
Abstract
The positive relationship between socioeconomic status (SES) and health is well established in Western societies. However, while research mainly focuses on SES measures such as education and income, these measures may not completely capture the characteristics of social stratification in China. In the socio-historical context of China, for example, the work unit sector is a crucial SES factor. Yet, few health studies have paid attention to unique SES factors in China. Furthermore, women generally report worse mental health than men, but it is unclear whether this gender gap could be influenced by SES. In this article, using data from the China Health and Retirement Longitudinal Study, we (1) expand SES measures to explore the impact of the work unit sector and use other SES measures, including Communist Party of China (CPC) membership and hukou (household registration) status, to examine the relationship between SES and depression and (2) investigate whether SES could modify the relationship between gender and depression. We find that all the SES measures negatively predict the depression symptoms of elderly individuals. We also find that women on average report higher depressive symptom scores than men. However, the gender differences in depressive symptom scores are smaller among elderly individuals with higher SES than among those with lower SES. We demonstrate that the work unit sector and CPC membership are crucial SES factors affecting the mental health of elderly Chinese individuals. Moreover, we show that the gender gap in depression could vary by SES, suggesting that women might benefit more from obtaining higher SES.
Introduction
China is home to more than 280 million elderly individuals, and this senior segment of the population is growing faster in China than anywhere else in the world (Ministry of Civil Affairs of the People's Republic of China and China National Committee on Ageing, 2023). As a consequence of the aging population worldwide, the study of depression among elderly individuals is also growing (Lu et al., 2021; Ren et al., 2020), as aging is associated with poor health, poor functioning, chronic medical conditions, and other diseases that affect not only individuals but society as a whole (Chen et al., 2022; Schramm et al., 2020). In China, the prevalence of depressive symptoms among older Chinese individuals was approximately 20% in 2011–2019 (Tang et al., 2021), increasing to 29.4% in 2020 (Ge et al., 2023).
Extensive studies highlight the importance of socioeconomic status (SES) for mental health, including depression, showing that mental health could be mitigated by higher SES (Clouston and Link, 2021; Link and Phelan, 1995; Phelan et al., 2010). In Western societies, however, research mainly focuses on education and income as the major SES measures and finds that both education and income are positively associated with mental health (Frech and Damaske, 2019; Hinata et al., 2021; Pei et al., 2020; Ross and Mirowsky, 2006; Ye et al., 2023). In addition, other research demonstrates that individuals with well-off family backgrounds (Luo and Waite, 2005; Schaan, 2014) or with more prestigious jobs (Lopes et al., 2019) are more likely to have lower levels of depression than those with poor family backgrounds or less prestigious jobs.
In the unique sociopolitical context of China, the work unit sector is a crucial SES characteristic. Prior to economic reform in China, the sector of one's work unit (danwei) defined the life-long “membership” to a type of employment and assured a standard of well-being for workers and their families (Naughton, 2015; Walder, 1986). Society followed a hierarchical structure in which the work unit sector determined how wealth was distributed (Wu, 2014). Economic returns, including income, goods, and services, were increased as an individual climbed the rungs of the sector's hierarchical ladder (Walder, 1992; Wu, 2014; Xie and Wu, 2008). Individuals working in the state sector were given priority access to resources, such as educational opportunities for their children and better medical care (Walder, 1992). Only a few studies have examined how work unit sector might influence health (see exceptions: Li and Zimmer, 2013; Nishimura, 2011), but none of the studies have concentrated on depression among elderly individuals in China.
Gender is a social and structural variable that results in inequities across many domains, including health (Ridgeway and Correll, 2004). Women generally report worse health than men but live longer than men (Denton et al., 2004; Read and Gorman, 2010; Stanley and Denney, 2023). Previous research examining the relationships among SES, gender, and health has reported mixed findings. Some studies report that the gender disparity in health decreases as the level of education increases (Ross and Mirowsky, 2006, 2010), while other studies find that the gender disparity in health is not affected by SES (Zajacova and Lawrence, 2018). In China, one study reports that the gender gap in depression among the elderly population decreases for migrants who relocate from rural to urban areas at an early age (Zhang et al., 2022). However, other studies find that education (Li et al., 2022) and childhood neighborhood quality (Chen et al., 2020b) do not influence the gender disparity in health. Thus, it is still unclear whether gender differences in depression vary by SES.
Using the China Health and Retirement Longitudinal Study (CHARLS), we examine the relationships between SES and depression and gender and depression, and the modifying effect of SES in the relationship between gender and depression among elderly Chinese individuals aged 60 and older. Specifically, our investigation encompasses various indicators that describe individuals’ unique social status in China, including the work unit sector, Communist Party of China (CPC) membership, and hukou (household registration) status, as well as personal education, parental education, and childhood financial conditions. Furthermore, we examine interactions between gender and these SES indicators to determine the role of SES in the relationship between gender and depression.
Background
SES and depression
According to fundamental cause theory (Link and Phelan, 1995; Williams, 1990), SES is perceived as the “fundamental cause” of health problems. Firstly, SES influences multiple disease outcomes through multiple risk factors, such as poor diet, cholesterol, lack of exercise, and high blood pressure. Secondly, SES conveys the ability to access flexible resources. Flexible resources such as knowledge, money, power, prestige, and beneficial social connections can all be used to maintain health and prevent the consequences of risk factors. Thirdly, individuals with higher SES are more likely to have healthy lifestyles, live in safe neighborhoods, and have access to effective medical treatments (Phelan et al., 2010). However, individuals with lower SES are more likely to be exposed to risk factors and receive inadequate treatment (Freese and Kevern, 2013). Thus, we propose that elderly individuals with higher SES are more likely to have fewer depressive symptoms.
Human capital theory proposed by Mirowsky and Ross (1998) is also helpful for understanding how SES might influence depression. According to this theory, education improves health by increasing an individual's human capital, such as cognitive skills and the ability to manage and guide his or her life. Individuals’ health can benefit from the effective agency gained through education. Education helps individuals to develop personal learning habits, health behaviors, and positive values and attitudes; these, in turn, enhance individuals’ control over their lives and encourage a healthy lifestyle (Ross and Wu, 1995). Thus, we propose that education could help elderly individuals achieve better mental health. Elderly individuals with higher levels of education may have fewer depressive symptoms than those with lower levels of education.
An individual's early experiences are associated with both advantages and disadvantages in later life. Previous research has proposed different mechanisms by which such cumulative effects operate on outcomes in later life (Ben-Shlomo et al., 2014). Cumulative effects, in particular, suggest that the health condition of older adults is not only solely attributable to current risk factors, such as drinking and smoking, but is also a life-long process that begins in early childhood (Dannefer, 2003). Early-life experiences are connected to individuals’ health outcomes in old age. This process is characterized by the gradual accumulation of social influences that originate in early childhood (e.g., childhood disadvantage, working experiences, hukou status, education), resulting in advantages or disadvantages over the life course (Seabrook and Avison, 2012). Early-life advantages and disadvantages may accumulate over time and result in better or worse health in later life.
Many empirical studies have documented the negative association between depression and SES factors, including education (Bauldry, 2015; Niemeyer et al., 2019), income (Frech and Damaske, 2019; Muramatsu, 2003), social origin (Luo and Waite, 2005; Schaan, 2014), and occupation (Christ et al., 2012; Lopes et al., 2019). Using a German representative sample, Niemeyer et al. (2019) found that the gradient along education level also exists in depression. Based on the National Longitudinal Survey of Youth 1979, another study showed that the physical and mental well-being of men at the age of 50 was closely tied to their income trajectories (Frech and Damaske, 2019). Luo and Waite (2005) used the 1998 wave of the University of Michigan Health and Retirement Study to investigate the relationship between social origin and depression, and found that higher childhood SES was related to fewer depressive symptoms in later life. Moreover, Lopes et al. (2019) examined the relationship between SES and depression among workers using the United Kingdom's Psychiatric Morbidity among Adults Living in Private Households Survey and found that SES was significantly associated with workers’ depressive symptoms, especially the factors of job rank, gross household income, social class, gross personal income, and socioeconomic group.
SES and depression in China
It is essential to embed the association between SES and depression in historical and sociopolitical contexts. The work unit sector, CPC membership, and hukou status are all crucial factors in SES for elderly Chinese individuals. In pre-reform China (before 1978), work units played an all-encompassing role and served as a well-being provider for urban citizens. “Membership” in a work unit was effectively permanent and conveyed lifetime employment (Naughton, 2015; Walder, 1986). The economic returns of workers in a given work unit, including both salaries and in-kind goods and services, were dependent on its sector, particularly the ownership and position of that sector in the redistributive hierarchy (Walder, 1992; Wu, 2014; Xie and Wu, 2008). The closer an individual's work unit sector was to the central planning agency, either of the CPC or government, the higher was the priority of the individuals in that work unit in obtaining resources (Walder, 1992). The priority ranking of sector was typically as follows: (1) the state sector (government, public institutions, and state enterprises); (2) the collective sector (collective institutions and enterprises); (3) the private sector (private enterprises, foreign firms, excluding self-employed).
In the post-reform (after 1978) period, the work unit sector remains a crucial factor for constituting SES in Chinese society (Lin and Bian, 1991), but existing research has paid insufficient attention to the association between the work unit sector and health (see exceptions: Li and Zimmer, 2013; Nishimura, 2011). Using large-scale longitudinal data covering 1989–2006, Li and Zimmer (2013) noted that when parents work in the state sector their children show a lower likelihood of being obese. Based on the Family Survey of China 2006, Nishimura (2011) examined the relationship between work unit sector and depression among Chinese individuals aged 60 and younger. This study found that men working in the state sector experienced lower levels of depression than those working in the private sector or self-employment. In this study, we aim to fill a gap in the literature by examining the relationship between the work unit sector and depression among elderly individuals.
CPC membership confers privileged access to better goods and resources and is also the main means of upward career mobility (Dickson and Rublee, 2000; Walder, 1986). CPC members are advantaged in business and have higher incomes because they are able to obtain well-compensated positions within state-owned enterprises or CPC/government agencies (Li et al., 2007). Most previous studies neglected the role of CPC membership in health. Only a few studies have mentioned that CPC membership might significantly influence the health of individuals. Using cross-sectional data from CHARLS, Li et al. (2021) found that CPC membership is negatively associated with depression among the elderly population. Gong et al. (2016) found that CPC members had better quality physical examinations and inpatient care due to their ability to access medical facilities and health insurance. Yip et al. (2007) noted that CPC membership among rural residents also related to better self-reported health based on a sample of Shandong citizens. In this study, we intend to use longitudinal data to investigate the role of CPC membership in depression among elderly Chinese individuals.
The hukou system is a basic feature of social stratification in China and determines the allocation of resources and life opportunities from birth (Wu and Treiman, 2004, 2007). Individuals with rural hukou status have had limited access to the rights and privileges that the state grants to urban hukou registrants, including educational opportunities, healthcare coverage, retirement benefits, and stable employment (Wang, 2004). Some studies find that individuals with rural hukou status report worse health (Zimmer and Kwong, 2004; Zimmer et al., 2010) and higher levels of depression (Chen et al., 2020a; Li and Zhao, 2021; Li et al., 2016) than those with urban hukou status. Using CHARLS, Guo et al. (2017) identified a gradient in depressive symptom scores among villagers (rural residents with rural hukou status), temporary migrants (urban residents with rural hukou status), permanent migrants (individuals with rural-to-urban converted hukou status), and urban residents with urban hukou status. Based on the CHARLS 2015 and 2014 surveys, Song and Smith (2021) examined the relationship between urban hukou attainment and migrants’ psychological well-being in middle and later life and showed that attaining urban hukou was positively associated with psychological well-being.
Studies using data from China suggest that individuals’ health improves with higher education and income (Behrman et al., 2015; Cai et al., 2017, 2022; Zhou et al., 2018; Zimmer and Kwong, 2004). Ross and Zhang (2008) used national data from the Chinese Longitudinal Healthy Longevity Survey to examine the association between education and psychological distress. They found that older Chinese individuals with higher levels of education experienced lower levels of distress than their less-educated counterparts. Ye et al. (2023) found that higher income causally benefits mental health, based on a study of Chinese twins. Our study contributes to the existing body of literature on SES and depression by expanding SES measures to include the work unit sector, CPC membership, and hukou status as important indicators of SES in China.
Gender and depression
In general, women live longer but experience more health problems than men over the life course (Link et al., 1998; McDonough et al., 1999). The explanation for these gender differences is often addressed in exposure and vulnerability disparities between men and women (Bird and Rieker, 2008; Denton et al., 2004; Read and Gorman, 2010). Specifically, men and women experience varying degrees of exposure to factors that promote poor health and respond differently to their health conditions. For example, women tend to experience more depression after the birth of children relative to men (Shi and Shen, 2023). Simon and Nath (2004) proposed that gender differences in mental health were caused by the different experiences of specific emotions. They argued that women experienced more negative feelings and fewer positive feelings compared to men, since women generally lived in disadvantaged social conditions compared to men.
The status composition perspective suggests that the gender disparity in depression depends on the social roles and positions of women and men at different stages of their lives (Clarke et al., 2011). Women and men enter into and experience their unequal social statuses in family, employment, and economic well-being (Mirowsky, 1996). Women live in more stressful circumstances than men due to their dual responsibilities in the family and at work (Lennon and Rosenfield, 1992; Rosenfield, 1989). It is common for women to find themselves in dire circumstances due to the conflicts in balancing family and work responsibilities. Moreover, this gender gap in depression may vary across ages (Bracke et al., 2020; Platt et al., 2020). For example, Clarke et al. (2011) found that the majority of the gender gap in later life results from differences in social positions and the advantages of roles accumulated throughout an individual's life.
SES, gender, and depression: The modifying effect of SES between gender and depression
The gender differences in depression could be modified by SES differences between men and women. Women generally report lower SES than men (Short and Zacher, 2022), are less likely to occupy positions of power in the majority of occupational categories (Hartmann and Rose, 2004), and accumulate less wealth than men (Ruel and Hauser, 2013). Thus, women may be more likely to be depressed than men due to their limited access to resources that help prevent and treat depression (Link and Phelan, 1995). In this article, we ask whether gender differences in depression could vary at different levels of SES.
Ross and Mirowsky (2006) proposed two competing theories to address this question. Resource substitution theory proposes that, for women, higher levels of education may result in greater improvements in well-being relative to men, because women are disadvantaged in other SES dimensions and depend more on education to achieve better well-being. Resource multiplication theory proposes that education will improve well-being more for men by giving them advantages in the labor market, especially positions of authority and higher earnings. Men who are well educated will have more success in securing good jobs. Previous studies found mixed empirical evidence to support the two competing theories. Based on a 1995 survey of US adults with follow-ups in 1998 and 2001, research found that both depression (Ross and Mirowsky, 2006) and physical impairment (Ross and Mirowsky, 2010) decreased more for women than for men as the level of education increased. In contrast, other studies found that the educational gradient of mortality was steeper for men than for women (Bassuk et al., 2002; Montez et al., 2009), while other studies reported that SES had no influence on gender differences in health (Zajacova and Lawrence, 2018).
In China, the gender disparity in depression has been documented (Lu et al., 2021; Qiu et al., 2020). Research has found that women generally report more depressive symptoms than men (e.g., Chen et al., 2023; Lei et al., 2014; Williams et al., 2017). Only a few studies have examined the role of SES in the association between gender and depression. However, their measures of SES are limited, and findings are mixed. Using the life history data from CHARLS, Zhang et al. (2022) found that the gender disparity in depression was lower for elderly individuals who moved from rural to urban areas at early ages than those who stayed in rural areas, whereas Li et al. (2022) found that education did not affect the relationship between gender and depression based on CHARLS 2018. Similarly, Chen et al. (2020b) reported that childhood neighborhood quality had no influence on gender disparity in depression. Thus, the role of SES in gender differences in depression among elderly Chinese individuals remains uncertain.
Current study
In this study, we ask two questions: (1) Do important Chinese SES factors, such as the work unit sector, influence depression among elderly individuals? (2) Do gender differences in depression vary across different levels of SES? Embedded in the unique socio-historical context of China, we use multiple measures of SES, including the work unit sector, CPC membership, and hukou status, as well as personal education, parental education, and childhood financial conditions, to more thoroughly describe the social positions of the elderly Chinse individuals. Furthermore, we apply interactions between SES and gender to examine the role of SES in the relationship between gender and depression.
Data and methods
Data
This study uses data from CHARLS, a nationally representative sample of Chinese residents aged 45 and older. The survey has been conducted by the China Center for Economic Research at Peking University every two years since 2011. The baseline national wave of CHARLS included about 10,000 households and 17,500 individuals in 150 counties/districts and 450 villages/residents’ committees, covering demographics, family structure, health, retirement and pension, income and consumption, and other important information (Zhao et al., 2020). In 2014, the survey institution conducted a life history survey, which included all respondents from the first two waves who were still alive, and provided specific information about demographic backgrounds, working histories, and other time-varying factors.
To investigate the relationships among SES, gender, and depression in elderly Chinese individuals, we use data from four waves and the life history survey of CHARLS and restricted our sample to adults aged 60 years and older who had completed the questions describing depressive symptoms and had no missing data on the SES measures. Based on these restrictions, a total of 9185–11,792 individuals were selected, depending on the missing data for specific SES measures. We imputed control variables, but not the dependent variable or the SES measures, and constructed variables using data from the harmonized CHARLS data (https://charls.charlsdata.com/pages/Data/harmonized_charls/zh-cn.html).
Measures
Depression. The 10-item Center for Epidemiological Studies Depression Scale (CES-D-10) scores are used to measure the depressive symptom scores. CES-D-10 is the simplified version of CES-D-20 and is a 10-question self-reported scale measuring depressive symptomatology. CES-D, developed by Radloff (2016), is widely used to assess depression among elderly Chinese individuals and demonstrates adequate reliability and validity (Pei et al., 2020; Xu et al., 2020; Zhang et al., 2022; Zhou et al., 2021). In line with the methods used in previous studies, we reverse the coding of the two positive-emotion items (“I felt hopeful about the future” and “I was happy”) to be consistent with the order of other items reflecting the respondent's degree of depression; each item was given a value of 0–3. Thus, each respondent's overall CES-D-10 score ranges from 0 to 30, with a higher score indicating a higher level of depression (Bi et al., 2021; Chen et al., 2020b; Zhao et al., 2014).
SES. SES is measured by the following variables: the work unit sector, CPC membership, hukou status, education, parental education, and childhood financial conditions. The work unit sector is determined on the basis of in which sector the respondent had longest working experience, as reported in the data. Based on previous studies (Lin and Bian, 1991; Wu, 2014), we categorize work unit sectors as the state sector, the collective sector, or the private sector. The state sector consists of government and public institutions. The collective sector, formed in the 1950s, was widespread during the 1960s and 1970s and consists of rural collective economic organizations and collective firms, which are controlled by collectives under the jurisdiction of city, district, and township governments. The private sector consists of any other firms, such as private or family enterprises, publicly listed companies, and firms with investments from places outside of China.
For CPC membership, respondents are coded as “1” if they are CPC members and “0” otherwise. Hukou records the current hukou status of respondents. The primary hukou system only records two kinds of status: rural (“0”) and urban (“1”). However, in recent decades, the hukou system in China has been undergoing a unified reformation. The government has generated a unified hukou for both rural and urban hukou registrants and tried to eliminate differences between the two. In this sample, we excluded the respondents who reported unified residence hukou in all four waves of the longitudinal study. If respondents reported either rural or urban hukou status in one wave and unified residence hukou status in another wave, we used the rural or urban hukou status.
Education indicates the highest level of education obtained by the respondent. Parental education indicates the highest level of education attained by the parent, with the higher level of education between both parents. Given the low level of education among older cohorts, education and parental education are categorized as follows: illiterate, primary (including those who had finished primary school or sishu, and those without primary school diplomas but who can read and write), and middle and above (including those who had obtained middle school and higher diplomas).
Childhood disadvantage influences mental health in later life (Ferraro et al., 2016). We select childhood financial condition to describe the social conditions of individuals at early ages, which is determined on the basis of the respondent's perceived family financial condition before age 17 compared to that of other families in the same community/village. Following a previous study (Kendig et al., 2017), we categorize childhood financial conditions as follows: below average, average, and above average. In the harmonized CHARLS data, income is measured on the basis of multiple dimensions, such as earned income, pension income, financial assets income, and government/public transfers income. Among these, financial assets income and government transfers income are influenced by the efforts of other household members. Thus, household income is a better choice to measure SES than individual income. However, the household income variable was missing for 23.3% of observations. Thus, instead of individual income and household income, we use childhood financial condition as the measure of income based on a question asked in the CHARLS life history survey conducted in 2014: “When you were a child before age 17, compared to the average family in the same community/village at that time, how was your family's financial situation?”
Covariates
In our analysis, the control variables are respondent's age, gender, residential area and region, marital status, retirement status, perceived health, and household per capita expenditure. In addition, we also include variables describing whether respondents were covered by public health insurance and public pension, whether they participated in one or more social activities in the previous month, the number of living parents, whether they co-reside with any child, whether they live near any child (in the same city or county), and whether they have weekly contact with any child. Table 1 shows the descriptive statistics and the definitions of all variables used in this study.
Descriptive statistics for variables in analysis.
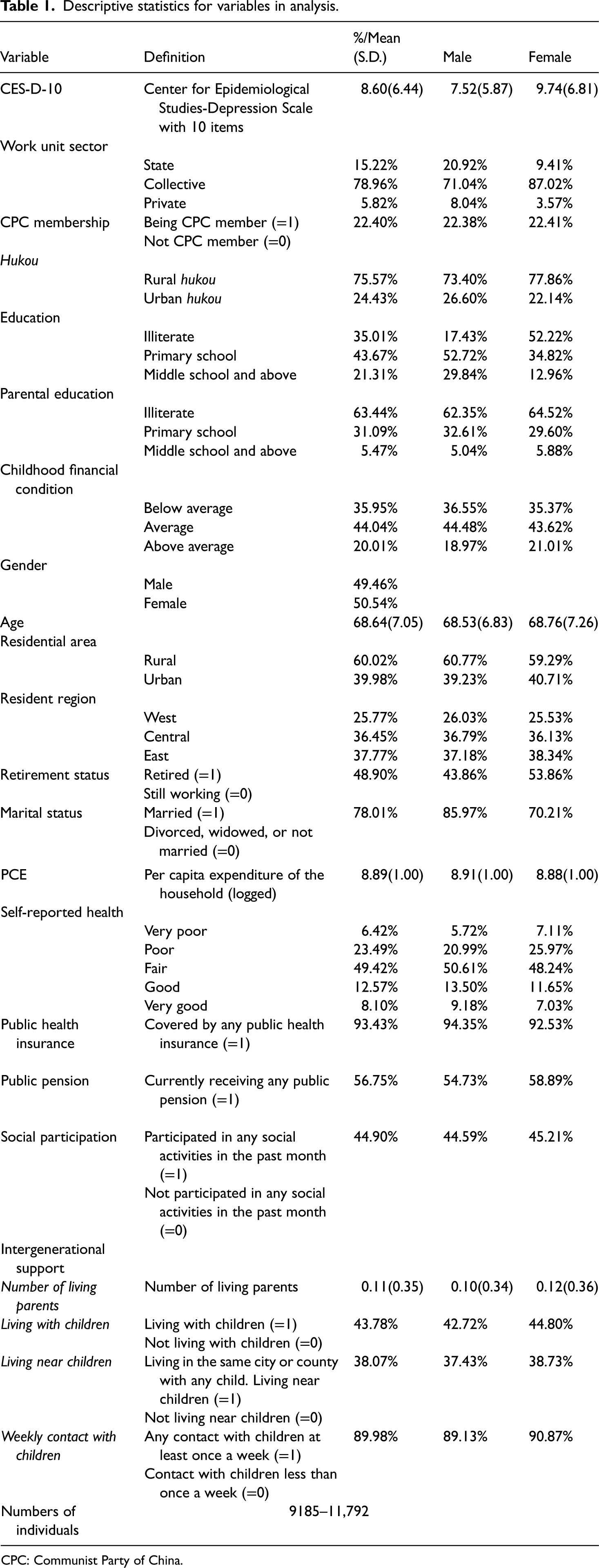
CPC: Communist Party of China.
Analytical strategy
To assess the relationship between SES and depression among older Chinese individuals, we first constructed random effects models to estimate the variation in depressive symptom scores across various SES predictors, including the work unit sector, CPC membership, hukou status, education, parental education, and childhood financial conditions. These multilevel models nest observations across various survey waves within individual respondents. The random effects in models account for the correlation of residuals across different waves within individuals and indicate between-individual variance in intercepts.
We further interact all the SES indicators (one by one) with gender to explore whether the depression gap between men and women is influenced by SES. Interaction terms for SES and gender reveal whether the depressive symptom correlates of the work unit sector, CPC membership, hukou status, education, parental education, and childhood financial condition varied for males and females. The equations are as follows:

Results
Descriptive results
The descriptive statistics for our sample are displayed in Table 1. Firstly, the individuals in our sample report a mean depressive symptom score of 8.60. All respondents in our analysis are aged 60 and older. Most of the respondents have their longest work experience in the collective sector (78.96%), some of them have the longest work experience in the state sector (15.22%), and a small portion of the respondents reported that they worked mostly in the private sector (5.82%). In our analytical sample, 22.4% of respondents were members of the CPC, while about 77.6% were not. Similarly, the majority in the sample reported rural hukou status (75.57%), while 24.43% of the sample reported urban hukou status. Regarding education, the largest proportion of respondents had a primary school education (43.67%), followed by illiterate individuals (35.01%). The smallest group was composed of individuals with a middle school education and above (21.31%). In terms of parental education, more than half of parents were illiterate (63.44%), while less than 10% of the sample had parents with a middle school education or above (5.47%). Regarding childhood financial conditions, nearly half (44.04%) of the sample reported that their household income was similar to other families in the same area.
Women on average reported higher depressive symptom scores than men (women: 9.74, men: 7.53). The percentage of individuals working in state sectors was higher among men than women (women: 9.41%, men: 20.92%), while women had a slightly higher proportion of CPC members than men (women: 22.41%, men: 22.38%). In addition, the percentage of respondents with urban hukou status was 5.38 percentage points higher among men than women. More than half of women respondents were illiterate (52.22%), compared to 17.43% for men; men generally reported a higher level of education than women. The percentage of men with a middle school education or higher was 16.88 percentage points higher than that of women and 17.9 percentage points higher in the primary education category. However, for parental education, the percentage of men with parents with a middle school education and above was slightly lower, by 0.44 percentage points, than that of women, and for men with a primary school education, it was 3.01 percentage points higher. For the variable childhood financial condition, women generally reported better childhood financial conditions than men. Specifically, the percentage of women from a high-income family was 2.04 percentage points higher than that of men.
In the analytical sample, the average age was about 68. About 60% were living in rural areas. Close to half of the respondents had retired from work (48.9%). The majority were married (78.01%). Most of the respondents considered their health to be fair (49.42%). The percentage of elderly individuals who consider their health better than fair (20.67%) was lower than those who consider their health to be worse than fair (29.91%). Since participation in public insurance is compulsory for Chinese citizens, nearly all of the elderly individuals were covered by public health insurance (93.43%). Furthermore, many elderly individuals lived with children (43.78%) and near children (38.07%). Moreover, 89.98% of respondents reported that they regularly contacted their children at least once a week. A large proportion of respondents participated in social activities every month (44.9%). In our sample, 37.77% were from the eastern region of China, 36.45% were from the central region, and 25.77% were from the western region (based on the administrative divisions established by the Chinese government).
Influence of SES on depression
Table 2 shows the predictors of different indicators of SES on depressive symptom scores, with standard errors that have been adjusted for clustering effects within individuals in parentheses. In Model 1, individuals who were self-employed or had never worked are excluded, as suggested by previous research (Wu, 2014). We find negative associations between SES and depression among Chinese elderly individuals. Model 1 shows that the elderly individuals who worked in the state sector on average reported lower depressive symptom scores than those who worked in the collective sector (b = –1.309, p < 0.001). In contrast, those who worked in the collective sector did not show significant differences in depression compared to those who worked in the private sector. Model 2 shows that older people who were CPC members reported lower depressive symptom scores than those who were not (b = –0.895, p < 0.001). Model 3 shows that urban hukou status significantly predicted lower depressive symptom scores when compared to rural hukou status (b = –1.365, p < 0.001). Model 4 shows that the elderly individuals with a primary school education reported lower depressive symptom scores than those who were illiterate (b = –0.331, p < 0.001). Elderly Chinese individuals with a middle school and higher level of education reported lower depressive symptom scores than those who were illiterate (b = –1.353, p < 0.001). Model 5 shows that the elderly individuals with primary-school-educated parents also reported fewer depressive symptoms than those with illiterate parents (b = –0.468, p < 0.001). When parents had a middle school education and above, respondents were less likely to be depressed than those whose parents were illiterate or had a primary school education (b = –0.532, p < 0.01). Model 6 shows that the elderly individuals with average childhood financial conditions had lower depressive symptom scores than those with below average childhood financial conditions (b = –0.873, p < 0.001), and individuals with above average childhood financial conditions also had lower depressive symptom scores than those with below average childhood financial conditions (b = –0.738, p < 0.001). Elderly individuals with average childhood financial conditions reported the lowest depressive symptom scores, while women reported higher depressive symptom scores than men in all models.
Predicting depression by SES and gender.
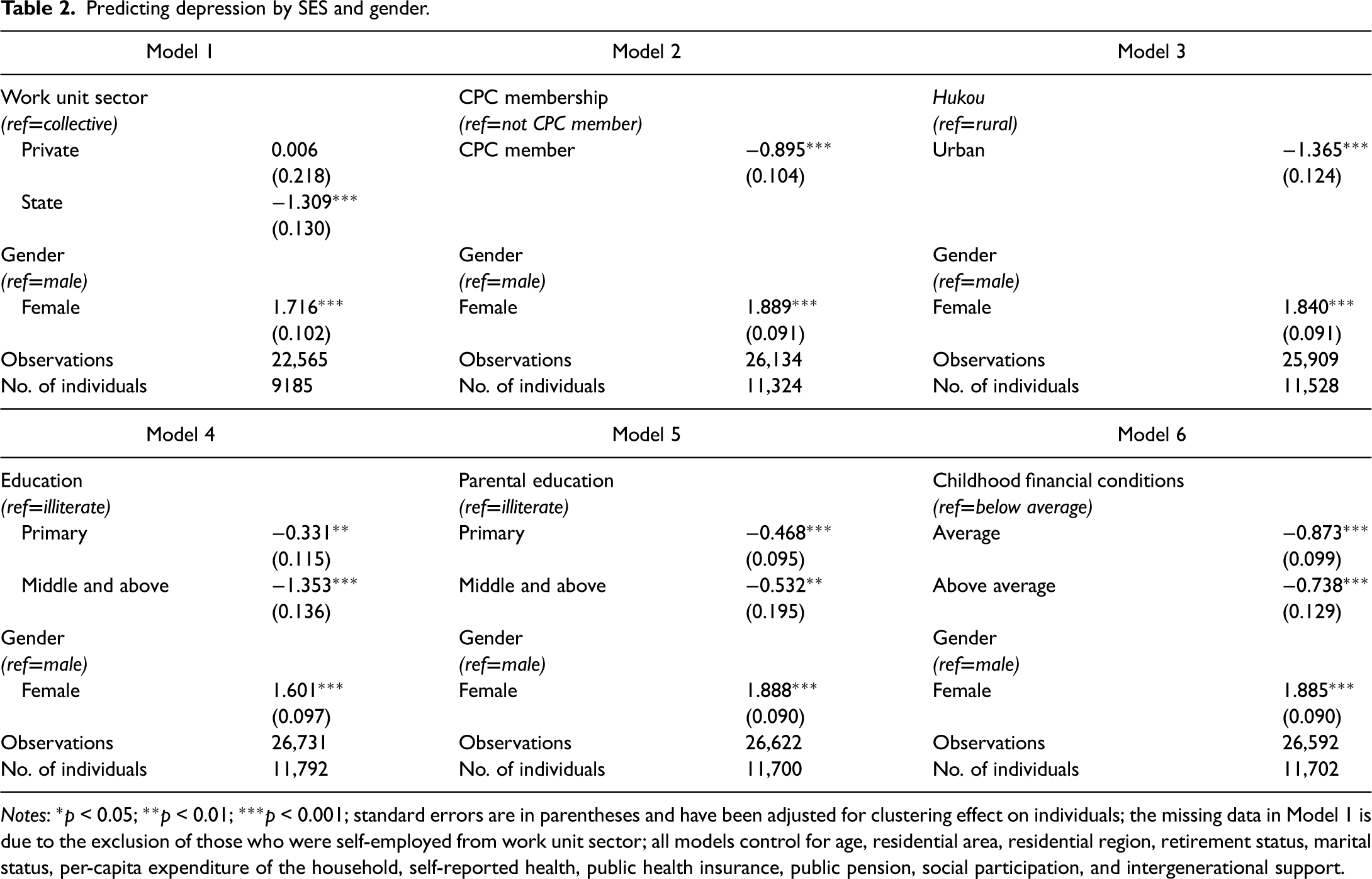
Notes: *p < 0.05; **p < 0.01; ***p < 0.001; standard errors are in parentheses and have been adjusted for clustering effect on individuals; the missing data in Model 1 is due to the exclusion of those who were self-employed from work unit sector; all models control for age, residential area, residential region, retirement status, marital status, per-capita expenditure of the household, self-reported health, public health insurance, public pension, social participation, and intergenerational support.
Interactive influence of SES and gender on depression
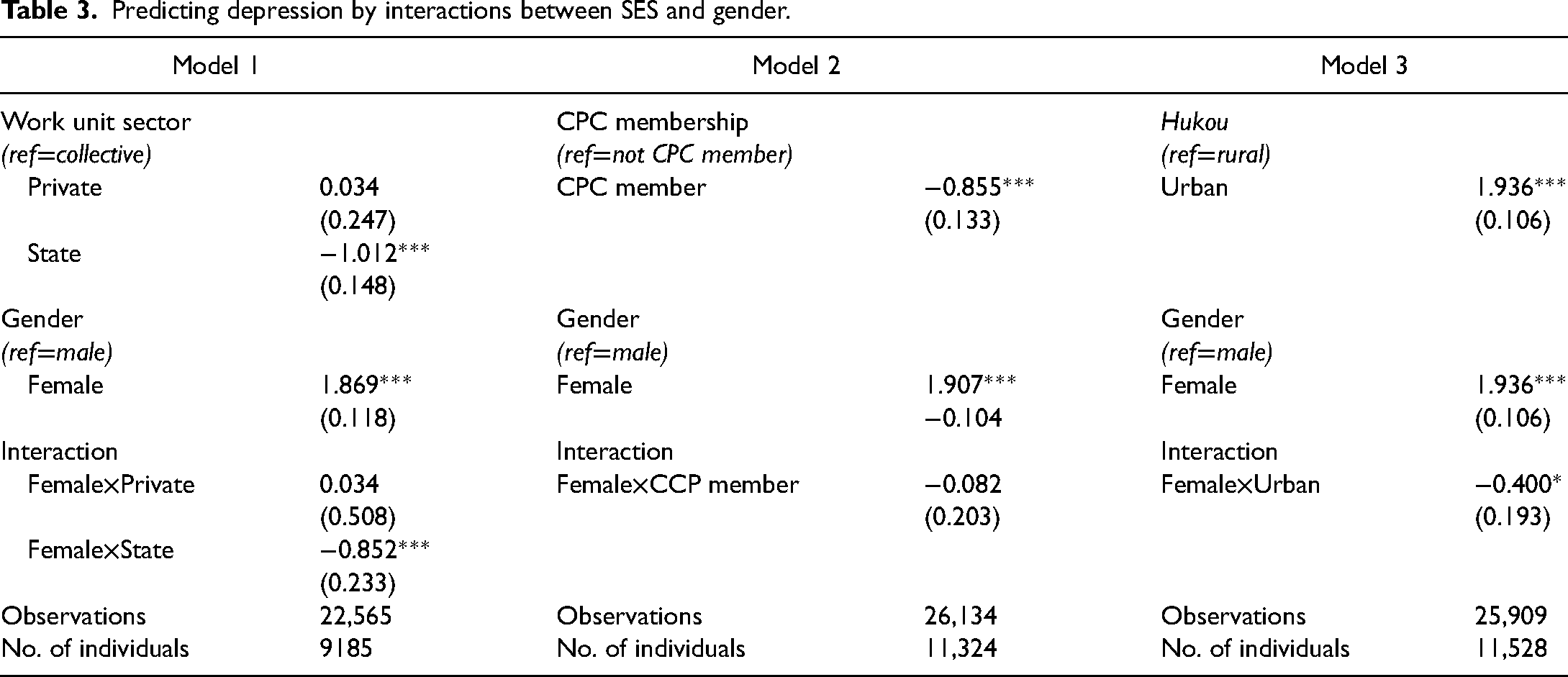
Table 3 summarizes the result of interactions between SES and gender. The standard errors in parentheses have been adjusted for the clustering effect within individuals. We find negative associations between SES and depressive symptoms and that the impact of elderly individuals’ SES was stronger for women than for men. Model 1 shows that the main effect of working in the state sector is negatively related to depression, and the interaction term of working in the state sector and gender is significantly and negatively associated with depression (b = –0.852, p < 0.001). The main effect predicts that depressive symptoms decrease when elderly individuals mostly worked in the state sector. The interaction effect suggests that gender differences in depression will be smaller among those who used to work in the state sector than those who used to work in the collective sector. Model 2 summarizes the main effect and interaction effect predicting depression by CPC membership. It shows that the main effect is negatively and significantly associated with depression and suggests that CPC members have lower depressive symptom scores than others (b = –0.855, p < 0.01). Model 3 shows the relationship between hukou status and depressive symptoms, and the predictors of the main effect and interaction term are both significant and negative. Predicted depressive symptom scores are lower for elderly individuals with urban hukou status than for those with rural hukou status (b = –1.936, p < 0.001). The reduction in depressive symptom scores for urban hukou holders relative to rural hukou holders was greater for women than men (b = –0.400, p < 0.05).
Predicting depression by interactions between SES and gender.
Continued.
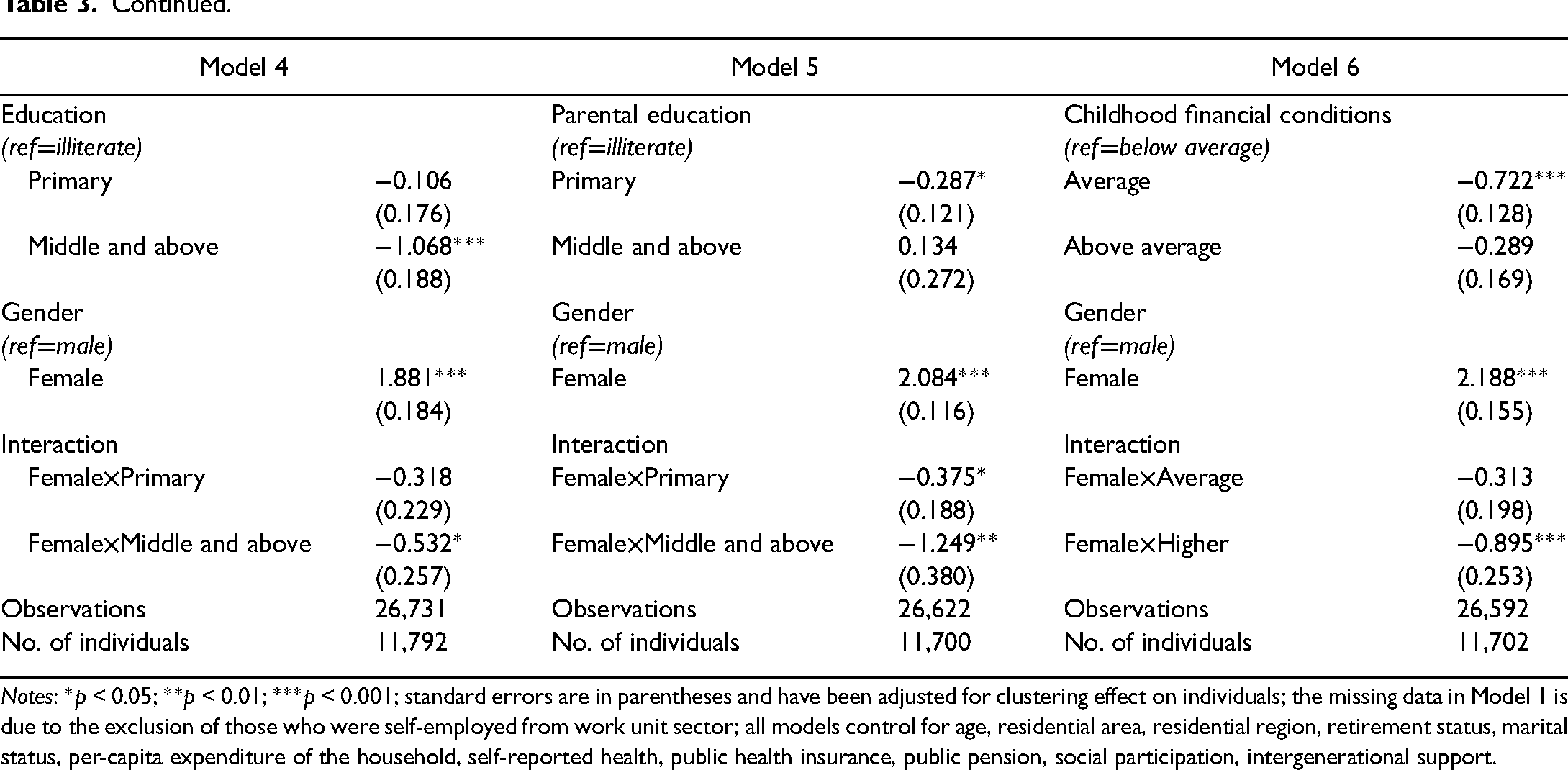
Notes: *p < 0.05; **p < 0.01; ***p < 0.001; standard errors are in parentheses and have been adjusted for clustering effect on individuals; the missing data in Model 1 is due to the exclusion of those who were self-employed from work unit sector; all models control for age, residential area, residential region, retirement status, marital status, per-capita expenditure of the household, self-reported health, public health insurance, public pension, social participation, intergenerational support.
Model 4 examines the relationship between education and depression. The results show that depressive symptom scores reported by individuals with a middle school and higher level of education were lower than those of individuals who were illiterate (b = –1.068, p < 0.001). Although a strong negative effect of education on depressive symptoms exists, women still have higher depressive symptom scores than men despite higher levels of education. However, gender differences in depression decreased among those with higher levels of education (b = –0.532, p < 0.05). Model 5 summarizes the interaction effect between parental education and gender. The results show that parental education is negatively associated with gender differences in depression among elderly Chinese individuals. The gender gap in depression narrowed as the level of parental education increased. Elderly individuals with parents who had a primary school education had a smaller gender gap in depression compared to those with illiterate parents (b = –0.375, p < 0.05), while those whose parents had a middle school education and above experienced an even smaller gender gap in depression than those with illiterate parents (b = –1.249, p < 0.01). Model 6 similarly suggests that above average childhood financial conditions result in a smaller gender gap in depression (b = –0.895, p < 0.001).
To better understand the interaction results, in Figure 1 we plot predicted gender differences in depression by work unit sector (Figure 1(a)), CPC membership (Figure 1(b)), hukou status (Figure 1(c)), education (Figure 1(d)), parental education (Figure 1(e)), and childhood financial condition (Figure 1(f)), based on Models 1–6 of Table 3. Our results show that gender differences in depression decrease as the level of SES increases. The gender differences by SES are significant for the work unit sector, hukou status, education, parental education, and childhood financial condition. Figure 1(a) shows that gender differences in depression are significantly lower among elderly individuals who worked mostly in the state sector than those who worked mostly in the collective sector (p < 0.001). Our results also show that elderly individuals who worked mostly in the state sector had a smaller gender gap than those who worked mostly in the private sector. Figure 1(b) shows that gender differences in depression are very similar between CPC members and non-members. Figure 1(c) shows significant lower gender differences in depression among elderly individuals with urban hukou compared to those with rural hukou (p = 0.038). Figure 1(d) shows that gender differences in depression among individuals with a middle school education and above are significantly smaller than gender differences among illiterate individuals (p = 0.039). Figure 1(e) suggests that the gender gap in depression among elderly individuals declines significantly as the level of parental education increases. The gender gap among individuals whose parents had a middle school and higher level of education is smaller compared to respondents whose parents had a primary school level of education (p = 0.026) or were illiterate (p = 0.001). Elderly individuals with primary-school-educated parents also had a significantly smaller gender gap than those with illiterate parents (p = 0.045). Figure 1(f) shows that gender differences in depression are smaller among elderly individuals from higher-income families than those from middle-income (p = 0.014) and lower-income families (p < 0.001).
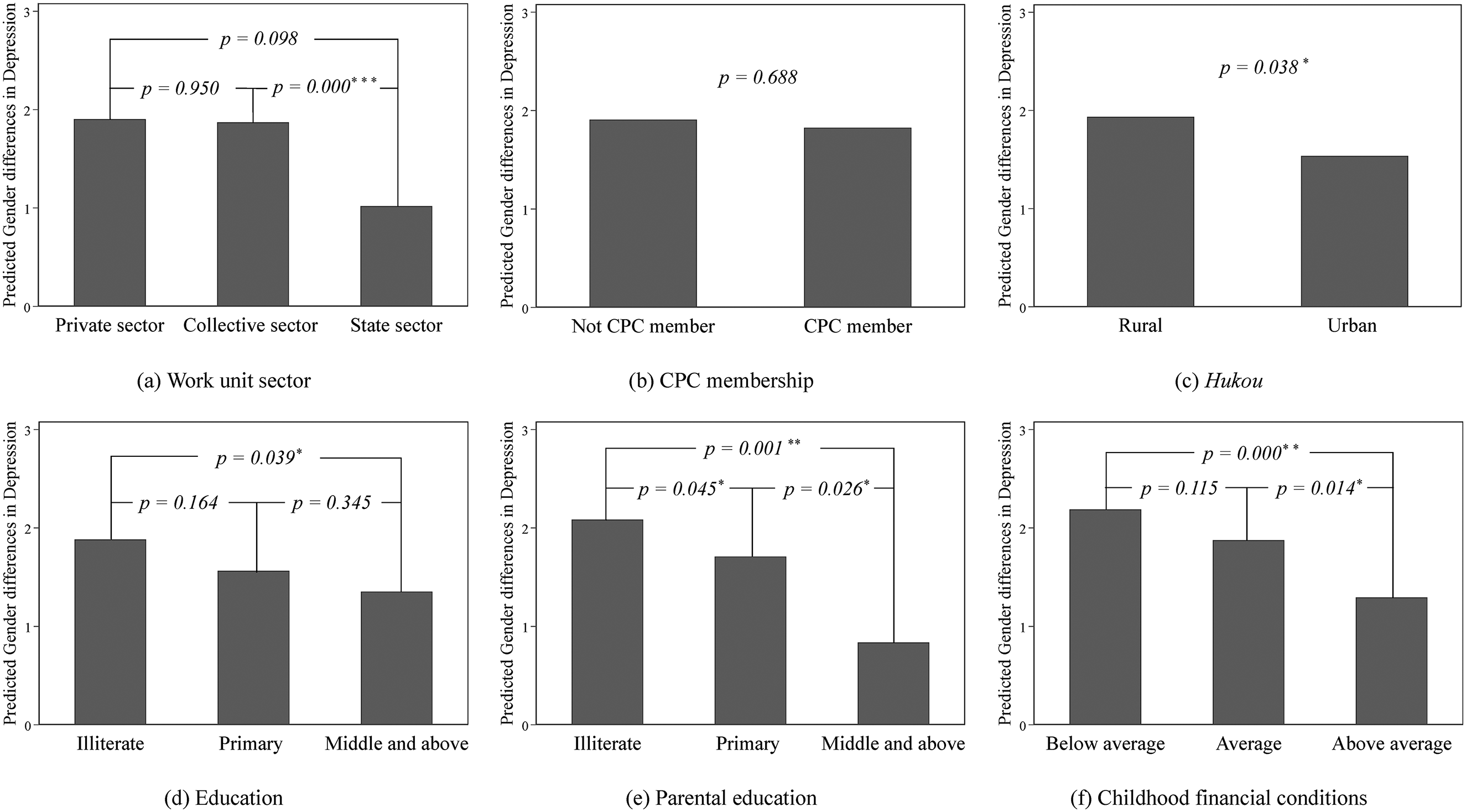
Interaction effect: gender differences in depression by socioeconomic status: (a) work unit sector; (b) Communist Party of China (CPC) membership; (c) Hukou; (d) education; (e) parental education; (f) childhood financial conditions. Note: *p < 0.05; **p < 0.01; ***p < 0.001.
Discussion and conclusions
Previous studies examining the relationship between SES and mental health primarily focused on education and income in Western societies (Clouston and Link, 2021; Zajacova and Lawrence, 2018). However, it is unclear whether the SES disparity in mental health still exists in the unique socio-historical context of China. Drawing on these gaps, we included SES indicators that described the unique characteristics of elderly Chinese individuals within the country's socio-historical context and covered influential life-long factors from childhood to old age, including the work unit sector, CPC membership, hukou status, personal education, parental education, and childhood financial conditions.
Previous research suggests that the work unit sector, CPC membership, and hukou status are major dimensions of social stratification in China (Bian, 2002; Wu, 2010, 2014; Wu and Treiman, 2004, 2007; Xie and Wu, 2008; Zhang and Wu, 2017). The work unit sector serves as both social and economic foundation in Chinese society, encompassing all aspects of individuals’ social and economic lives, including their social status and well-being (Xie and Wu, 2008). Individuals are separated into the state sector, the collective sector, and the private sector. Individuals working in the state sector are more privileged than others (Wu, 2010, 2014) and have more benefits. Furthermore, CPC members enjoy the privilege of accessing more resources and also have better career mobility (Dickson and Rublee, 2000; Li et al., 2007). Similarly, hukou divides individuals into “rural” and “urban” and determines their opportunities, resources, and well-being (Wu and Treiman, 2004, 2007). Individuals with urban hukou status have a greater chance of higher educational attainment, CPC membership, job opportunities, healthcare, and other privileges (Wu and Treiman, 2004). According to fundamental cause theory, we propose that individuals working in the state sector, CPC members, and those with urban hukou status experience fewer depressive symptoms than others because they have more flexible resources to maintain their health, such as routine medical care and more extensive social networks (Link and Phelan, 1995). However, there are only a few studies that examine the association among health, work unit sector (Li and Zimmer, 2013; Nishimura, 2011), and CPC membership (Guo et al., 2017; Li et al., 2016; Song and Smith, 2021).
Consistent with previous studies (Ross and Mirowsky, 2006; Zajacova and Lawrence, 2018), we conclude that depressive symptoms among elderly individuals are negatively associated with SES in China. Consistent with fundamental cause theory, this study shows that elderly individuals who spent most of their lives working in the state sector have better mental health than those who worked in the collective or private sectors. Being a member of the CPC is also associated with a reduction in depressive symptoms. Elderly individuals with urban hukou status have lower depressive symptom scores. The work unit sector, CPC membership, and hukou status partially influence the resources an individual can access and represent individuals’ social status, which largely determines the living environment and medical services that they can obtain. Thus, elderly individuals with higher social status may have better mental health. Consistent with human capital theory, our findings suggest that elderly individuals with higher levels of education (middle school or more) generally report significantly lower depressive symptom scores than their illiterate counterparts. Moreover, from a life-course perspective, we found that social origin is also crucial for the mental health of elderly individuals. We confirmed that early-life experience has cumulative effects that provide individuals with advantages or disadvantages in terms of depression in later life. Elderly individuals with highly educated parents reported fewer depressive symptoms than those with less-educated parents. Similarly, we observed that individuals raised in higher-income families reported fewer depressive symptoms than individuals raised in families with lower incomes.
Recent research has paid increasing attention to the role of SES in the relationship between gender and mental health (Ross et al., 2012; Stanley and Denney, 2023; Zajacova and Lawrence, 2018). In this article, we explored the role of SES in the association between gender and depression by examining interactions between gender and SES, such as the work unit sector, CPC membership, hukou status, education, parental education, and childhood financial conditions. Consistent with resource substitution theory, we conclude that women with higher SES generally experience less depression than men, resulting in a narrowing of the gender gap among individuals with higher SES (Ross and Mirowsky, 2006). SES appears to have a greater impact on overall well-being for women than for men. This could be attributed to the fact that women face more disadvantages in other socioeconomic aspects and depend more on higher SES to enhance their well-being. Specifically, we observed smaller gender differences in depression among elderly individuals who spent most of their lives working in the state sector than those who spend most of their lives working in the private or collective sectors. Possessing urban hukou also predicted a smaller gender gap in depressive symptom scores. Our results show that gender differences are smaller among elderly individuals with a middle school and higher level of education. Elderly individuals whose parents have a middle school and higher level of education also demonstrated a smaller gender gap in depressive symptom scores than those whose parents have lower levels of education. Similarly, individuals from higher-income families have significantly lower gender differences in depressive symptom scores compared to those from average-income families or poor families. Consistent with the status composition perspective, our results suggest that gender differences in depression depend on the different social positions of women and men (Clarke et al., 2011). Based on the cumulative advantage/disadvantage theory, we conclude that the gender disparity in later-life depression could be influenced by childhood conditions (Dannefer, 2003).
Compared to men, women in the CHARLS data appeared to benefit more from the increasing levels of SES attributed to the work unit sector, hukou status, education, parental education, and childhood financial conditions. Elderly women are disadvantaged in society and face more difficulties in obtaining higher SES. Thus, they depend more on their advantaged SES to mitigate the negative impact of other factors on health. Future research might examine how women and men from the different birth cohorts experienced different life-course hurdles. In this article, we focused on individuals born before 1958; in China, individuals of this age range underwent several major social changes. Thus, their early-life experiences may have had significant influences on their later-life mental health. However, recent cohorts, populated by individuals born between 1980 and 1990, have not experienced such significant social changes. However, these individuals are experiencing rapid societal changes that may affect them in later life. In addition, in the cohorts we studied, education levels were generally low, and individuals may not have had opportunities for education, especially women. In contrast, individuals in recent cohorts have had greater opportunities to obtain higher levels of education but are experiencing more stress in employment. Thus, future studies could examine the differences in mental health among cohorts by contrasting their various social and socioeconomic conditions.
One notable limitation of this study is that this is a retrospective study and mainly focuses on individuals from the 1940–1960 birth cohorts. Such a retrospective study can only address depression among the current elderly population. Our study also includes the work unit sector to address how work experience may explain the differences in depressive symptom scores among sectors, but we could not investigate the variations within each sector. In China, the state sector is a hierarchical structure, which is classified into CPC/government agencies, public institutions, and state-owned enterprises (Wu, 2014). The social statuses of individuals working in each unit within the state sector are also different. Another limitation of this study is that we used self-report data to measure depression, which is inherently biased. Older adults with higher SES may experience fewer setbacks and lead happier lives, thus fostering more positive assessments of their mental health. In addition, individuals with higher SES may receive routine physical examinations and have higher aspirations for their futures. Conversely, those with lower SES may be influenced by their living environments, potentially leading to a more pessimistic assessment of their mental health. Thus, the use of such self-reported data may exaggerate the SES gradient in depression scales. Similarly, women generally report worse mental health than men, resulting in greater gender differences in depression scales.
Our study indicates that elderly women with lower SES are more vulnerable to mental health issues. To alleviate depression in this population, future policies might address the health problems of elderly women comprehensively, considering various aspects of their lives. The government and social organizations should develop more social support programs specifically for these women. Such programs could include financial aid, employment support, and home care services. Financial stability and employment stability can alleviate stress and improve mental well-being. Home care services may include training programs for healthcare professionals, social workers, and caregivers to better identify and address the unique needs of elderly women with lower SES. It is essential for communities to have educational campaigns aimed to raise awareness about depression and mental health issues among elderly individuals, provide information about available resources, and encourage early intervention and treatment-seeking behavior.
Our study makes important contributions to research on SES and gender disparities in depression. Firstly, we included multiple measures of SES to describe the unique socio-historical context of China. Secondly, we found that the gender disparity in depression varied across different levels of SES, especially the work unit sector, hukou status, personal education, parental education, and childhood financial conditions. While previous studies paid limited attention to the impact of the work unit sector on health, our study provides valuable empirical evidence demonstrating that the work unit sector can be crucial in influencing health among older Chinese in the aging society. Our research indicates that the work unit sector, parental education, and childhood financial conditions could negatively influence gender differences in depression. The findings from our study will expand future discourse on depression and the role played by SES in gender disparities.
Footnotes
Acknowledgments
This research uses data from CHARLS, a program project supported by Peking University, the National Natural Science Foundation of China, the National Institute on Aging, and the World Bank. Information on how to obtain the CHARLS data files is available on the CHARLS website (https://charls.pku.edu.cn). This analysis uses data or information from the harmonized CHARLS dataset and codebook, Version D as of June 2021 developed by the Gateway to Global Aging Data. The development of the harmonized CHARLS was funded by the National Institute on Aging (R01 AG030153, RC2 AG036619, R03 AG043052). For more information, please refer to ![]() . No direct support was received from grant R01 AG030153, RC2 AG036619, or R03 AG043052 for this analysis.
. No direct support was received from grant R01 AG030153, RC2 AG036619, or R03 AG043052 for this analysis.
Contributorship
Yixuan Tang and Yi Li designed the study, contributed to the data analysis, and drafted the manuscript. Both authors reviewed and edited the manuscript prior to submission.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported the University of Macau (MYRG2022-00201-FSS to Yi Li).