
Abstract
The Study was done to examine the use, non-use, the quality of clinical advice, challenges in acquiring AFOs (Ankle Foot Orthosis), and user satisfaction, using a WHO based Rapid Assistive Technology Assessment (rATA) and Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST) questionnaire. The cohort (n = 100) consisted mainly of males (71%) and residents of city (82%). It was found that 98 subjects were under advice from healthcare providers to use an AFO but only 59 subjects were using AFO at present. Common complaints were pain, fitting related and social stigma among users. The majority of the subjects (87%) paid for their AFOs. It was found that the majority of the subjects were “more or less satisfied” with the device however 59% strongly agree that they dislike the appearance of their AFO and 37% were completely dissatisfied with the accessibility of their home and surroundings while using the AFO. It is evident that we should work on improving the design and fit of the orthosis so that the acceptance and satisfaction improves. This study also explores the possibility of usage of rATA for the specific assistive Technology (like AFO in this context) assessment. It was observed that patients often have high expectations regarding a cure with the use of an AFO. Therefore, it is essential for service providers to explain that the AFO is intended to improve function rather than provider a cure. This mismatch of understanding may contribute to dissatisfaction by patients using AFOs, hence user education is essential along with technology provision.
Introduction
Orthotic management is a useful and significant treatment option for a number of conditions that affect gait, posture and forms a part of an overall rehabilitation program for patients with Cerebral Palsy, Stroke or Spinal Cord Injury.1–3 These devices can be categorized into three anatomical types: spinal orthoses, upper limb orthoses, and lower limb orthoses. There are various kinds of orthoses for lower limb such as foot orthotics (FO), ankle foot orthoses (AFO), knee- ankle foot orthosis (KAFO), and hip-knee ankle foot orthosis (HKAFO). 4
Ankle- foot orthoses are used to address problems related to the foot and ankle that are either biomechanical or neurophysiologic in nature. An AFO is applied to the lower limb to improve the gait limitations of patients as it has a beneficial effect on mobility, balance, gait and reduces fall risks.2,5 An AFO includes the ankle joint as well as all or part of the foot and serves to regulate motion, correct deformities, and/or compensate for weakness. 6 There are many types of AFOs and they can be manufactured using various materials involving metals, plastic or carbon fiber. 4
Several studies in the literature indicate a high level of dissatisfaction or low acceptability rates of lower limb orthoses. A study examined the use, nonuse, satisfaction, and dissatisfaction among 211 AFO users, finding that 1 in 15 AFOs was not used at all. About three-quarters of the AFO users were satisfied, while one- quarter were dissatisfied with the device in the Netherlands. 7 Another study involving 17 AFO users reported that most users felt comfortable walking on even surfaces, but they experienced difficulties with donning/ doffing, climbing stairs, and performing certain routine activities. 8 Study investigated user satisfaction with orthoses in Taiwan and found that participants with mild disabilities who had been using the orthosis for less than a year were the most satisfied with their devices and the services. 9 However, the satisfaction score for orthotic services was lower than that for the devices themselves. 9 A study reported pain associated with the use of the device and difficulties in walking on challenging surfaces as important reasons for dissatisfaction in their study. 10 However, these studies were all limited in scope, either by focusing on specific types of AFOs or evaluating only a few aspects of daily life (e.g., fitting, pain, fatigue or falls). Limited studies are done in India to examine the satisfaction and expectations of AFO users. The lack of credible evidence regarding individuals’ experiences of AFO indicates a need for further work. User satisfaction is an important outcome in evidence-based and patient centred practice. Therefore, the aim of the study is to assess user satisfaction with AFOs and related services in India, and to identify the outcomes and features users wants.
Materials and methods
Ethical approval and informed consent
The present study was conducted according to the Declaration of Helsinki. Ethical Clearance was received from the Institute Ethics Committee (IEC-649/06.10.2023), at AIIMS, Delhi. The trained staff explained the study to each participant using the patient information sheet (PIS) and a signed informed consent form was obtained from all participants. For those aged below 18, a consent form was obtained from their caregivers.
Sample size
Total 100 participants were enrolled at the PMR department of tertiary care hospital setting via convenience sampling. Inclusion criteria for enrolling the participants were- individuals who were using AFO for greater than 3 months, individuals who were prescribed AFO but may or may not be using the same due to any reason, parents/guardians of children using AFO below 18 years of age and relevant caregivers involved in their care of elderly patients or PWD (persons with Disability) using AFO with communication difficulties. Participants who were, critically ill, not willing to participate or unable to understand Hindi or English language were excluded from the study.
Tools and techniques
rATA
The WHO rATA (Rapid Assistive Technology Assessment) scale was used to gauge user satisfaction, which reflects perceptions of service quality, the physical characteristics of the product, client needs, and alignment with clients’ priorities and aspirations. It uses a Likert scale to measure satisfaction indicators with assistive technology (AT), such as: appearance, weight, durability, effectiveness, ease of use, comfort, safety, assessment and training, and maintenance and environmental limitations. 11 There are no studies done on its use for assessment of specific device (like AFO as in current study) and is used as a general assistive technology assessment tool.
QUEST
Quebec Evaluation of Satisfaction with Assistive Technology (QUEST) is a standardized scale consisting of 12 items that identify user’s satisfaction with assistive technology and services. Eight items focus on satisfaction with assistive devices (including dimensions, weight, ease of adjustment, safety, durability, simplicity of use, comfort, and effectiveness), while four items address service delivery (service-delivery program, repairs and servicing, quality of professional services, and follow-up services). QUEST employs a five-level response scale: (1) Not satisfied at all; (2) Not very satisfied; (3) More or less satisfied; (4) Quite satisfied; and (5) Very satisfied. QUEST has been proven to be a valid and reliable assessment tool. 12
Additional questions
A combination of other relevant questions were also formulated and compiled to analyze various components such as user satisfaction, use and non-use of AFO that are not covered by both the above questionnaires and are necessity for developing countries.
Data analysis
Based on the questionnaire, the data were entered into excel sheet for further analysis. The statistical analysis involved descriptive analysis of the gathered data.
Results
Patient demographics and characteristics
Demographic characteristics of the participants.

*remaining 50 were not involved in employment and study.
Clinical characteristics of the participants.

N; no of respondents, * We still included the 2% subjects as they had the past experience of using AFO 2 years ago.
In our study, 89 participants were under the age of 18, of which 21 were below 5 years, and 68 were aged between 5 and 18 years. Among the 5-18 years old participants, 46 were actively pursuing education, while 22 were non-literate. Notably, 33% of the participants were receiving education from school and colleges, and 13% were engaged in home- based learning. The Majority of participants, spanning the ages of 5 to 28 years, were involved in education activities, either from home or otherwise.
Overall, 50% of the subjects were engaged in either education or employment. Of those, 13 were engaged in studying or working from home, while 37 were doing so outside the home. Modes of commuting among participants varied, with 16% commute by walking, 10% using public transport, and 12% relying on private transportation. The use of AFOs reportedly improves commuting for some (15%), reduces it for a few (3%), and has no impact for others (20%).
The majority of visits were for follow-up on their AFO’s (60%) and ongoing illness treatment (35%). The majority of the participants were diagnosed with Cerebral Palsy (n = 46). It was noted that 98 subjects were under advice from healthcare providers to use an AFO; but only 59 subjects were using AFO at present. Most subjects use plastic AFOs (58%), with some using night splints (22%) or both (19%) (Table 2).
The most common indications for using AFO and diagnosis of the AFO user is given in Figures 1 and 2. Showing the most common indications for using AFO (N = 100). Diagnosis (N = 100).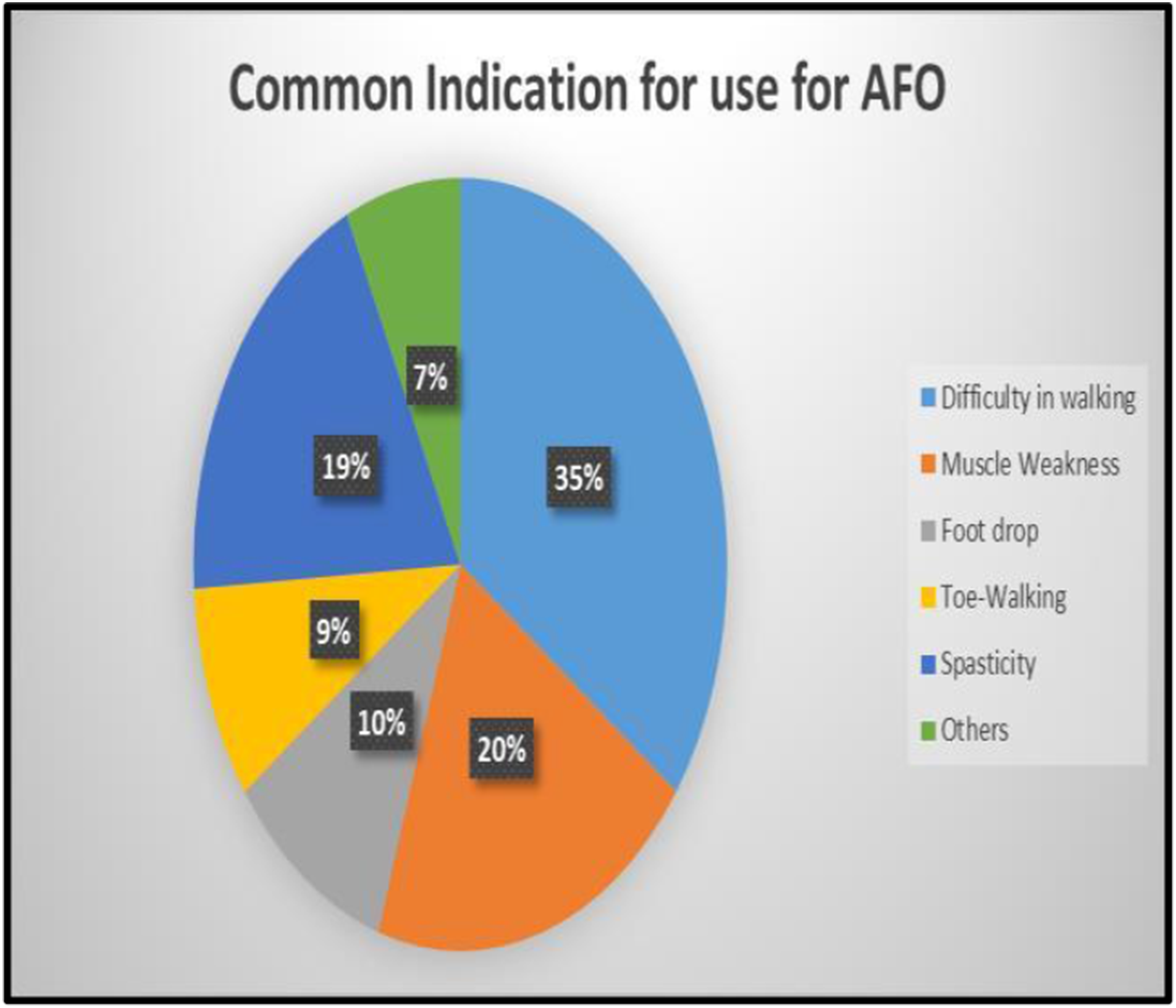

Common indicators identified by AFO users as seen in Figure 1 are as follows: Difficulty in walking 35%, muscle weakness and spasticity was (20%) and (19%) respectively, very few indicated that foot drop (10%), Toe- walking (9%), others (7%) were the reasons to use AFO.
The most common diagnosis seen in participants were cerebral palsy (46%), followed by others were (34%), growth development delay (14%), spina bifida (6%) in Figure 2.
Health-seeking behaviours
Subjects sought clinical advice from various health care providers before receiving their first AFO prescription; the majority 41% from four healthcare providers, 33% from three providers. The majority of final prescriptions were from Physiatrists (68.69%). All participants were thoroughly counselled by the prescriber before beginning the use of AFOs. Of these, 29.90% strongly agreed that the counselling was adequate, 55.67% agreed, and 14.43% expressed disagreement. Despite this, every participant acknowledged that the prescriber clearly explained both the benefits and potential risks associated with using AFOs, ensuring they were well-informed before proceeding with the treatment.
Quality of clinical advice given by the prescribers
Participants from both the public (85%) and the private sector (15%) received sufficient guidance from the prescriber regarding AFO usage, including benefits of use and potential risks associated with non- use. The majority (85 %) of the participants were satisfied with the clinical advice given by the prescribers. Additionally, they were well informed about repair and customization options.
Challenges in acquiring AFO
The majority of subjects 96% procured AFOs through referrals from prescribers. Users received adequate information about their AFO providers and typically contacted them within an average of 2 days. Upon ordering, the mean waiting time was 19 days to receive their AFOs, often requiring minimal or no additional modifications.
AFO procurement process
Subjects at the tertiary hospital were referred to the Physical Medicine and Rehabilitation (PMR) department either directly or through other specialties like pediatrics, neurology, and orthopedics. Out of the present sample of the subjects, 71% procured AFOs from Government organizations, 24% from private sources and rest from NGOs (Non Government organizations) (refer Figure 3 for details). A significant variation was found in the price of AFOs charged from the subjects, ranging from 50 INR to 10,000 INR, with an average of 1025 INR. Since the hospital where the study was conducted has its own Prosthetic and Orthotic Workshop under the PMR therefore most of the users were having custom Built AFOs made in hospital workshop only . Showing sources of users first AFO Procurement.
Figure 3 is a pie chart showing that majority (71%) of the users procure there AFO from Government organization, 24% from private, 4% from NGOs and 1% indicate from others.
Challenges with AFO use
Top challenges among users who stopped using AFO completely, before the recommended duration (N = 44).

AFO and social acceptance
A significant portion, 59% strongly agree that they dislike the appearance of their AFO and that it resembles a disability device, which impacts their usage. While 30% of respondents agree, though less strongly, that the appearance and association with disability limits their use of the AFO, indicating some concern over its design and a smaller group, 11%, disagrees with these sentiments, suggesting that a minority do not find the look and feel of the AFO as a limiting factor. Detailed information is provided in Figure 4. AFO and perceived social acceptance.
Figure 4 is a bar graph blue colour indicated “I don’t like the look and feel of my AFO” and orange colour indicated that “AFO look like a disability device”. Majority (59%) of the users find their AFO look like a disability device, 30% were agree with the statement and only 11% were disagree with the statement, none of the users were strongly disagree.
Satisfaction with AFO and its related services using QUEST
Satisfaction with AFO and its related services using QUEST (N = 100).

AFO and its related services assessment based on WHO rATA
The WHO rATA-based questionnaire was used to access areas of need with relation to AFO as assistive technology. Subjects were asked various questions, and most reported neutral levels of satisfaction with their Ankle-Foot Orthoses (AFOs), feeling neither satisfied nor dissatisfied. The top issues identified were pain or discomfort, concerns with fit, size, or shape, and social stigma or appearance. Despite these concerns, all subjects indicated that they would recommend AFOs to others in need, demonstrating their overall belief in the benefits of the orthoses.
In Figure 5 Pie chart shows the most common reasons among the users for not using AFO. Reasons for not using AFO (N = 100).
AFO and its related services assessment based on WHO rATA (N = 100).

In Figure 6, pie chart is display showing the payer of the AFO, three colours were use grey indicated by self (87%), blue by government (12%) and red indicated by NGO/charity. Payer of the AFO (N = 100).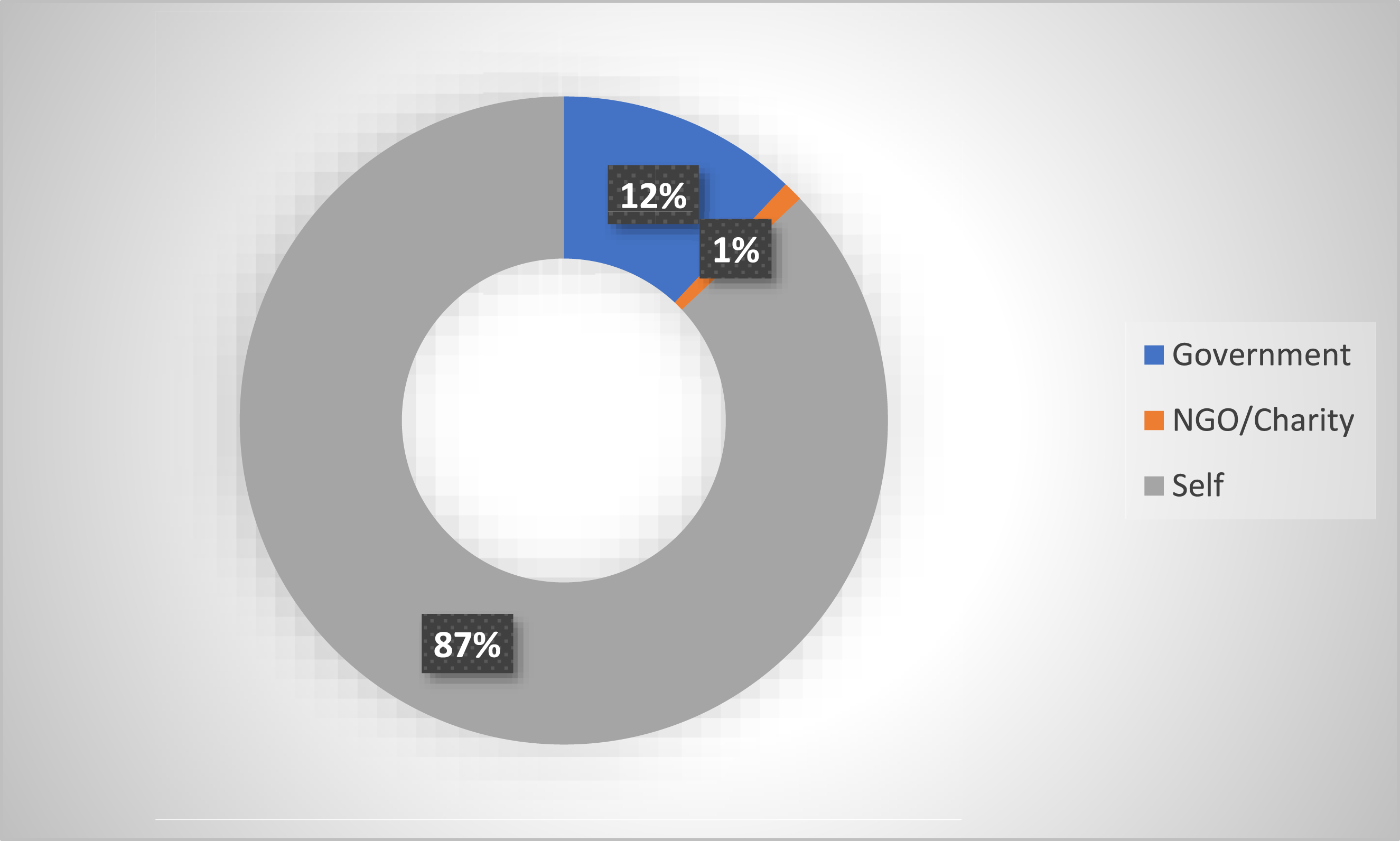
It was found that 87% of subjects paid for their AFOs, with 78% reporting they paid less than 1000 INR for their AFOs in the last 12 months. Also, it is to be noted that the highly subsidised rates are charged in the government setup which are almost 20 times less than the cost to the organisation and 30 times less than the market rates (Figure 6). The degree of satisfaction with AFO accessibility showed 37% of respondents were completely dissatisfied with the accessibility of their home and surrounding, 43% thought it was moderately accessible and 10% regarded it as moderate. When asked for assistance by AFO to the user, 41% stated it was moderately helpful, while 42% reported it didn’t help them much details is given in Figure 7. Level of satisfaction among AFO users.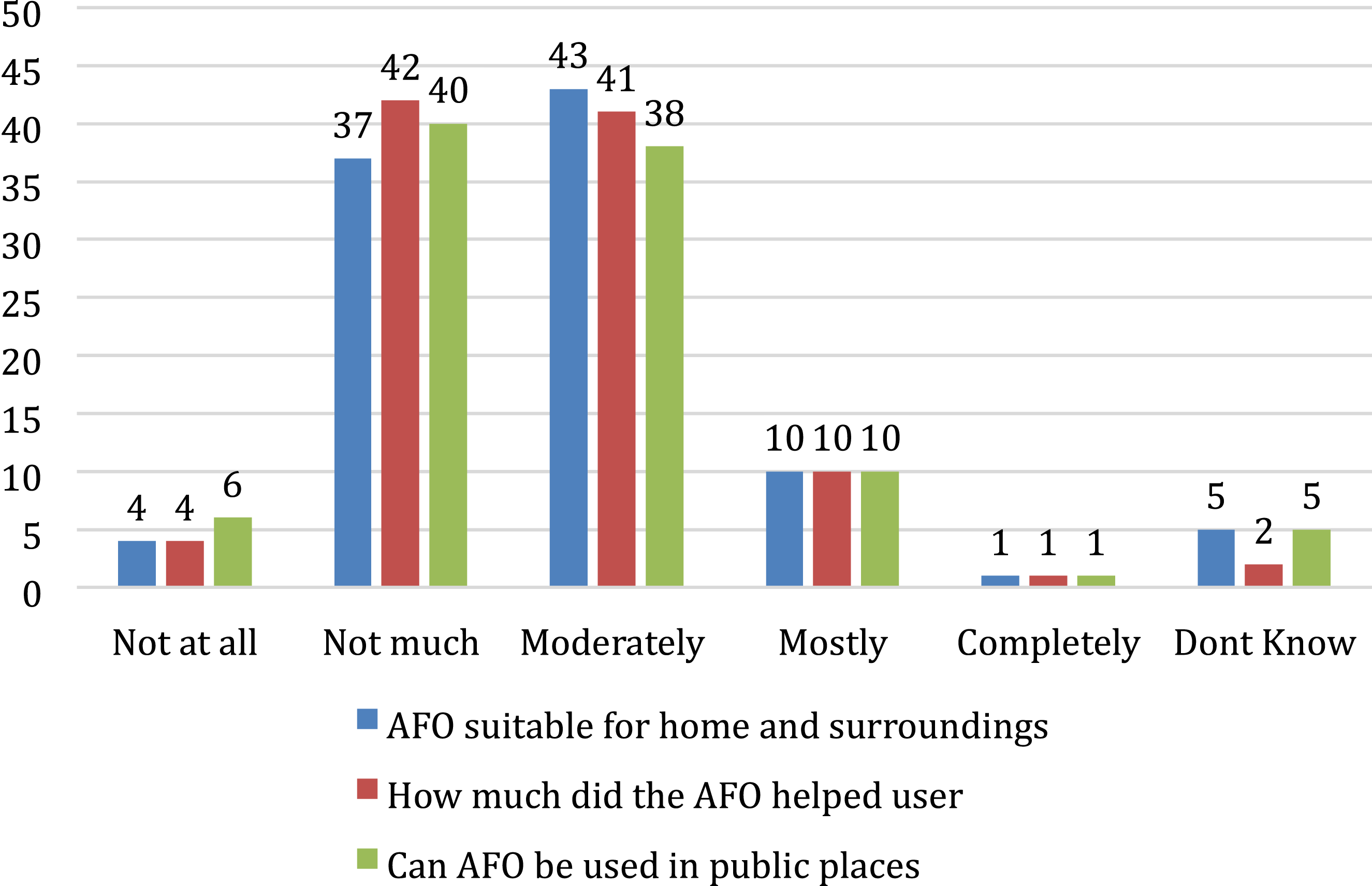
Level of satisfaction among AFO users if given in Figure 7, it’s a bar graph display three colour blue indicate “AFO suitable for home and surrounding”, red indicated “how much did the AFO helped user”, green indicated “can AFO be used in public places.
Expectation from using AFO
Expectations from AFO.

Discussion
The Ankle foot Orthosis is one of the most commonly prescribed orthoses in condition that impact the knee- ankle and foot complex. A broad overview of demographics and clinical data of AFO users in a tertiary care hospital setting, with specific focus on areas of satisfaction and dissatisfaction, is given by this study. The results are concurrent with the existing literature on how AFOs are used in other low-income countries emphasizing a need for a multimodal approach and patient education to optimize outcomes for AFO-users. There was demographic trend of having younger people and urban settings due to early referral from the pediatric department and the urban tertiary care set up however it is evident that there is a large majority of population is underserved due to limited awareness and availability in the rural areas. 13 In our study, Physical Medicine & Rehabilitation (PMR) doctors prescribed most AFOs (68.69%) demonstrating their involvement in understanding the role and effectiveness of AFO in managing these patients. 13
The fact that the patient had to consult 3-4 healthcare providers before they reached a provider that prescribed an AFO highlights the need to increase awareness regarding AFO in the general clinician community. This points toward the need to increase awareness in the community so that persons who can benefit from AFO receive appropriate prescriptions sooner. A mean waiting time of 19 days was observed from measurement to delivery in the procurement process. Only a few subjects reported that minor adjustments were needed, demonstrating how accurate and reliable the fitting process can be. Previous studies show high rates of abandonment due to discomfort and practical issues and the same is revealed in this investigation that orthoses are subject to high rates of non-compliance. Holtkamp et al. and Aftab et al. have also pointed that issues like difficulty in donning/doffing or walking on uneven surfaces did affect the acceptance by the patients.7,8 This not withstanding, there was high satisfaction amongst users, which could suggest that people recognize some advantages of using these devices as they promote mobility as suggested by Author. 10 It can conclude that public hospitals provide essential and sufficient guidance. This comprehensive approach underscores public hospital commitment to patient education and support, ensuring that individuals are equipped with the knowledge needed to effectively manage and maintain their AFOs. However, there is a need for increased awareness and education about AFOs in private hospitals and the health systems at grassroot level to ensure that all patients receive the same level of understanding and care.
However, unlike the studies conducted in developed countries, this study underscores the challenges faced by users in a developing country context, such as limited access to orthotic services and the need for more patient education on AFO use and maintenance. The efficiency of tertiary level hospital services is highlighted by a high level of satisfaction with initial fitting and procurement process although it indicates similar standards should be adopted across other healthcare facilities within India.
The qualitative responses from users highlight crucial areas for improving access to Ankle Foot Orthoses (AFOs) in India, with a focus on pricing, awareness, and accessibility. Many responses emphasised the importance of cost reduction in private set up and also account for travel expenses incurred during multiple visits for getting customised AFO at government facility where it is highly subsidised, implying that local manufacture and distribution could help to alleviate these concerns. There is also a considerable need for healthcare professionals and the general public to become more aware about AFOs and their benefits. Furthermore, respondents stated a need for speedier procurement processes, better aesthetic and functional design, and increased durability in order to boost user satisfaction and compliance. The high user expectation that the AFO will cure the underlying condition may be a contributory factor for less satisfaction in long term.
It is important to note that the study has a number of limitations. The study was limited to one institution which may have affected the wider understanding regarding the usage in other regions in India especially at the rural setup. In future, we can do a multicentric evaluation of several centers for this purpose to obtain full understanding of AFO use among patients who are managed in different locations. We used rATA-based questionnaire but had to add few more questions to get a clearer picture of user satisfaction with the AT provision A prospective study would allow better information by collecting data through longitudinal studies on AFO use or AFO-related outcomes.
Conclusion
This study helps in assessing Patient’s use and Satisfaction with Ankle Foot Orthoses and Service in a tertiary care hospital in India. It is evident that we should work on improving the design and fit of the orthosis so that the acceptance and satisfaction improves while keeping cost in control. Further, service delivery, patient education and awareness amongst the service providers are the areas we need to work on in future.
Footnotes
Acknowledgment
This paper was made under the guidance and support of experts and colleagues at the National Center for Assistive Health Technology (NCAHT), All India Institute of Medical Sciences (AIIMS), and the Indian Council of Medical Research (ICMR), New Delhi, India.
Funding
This work was supported by the Indian Council of Medical Research, New Delhi, India under its project National Center for Assistive Health Technology (NCAHT), All India Institute of Medical Sciences, New Delhi (02/WHOCC/ADR/2019-NCD-II dated 18 /02/2022).
Declaration of conflicting interests
The authors declare no conflict of interest.