
Abstract
This paper focuses on the religious psychology of peasants who undergo religious conversion in order to cure an illness or disease. Field research was conducted in Wang village in Northern Jiangsu, examining the psychology of newly converted peasants. In academic circles psychology of peasants is usually critiqued according to utility and rationality. In this paper, belief is a starting point for understanding the psychology of peasants. The natural mentality and family ethics of the peasants lead them to place high expectations on religion as a tool for curing disease and facing life crises and dilemmas. The three levels of religious practice include: religious construction of ‘belief’; emotional embedding of ‘belief’; and developing ‘faith’. These requirements lead to the transformation of the individual’s psychological status from secular to religious. Based on the interaction between the individual and religion which is affected by the initial disease and its seriousness, peasants’ religious psychology is divided into three types: collapse of belief; transition of belief; and upgrading of belief. The rituals and different attitudes towards belief constitute the mechanism of developing religious psychology and also shape peasants’ attitudes towards faith. In addition, this paper explores the role of belief in understanding individual religious psychology, religious conversion, and religious revival in Chinese rural religious practices.
Keywords
Introduction
The phenomenon of peasants’ conversion to religion as a possible disease-cure is very common in rural society. Taking Christianity as an example, a national sample survey shows that over two-thirds of Christians confess they became religious because ‘they or their relatives fell ill’ (Jin and Qiu, 2010: 192), and other studies have also revealed this phenomenon (Chen, 2007; Liang and Qi, 2015; Liu, 2006: 65; Zheng and Wang, 2014). In general, in rural areas, when individuals or their close relatives are faced with the miseries of diseases or threat of death, they tend to become religious in response to propaganda and the mobilization of forces inviting them to ‘cure diseases by believing in God’ (Liang, 2006); thus, disease has become one of the most important factors that currently affect peasants’ faith choices.
In recent years, the phenomenon of peasants’ conversion to religion as a possible disease-cure has aroused concern in academic circles. Existing studies mainly involve: (1) the structural background of peasants’ conversion to religion as a possible disease-cure, for example, increasing uncertainty in a high-risk society, individualization of risk bearers in the structural transition in rural areas, insufficiency of medical resources, and imperfect social security (Han and Wang, 2014; Li, 2012; Wang, 2008: 47; Zheng et al., 2010); (2) religious practices concerning disease treatment, for example, Christianity has historically provided its own interpretation systems for the treatment of diseases, giving diseases and sufferings positive value and meaning (Li, 2012) and maintaining that diseases can be treated through the ‘integration of therapies and God’ (Liang, 2014: 45–46); and (3) social results of peasants’ conversions to religion as a possible disease-cure, for example, the prevalence of ‘devil culture’ (Liang and Qi, 2015) and its hidden troubles to the order of rural society (Zheng and Wang, 2014).
These studies have provided useful insights for understanding the background, process, and results of peasants’ conversion to religion as a possible disease-cure. However, we should also note that existing studies have shown insufficient concern with the subjective reactions of peasants’ religious psychological experiences and their evolution. Thus, this paper will focus on this topic, 1 not only to consider the matter from the ‘subject’s’ perspective, but also because it is an essential aspect of faith life and may even constitute a micro-foundation for better understanding existing topics.
In psychology of religion, some scholars tend to associate the phenomenon of the old saying, ‘Embrace the Buddha’s feet and pray for help in times of crisis’ with the psychological reactions of individuals suffering from life difficulties or crises, especially those who become religious after encountering a disease, a phenomenon which these scholars attribute to the converts’ having ‘utilitarian’ motives. For example, Gao (2005) believes that when actual conditions can hardly satisfy peasants’ appeals for peace and the elimination of disasters and diseases, religion becomes the last resort from which they may improve their situation. Therefore, religious motives show strong utilitarian and practical characteristics; Zhang (2010) critically pointed out that ‘Utilitarian religious belief is a transaction with Buddha and God’ (Zhang, 2010); Qin and Kong (1990: 53) also maintained that the Chinese have only purely utilitarian piety and are often concerned with seeking maximization of their immediate interests; Wu (1999) explored the Chinese tradition of utilitarianism; and Japanese scholar Nakamura (1989) even considered it standard thinking among the oriental nationalities as a whole.
In essence, many scholars have regarded utilitarianism as a distinguishing characteristic of Chinese religious culture. For example, Tang (1943: 222) maintained, in early studies, that Chinese religions were filled with secular spirit, while Liang (2005 [1949]: 90–92) even pointed out that there was no religion characterized by the ‘supramundane’ in China. This distinctive pattern in Chinese ‘becoming religious’, informed the dispute on the existence of ‘pure faith’ and even ‘religion’ in China (Fang, 2014). By applying the popular theory of ‘rational choice’, some studies have judged an individual’s religious psychology based on the ‘rational person’ 2 hypothesis and assumed that conversion to a religion as a possible disease-cure is rational behavior on the part of an individual, a rational calculation based on a ‘cost–benefit’ analysis to satisfy the person’s secular demands proactively and purposefully (Han and Wang, 2014; Zheng et al., 2010).
We believe that although the judgments of utilitarianism and the ‘rational person’ may reflect some psychological and behavioral characteristics, they cannot precisely represent the complex psychology of Chinese peasants resorting to religion as a possible disease-cure, and thus these judgments may hinder further research in this area. On the one hand, they failed to take the dynamic and evolving characteristics of religious psychology into account. As both empirical studies and religious practices themselves have revealed, not all believers in a given religion are alike: taking Christians as an example, although some people gradually become pious believers, others hold utilitarian attitudes; some may choose to stay in the church, while others may choose to leave (Liang and Qi, 2015). In general, in understanding an individual’s psychological changes, especially non-utilitarian and ‘irrational’ behaviors that are not goal-oriented (for example, maintaining a devout conversion despite no improvement in a disease), it is unconvincing to make judgments based merely on utility and rationality. On the other hand, with the general judgments based on utility and rationality, scholars tend to believe that conversion to religion as a possible disease-cure is the same as other utilitarian or rational religious behaviors, such as praying for children and peace, and deem it unworthy of specialized research; even in many doctoral theses based on substantial field studies, seeking a possible disease-cure is regarded as just one reason for becoming religious, without any further discussion (Huang, 2003: 59; Liu, 2006: 65; Wang, 2008: 47).
Here, we need to set aside the existing judgments based on utilitarianism and rationality and analyze the religious psychology of peasant believers based on empirical materials. Before beginning our main discussion, we need to conduct a brief review of the relevant theoretical resources. Apparently, conversion to religion as a possible disease-cure mainly refers to the relationship between ‘crisis’ and ‘conversion’ 3 . It is generally assumed in existing research studies that the dilemmas and crises in individuals’ lives are key factors for their religious conversions. William James’s understanding of conversion implies an emphasis on crisis; in his opinion, conversion indicates a psychological process, that is, ‘a self hitherto divided, and consciously wrong inferior and unhappy, becomes unified and consciously right superior and happy, in consequence of its firmer hold upon religious realities’ (James, 2012: 142). Here, crisis is generally regarded as an opportunity to discover the meaning of religion. Based on this idea, the classic theories on conversion take crisis and the resulting intense experiences as the basic conditions for conversion (Lofland and Stark, 1965; Rambo and Bauman, 2012).
The literature contains abundant discussions about how crisis has contributed to religious conversion. On the one hand, some studies emphasize that this kind of conversion is a gradual mental process, rather than a sudden and instantaneous experience. It consists of several stages, and a believer’s conversion evolves step-by-step along this path (Johnstone, 2012: 184–185). During the process, individuals gradually achieve religious maturity in respect to cognition, emotion, and morality (Conn, 1986). On the other hand, some studies analyze the external elements of promoting conversion. For example, some scholars have noticed the influence of religious groups and believe that conversion is subject to their influence and manipulation, maintaining that group relations and their emotions have contributed to the occurrence of conversion (Zetterberg, 1952); some studies have focused on the role of preachers and point out that preachers often incorporate individual crisis experiences into religious discourses through persuasive language, thus providing individuals with powerful religious narratives (Stromberg, 1993); some studies emphasize the importance of doctrines and rituals (Sarbin and Adler, 1970) and even miracles (Stark and Finke, 2004: 135–136). The theoretical resources above suggest that we should pay attention to the stages of a process and focus on the external mechanisms that cause changes in religious psychology. On this basis, we try to analyze the initial religious psychology and its tendencies and differentiation in the interaction between the individual and religion. Therefore, we try to summarize the evolutionary mechanisms of peasants’ religious psychology and expound upon the topics of individuals’ religious psychology, religious conversions, and religious revivals in rural China as represented by the phenomenon of conversion to religion as a possible disease-cure.
This type of conversion among peasants has been the main driving force for the development of Christianity in the rural areas of northern Jiangsu. This paper focuses on the phenomenon of conversion to religion as a possible disease-cure among peasants in Wang village in northern Jiangsu province. 4 Wang village is located in SY County, SQ City, northern Jiangsu province. According to the staff of the County Ethnic and Religious Affairs Bureau, Christianity has enjoyed rapid development in SY County since the 1980s and has become the main religion in the rural society of SY County. Wang village has 12 groups of villagers, 1070 households, and a total population of over 4600. There is a Christian church called ‘Wang Village Church’. Before 1982, the Christian activities were more like an irregular family gathering, which was changed by the formal establishment of the church in this year. As the number of attendees increased, the church was rebuilt in 2003 on a large scale and at present has a hall accommodating 1500 people. With a readily available infrastructure, it is the best-known rural church in the northern area of SY County. Attendees come not only from Wang village, but also from the 24 surrounding villages. As with many rural churches, the church does not have a strict registration system of attendees, and thus, it is difficult to obtain accurate statistics. According to the rough estimate of the person in charge of the church, 5 there are at least 2000 attendees. In the local area, people generally judge Christians by ‘going to the church or not’. In other words, there is no strict system for identity acquisition as Christians. In addition to the traditional personnel composition of many old people, women, and illiterates, in recent years, the number of middle-aged attendees has also increased. Among them, believers after conversion to religion as a possible disease-cure account for more than two-thirds of the total, generally having been introduced to the church by relatives or acquaintances. There are cases of individuals falling ill themselves, and in many cases, if one member in a family falls ill, all other family members may convert to Christianity.
By browsing the attendees’ medical records from the village clinics and consulting with local doctors, we found that the peasants were afflicted with various chronic diseases before they became religious, 6 particularly diseases that had a long course and were difficult to cure (World Health Organization, 2005). In recent years, although Jiangsu province and SQ City have launched a series of beneficial initiatives in the new rural cooperative medical care system, due to type and proportion limitations in reimbursement, medical care is still a large burden on farmers suffering from chronic diseases. Yang and Liang (2009) pointed out that peasants tend to divide diseases into ‘minor diseases’ and ‘serious diseases’, which are judgments based on treatment costs (expenditure and time), and chronic diseases that require long treatments are undoubtedly ‘serious diseases’ for peasants due to their high costs. When the conventional channels for health-care seeking are unable to satisfy peasants’ aspirations for disease cures, the dissemination slogan ‘curing diseases by believing in Christianity’ constructed by rural Christian churches is appealing to them and becomes the direct motivator for peasants seeking medical care to convert to the religion. From 2014 to 2016, we went to Wang village several times to conduct investigations. In order to capture the religious psychology of subjects’ emotional experiences, this article is presented mainly through the narration of church-attendees and their families. We completed about 90 interviews with Christians and their family members affected by diseases, church leaders, preachers, non-Christians, village doctors, and village cadres. In the meantime, we also conducted long-term diachronic observations of several church attendees and observed preaching activities and treatment rituals in churches.
‘Belief’ as the psychological starting point
Some scholars have said that when studying religious practices in China, special attention should be paid to the social scientification of ‘local concepts’ such as ‘efficacy’ and ‘righteousness’, that otherwise, the most imperceptible and core content of Chinese religions will be neglected (Lu, 2013). We quite agree with this view and believe that we should carefully review the pre-defined understanding of the ‘native concepts’ we present and reconsider the true meanings of these concepts from the perspective of those using them. As a matter of fact, the daily expression of ‘believing in a religion’ for peasants entails two concepts: ‘belief’; and ‘religion’. Although the word ‘religion’ corresponds to the discourse of religion, in recent years, there have been reflections and introspections on this in academic circles, 7 with scarce concern for the concept of ‘belief’. ‘Belief’ in the Chinese context contains various connotations. If we take up ‘belief’ again and consider its possible meanings, we may be given new insights. In this paper, the Chinese ‘belief’ is the starting point for our understanding of individuals’ religious psychology.
The first issue researchers must deal with is the conventional judgment of ‘faith’ on ‘belief’ in religious life. We believe that it is far from precise to talk about farmers taking up a ‘belief’ as ‘faith’ in the early stage of converting to a religion.
8
Interviewee X, a current local religious leader, expressed her feelings when she first converted to Christianity: I converted to Christianity over 30 years ago, when I was paralyzed from an unknown disease. I wasn’t cured and later had no money for treatment, and had to lie paralyzed at home. Later, I heard from the preachers that my disease could be cured if I believed in Jesus, so I believed in him since I didn’t have to spend money or take medicine. To be honest, we all experienced the ten years (1966–1976), when we struck down all the monsters and demons, so how can we believe in God? Christianity was restricted at that time, although even then, we believed that religion could cure diseases. In a disease attack, we went to church to pray and read the Bible. When we felt better, we stopped going to church. It is the same with the hospital. When in good health, we won’t take medicine and see the doctor, and when we feel ill, we do take the medicine and visit the doctor. (Interview, 3 February 2014)
As for the conventional concept of ‘(religious) faith’, it is undoubtedly meaningful. In a broader sense, it refers to a ‘complex system’ that includes religious organizations, groups, rituals, and doctrines. In this sense, ‘religious belief’ basically equals the use of the concept ‘religion’ with unified and integrated connotation characteristics (many academic expressions use ‘religious faith’ in a general sense). In a narrow sense, religious faith is an essential element of ‘religion’. It denotes the cognitive and conceptual aspects of religion and is a self-contained conceptual system usually codified in formalized religious classics, doctrine manuals and creeds, or non-formal myths, icons, norms, and values (Sun, 2015: 72). Thus, religious faith and religious rituals, religious groups, and religious organizations altogether compose the basic elements of ‘religions’; whether used in a narrow or broad sense, we find that both concepts point to external matters at the institutionalized level while ignoring concerns about religious psychology based on people’s inner feelings. In other words, for individual practitioners, the existent expression of ‘religious faith’ is more about a superficial ‘identity declaration’, which is institutionalized, static, and easily observable. For instance, when we say someone has ‘Christian faith’ or ‘belief in Christianity’, we generally mean that the person has acquired a religious identity as a ‘Christian’; therefore, expressions such as ‘superficial faith’ or ‘moderate faith’ refer to the instrumental appeals behind the religious identity (that is, meeting one’s pragmatic objectives by acquiring a religious identity), and the status of ‘faith’ in a psychological sense, for example, the emotional and religious experiences embodied in faith and the God–man relationship embodied in ‘faith’ are neglected. James defined ‘religious faith’ as ‘the feelings, acts, and experiences of individual men in their solitude, so far as they apprehend themselves to stand in relation to whatever they may consider the divine’ (James, 2012: 23). In this sense, whatever the literal meaning of ‘faith’ or its essential requirements might be, the individual should have a kind of transcendental rather than secular, pious rather than pragmatic experience and ultimate concern, which points to ‘sacredness’. In this paper, we discuss the relationship between ‘faith’ and ‘belief’ of peasants converting to religion as a possible disease-cure in terms of individuals’ religious psychology and religious experiences.
From the perspective of religious psychology, ‘faith’ has nothing to do with utilitarian appeals, but is a transcendental state in pursuit of supreme value and ultimate meaning. Compared with the type of faith that regards religion as an end in itself rather than as an instrument, the religious attitudes of the peasants in the early days of converting to religion can hardly be seen as stemming from ‘faith’. 10
In fact, church attendees have pertinent views on their ‘beliefs’ in the early stages of practicing a religion. In a focused interview, in answering questions regarding their beliefs they made similar statements. For example, S said: When I believed at that time, how should I say, I was partially doubtful about the existence of God, since God can’t be seen and touched. That kind of ‘belief’ was ambiguous, and I didn’t follow God’s requirement from my heart. At that time, other than believing in Jesus, I believed in the devil’s chief.
11
I chose to believe in whomever if they could cure my rheumatic disease that tortured me for years. At that time, I felt I was indebted to God and had no confidence in God. I held the belief that I would be granted whatever is requested. If I believed in God, my disease would be cured, otherwise, I believed that God was of no avail. I always felt that I could do nothing if I went to the church on every worship day. It is really a waste of time. How can I come to church again? When I first believed in God, I felt I was not totally committed to it. At that time, when other people beside me were praying, murmuring some words, I just followed them and knelt down, but I could understand nothing. After I went to church with others for some days, I found that my disease didn’t recover, and moreover, I needed to take care of kids and do farm work, earn some money, so then I went to the church much less often... I felt I treated church as an instrument (Focused interviews, 10 March 2014).
In this paper, the pre-judgment of faith is temporarily laid aside, and the proper meaning of ‘belief’ will be explored. Such treatment is not merely an analysis of word meaning, but is helpful for us to understand the true psychological status of peasants in the first stages of believing in a religion. Danièle Hervieu-Léger, the French sociologist of religion, has keenly pointed out that belief in modern society is not necessarily associated with religion, that people can believe in science, progress, or revolution, and that belief in a religion is just one form of the many beliefs in modern society (quoted by Ji, 2005). In other words, ‘belief’ as a channel that connects ‘disease-cures’ and ‘religion’ has a certain degree of logic; however, it does not mean religiousness as a kind of inborn and inevitable impulse towards faith. Church attendee P described his cognitive changes concerning the relationship between disease and his religion: Now it seems that disease is the way through which God chose us. However, at first I didn’t think so; I only believed that since I had fallen ill and become paralyzed, I would believe in whatever if it could cure my disease... At first, I went to the hospital and believed in doctors, not God, but I was not cured. I converted to God since I had nowhere else to go... Such feeling was just like I fell into a river but could not swim. I reached my hand out to catch something before I drowned. (Interview, 15 April 2014)
The difference between ‘faith’ and ‘belief’ in the Chinese context is that while ‘faith’ implies value and significance as a response to the ultimate questions of life and an expression of value rationality, ‘belief’ is a kind of ‘convinced view by oneself’ 12 that has some hint of objective orientation. ‘Faith’ contains the unconditional, definite cognitive status towards the ‘divine being’, with strong traits of transcendence and redemption in emotion and will. ‘Belief’, on the other hand, implies cognition that regards religion as an instrument, and the emotion and will in it are centered on a particular goal, which is generally secular rather than an absolute value hierarchy. It is the psychological status of the subject who expects to achieve the secular goal of ‘success’. As the usual expression of ‘the belief that must win’ shows, the ‘belief’ status is an important condition for the subject to achieve the goal, and it is based on instrumental rationality. In general, as psychological processes of different natures, faith and belief have significant differences in terms of cognition, emotion and will. 13
If we take ‘belief’ as describing peasants’ mental status in converting to a religion, ‘seeking disease treatment’ as the specified goal and the resulting instrumentalization of religion are self-evident. How, then, can we understand the emotion and will investment in the process? In field investigations, we made diachronic observations of several church attendees who first converted to a religion and found that each follower showed intense emotion in rituals, with high levels of concentration and devotion, and some people burst into tears. In the several observations, we learned that practitioner C, a typical case, went to church only to pray when he was attacked with disease and had never even read the Bible. After a prayer session, when we asked him if he devoted all his heart to praying, he seemed very surprised by our question and replied with absolute sincerity: How could I not put my heart in it? Only by offering myself to the God, can He feel my devotion... I believe that God has great ability... to cure my disease. There is no need to come to the church if I am not devoted. I expect to recover from my disease. After each prayer, I would recall all the tortures I experienced from my disease and burst into tears. (Interview, 22 July 2014) At first, their ‘belief’ was the same as mine: we had to believe in it. There was no hope of curing the disease; we had to place our hope in Christianity and God. There was a sense of forcing ourselves to believe in it. We had to force ourselves to believe in it. How could we find the way if we didn’t believe in it? Otherwise, we had to wait for death. There might be hope of curing our diseases if we believed in it... It is just like the situation in which you see a doctor when you are seriously ill; you have to believe that doctor... it is just like a life-saving straw, there is some hope if you can catch it; otherwise, you are entirely hopeless. (Interview, 23 July 2014)
Furthermore, Chinese ‘belief’ also carries the family ethics of settling down and living a peaceful life. In the interviews, many practitioners in the early stages of converting to Christianity revealed their concerns and worries about their families and loved ones. Church attendee S said: My disease [note: serious rheumatoid arthritis in personal statement] required an intravenous drip, which cost me thousands of yuan; however, it was not cured. I can’t work, can’t earn money, my two children are still young, their father does heavy manual work, and is also not in good health. If my disease is not cured, I don’t care, but my poor children, they are so young... For the sake of the children, I will endure whatever I have to suffer. (Interview, 22 July 2014) I feel great pressure, not only for the reason of my disease, but also because my two sons are not married, and I haven’t built a new house. I haven’t finished my family mission. People say, ‘When one believes in Christianity, the whole family would live in peace’. When I am praying, I pray for my health and my sons’ marriages and smooth careers. (Interview, 22 July 2014) Conceptual structure of ‘belief’.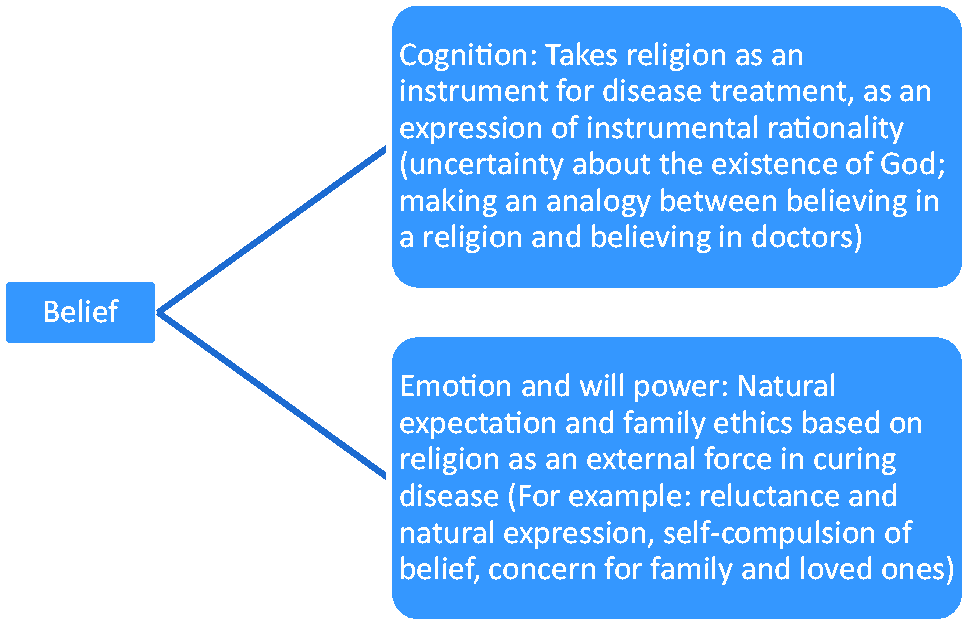
Without doubt, the conceptual structure of ‘belief’ introduced here is rough and may even be a summarization of the lowest level. Religious psychology itself is complicated, and individuals’ experiences of belief possess specialized features (for example, being influenced by age, gender, personality, etc.); nevertheless, we feel that such induction represents the realistic and cultural structure of ‘belief’, which comes from individuals’ desires to overcome difficulties under structural circumstances as well as from the cultural traditions of their families. It transcends individualism and privacy to some degree and becomes a common group-mind for each peasant converting to religion as a possible disease-cure.
Religion and belief
We believe that in order to better understand individuals’ religious psychology, it is necessary to study the evolution of individuals’ beliefs in relation to their religious practices from the perspective of dynamic interaction. In the interaction between individuals and religion, we found that, through a specific technological practice mechanism, religion tries to change an individual’s mental status from mere belief as a starting point to the status of faith, which is a progression from secular to religious. The progression includes three stages – religious construction of ‘belief’, emotional embedding of ‘belief’, and ‘faith requirement’ 14 – while the ‘family ethics’ embodied in ‘belief’ remain in a stable and reinforced status.
The ‘religious construction’ of ‘belief’
‘Religious construction’ refers to the inclusion of individuals’ ‘beliefs’ into the domain of religion, endowing them with religious orientation. During the process, abstract and rough expectations in the minds of actors towards a common outside force are changed into specific psychological feelings toward some outside force (event or matter), and this process is realized through the religious attribution of diseases. Anthropologist Robert Hahn (2010: 23) calls the various views and understandings of disease ‘accounts of diseases,’ which address the questions of ‘who has the disease’; ‘what kind of disease it is’; ‘what organ has the disease’; ‘when did someone come down with the disease’; and ‘why does one get such a disease’. In the account of diseases in rural Chinese Christianity, disease is attributed to ‘being possessed by a devil’, that is, the diabolical possession produced the disease symptoms. 15
For believers, ‘devils’ as ‘demons’ and ‘pests’ are the real sources of human disasters. Patients’ diseases are caused by ‘evils by devils’; thus, in order to cure diseases, one must drive the devils away. It is worth mentioning that in the religious lives of believers in Wang village, the ‘devils’ refer to certain animal spirits, such as snake and fox spirits in Chinese traditional spirits culture. The ‘devil possessed disease’ constructed by rural Christianity is a mixture of the Christian Satan and Chinese folk culture, and the compatibility between them makes the explanation ‘being possessed by the devil’ more understandable and acceptable. In addition, diseases are regarded as a kind of trial by which God selects disciples (Liang and Qi, 2015). Preacher K said: If we are safe and sound, who will see God? Such people have no diseases or difficulties, and thus they would not seek blessing from the God, and naturally they cannot understand God. Only when they are ill and have suffered from difficulties, can they communicate with God. (Interview, 1 October 2014) May the Holy Spirit come fast; Jesus shall give them a deadly blast... The first strike to the old demon, to beat it off to its den; the second strike to the weasel spirits, who are the most wicked pests; the third strike to the ghost turned from a weasel, which will survive tonight at most; the fourth strike to the fox spirits, for whom there’s no time to rest; the fifth strike to the old monster, who has nowhere to shelter; the sixth strike to the deaf and blind spirits, all of whom Jesus will send to the fiery pit; the seventh and eighth come together, which will make those demons fluster; the ninth strike to all ghosts, so the gospel will prevail all over the world; and the tenth strike to the white snake, which we will send into the fiery furnace to bake. (Participant observation, 20 August 2014)
16
My previous illness was not cured after I went everywhere to find a treatment. I went to the county and provincial hospitals and felt I was dying. At that time, it was too late to cure my disease. Then I believed in Jesus and He cured me. You see, I am safe and sound now... I wasn’t cured before, because the devil was in me, but now God has driven the devil out of me, and I am cured. (Participant observation, 24 August 2014)
17
An individual was experiencing the onset of a disease involving serious convulsions and vomiting, and his family immediately sent him to the church. X walked over to the sufferer and patted his forehead with his hand, chanted some scriptures, and then yelled, ‘You devil, in the name of Jesus, I command you to stay away from him!’ (Participant observation, 20 July 2015)
18
The rituals described above endow disease with religious meaning that forms the religious construction of ‘belief’, which can be found in the following effects of the rituals: first, they shape a justified cognition on the subject of devils. After many rituals (especially the exorcism ritual), under repeated indoctrination regarding the ‘devil's disease’, believers feel that ‘the devil is around’ and produces the fearful experience of being possessed; and second, they enhance confidence in God’s exorcising ability, endowing individuals with confidence in God’s exorcising ability and the consequent increased willpower among individuals. Church attendee F vividly described his feelings after attending witnessing and chanting rituals: The whole body is full of energy, and I have never felt such power before. It seems that the Lord is in me. I am no longer the me I was before. I seem to have an amulet, and no devils can approach me. (Interview, 22 August 2014)
Emotional embedding of belief
Emotional embedding refers to the embedding of specific religious emotions (such as guilt or awe) experienced during religious activities into the belief experiences of individuals. It can be said that all aspects of religious life, including doctrine learning, evangelists’ guidance, prayer, and poetry chanting will promote this process. Among the various factors affecting individuals’ religious emotions, we have discovered a special mechanism: attributing the onset of disease to ‘sin’. This mechanism is key to the embedding of religious emotions.
First, let us discuss the onset of disease. From the perspective of modern science, religious treatment is effective in improving people’s mental health, but less effective for the objective aspect of physical health (Argyle, 2005: 150). A great deal of research shows that, although the religious individual may believe that their health status has improved, the objective condition of health has not been changed (Glik, 1986; Idler, 1995). In this case, even if an individual accepts religious treatment, another onset of the disease (including the duration, repetition, and exacerbation of the original symptoms) is not rare. How does local Christianity deal with such cases? This is related to the attribution of ‘sin’. Preacher Z said: We didn’t mean that the disease will be cured if we come to the church. If you are not cured, that’s because the devil invaded in your body, while the reason for the invasion was that you have sin. God wants to see your heart. If you have sin, you must confess your sin before God, and ask for blessing, to cleanse your sin, and forgive all sins. After repentance, you should pray in front of God every day. In short, you should repent, repentance can cure the disease... As with the government now, if you have committed a crime, only after you admit your mistakes in the cell can you reduce your sentence. In the same way, you must repent before God and ask God to forgive your sins. For example, idolatry, swearing, showing no respect for the elderly, greed, stealing, they are all sins, and there are ‘The Ten Commandments’ in the Bible. In short, if we don’t act in accordance with God’s words and requirements, we have sin. That is to say, we are indebted to the glory of God. (Interview, 28 August 2015) When I was attacked by the disease, I thought at the beginning that since I had the disease, there are just cases of the onset of the disease. Later, after I heard the gospels from preachers and my brothers and sisters, I knew the reason was that I had sin. I didn’t listen to God, so the devil was in my body. If you want to get cured, you must repent and be wholeheartedly devoted to God. (Interview, 3 September 2014) Recall whether you have done anything against God in this period or before. If the disease is not cured, the reason is that the sin has not been found. If you have found the sin, and then repent in front of God, the disease will be cured. I came to the church every day to repent and asked God to forgive my sins. I reflected on what I had done during this time, and I confessed. I am still ill. I knew that my sin was not found, so I recalled what I had done before. I thought hard, and thought about what I could remember, thought about what sins I have committed before. Then I recalled that more than ten years ago, I cut a large area of corn in the field of my neighbor after some quarrels with him. I sincerely repented to God and prayed for God’s forgiveness. Shortly afterwards, my health status became better. I knew that my sin was found. (Interview, 3 October 2016)
After this period, although the religious experience is constantly changing in terms of the individual’s beliefs, it is still focused on ‘disease treatment’, and therefore, it is far from faith in a strict sense, which will be discussed in the next subsection.
‘Faith requirements’
The phrase ‘Faith requirements’ refers to the fact that religion guides believers to abandon the core goal of disease treatment in the belief experience, and turn to a higher faith state which takes transcendental values as its appeal. In terms of rural Christianity, it refers to guiding believers’ transformation from seeking ‘physical peace’ to the pursuit of ‘soul salvation’. This is mainly implemented through frequent sermons in church.
Peasant believers with limited education have to deal with many daily life chores, and the sermons on Wednesdays and Sundays serve as their main channel for acquiring religious knowledge and understanding the Christian faith. The preachers are mainly middle-aged peasant women with strong beliefs and good expressiveness skills. The main goal of a sermon is to guide church attendees to the ‘right path’ (as stated by the preachers). The essence of preaching is to encourage them to give up utilitarian ideas of getting what they need and focusing only on physical peace and turn to a faithful life of devout service and the pursuit of soul redemption. Through attendance at several sermons, we observed the following stages: 19
First, the idea that emphasizing God’s willingness to ‘grant whatever is requested’ is an expression of impoliteness towards God and constitutes a kind of sin. In the sermon, Z criticized believers for holding utilitarian ideas: They are not devoted to God, and God certainly will not bless them. They cherish the idea of ‘getting whatever I requested of God’, that is to say, since I asked God, God should improve my condition... I usually don’t come to church, I come to the church only when I am seriously ill. I am not devoted and not pious, I was just pretending to be a Christian... It’s sinful to God. Since I had sin, the devil would invade me and the disease will attack me. (Participant observation, 9 October 2016)
Next, the preacher pointed out that the only way to get rid of sin is to listen to God’s words and do whatever God requires: Although you sinned, have been left behind, and feel irresolute, God will not abandon you. God will bring you back... Just talking about myself, I have rheumatism, which can hardly be cured, then I believed in Jesus, and my health indeed became better. If you want to get better, you don’t have to go; later I sometimes quit going to the church and wanted to earn some money, but the disease attacked me again. As X told me, I understood that I am indebted to God, that is sin. Later, when I realized that I had sin, I came to the church every day to pray and made sacrifices to the church, listened to the words of God, met God’s requirements, and the disease slowly improved. My rheumatism is now much better and I rarely take medicine. (Participant observation, 9 October 2016)
Finally, the preacher stated regarding requests of God that the ‘salvation of the soul’, is more important than physical peace and highlighted the sense of holiness in religious experiences. Preacher W said: God’s mind, God’s path, God’s view, and God’s standard are totally different from that of ours. What God treasures is not the thing that we treasure. This is because we often treat questions with secular opinions, we are so realistic. And when we practice the wisdom in the Bible in our lives, God will lead us to abandon what we value and pursue what God values, and make us Christians who match the requirements of God. Among many of our brothers and sisters, some people prayed to God, and believed that God would give them whatever they requested, and that God should do what they wished God to do. They valued their physical health more, but on the contrary, God values the salvation of the soul more. God says, ‘It is the spirit that quickeneth; the flesh profiteth nothing’. ‘God values moral quality, because moral quality is more important than the sacrifice’; ‘God values what’s inside, because that is more important than what’s outside’; and ‘God values the motivation, which is more important than the action’. Among them, the emphasis is on the importance and path of the salvation of the soul and faith in God. Faith requires one “to worship God with heart and honesty. Never fancy your smartness; you should not deceive God with a respectful appearance, but give your heart to God so that your soul can be saved, and change the ‘old person’ into a ‘new person’ ”. (Participant observation, 9 October 2016)
Through the presentation of the three stages above, we can see the gradual transition from ‘belief’ to ‘faith’ among those receiving the guidance of religion. Church director and preacher L summarized the methods and skills involved in preaching: Our mission is to slowly put them on the right track. It is just like the guidance of parents to children, you can’t ask a child to do something well all at once. You should let him grow slowly and educate him. When people come to God, it is just like children before their mothers. First is breast nursing and after they grow up, educate them and feed them with food, and later, they can eat by themselves. After he comes here, tell him you are safe and your soul will be saved if you trust God. He will benefit from believing in Jesus, and his family also will benefit from it. So, we should give guidance gradually. At this time, you can’t say that this can’t be done, or that can’t be done. Then through rituals, prayers, and sermons, lead them to give their hearts to God, fill them with the words of God, and guide them to abandon utilitarian ideas. (Interview, 9 October 2014)
Differentiation of ‘belief’
The Chinese concept of ‘belief’ includes an evolutionary path that encourages individuals’ religious psychology to evolve from secular to religious status, which can be expressed as shown in Figure 2.
Evolutionary path of individuals’ religious psychology in religious practice.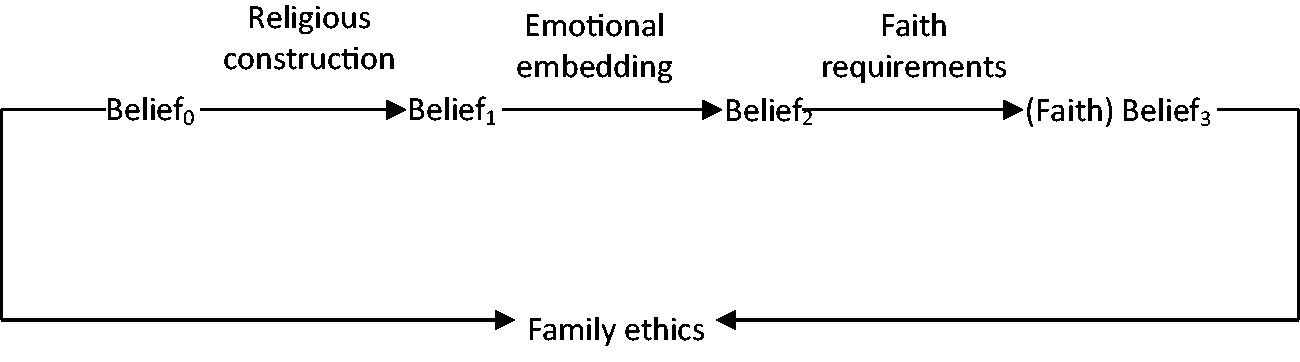
On this path, ‘belief0’ is a general belief. As a psychological starting point, the concept indicates openness, to which religion is only one possibility, a possibility that represents the ‘natural expectations’ of individuals facing of external forces causing them difficulties. ‘Belief1’ is a ‘belief0’ within the religious domain. It refers to confirmed cognition regarding the devil and confidence in God. ‘Belief2’ is embedded in a specific sense of sin, repentance, and awe based on ‘belief1’; ‘faith (belief3)’ can be understood as ‘pure’ faith, the pursuit of transcendental values in religious belief, which corresponds to the sense of salvation and transcendence. If this path is regarded as the belief journey for peasants converting to religion as a possible cure for diseases, then it can be said that ‘belief0’ constitutes the starting point of faith; ‘belief1’ and ‘belief2’ constitute intermediate stages of faith; while ‘faith (belief3)’ constitutes the ultimate stage of faith practice. Family ethics run through the entire evolutionary journey of belief.
Undoubtedly, this possible route is directed to every believer converting to religion in search of a disease-cure, but it does not mean that the individual’s psychological evolution will necessarily follow this path. On the contrary, there are still obvious facts regarding differences between believers. However, our findings differ from the differentiation mechanism based on efficacy in terms of ‘utility’ and ‘the rational man’. As our interviews with church attendees showed, the onset of a disease often provides an opportunity for the religious to elevate the belief experience. It is precisely because the individual does not fully recover that the individual reflects on the issue of sin, which carries the sense of sin, repentance, and awe, to provide a psychological foundation for the further elevation of faith. Before discussing the mechanism of belief differentiation, we first present the following three typical cases:
Differentiation of ‘belief’.
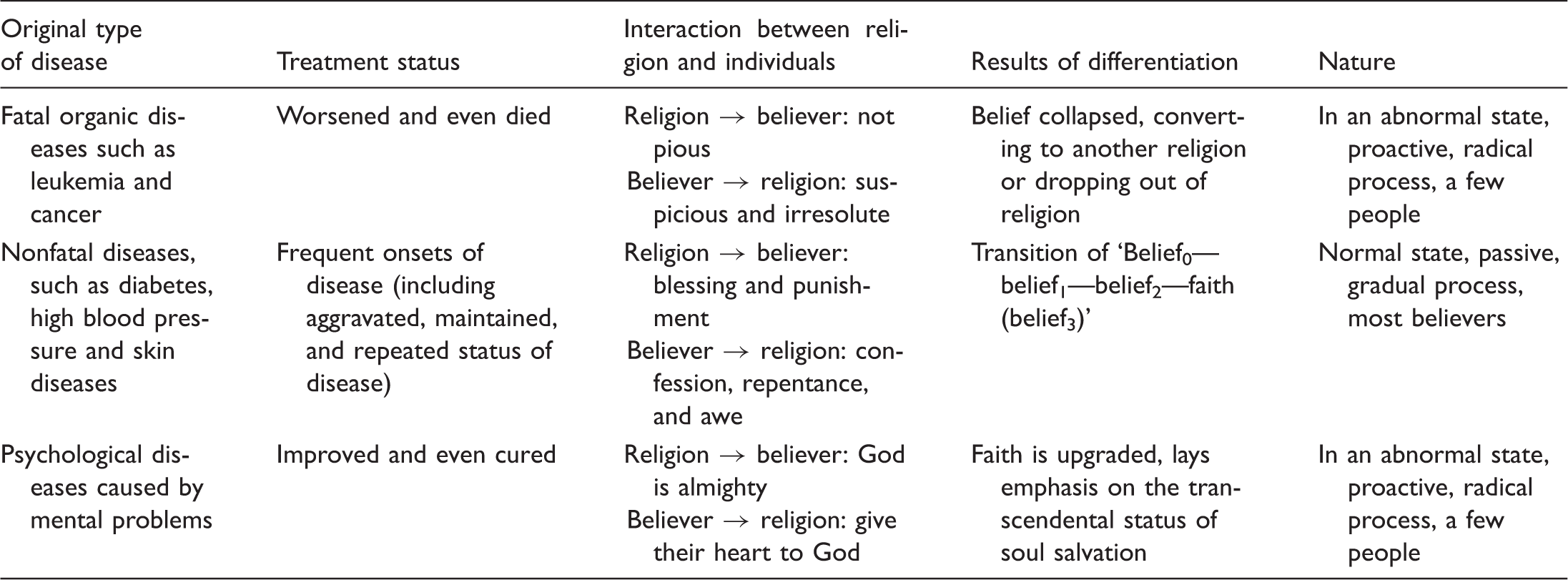
Among church attendees who had organic diseases that proved fatal, such as cancer, heart diseases, and leukemia, as in Case 1, except for a very small number of people who were cured and were cited as propaganda prototypes to reflect God’s ability to bring people back from the dead, the health status of most of these people worsened, and many soon died. In the face of some incurable diseases, medical science could do nothing, nor could religion. Before the collapse of belief, the individual’s mental status was like that of most believers, being in the transitional phase on the path from general belief to pure faith. The sudden onset of deterioration or death directly undermined the person’s belief that God was healing the disease. It reflected the nature of proactivity and discontinuity. This collapse led to individuals experiencing doubts in regard to their religion. How did religion respond to their questions? Here, we use the words of church leader L to answer: Can they blame God if they are not cured? They are not devoted to religion, and the Lord will certainly not bless them. As long as you are pious, the disease can be cured.... Why can people’s cancer be cured? It is because they are devoted. (Interview, 23 February 2015)
For church attendees represented by Case 2, with non-fatal organic diseases such as skin diseases, diabetes, headaches, and high blood pressure, the onsets of their attacks are subject to multiple factors such as diet, psychological state, and weather. People with such diseases are characterized by frequent changes and recurrent attacks. The onset of a disease serves as an opportunity to strengthen an individual’s beliefs, which fit the belief experiences of individuals by religion. Investigation has shown that, in believers’ opinions, the improvement of the health condition is ‘a blessing from God’ resulting from finding the right sin so that God drove the devil out of them, while deterioration in health is a punishment from God, meaning that they have not been pious enough or have failed to find the right sin, and thus God will not shelter them and the devil might invade them at any time. Compared with the early stages of becoming religious, in the later period, believers frequently participate in religious life (e.g., preaching, Bible reading, and chanting), offer money and other donations, and become voluntary workers. The intervention degree of religious behaviors has greatly increased and the individuals enter the transition stage on the belief path, involving multiple psychological experiences, such as increased confidence in the existence of devils, confidence in God’s ability to drive devils away, and senses of sin, repentance, and awe. They engage in the daily practices within the God–man relationship that involve both instrumentality and divine experiences. As for the stage on the transition path, it varies with each individual and time. In the long run, believers with such diseases (like everyone) will face unavoidable death; however, for them, the process is gradual and slow, during which individuals gradually become integrated into religious life through religious practices. Their belief will not collapse with the arrival of death. On the contrary, even if they die at last, their families will still believe in the Christian religion. As a normal phenomenon, except for a few church attendees, such as those in Cases 1 and 3, who experience belief collapse and faith upgrading, most remain generally at this stage. How to make the majority of believers at this stage abandon their utilitarian motives and pursue pure, sacred experiences has become a core issue for Christian practice in China.
Believers who have improved or even recovered from their diseases, such as the individual in Case 3, generally have mental and psychological diseases. Rural Christianity fills the diseases with meaning and also offers hope for healing, especially giving play to the function of psychological adjustment. For all kinds of mental and psychological illnesses, religious rituals greatly relieve the mental pressure of practitioners. Those whose health condition has improved firmly believe that ‘Almighty God’ has defeated the devil, so they give their hearts to God and become devout Christians. Such believers play the role of witnesses in religious life, that is to say, on Wednesdays and Sundays, they narrate to church attendees the stories of God healing their own diseases and inspire their audiences. In daily life, they try to integrate religious creeds into their own codes of conduct and moral laws, and thus an ‘outside believer’ becomes a devout ‘inside believer.’ 22 At this point, individuals no longer take disease curing as the fundamental goal of their religion. ‘Trusting God and pursuing the truth’ becomes their ultimate ideal, and a quantum leap from mere belief to the faith transition state occurs. However, such individuals make up only a relatively small number, being an abnormal phenomenon.
Conclusions and discussions
Unlike in past studies on the conversion to religion as a possible disease-cure, in this paper, belief was taken as the starting point from which to discuss the religious psychology of individuals and its development. Based on the analysis of religious practices and the differentiation of belief concepts, the general mechanism of psychological evolution in the interaction between individuals and religion has been studied. Although the empirical materials have a strong coloring of Christianity (such as holding high the words of God, paying attention to the understanding of sin, emphasizing the construction of believers’ characters, etc.), we believe that this mechanism can be generalized to some extent. This is not only because there are similar practices in other religions, but also because belief exists as a typical mentality among individuals who are suffering from diseases and are trying to recover from them by seeking religious help. This mentality is unlikely to change in accordance with changes in the distribution of religious systems. Similarly, although the logics of religious beliefs and practices differ in terms of specific contents and extent, the same mechanism also applies to other religions, to some extent. Among them, religious construction incorporates belief into the religious domain 23 through the religious attribution of diseases, emotion related to holiness experiences being embedded into belief experiences, and the requirements of faith promoting the purification and transcendence of individuals’ religious mentalities. Among believers, certain types of diseases and their effects will ultimately affect the developmental trends of beliefs and lead to their differentiation.
In studying the mental processes of individuals converting to religion as a possible disease-cure, we found two rules of alternatively functioning logic. The first is logic determined by actors. This logic reflects the common mindset of individuals seeking relief from difficulties when confronting crises; meanwhile, the expectations of religion held by individuals’ beliefs and family ethics have given the dependence a hint of reluctance. The second rule is the sorptive logic of religion. Enhancing believers’ experiences and dependence on religion through the technological process of belief practice shows the strong controlling power of religion itself. As a product of objectivation,
24
the dependent sorptive logic of religion leads to believers converting to a religion as a possible disease-cure starting to be controlled by the religion. In the interaction between dependence and sorption, the explanation regarding diseases and belief practice that religion provides possesses natural emotional advantages and meaning space. Compared with modern medicine, it pays adequate attention to the emotions involved in the illness experiences of individuals
25
and endows diseases with meaning, offering believers powerful emotional support in the face of diseases. In addition, the group living associated with religion constructs an interdependent and caring relationship network for individuals, which is somewhat helpful for restoring the order in their daily lives that has been disrupted by disease. This point has been perceived by non-believers: When she didn’t go to church before, I saw the aunt [note: the aunt of the interviewee’s child] frown and sigh all day long. She kept worrying about everything... Since she went to the church, regardless of whether her disease was cured or not, she kept visiting it and talking to someone, and she told us what she heard in the church after she came back... Her acquaintances from her church also came to her home frequently and talked with her, sometimes they helped her... I felt her life became normal again. (Interview, 25 July 2014)
First, the perspective of belief fits with the psychological phenomenon of individuals converting to religion because of a crisis or dilemma. It not only helps us make judgments concerning ‘utilitarianism’, but also supports reflection on the emerging hypothesis of ‘rational man’. In the judgment of people holding ideas of utilitarianism and rational man, individuals are simplified as objects in pursuit of maximum profit. This orientation not only neglects the complexity of individuals, but also conceals the space for further understanding the evolution of religious psychology, and the concept of ‘belief’ can help make up for this inadequacy. Meanwhile, the use of the ‘belief’ concept helps us to clarify the psychology of religion and to discern its nature beyond the individual level with its group, contextual, and universal characteristics, and thus to undergo a sociological analysis.
In studying the original psychology of believers using the concept of ‘belief’, we should notice the following points: first, such belief is not necessarily associated with religion; in the face of lifetime dilemmas and crises such as diseases and disasters, belief in the early stages of becoming religious is open and multivariant; one can believe either religion or non-religions (e.g., one figure, object, feng shui or glyphomancy). In other words, belief is not necessarily associated with religion, but is merely an expression of a natural mentality when one confronts crises and pursues outside forces to try to resolve them. As Liang (2005) revealed, peasants in crises are not ‘religion seekers’ as Lofland and Stark stated (1965: 862–872), that is, although undergoing a highly stressful experience, they would be unlikely to resort to religion; instead they generally approach religion as something to try under the encouragement of religious believers’ ‘faith witnessing’ and guided by an external social network; second, taking belief as the psychological starting point does not mean that believing in a religion is equivalent to believing in feng shui, glyphomancy or doctors; the experiences of a majority of believers in the ‘transitional belief’ stage in our field study show that the special nature of religion in absorbing and dealing with individual beliefs is like the ‘self-contained force’ of religion in Durkheim’s sense (cited by Ji, 2009), which is the key to the transformation of individual beliefs; and third, most importantly, the use of belief rather than faith in this paper to re-examine the starting mentality of individuals after converting to religion is not meant to highlight the so-called ‘cultural specificity’ of religious practice in China, nor to replace the core position of the ‘faith’ concept in the discourse of religious studies, nor to downgrade peasants’ religious practices. At the level of individuals’ religious experiences, belief in the early stages of becoming religious serves as the starting point for future psychological evolution. Once one adopts religious practices, this kind of psychology enters the dynamic pedigree of the God–man relationship and sacredness construction and then the follow-up of belief differentiation and even sublimation of belief; in this sense, it can be said that the belief perspective has deepened the understanding of the complexity of faith patterns. 26
Second, the concept of ‘belief’ is helpful for understanding religious conversion. Empirical research studies show that the peasant’s progression from pursuit of ‘physical peace’ to pursuit of ‘soul salvation’ is a psychological process moving from secular to religious. Religion gradually guides peasants to abandon practical, utilitarian ideas and aims to make pure faith requirements the core of peasants’ religious lives. In this sense, as William James wrote, ‘When we say conversion of a person, we mean that the religious concept originally on the edge of consciousness now occupies a core position, and the religious goal constitutes the habitual center of the believer's ability’ (James, 2012: 119). It is an experience in which ‘higher emotion actively drives the lower out’, that is, ‘the subconscious ripening of one affection and exhaustion of the other’ (James, 2012: 157). On this basis, we believe that this study will start from the intrinsic psychology to promote the study of religious conversion in Chinese society. Most of the existing studies focus on the external mechanisms and motivations that encourage the conversion of believers, but fail to pay enough attention to the inner psychological experience and its evolution. For example, Lu (2008) revealed the mechanism of Christian cultivation through the research seminars, assemblies, and enrollments of the I-Kuan Tao in Taiwan province, and believed that this approach fits the environment of multi-god worship in Chinese society; Lin (2003) found that ‘belief conversion media’ such as Qigong, Zen sitting, and meditation play an important role in the process of conversion, after studying the emerging religious groups in Taiwan; Liang (2006) and Fan (2011) emphasized the importance of miracles, doctrines, and rituals. This paper takes belief as the core entity in studying the psychological development in the interaction between individuals and religions, focusing on the development’s starting point, evolution, and final trend. On the issue of specific conversion mechanisms, it considers the interaction of ‘dependence and sorption’ between individuals and religion to be the most important mechanism. This study provides a somewhat different interpretation of religious conversion in Chinese society.
Finally, we examine the enlightenment of belief in the revival of religion in rural China from a macro perspective. Peasants converting to religions in the face of life crises are undoubtedly the most important and chief driver of the revival of religion in rural China. In previous empirical studies, religious revival was attributed to a variety of factors, such as spiritual emptiness, the failure of local organizations, the rebuilding of temples, loosened state control, and increased social risks. Liang (2015) summarized these explanations under three headings: ‘invention of traditions’; ‘state–society relations’; and ‘religious market theory’. Stating that we should avoid the three explanations above that relate religious problems in rural society to political or economic issues, he further maintained that religious revival should be regarded as a kind of self-contained fact, a basic condition for human beings. We agree with this judgment and believe that the belief perspective will, to some extent, inspire understanding of such self-contained facts. Without doubt, we do not deny that the specific structural factors such as politics or economics underlie the phenomenon of rural religious revival. Concerning farmers’ conversion to religion as a possible cure for disease as discussed in this paper, the lack and high cost of medical care in rural areas, the limitations of modern medical technology, and the tension between doctors and patients are all external factors that promote peasants’ conversions to religion. However, paying attention only to the issues above seemingly provides a persuasive structural explanation; in essence, we have ignored the more general mechanism of the natural mentality of human beings. It is known that regardless of any political or economic conditions or type of society (traditional or modern) in which individuals are living, there is always a crisis that cannot be solved by conventional channels. The individuals facing dilemmas and difficulties try to free themselves from their predicaments and must resort to getting external help (religious or non-religious) and develop expectations of their sources of help. At the same time, they also receive care from their families. This is undoubtedly human nature. Therefore, we believe that as long as there are problems that cannot easily be solved through conventional channels and the political and social environment for religion conversion continues to exist, peasants will seek help from religion in order to free themselves from difficulties and safeguard their families. The reasons for the religious revival are undoubtedly complicated. This paper aims to provide a new path to understanding, and undoubtedly, it is a natural mechanism.
Any concepts and theories have their specific interpretation boundaries and limitations. The explanation mechanism in this paper starting from belief applies to the group of people who believe in religion due to life crises or dilemmas, and this is the normal state of religious practice in rural China. Meanwhile, what needs to be explained is that religious psychology is a complex subjective experience, that any kinds of induction will inevitably lead to reductionism, and how to further understand this remains to be studied.
Footnotes
Acknowledgments
The authors would like to express their heartiest gratitude to certain teachers and friends, including Yi Wu, Hong’en Xiao, Qi Chen, Dandan Zheng, Sutong Ouyang, Chengbin Liu, and Feng Li, for their assistance in writing and revising this paper. The authors would also like to thank the anonymous peer reviewers of the Chinese Journal of Sociology for their helpful comments for revision of this paper.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors take sole responsibility for their views.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Graduates’ Innovation Fund of Huazhong University of Science and Technology under the title ‘The Relationship Between Disease and Religion in Rural Society’ (Grant Number: 3007404102), and the Independent Innovation Fund of Huazhong University of Science and Technology under the title ‘The Social Basis of Rural Religious Governance in the New Era’ (Grant Number: 2019kfyXJJS108).