
Abstract
Keywords
Introduction
A confluence of multiple factors contributes to the formation of pressure injuries (PrIs). Nonetheless, mechanical compression and shearing of muscle and fat tissues against bony protuberances are considered the primary causes.1,2 When pressure or shear stresses exceed certain thresholds, cell deformation occurs, leading to cell death. Additionally, pressure-induced capillary occlusion can result in cell death due to ischemia if the pressure is not relieved over time. PrIs develop slowly under low pressure but can form rapidly under higher pressures.3–5 Therefore, it is crucial to minimize both the magnitude and duration of external mechanical loads on soft tissues to reduce deformation and ischemic cell death. 6
Prolonged immobilization is inevitable during long-range aeromedical evacuation (LAE) to stabilize casualties with spinal fractures, suspected spinal cord injuries, polytrauma involving major bones like the pelvis and femur, and traumatic brain injuries.7–9 However, PrIs are a significant concern during such long durations of immobilization as prolonged and high mechanical loading on soft tissues can lead to pressure injuries.3,10 This issue is particularly concerning for military LAE for several reasons. Casualties are often placed in a supine position for 6 to 16 h, as seen during LAE in the Iraq and Afghanistan conflicts.9,11 The use of military litters, litter pads, and vacuum spine boards can create high-pressure points on vulnerable areas of the body, such as the occiput, sacrum, buttocks, and heels.8,12,13 The combination of longer flight duration and high pressure exerted on soft tissues by the support surface can easily exceed the pressure magnitude and duration thresholds for PrIs. Further, conventional techniques to reduce pressure injuries, such as patient repositioning, are often impossible in LAE due to limited space and patient conditions. 9
The prevalence of PrIs among critically injured casualties transported from combat zones by US Air Force Critical Air Transport Teams highlights the severity of the problem.9,13,14 Retrospective analysis shows PrI rates over 50% among casualties from Iraq before admission to VA Hospitals. 13 Although commonly used vacuum spine boards are known to reduce interface pressure compared to military litters and pads, 8 prevalence rates of 4.9–9.3% have been reported in critically injured casualties transported using vacuum spine boards.9,14
In general, the consequences of PrIs are significant, leading to pain, discomfort, reduced mobility, depression, and anxiety. Additionally, pressure injuries can result in more surgeries, longer hospital stays, increased risk of infection, and higher mortality rates. 15 For severely injured casualties, this secondary medical complication adds more complexities in overall care, which can significantly delay recovery and complicate the overall treatment and rehabilitation processes, potentially leading to long-term disabilities. The treatment cost is also substantial, ranging between $500–152,000 (USD) per patient. 16 Considering the prevalence rate, human toll, and cost, not much research has focused on understanding and improving pressure redistribution to reduce PrI risk during LAE.
Multiple studies have evaluated the interface pressure between the body and support surfaces on commonly used military litters and pads, as well as newly developed overlays for military litters. Bridges et al. investigated interface pressure at vulnerable areas of the body while using the NATO Litter, as well as the NATO Litter with an Aeromedical Evacuation (AE) mattress. The NATO Litter produced pressures ranging from 102 to 148 mmHg on the scapula, sacrum, and heels, while the NATO Litter with the AE mattress resulted in pressures of 72–76 mmHg. 11 In 2009, the vacuum spine board was designated by the US Air Force as the preferred method of immobilization during aeromedical evacuation to reduce pressure injuries. The vacuum spine board can increase the contact area and distribute weight over a larger surface area.8,17 However, the effectiveness of reducing pressure injuries is marginal.8,9,14 Recent work compared the Talon litter and the Warrior Evacuation Litter Pad (WELP) to a prototype mattress, which has a void corresponding to the sacrum area to offload pressure. Compared to the WELP, the prototype was shown to reduce peak interface pressure on the sacrum, occiput, and heels, but not on the buttocks. 12 Sun et al. compared the interface pressure from a prototype foam overlay with a hard spine board, which produced pressures of 51.9 mmHg on the head, 60.1 mmHg on the scapulothoracic region, 66.8 mmHg on the sacroiliac region, and 60.2 mmHg on the heels. 18 A recent report on a pressure-alternating pad combined with WELP shows the ability of this combination to reduce interface pressure on vulnerable regions of the body. However, the immobilization capabilities of the pressure-alternating pad are not discussed. 19
Despite several research efforts, current technologies and recommendations for LAE and other modes of transportation (land, sea, and rotorcraft) are insufficient to prevent PrIs, as none of them reduce pressure below 40 mmHg across all regions, which is the recommended maximum interface pressure to prevent PrI formation.5,12,20 Improvements are needed to address PrIs at the occiput, scapulothoracic region, sacrum, buttocks, and heels. Since existing technologies are designed as universal litter pad solutions, they do not target all vulnerable regions and may not be suitable across the spectrum of body sizes to reduce interface pressure. To address this, a support surface technology that utilizes air-cell-based cushions to control interface pressure in selective sections could be utilized. Our previous work on smart seat cushions and cyclic pressure offloading shoe insoles for PrI prevention demonstrated the feasibility of an air cell based customizable solution that can target pressure reduction in sensitive areas.21,22 This work aims to develop an adaptable overlay cushion for military litters and spine boards that reduces interface pressure in high-risk regions, regardless of patient anatomical variations and casualty conditions.
This manuscript presents the preliminary design and experimental test results of the adaptive spine board (ASB) overlay. The air cell array-based overlay consists of four segments: head and neck, shoulder/upper trunk, buttocks/pelvis, thigh and shank, and foot/heel. The design considers pressure modulation on pressure injury-prone vulnerable region: occiput, scapulothoracic region, sacrum, and heels. The pressure in each region can be independently controlled using sensor-driven technology. Additionally, an algorithm was implemented to maintain air cell pressure, compensating for environmental effects such as temperature and barometric pressure changes, which is crucial for air cell-based cushions operating in varying conditions, such as those experienced in ground and air transportation.
Methods
System description
The ASB overlay system consists of an air cell array cushion, a pneumatic control unit, and a graphical user interface (GUI) with operation algorithms shown in Figure 1. The cushion has five sections, where one section (S4) is made with foam and the other four sections (S1, S2, S3, S5) are each made of a group of air cells. The air cells within each group are connected to each other and share the same air channel, making up one section. The pneumatic control unit consists of an air pump, designated pneumatic valves and pressure sensors for each air cell group (section), a pressure sensor to measure atmospheric pressure, and a microcontroller, similar to the control unit reported in our previous work.
23
The system is controlled through the GUI, and pressure sensor data are used for closed-loop control of internal pressure of air cells using operation algorithms. A detailed description of the operation is described in the control and operation section of this manuscript. Schematic of ASB overlay system overview.
Design and simulation
The adaptive spine board overlay is designed to be placed on top of a standard military litter. It consists of four sections made with air cells and one section made with foam. Figure 2 shows how the air cell sections correspond to the pressure injury-prone regions of interest: occiput, scapulothoracic region, sacrum, and heels. The foam section corresponds to the thighs and shanks where there are no bony prominences. As shown in Figure 2, the head and neck section is comprised of four interconnected cells, the shoulder/upper trunk and buttocks/pelvis sections each feature eight interconnected cells, and the foot/heel section contains ten interconnected cells to make the section longer to accommodate people with varying heights. CAD model of ASB overlay design showing the different sections corresponding to pressure injury-prone body regions.
Details of ASB overlay.

Finite element simulations were conducted to study air-cell designs for the ASB overlay to optimize the cell geometry and evaluate their deformation under various initial internal cell pressures and loading conditions. Key parameters such as cell height, width, wall thickness, and top surface geometry were adjusted through an iterative design process.
ANSYS transient structural simulation analysis was utilized to perform design optimization. Two types of hyperelastic materials were simulated: polyurethane (PMC-724) and silicone rubber (XIAMETER RTV-4334-T4). Experimental data for polyurethane and silicone uniaxial and planar tension were used to obtain the parameters for Yeoh’s third-order material model (best-fit curve).
24
A hydrostatic fluid element was applied to the inner walls of the cell to set and track the air cell pressure (illustrated in Figure 3(a) in red). The air cell was fixed at the bottom, with pressure applied ranging from 0.5 to 1.5 kPa in 0.5 kPa increments, and loads of 10, 20, and 30 N were applied through a rigid block. These cell pressure and load values were determined based on our previous work.
25
Interface pressure, shear pressure, surface expansion, and immersion values were used as outcome measures to compare different designs. Since the ASB cells in the four sections are made of polyurethane, simulations using its material properties were conducted first until the final design was achieved. Then, the final design was studied using silicone materials properties to ensure that the material does not cause any high-pressure points. (a) Hydrostatic fluid element (top) and simulation boundary conditions (bottom), (b) the initial air cell designs along with a cross-section view, (c) the optimized air cell design with a cross-section view.
The initial simple cell design (Figure 3(b)) was selected as the starting point of simulation. To improve stability and ensure compatibility with the MedEvac Litter, the cell dimensions were reduced from the initial design. Simulations were then used to optimize cell wall thickness and refine the top surface geometry by rounding and smoothing the surface to eliminate any high-stress concentration. While the initial design had a uniform thickness, the optimized design (Figure 3(c)) featured a reduced wall thickness at the top and rounded walls of the cell, relative to the side wall near the base, to further decrease high-pressure points caused by steep edges during weight bearing.
Fabrication
The air cells are made of polyurethane (PMC-724) and silicone rubber (XIAMETER RTV-4334-T4), as simulation results demonstrated that both materials provided similar results. The air cells were created through a two-step molding process combining injection molding and over-molding techniques similar to previously published work.
26
The molds for the air cells were designed using SolidWorks and printed using 3D stereolithography. Each air cell is fabricated individually and assembled to a soft mat (shown in Figure 4 in light blue) using plastic fasteners around the rims of the air cells. Each cell is strategically assembled at an optimal distance from each other as obtained from the simulation results. Cells in each section are pneumatically interconnected, and each section is connected to a pneumatic control box. In the current prototype, the shoulder/upper trunk, buttocks/pelvis, and foot/heel sections were fabricated with polyurethane, while the head and neck section were fabricated with silicone. Of the two materials, silicone may be a better choice for fabrication because of its ability to bond to itself and silicone tubing, ensuring secure tubing connections while also simplifying the fabrication process. The thigh and shank section is composed of a foam block. Fabricated and assembled ASB overlay.
Control and operation
The ASB overlay enables interface pressure control at each vulnerable region of the body through adjusting air pressures of each air cell sections. It also has a built-in safety feature for maintaining air cell pressure at the appropriate levels regardless of environmental effects including temperature and pressure variations. To achieve this level of control, a pneumatic control system was designed as follows.
The control systems diagram, shown in Figure 5, consists of various electronic and pneumatic components to operate the ASB. It features four pneumatic channels, each designated for the head and neck, shoulder/upper trunk, buttocks/pelvis, and foot/heel sections of the spine board. Each channel is connected to a pressure sensor and a solenoid valve. The pressure sensor measures the pressure inside the air cells, while the solenoid valve controls the airflow to and from the air cells. Two pumps are used—one to generate pressure and the other to create a vacuum for the air cells. Additionally, two solenoid valves switch between pressurization and vacuum modes. Two proportional valves are employed to regulate airflow: one for pressurization and the other for vacuuming. The opening of these proportional valves is controlled using a PID controller based on feedback from the pressure sensors, ensuring that each section of the spine board maintains the required pressure. Schematic diagram of pneumatic control system hardware for ASB.
To operate the system, all sections must first be pressurized prior to the patient lying down to support their weight. With the current hardware capabilities, the internal air pressure values for each section can be set, monitored, and adjusted separately to accommodate the patient’s body shape and weight distribution throughout their transport. A pressure-maintaining algorithm was also implemented to ensure the ASB overlay operates regardless of external factors. For instance, in the event that internal air pressure changes due to environmental temperature and pressure fluctuations, pressure and vacuum pumps will operate in coordination to maintain the cells’ internal pressures at the set values, preventing undesired cell volume expansion or contraction that would affect the efficacy of the ASB overlay.
Experimental setups
Three preliminary tests were performed to understand the Adaptive Spine Board overlay’s immersion and interface pressure reduction capabilities, as well as the efficacy of its pressure-maintaining algorithm under varying environmental conditions. During all experiments, the ASB sections were inflated to an initial pressure of 1.5 kPa. For the immersion and interface pressure tests, internal pressures of air cells were not modulated to understand the initial effect of the ASB on interface pressure distribution.
Immersion test
The immersion capabilities of our engineered ASB overlay were tested following the support surface standards set forth by Rehabilitation Engineering and Assistive Technology Society of North America (RESNA) SS-1:2019. As shown in Figure 6, the setup consists of a test bench, a National Pressure Ulcer Advisory Panel (NPUAP) 50th percentile male mannequin and a fixture with a winch system capable of raising and lowering the mannequin. The mannequin was fabricated using CNC machining based on a CAD model obtained from RESNA. The immersion capabilities of both the WELP pad and the ASB overlay were tested. A protocol for the immersion test was adapted from the RESNA SS-1: 2019 Vol.1 Sec.2 protocol. The internal pressure of the ASB cells before applying load was set to 1.5 kPa in each section. Immersion measurements were taken for the ASB and the WELP pad at locations corresponding to each ASB air cell section (S1-S3 and S5). RESNA standard immersion test setup with (a) the WELP and (b) the ASB overlay. (c) A close-up of the immersion of the head and neck region.
Interface pressure comparison test
In this test, full-body interface pressure maps and average interface pressure at peak pressure regions ‒ the head and neck, shoulder/upper trunk, buttocks/pelvis, and foot/heel regions ‒ were compared for the MedEvac Litter, WELP, and our engineered ASB overlay using a commercial pressure mat (Boditrak2 Pro) with five participants. Figure 7 shows the MedEvac Litter, WELP on Litter, and ASB on Litter, respectively. The interface pressure mat was placed on each surface, and participants were asked to lay in a supine position. Prior to the ASB testing, all sections were inflated to a pressure of 1.5 kPa before the participant lay down. Subsequently, no further pressure adjustments were made after the participant was placed on the ASB. (a) MedEvac Litter, (b) Warrior evacuation litter pad on litter, (c) adaptive spine board overlay on litter.
Pressure map screenshots were recorded for all participants laying on each of the support surfaces. Interface pressure values were recorded by calculating the average of readings from nine sensors (3 × 3 array) at the area of peak pressure in each region (head and neck, shoulder/upper trunk, buttocks/pelvis, and foot/heel). For example, Figure 8 shows the interface pressure map of a shoulder region, where the nine measured sensors (black dots) are boxed by the dotted lines. This pressure calculation approach has been used in previous evaluations to compute interface pressure on different support surfaces such as seat cushions and mattresses.27,28 By using this approach, any outlying high-pressure points that may be caused by a participant’s clothing or the sensor mat kinking are eliminated, thus preventing misinterpretation of the data and analysis. Full-body pressure maps of each participant while lying on the MedEvac Litter, WELP, and ASB were compared, and each region was analyzed separately, with average and standard deviation values calculated. 3 × 3 sensors at peak pressure for the shoulder region.
Participants’ heights and weights, including their averages and standard deviations.

Environmental effect test
The ASB overlay was tested for its capability to maintain a given desired air cell pressure regardless of environmental conditions, including temperature and atmospheric pressure.
For temperature testing, an enclosed chamber (33 × 25 × 25 in) was built using polycarbonate sheets with two separate hose connections to an electric heater and portable air conditioner, as shown by the orange components in Figure 9. The heating and cooling systems were connected to a temperature control unit, along with a temperature sensor, where chamber temperature could be set and maintained at a desired temperature ±0.5°C. A section of the ASB overlay (4 × 2 array) was placed inside the chamber along with the temperature sensor. The chamber temperature was set at 15°C initially, then the air cells were inflated to a starting pressure of 1.5 kPa. Next, temperature was increased in 2°C increments, where temperature was held for 3 min at each increment, until reaching 35°C. Then, the test continued repeating these steps but ramping back down in 2°C increments until returning to 15°C. Internal pressure of air cells was recorded over time with and without the pressure-maintaining algorithm to observe the effect of temperature on the air cells. Environmental chamber setup.
For atmospheric pressure testing, the chamber was modified to have 3 ports, as shown by the green components in Figure 9. The first port was connected to a vacuum pump for creating negative pressure inside the chamber. The second port was connected to a simple control unit to manage the negative pressure inside the chamber. The last port was connected to the air cell array, allowing flow of air in and out of the air cells, which was controlled by the ASB overlay control unit. A portion of the air cell cushion was placed inside the chamber and inflated to 1.5 kPa. Pressure and vacuum sensors monitored the internal pressure of air cells, as well as the internal pressure of the chamber. Starting at 101 kPa (atmospheric pressure), pressure within the chamber was decreased in 3.7 kPa increments until reaching 75 kPa (equivalent to aircraft cabin pressure at 8000 feet). Internal pressure of air cells was recorded at each increment with and without the pressure-maintaining algorithm to observe the effect of atmospheric pressure on the air cells.
Results
Single cell simulation
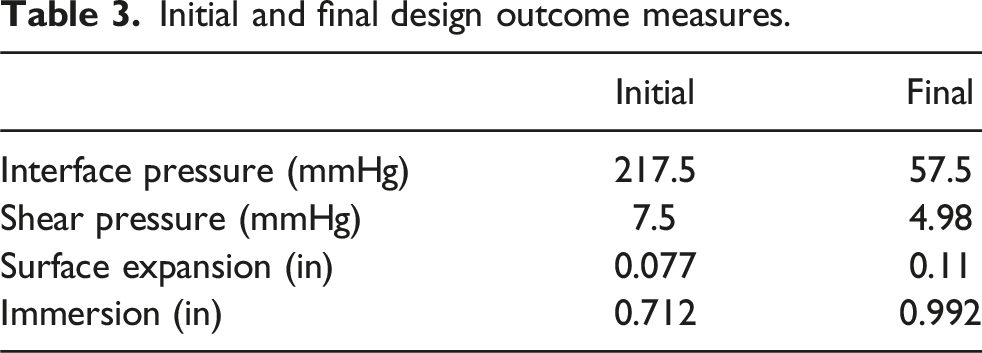
Single-cell designs were simulated to optimize geometry and reduce contact pressure by utilizing interface pressure, shear pressure, surface expansion, and immersion outcome measures. Figure 10 shows the initial and final cell design interface pressure maps, with red regions indicating areas of high stress with 1.5 kPa initial internal air pressure and 30 N load. The final design achieved lower interface and shear pressures, along with higher surface expansion and immersion, effectively reducing high-stress concentration points that will help to mitigate pressure injuries. Table 3 shows initial and final design pressure and displacement values under 30 N load with 1.5 kPa internal pressure. (a) Initial and (b) final design interface pressure maps. Initial and final design outcome measures.
Immersion test
The immersion results are displayed in Figure 11 for both the WELP and the ASB overlay. Overall, the ASB exhibited greater immersion compared to the WELP. The immersion values for the WELP are head/neck 3.07 ± 0.1 cm, shoulder/upper trunk 2.87 ± 0.1 cm, buttocks/pelvis 2.87 ± 0.1 cm, and foot/heel 4.21 ± 0.1 cm. In contrast, the immersion values for the ASB are head/neck 4.29 ± 0.1 cm, shoulder/upper trunk 4.24 ± 0.1 cm, buttocks/pelvis 4.34 ± 0.1 cm, and foot/heel 4.34 ± 0.1 cm. Immersion results of the WELP and ASB support surfaces.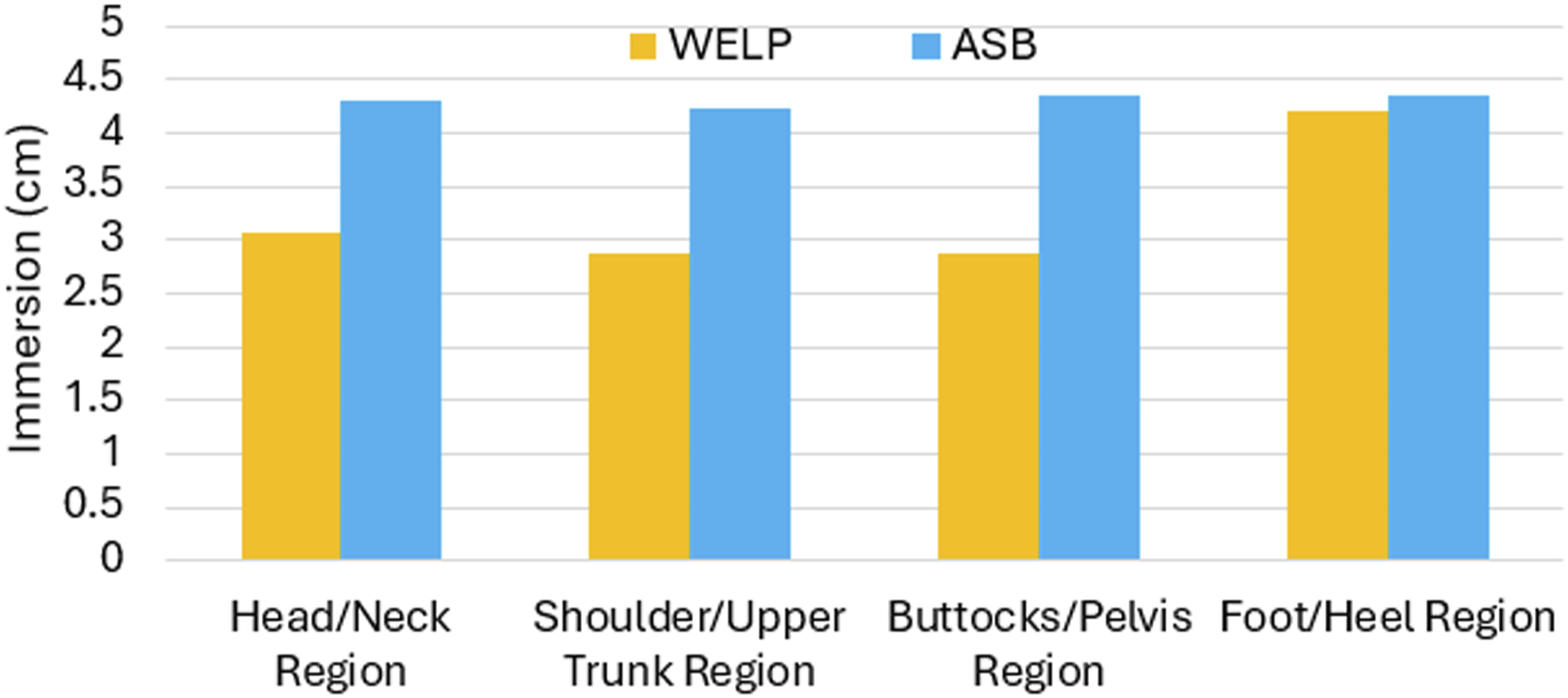
Interface pressure
Figure 12 shows the interface pressure maps for Participant 1 across all tested support surfaces. For this participant, the interface pressure map for the MedEvac Litter displayed the largest high-pressure area (indicated in red). The WELP showed small red areas at the head and buttocks regions, while the ASB displayed no red areas at all. Interface pressure maps for MedEvac Litter, WELP, ASB.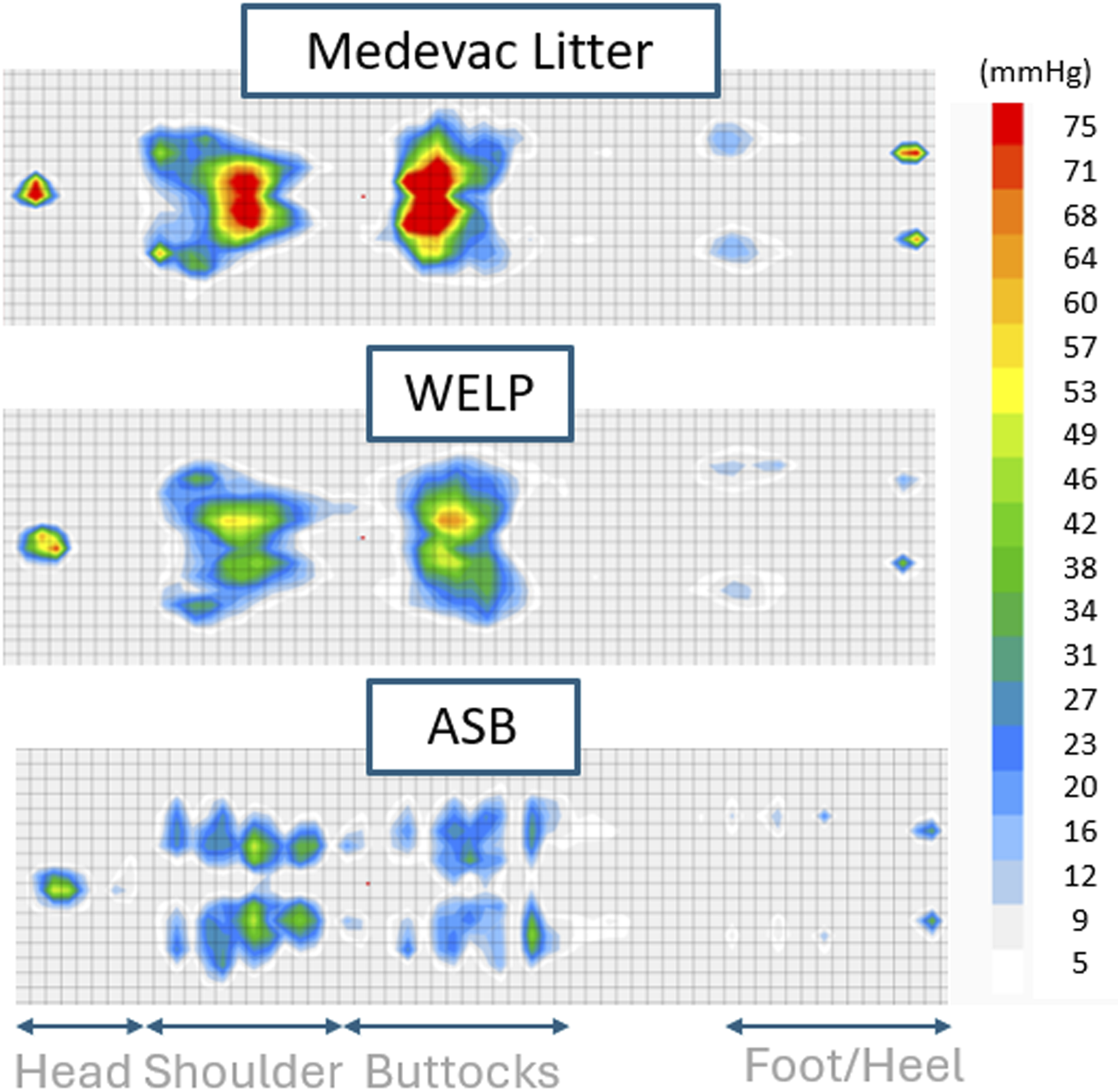
Interface pressure was assessed among five participants for all regions with average and standard deviation values, shown in Figure 13. For the MedEvac Litter, the head region exhibited the lowest average interface pressure, whereas for both the WELP and ASB, the foot/heel region showed the lowest pressure. When examining the peak interface pressure regions for all support surfaces, the MedEvac Litter produced the highest pressure on the buttocks, whereas similarly high values were observed for both the WELP and ASB in the buttocks and shoulder regions. Comparison of the peak pressure areas for the head and neck, shoulder/upper trunk, buttocks, and foot and heel regions between MedEvac Litter, WELP, and ASB (n = 5).
When assessing average interface pressures across all regions, the ASB yielded the lowest values, followed by the WELP. Among five participants and four different regions, there are only two instances in which the WELP interface pressure value is lower than that of the other support surfaces, which occurs in the buttocks and foot region, out of a total of 20 instances.
Environmental effect test
Figure 14(a) shows the change in internal pressure of the air cell array (representing a single ASB section) over time as temperature ramped up and down over the range of 15°C–35°C. The blue line shows that, without the pressure-maintaining algorithm, internal pressure increased about 0.75 kPa from the starting temperature to the maximum temperature. The orange line shows that, with the pressure-maintaining algorithm, internal pressure remained at 1.5 ± 0.15 kPa. Variations in internal pressure in response to (a) temperature (b) chamber pressure changes with and without the control algorithm.
Figure 14(b) shows the change in internal pressure of the air cell array at eight discrete environmental chamber pressures (blue line), in the range 101–75 kPa. When the chamber is at atmospheric pressure (101 kPa), the internal cell pressure is shown to be initially inflated to 1.5 kPa in both cases, with and without the control algorithm. Without the control algorithm (orange line), the 1.5 kPa pressure difference between the air cells and the surrounding environment begins to diverge after chamber pressure drops below 97 kPa. With the control algorithm (green line), pressure in the air cells was maintained at 1.5 kPa above the recorded measurements of the environmental pressure.
Discussion
Immersion test
It is evident that ASB overlay provides greater immersion compared to the WELP pad across all tested body regions. Specifically, the ASB shows increased immersion values in the head region (12 mm increase), shoulder region (13 mm increase), buttocks region (14 mm increase), and heel region (1 mm increase) compared to the WELP. The higher immersion values indicate that the ASB overlay sinks and conforms better to the body compared to the WELP, allowing for better pressure distribution thereby lowering the interface pressure and reducing the risk of pressure related injuries. It was observed that all regions showed a great difference in immersion between the ASB and WELP, except for the heel region. Due to the length of the RESNA model, the heel region was very close to the edge of the WELP and likely explains the increased immersion in this region.
While immobilization capabilities were not investigated during the immersion tests, it is postulated that higher immersion will provide greater conformity of the cushion to the body (similar to vacuum spine boards used for immobilization). The immersion provided by the ASB compared to the WELP may indicate better performance in immobilization.
Interface pressure test
Looking at the interface pressure maps of one individual (shown in Figure 12), the MedEvac Litter displayed the largest area of high interface pressure (red areas), whereas the ASB showed the smallest area of high interface pressure. It is postulated that the material and geometric features of the support surfaces contribute to the differences in interface pressure. The MedEvac Litter is made of a thin, tight fabric, the WELP is composed of medium-firm foam (2-inch height) covered with a soft fabric, and the ASB is an air cell array consisting of 2.6-inch-high hyperelastic silicone and polyurethane air cells. Based on this examination of material and geometric features, elastic and soft materials that allow displacement of a load (immersion) with surface geometry that support the body regions appear to provide lower interface pressure.
Figure 13 helps to visualize which body regions experience the highest amount of pressure when using each type of support surface by investigating the average peak interface pressure of all tested subjects. For the MedEvac Litter, the buttocks region exhibited the highest pressure, while the head region had the lowest. On the WELP, the shoulder and buttocks regions showed similar pressure values, while the heel region had the lowest. The ASB demonstrated a similar pattern to the WELP. The MedEvac Litter exhibited the largest standard deviations in interface pressure, particularly in the shoulder, buttocks, and heel regions, compared to the WELP and ASB. This variation may be due to the stiffer surface of the Litter, causing more pronounced differences in interface pressure profiles for people of differing body shapes.
In most instances, peak pressure values on both the WELP and ASB were below 40 mmHg, which is generally considered safe in terms of maintaining capillary perfusion. One reason for these low-pressure readings may be due to the size of participants who were relatively small compared to U.S. Army personnel anthropometric data. 29 Testing with a wider range of body sizes, shapes, and weights may reveal clearer differences in interface pressure data between the ASB and WELP.
Environmental effect
The environmental effect study demonstrated how temperature and pressure of the atmosphere have a critical effect on the behavior of air cells, which could alter the air cells’ effectiveness in safety and pressure reduction for cushion applications in airplane environments.
As expected, heat caused air within the cells to expand, 30 increasing internal pressure by about 0.75 kPa. The control algorithm, which continuously reads internal pressure of the cells, was able to open and close the valve in the ASB overlay control unit to reduce or increase pressure as necessary to maintain 1.5 kPa.
It was also predicted that the air cells would expand under vacuum in order to maintain equilibrium between the air inside the cells and the air in the vacuum chamber. Although expansion of cells may typically suggest an increase in internal pressure, the pressure sensor reading the inside of the cells decreased. The internal air cell sensor reading shows that pressure decreases along with the environmental pressure. As environmental pressure decreased, the difference between the pressure reading of the cells and the chamber increased, which can explain the observed increase in air cell size and volume. When the difference between the cells and chamber pressure readings was maintained at 1.5 kPa (the same difference at initial pressure), the air cells did not expand in volume.
The usability of the system in airplane environments (air worthiness) will be considered in future iterations and during conception of an industrial manufacturing process. Those aspects will include use of flame-resistant materials, as well as incorporating a foam layer within the air cells to provide passive protection in the event of technical failure or rapid decompression, where response of the ASB algorithm might be delayed. In addition, the control unit will be made with Institute for Printed Circuits Standards to make them safe for use in aircraft.
Limitations
This preliminary study demonstrates promising immersion and interface pressure performance of the ASB compared to existing support surfaces; however, there are additional aspects that can be studied and other capabilities of the ASB that can be implemented and explored. First, during the immersion test, the use of standardized models does not fully capture the diversity of the human body, nor does it replicate the dynamic nature of human activity (e.g., shifting, breathing, and tissue compression). While the interface pressure test was conducted on five participants, the average weight and height of this sample was relatively small compared to average U.S. Army personnel anthropometric measurements. 29 It is essential to test the current cell layout on a larger, more diverse group of participants with varying body sizes, heights, and weights to better assess the effectiveness. We do not anticipate any significant impact on interface pressure results for taller and/or heavier participants as the ASB layout has a sufficient number of interconnected air cells at each body region to accommodate a wide range of body weights and contact areas. Additionally, while immersion is linked to better pressure relief, this study did not allow for conclusions about subjective comfort, which will need to be assessed in future testing with a larger number of human participants. Second, interface pressure during immobilization is noted as a major concern but participants were not tested under these conditions. The ASB has an additional design feature specifically for immobilization that was not within the scope of this manuscript and will be investigated in a separate study and compared with other support surfaces during immobilization conditions. Third, optimizing the internal pressure of the cells, before and after participant placement, and adjusting the pressure in each region based on individual body weight and size could further reduce interface pressure and increase immersion. Lastly, an environmental effect test was conducted for a section of the ASB. Testing the entire ASB overlay with real human weight distribution in an environmental chamber will be needed to evaluate the pressure control algorithm across multiple sections simultaneously. These limitations will be addressed in future studies to advance the design and functionality of our Adaptive Spine Board.
Future research
A pilot study involving 20–30 participants will be conducted to obtain interface pressure data for the ASB across various body sizes and weights. This addition will provide the authors with a better understanding of body interface pressure distribution across a larger participant sample. Additionally, an internal pressure modulation algorithm will be developed and implemented on the ASB to further reduce interface pressure during patient transportation. This algorithm will help automate the ASB by targeting high pressure regions to reduce interface pressure, enhancing its efficiency and functionality.
Conclusion
This manuscript suggests that the Adaptive Spine Board overlay may provide advantages over both commercial and currently available support surfaces, particularly in terms of immersion and interface pressure. The ASB resulted in the lowest interface pressure across all regions, with values remaining below 40 mmHg based on the pressure map readings. Furthermore, the ASB shows a notable ability to maintain air cell pressure despite temperature and pressure variations due to the integration of a pressure-maintaining control algorithm. This feature enhances the overlay’s functionality across a range of climate conditions, as well as elevation changes.
Footnotes
Acknowledgments
We would like to acknowledge the Trauma Research and Combat Casualty Care Collaborative for their funding support. We also thank the participants involved in testing and the students who contributed to the fabrication of the Adaptive Spine Board Overlay.
ORCID iDs
Author contributions
VE, AP, AJ, IS, and SK contributed to the design, fabrication, testing, data analysis, and manuscript writing. YTZ and MBJW were involved in the immersion tests, manuscript writing, editing, and supervision. All authors reviewed, edited, and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Trauma Research and Combat Casualty Care Collaborative (TRC4 grant number TRC4-2024—0000000068).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.