposition to change, but the prevailing organizational social context perhaps allows it. This result is supported by Trus et al., 31 when working in proficient and resistant cultures, nurse managers had access to opportunities and information, and when the culture was less rigid, they had more access to resources.
It is worth noting that cultural proficiency and climate engagement varied both among managers and at the organizational level. Although not statistically significant, the negative ICC values suggest that there were indeed variations within and between the groups. If we consider that both are positive aspects of the social context, they do not belong to the result of the general healthcare sector. For example, is patient-centeredness the default value in the prevailing culture, or does patient-centeredness mean different things, depending on the group or organization? It has previously been found that nurses learn the culture of the work unit by way of being told what to do,15,43 but can each of the work units allow their own kind of culture? If so, then the application of this result could be expected to affect the patients’ quality of care and the ability of nursing to achieve its goals or other organizational outcomes.7,33,42 According to Weinberg et al., 40 the variation of work environments both by unit and by occupation underlines the important role of the middle manager.
Cultural rigidity varies between organizations. First-line nurse managers considered that decision-making is centralized and regulated, depending on the organization. The result reflects the fact that Finnish healthcare organizations are heavily influenced by the law, but also by the organizations’ rules and instructions. According to Glickman et al., 18 the development of a less centralized, service-line orientation should help support management at the division or ward level. In years to come, hospital structures formed around medical specialties in Finland will transform into more professional organizations. This subsequently requires a review of decision-making processes and management, and the role of cultural rigidity needs to change in this respect. However, the results of this study do not indicate whether cultural rigidity has a negative impact on nurse managers’ management opportunities, or on operation within an organization. A previous Finnish survey 42 has found that organizational rules as perceived by first-line nurse managers did not facilitate their power in the unit.
Examining the results of different divisions showed that statistically significant differences emerge regarding climate stress on surgical wards, and cultural resistance and climate functionality on psychiatric wards. Except for the medical divisions, statistically significant differences were found, but according to ICC calculations there also appeared to be variation within the groups. According to the views of first-line nurse managers in the surgical division, climate stress seems to be consistently observed regardless of group or organization, and in line with the ward-level view that the cultural climate includes emotional exhaustion, work overload and role conflict. It is worth knowing how these issues affect daily operations, the fluency of patient care chains or the job satisfaction of nurse managers or nurses.
In this study, cultural resistance in the psychiatric division was associated with competition and a lack of flexibility, and with avoiding difficulties and challenges. The results indicate that the individuals in this division are assumed to be both dominant and assertive. Professional growth and career progress, as well as the clarity of roles and collaboration, are key features of the climate’s functionality as revealed by this study. The reason these features are emphasized in the psychiatric division may be explained by its representative social interactions and social structures. 43
Overall, first-line nurse managers seem to have a collective understanding and interpretation of the organizational social context. The results revealed that there are differences in various divisions, regardless of the organization or group. Although nursing work is carried out following basically similar policies and functional environments, it is shaped around medical specialties (surgical, medical and psychiatric) and their own organizational social contexts. If these specializations cannot define their own operations, the lack of definition is likely to affect employees’ job satisfaction, their commitment to the organization and common goals, or even to impair the flow of care chains and patient safety. From the perspective of nursing and nursing management, different social contexts could also impact on working conditions, for example through the influence of power. Healthcare is changing rapidly and is recorded on both global and national scales, as opposed to culture which is slowly changing. The new types of operations and innovations that are part of the occurrence are also going to require changes in the social context. Nursing managers have their own role to play in this process. The social context offers new ways of organizing work in hospitals. 31
Conclusion
If an organization is to maintain or promote a certain organizational social context, it is necessary to identify the different issues and contexts involved, and to discuss what kind of image they want to convey regarding their organization and performance. Considering organizational culture, and the connection between climate and morale, many things can be changed to improve the efficiency and effectiveness of the organization, division or unit. Attention should be paid to why differences are found in and between different divisions, and how these might affect patient care and patient flows. In the implementation of change in healthcare, it is vital to recognize what barriers social context highlights, and how these can be dismantled or reduced.
Footnotes
Funding
Competitive Research Funding of the Central Finland Health Care District (B12202) and Pirkanmaa Hospital District (9L099), (9N074), (R9048). The Finnish Doctoral Program in Nursing Sciences and Finnish Foundation for Nurse Education have provided financial support for this study.
Conflict of interest
The authors declare that there is no conflict of interest.