
Abstract
Introduction
This study aimed to explore the relationship between training volume during 4 weeks of robot-assisted arm training (RAAT) and changes in arm-and hand function, grip strength, gross motor skills, spasticity, and daily activities.
Methods
Twenty participants, >18 years of age, in subacute phase following stroke, with impaired arm function admitted to Sunnaas Rehabilitation Hospital, completed 4 weeks robot-assisted arm training (45 min, 3-5 times a week). Before and after this intervention, the participants’ arm and hand function, grip strength, gross motor dexterity, spasticity and activities of daily living were assessed.
Results
The key findings of this study indicated no association between training volume and improvements in arm and hand function, grip strength, gross motor dexterity, spasticity, or activities of daily living. Also, no significant associations between changes in arm and hand function and age, gender, or affected side. However, subgroup analysis showed significant improvements in arm-hand function for participants with shorter time post-stroke (p = 0.01) and better initial arm and hand function (p < 0.0001).
Conclusion
These findings highlight the importance of early initiation and individualized treatment based on initial function when using robot-assisted arm training in stroke survivors.
Introduction
Stroke is a leading cause of disability worldwide, affecting approximately 12.2 million people annually 1 . The increasing prevalence of stroke is attributed to an aging population and a rise in lifestyle-related risk factors. 2 One of the most prevalent consequences of stroke is motor impairment, which affects nearly 80% of survivors. 3 This impairment often results in diminished muscle control and movement, typically affecting one side of the body and leading to upper limb dysfunction. 3
Upper limb impairment is considered one of the most burdensome consequences of stroke by survivors 4 and has been identified as a key research priority. 5 The ability to use one’s arms and hands is crucial for independence, engagement in meaningful activities, 6 workforce participation, 7 and overall quality of life. 8 Consequently, effective rehabilitation strategies for restoring upper limb function are essential not only for individuals but also for broader societal and economic benefits. As stroke incidence continues to rise,2,9 the demand for rehabilitation interventions targeting upper limb recovery is increasing.
Current rehabilitation approaches for upper limb function primarily involve individualized motor training sessions, typically administered with manual guidance from a therapist. 10 However, this method is resource-intensive, requiring significant personnel, time, and financial investment. 10 Given the growing challenges in healthcare, including workforce shortages 11 there is an urgent need for innovative solutions that optimize resource utilization while maintaining high-quality treatment outcomes. 11 Advances in robotics and technology offer promising alternatives, enabling one therapist to oversee multiple patients simultaneously, thereby reducing resource demands.12,13
Emerging evidence suggests that robotic-assisted arm training (RAAT) is more effective than conventional therapy in improving important outcome measures in stroke rehabilitation, such as muscle strength, 14 spasticity,14,15 activities of daily living 15 and upper extremity performance (ARAT) 15 The Norwegian clinical guideline is now also recommending RAAT as an intervention in upper limb rehabilitation. 16 Moreover, RAAT enables the treatment of a larger number of patients while requiring fewer resources, making it a viable solution for addressing future healthcare challenges.12,13 By enhancing efficiency without compromising treatment quality, RAAT presents a promising approach to stroke rehabilitation. 13
However, despite growing knowledge in this field, there is still limited understanding of the factors influencing RAAT effectiveness. Recent efforts to develop Norwegian clinical guidelines for RAAT 16 highlight the need for further research into variables such as robotic device type, patient demographics, stroke-related characteristics, and training volume to optimize rehabilitation outcomes.
Objectives
The aim of this study was to investigate the relationship between training volume and changes in arm and hand function, grip strength, gross motor dexterity, spasticity, and activities of daily living, after 4 weeks of RAAT.
Methods
Study design
This longitudinal, exploratory observational study is based on data retrospectively collected from another study, the ARIS study, that resulted in a clinical guideline for the use of robotics in rehabilitating hand and arm function in stroke survivors in Norway. 16 In the ARIS study, participants’ experiences from a robot-assisted arm intervention were examined. All participants were asked to also participate in the current study. After the ARIS study 16 was completed, the baseline and the post results were collected for data analysis in the current study. Informed written consent was obtained for all participants prior to inclusion.
Participants
The participants were recruited at Sunnaas Rehabilitation Hospital, Norway from June 2022 to June 2023. Individuals >18 years in subacute phase following stroke, with impaired arm function (ARAT ≤ 51) admitted to Sunnaas Rehabilitation Hospital for a 4 weeks in-patient rehabilitation period, were invited to participate. Type of stroke (ischemic/hemorrhagic) and the location of the lesion has not been taken into account as a criterion. Participants who had severe cognitive impairments, language difficulties, contractures, or poor sitting balance were excluded. Inclusion and exclusion criteria were evaluated by a medical doctor, based on the participants’ medical history and clinical assessments.
Procedures
The participants’ arm and hand function and their ADL performance were assessed before and after the intervention period by occupational therapists (OT’s). Injury characteristics were collected from the patient’s medical record.
The intervention consisted of robot assisted arm training for 45 min, 3-5 times a week, for 4 weeks. The training was conducted using the robotic devices Armeo®Spring (Hocoma, Switzerland) and/or Amadeo® (Tyromotion, Australia). Specially trained healthcare professionals selected and customized robotic devices and games to match each participant’s functional abilities and training goals, adjusting the difficulty level throughout the period for optimal adaptation and progression while also recording the participants’ exercise training log.
Robotic devices
Armeo®Spring (Hocoma, Volketswil, Switzerland) (Figure 1(b)) is an exoskeleton that consists of a robotic arm with three separate joints (wrist, elbow, shoulder) and six degrees of freedom that can be attached to the upper extremity.
17
It features task-oriented games and movement exercises with varying difficulty levels, with real-time auditory and visual feedback.
18
The exoskeleton offers tailored support by unloading the weight of the arm and enabling performance of a large range of 3-dimensional movements,
18
This device is designed as a passive exoskeleton without motorized assistance. Users must actively move their arms to guide the exoskeleton’s movement. This necessitates some active upper limb function. (a) Amadeo®. (b) Armeo®Spring.
Amadeo® (Tyromotion, Gratz, Austria) (Figure 1(a)) is a robotic device for training of hand and finger functions. 20 The hand is positioned using a fastening strap that secures the wrist, 20 while magnets are attached to the fingers and connected to motion-driven units. 21 The robotic device facilitates intensive, repetitive training of both flexion and extension movements of one or multiple fingers. The patient receives real-time visual feedback on a computer screen. 20 The training can be customized using passive, active, or active-assisted support during the exercises. 22 As a result, this device can also be used by patients without an active hand and finger function, i.e. all participants included in this study.
Outcome measures
Action research arm test
The primary outcome was upper limb function, assessed by the Action Research Arm Test (ARAT). 23 ARAT includes 19 tasks in four categories: grasp, grip, pinch, and gross motor movement, each rated from 0 to 3, and summed (0–57 points), with higher scores indicating better function. 24 ARAT has shown high validity 25 and strong reliability.26,27 The minimal clinically important difference (MCID) has been reported to be 5.7-points for chronic stroke patients 26 and 12–17 points for acute patients. 28 MCID for subacute patients has not been established, therefore, an MCID of 5.7 points was chosen in the current study. For participants to possibly reach MCID, the inclusion criteria were set at an ARAT score of ≤51 points. Results are presented as ‘ARAT pre-test’, ‘ARAT posttest’ and as change in ARAT score from pre-to posttest, that is ‘ARAT Δ’.
Secondary outcomes
Box & Block Test
Gross manual dexterity was assessed with Box & Block Test (BBT) (Richardson, USA). BBT is a standardized test consisting of a rectangular box with 150 cube-shaped blocks (2.5 cm) and a divider separating the box into two sections. 29 The total blocks transferred from one section to another in 1 min was recorded and compared to gender, age and dominant hand specific normative data. 29 The BBT demonstrates strong validity 25 and reliability.25,30 The MCID for patients in both acute and chronic phase post-stroke is six blocks. 30
Jamar dynamometer
Isometric grip strength was measured with the Jamar® dynamometer (JD) (Fabrication Enterprises, White Plains, USA). Three measurements were taken for each hand, 31 and the mean of these three measurements was computed in kilograms (kg). The results were compared to reference values for age, gender, and the hand used. 32 Dynamometer measurements show strong validity 33 and reliability.33,34 For both patients in acute and subacute phases post-stroke, the MCID is 6.2 kg for the non-dominant hand and 5.0 kg for the dominant hand.28,35
Barthel ADL index
Activities of daily living (ADL) were assessed with Barthel ADL Index (BI), an assessment tool for evaluating independence in various activities of daily living (ADL). 36 It records the need for assistance across 10 domains, documenting levels of independence in basic daily activities, with a range 0–100 points, where a higher score indicates better function. 36 In this study, the Norwegian version was used. 37 The BI shows high validity 38 and reliability.39,40 The MCID for patients in the acute phase post-stroke is 9.25 points when using the 0–100 scoring range. 41
Modified Ashworth Scale (MAS)
Spasticity in elbow, wrist and finger flexors was assessed using the Modified Ashworth Scale (MAS), a tool for quantifying muscle spasticity. 42 The test is conducted by moving the joint being evaluated from its starting position to its endpoint within one second. 42 The scale consists of six levels (0, 1, 1 +, 2, 3, 4), where ‘0’ indicates no increase in muscle tone and ‘4’ indicates rigidity that significantly restricts joint movement. In this study, the approach by Chen et al. (2019) is used, where spasticity (MAS) in elbow, wrist, and finger flexors forms a spasticity index based on the average of these three measurements. 43
Reliability varies by joint; for elbow flexors, test-retest reliability in those with CNS injuries is good, 44 with high intra- and inter-rater reliability for elbow, wrist, and finger flexors. 43 The method shows strong construct validity 45 and the MCID is 0.48. 43
Statistical analysis
The data in this study were analyzed using the Statistical Package for the Social Sciences (SPSS), version 29.0.0.0. The descriptive results were reported as medians and interquartile ranges (Q1–Q3) when the data appeared to be skewed. Normally distributed data was presented using means and standard deviations (SD). The relationship between training volume and both ARAT Δ and secondary outcome measures, as well as between the ARAT Δ and demographic and disease-related factors was examined using Spearman’s Rho. A correlation coefficient between 0 and 0.5 was considered low, 0.5–0.7 as moderate, and 0.7–1 as high. 46 A Wilcoxon signed rank test was used to analyze the difference between ARAT pretest and posttest, while the Spearman’s Rho test was used to analyze the correlation between these two variables. Subgroup analysis on the change in ARAT score from pre- to posttest were performed for participants with a pretest ARAT score below versus over median using a Mann-Whitney U test. The significance level in this study was set at p < 0.05.
Results
Participants, demographics and disease-related factors
A total of 29 individuals were invited, and 24 agreed to participate. After screening, three were excluded due to an ARAT sum score >51. Of the 21 included, one withdrew because of medical complications (unrelated to the study). Data from 20 participants (15 males/5 females) were analyzed (Figure 2). Flowchart of the study recruitment process.
Participants (n = 20) demographics and disease-related variables, presented in median (min-max).
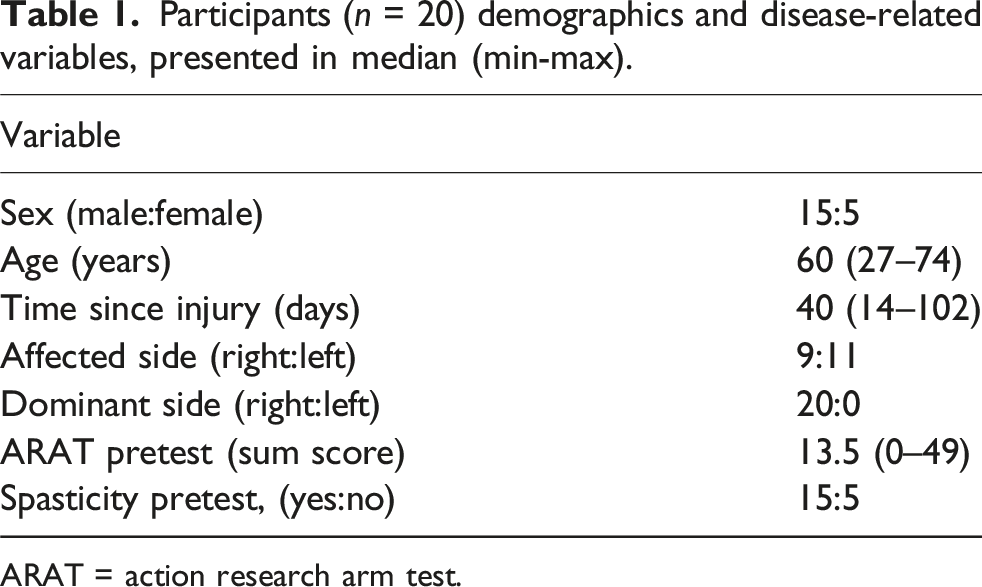
ARAT = action research arm test.
Descriptive analysis of the intervention
All participants completed 4 weeks of training. The average number of planned training sessions was 17.8 (SD = 1.9) over the 4-week period, resulting in an average of 4.5 planned sessions per week. The participants completed an average of 3.95 (SD = 0.8) sessions per week, that is 88% (SD = 13) of the planned sessions were completed. The number of sessions varied from 2.25 to five per week. During the intervention period, the average total active training time (without installing (don) removing (doff) equipment was 503 min (SD = 166) per participant, ranging from 223 to 754 min, which equals 31.4 min per session (SD = 6.1). Three participants used the Amadeo® arm robot, seven used Armeo®Spring, while 10 participants used both robotic devices.
Descriptive analysis of the outcome measures
Overview of the outcome measures during pre- and posttest results (including change scores), presented as median and interquartile ranges (Q1–Q3).

ARAT: action research arm test; MAS: modified ashworth scale; BI: barthel ADL index; BBT: box & block test.
Approvement (MCID in arm and hand function (ARAT) and gross motor dexterity (BBT) was achieved by 10 out of 20 participants. For grip strength (JD), four out of 20 participants reached MCID. The spasticity index decreased in five participants, increased in 4, and remained unchanged in the remaining 11. A clinically important difference (MCID) in activities of daily living (BI) was observed in 13 out of 20 participants.
Association between training volume and changes in arm and hand function
Association (spearman’s rho) between changes in arm and hand function (ARAT Δ) and training volume (training frequency, session duration, and total active training time.
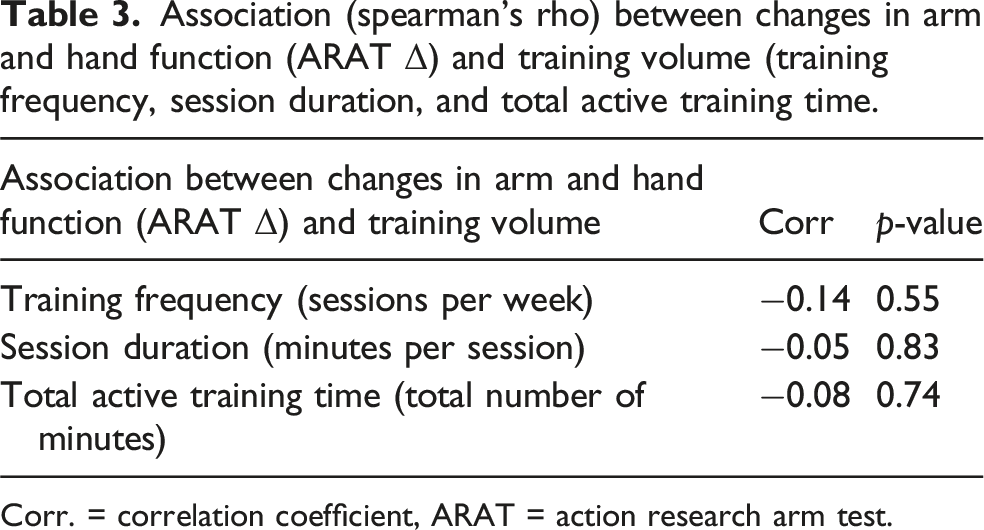
Corr. = correlation coefficient, ARAT = action research arm test.
Association between training volume and changes in spasticity, gross motor dexterity, grip strength, and ADL
Analyses (spearman’s rho) of the associations between training volume and changes (

Corr. = correlation coefficient, JD = Jamar dynamometer, BBT = box & block test, BI = Barthel ADL-index, MAS = modified Ashworth scale.
Associations between demographic and disease-related factors and changes in arm and hand function
Analyses (spearman’s rho) of the associations between changes in arm and hand function (ARAT change score) and age, time since injury, ARAT pretest, sex, and affected side.

Corr. = correlation coefficient, ARAT = action research arm test.

Scatterplot of the association between changes in arm and hand function (ARAT change score) and time since injury.
Arm and hand function before and after intervention
The scatter plot illustrated in Figure 4 shows the relationship between ARAT scores at pretest and posttest for the affected side, with a diagonal identity line added. The figure indicates that participants with a low ARAT pretest score show little or no change to posttest. In contrast, participants with better arm and hand function at pretest appear to demonstrate greater changes in ARAT scores at posttest. Wilcoxon signed rank-test showed a statistically significant difference (5.5 points, p = 0.003) between ARAT pretest and ARAT posttest scores. Spearman’s Rho indicated a strong correlation (r = 0.9) between ARAT pre- and posttest scores. The relationship between arm and hand function (ARAT) at pretest and posttest. Abbreviations: ARAT = action research arm test. AThree participants had an ARAT score of ‘0’ during both pre- and posttest.
Initial arm and hand function – subgroup analysis
As participants with better arm and hand function scores at admission appeared to experience greater improvements at discharge, an additional analysis was conducted. This analysis revealed that those with an ARAT score above the median admission score (<13.5) demonstrated significantly greater improvements (2.7 vs 13.6 points, p < 0.001) compared to those below.
Discussion
Current findings
The main findings of the study were that individuals with a shorter time since injury (stroke) and better initial arm and hand function exhibited greater improvements after 4 weeks of RAAT. However, no associations were found between training volume and improvements in arm and hand function, spasticity, grip strength, gross motor dexterity, or activities of daily living.
Training volume
These results align with the findings of Johansen et al. (2023), who also reported no significant correlation between training frequency, session duration, and the outcomes of RAAT. According to Johansen et al. (2023) the substantial variability inf frequency and duration of training sessions, likely contributed to the observed variations in findings. This variation in training volume in previous studies, complicates direct comparisons to the current study. Several systematic reviews have highlighted challenges in comparing training dosage and intensity across studies due to inconsistent reporting of these variables47,48 and differences in the types of robotic devices employed. 48
However, numerous systematic reviews have demonstrated that RAAT yields more favorable outcomes in arm and hand function compared to conventional therapy.4,14,47 Increased training intensity and a higher number of repetitions have been suggested in several studies as potential explanations.4,47 The importance of training intensity,49,50 the number of repetitions, and task-specific training has been highlighted as critical factors in motor function rehabilitation following a stroke. 49 Furthermore, the severity of arm and hand dysfunction after a stroke plays a significant role in determining functional recovery. 51 In line with our finding, other research indicates that higher baseline levels of arm and hand function post-stroke/ higher initial arm and hand function levels post-stroke are strongly associated with a greater potential for improvement.51–53
Spasticity, grip strength, gross motor dexterity and ADL activities
The present study found a significant negative correlation between training frequency and changes in spasticity; in other words, participants who underwent RAAT more frequently exhibited lower spasticity levels. Prior research on RAAT and spasticity has been inconsistent, with some studies reporting reductions in spasticity54,55 0, while others found no significant effects56,57 Unlike our study, these investigations did not account for training dosage variations, such as frequency, session duration, and total active training time. Furthermore, differences in robotic device types, training intensity, participants’ functional levels, and time since injury further complicate comparisons. No significant associations were found between training volume and changes in grip strength or gross motor dexterity, although prior studies suggest that robotic intervention may enhance these outcomes compared to conventional therapy. 58 Participants in Doo Han’s study showed higher initial functional levels compared to those in the current study. Prior literature 59 highlights the role of active finger function in recovery of arm and hand function. Given that many participants in the current study had severe upper extremity impairments at baseline, the limited progress in arm and hand function may reflect the lack of active finger function. No studies directly examined training volume’s impact on gross manual dexterity or grip strength. Similarly, no significant associations were found between training volume and ADL performance after 4 weeks. While some systematic reviews4,47 support a positive link, others do not14,48 possibly due to differences in robotic devices and training focus.
Demographic and disease-related factors
Results from the current study indicate that participants with a shorter time since injury exhibited greater improvements in arm and hand function following 4 weeks of RAAT Otherwise, no significant associations were found with other demographic and disease-related variables.
A consensus study by Bernhardt et al. (2017) highlighted that brain plasticity, spontaneous recovery, and functional improvements are most prominent in the early stages following a stroke. The greatest progress typically occurs during the acute phase, within the first few weeks’ post-stroke, after which the recovery rate gradually declines and stabilizes around 6 months. 60 These findings are consistent with the results of our study, emphasizing the critical importance of the timing of rehabilitation to optimize recovery outcomes. Early initiation of rehabilitation is therefore crucial to fully take advantage of the “window of opportunity” available during the initial post-stroke period. Also supported by the Norwegian guidelines who emphasizes the importance of early rehabilitation as an important factor in reducing disability after stroke. 61
Initial arm and hand function
Further analyses showed that participants with an ARAT score above the median (>13.5) demonstrated significantly greater improvement in arm and hand function compared to those below the median (<13.5). As previously noted, the severity of functional impairment following stroke is a critical determinant of motor recovery.51–53 A study by Yang et al. (2023) suggests that RAAT produces better outcomes for patients with mild to moderate impairments. 4 This may be due to the robot’s ability to adapt and grade the level of assistance, allowing participants to maximize their functional abilities. 4
These findings align with our study results and may indicate that the degree of impairment in arm and hand function significantly influences the potential for improvement through RAAT This emphasizes the need for rehabilitation strategies that are both well-tailored and adaptive, considering everyone’s progression and potential throughout the therapy process.
Study limitations
The study adopted an experimental, prospective, and longitudinal design, utilizing pre- and post-intervention data from the ARIS project. 16 This approach constrained the selection of study design, outcome measures, training protocols, and variables critical for addressing key research questions and managing confounding factors.
Using existing data for these analyses has been time- and resource-efficient. The sample size (n = 20) is relatively small, restricting the statistical power of the analyses and limits the ability to detect potentially meaningful associations between training volume and clinical outcomes. With a larger sample size, it would have been possible to uncover actual associations that we did not detect in this study due to low sample power. Despite some limitations, this design succeeded in identifying clinically meaningful associations that can generate new hypotheses for future research, such as questions regarding patient selection criteria for optimizing therapy protocols, ensuring the effective and efficient use of RAAT.
ARAT has previously been found useful in predicting outcomes, including improvements in arm and hand function based on baseline scores, for instance by Chen et al. (2012), who demonstrated ARAT’s good predictive validity. 62 ARAT also has strong construct validity 25 and inter- and intra-rater reliability,26,27 making it a suitable tool for both clinical and research use. However, ARAT has demonstrated ceiling and floor effects, 63 potentially impacting results by failing to capture changes in participants at the scale’s extreme ends. This limitation is relevant, as many participants in this study fall into these categories, meaning that those with high scores may not have fully regained pre-stroke function, and subtle changes in low-scoring participants may go undetected.
Since no studies on MCID for subacute-phase patients were available, we applied an MCID threshold of >5.7 points established for chronic-phase patients. In our study, 10 out of 20 participants had ARAT change scores exceeding 5.7 points, indicating a clinically significant improvement. However, it is possible that fewer than 10 participants experienced a truly meaningful clinical benefit.
The participants’ cognitive level was, prior to inclusion, evaluated by a medical doctor, based on the participants’ medical history and clinical assessments. As no specific clinical tests or scales were used, the participants’ cognitive level is uncertain and might have influenced the participant’s compliance.
Also, the fact that all participants were right-handed, with only nine of them having the same dominant side as their affected side, might have caused potential bias.
Participants engaged in a consistent training program, completing 3–5 sessions per week over a 4 week period, with the majority of sessions lasting approximately 45 min. This limited variability in training frequency, session duration, and total active training time could reduce the likelihood of finding significant associations between training volume and functional changes.
Participants in this study performed RAAT by using either Amadeo® (n = 3), Armeo®Spring (n = 7) or a combination of these two devices (n = 10). As the therapeutic benefits and improvements associated with Armeo® may differ from those associated with Amadeo®, outcomes could have been analyzed separately for participants who used only one device, those who used the other device, and those who used both. However, the small sample size in this study limited this opportunity.
Program adjustments, including game selection and robot control, were personalized based on therapist and participant assessments. However, training intensity metrics—repetitions, resistance, and game success rates—were not recorded, leaving intensity unknown. Active engagement is crucial for post-stroke rehabilitation 64 and robotic systems allow for adjustable difficulty based on functional level. 65 Yet, excessive assistance may promote passivity. 65 Fasoli et al. (2003) found greater improvements in participants who actively engaged compared to those needing high assistance. In the current study, many had severe impairments requiring substantial robotic support. While limitations restrict training intensity, those with better function can actively engage in repetitive, task-specific training, potentially enhancing rehabilitation outcomes.
Clinical implications
The findings from this study underline the critical importance of tailoring robotic-assisted therapy to individual patient profiles in stroke rehabilitation. While no overall association was found between training volume and functional improvements, significant gains were observed in patients who started therapy earlier post-stroke and those with better initial arm-hand function. This suggests that clinicians should prioritize early intervention, and a personalized approach based on baseline functional status to maximize the benefits of RAAT. Additionally, these results emphasize the need for further research to refine patient selection criteria and therapy protocols, ensuring effective and efficient use of robotic technologies in stroke recovery.
Conclusion
The current study found no relationship between training volume and changes in arm and hand function, grip strength, gross motor dexterity, spasticity, and activities of daily living. The most notable finding was that participants with better initial function and/or a shorter time since injury, experienced the greatest improvements in arm and hand function after 4 weeks of RAAT. Further research in the area, with more robust study design, is essential to identify several factors that enable targeted, individualized, and effective RAAT.
Footnotes
Ethical Approval
We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during this research. The study was approved by the Norwegian Regional Committee for Medical and Health Research Ethics (Ref: 556789) and the Norwegian Agency for Shared Services in Education and Research (Ref: 411964). The robotic systems utilized in this study underwent a risk and safety analysis for medical technical equipment. This analysis concluded that patient information security and privacy are adequately protected and are in full compliance with General Data Protection Regulation (GDPR) standards.
Author Contributions
CÅ was responsible for designing the research protocol, data analysis, testing of the patients and writing the manuscript. AO and MFW contributed to the protocol, data analysis and writing the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Sunnaas Rehabilitation Hospital and Birgit and Rolf Sunnaas Memorial Foundation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Additional data are available from the corresponding author on reasonable request.