
Abstract
Introduction
The Ponseti technique is highly effective for correcting congenital clubfoot; however, recurrence must be prevented using orthoses. The double abduction brace (D- A) is recommended by Ponseti and is widely used. However, more user-friendly orthoses have been developed because treatment abandonment with the traditional orthosis is frequent. We report the results obtained using a newly designed unilateral orthosis.
Methods
A unilateral orthosis (UNIC-Brace) was developed and tested in a prospective non-randomized study conducted between 2017 and 2020. The Pirani score was used to monitor the progression of the deformity during plaster correction. The D-A brace (Denis Browne model) served as the control group. The primary outcomes were recurrence rate, treatment adherence, and caregiver satisfaction.
Results
The study included 58 patients (87 feet) in the test group and 51 patients (75 feet) in the control group, with a minimum follow-up period of 3 years. No significant differences in epidemiological data or follow-up duration were observed between the two groups. The failure feet rates in D-A brace and UNIC-Brace groups were 41.3% and 17.2%, respectively (p < .001). Non-adherence patients to treatment were 23.5% in the D-A brace and 13.8% in the UNIC-Brace group (p < .001). Overall, 13.7% of families were not satisfied with the D-A orthosis, whereas 5.2% were not satisfied with the UNIC- Brace (p < .001).
Conclusions
The UNIC-Brace yielded better outcomes than the traditional orthosis at a minimum follow-up period of 3 years.
Keywords
Introduction
The current approach to treating idiopathic congenital clubfoot in newborns includes a series of manipulations and castings to correct the cavus, adductus, and varus, and if necessary, Achilles tenotomy to address the equinus (Ponseti method). This sequence is relatively short, leading to remarkable correction of the foot. Nevertheless, deformities inherently tend to relapse,1–3 and prevention is achieved with splinting.4,5 The most widely used braces are based on the Denis Browne model and are adjusted to hold the foot in an external rotation of 60-70° and dorsiflexion of 10°. 5 This is achieved by using open- topped shoes attached to a rigid bar. The orthosis should be consistently worn until the child reaches 4 years of age. 6 Initially, the recommended usage was 23 hours per day until crawling. Later, the orthosis is worn during nighttime and daytime naps. 7 If the protocol is adhered to correctly, the recurrence of deformities requiring surgical intervention decreases significantly. 3
The single factor most frequently associated with clubfoot relapse was noncompliance with the double abduction brace (D-A brace).8–10 However, strictly following the brace protocol may be a major challenge in the Ponseti method, 11 as parental adherence to treatment diminishes rapidly as the child grows.2,12
To improve compliance, the D-A brace has been modified to enhance patient comfort and adherence.13,14 Some authors have explored the use of unilateral orthoses, although the relapse rates are unacceptably high. 15 Conversely, other studies have supported the use of unilateral orthoses.16–19 Although they may be effective, some have mechanisms that increase their cost and limit their use.
To address the limitations associated with the currently employed orthoses for preventing relapse following congenital clubfoot correction, this study developed and tested a novel unilateral orthosis model. Theoretically, this orthosis satisfies the essential adherence criteria because of its affordability, ease of application, simplicity, and low impact on lower-limb movements. This study aimed to present our experience with this orthosis and compare its outcomes with those of the traditional D-A brace. We hypothesized that both braces would exhibit similar performance.
Materials and methods
This study was approved by the institutional ethics committee (approval number 2.638.423; May 7, 2018) and conducted in accordance with the Declaration of Helsinki guidelines.
Prototype development
The development of the new orthotic model spanned 24 months and involved successive modifications and subsequent clinical tests in a small sample. The plaster molds obtained from the lower limbs of children of different ages were used until the prototype was suitable for clinical trials.
The orthosis was custom-made, and its construction began with a limb plaster mold obtained from the distal thigh to the foot to ensure anatomical modeling of the limb. The foot was maintained in slight dorsiflexion (∼10°), abducted ∼45°, and slightly everted. At this stage, the technician’s thumb provided counterpressure to the lateral aspect of the talar head, mimicking the Ponseti technique. A positive mold was obtained, finalized, and trimmed to achieve a precise replica of the limb end, which served as the basis for the orthosis manufacturing.
The next step involved vacuum thermoforming of the positive model using polypropylene. Subsequently, finishing was performed with emphasis on the knee region, where the two flaps were kept in contact with the femoral condyles, as in the patellar tendon-bearing prosthesis. The trimline of the orthosis was lowered in the posterior part of the knee to allow knee flexion of up to 90°. Ethylene-vinyl acetate pads were used to protect the pressure areas on the inner sides of the orthosis. One opening hole in the heel allowed the monitoring of the heel position. The brace was secured to the limb with Velcro straps positioned precisely below the knee, at the ankle (supporting the talar head), and in the middle of the foot (Figure 1). Aspect of the left UNIC-Brace. (a) Front view demonstrating the femoral flaps and the abducted of the foot, (b) posterior view demonstrating condylar flaps, the cut to allow the flexion of the knee, and the abducted foot, (c) superior view to show the abducted foot. (d) patient wearing the brace.
Patient cohort
The present study included children with idiopathic congenital clubfoot who received primary treatment initiated before 4 months of age and whose feet were corrected using the Ponseti method. A minimum follow-up of 3 years of orthotic treatment was established. Patients who were initially treated elsewhere or had incomplete medical records were excluded.
Between 2017 and 2020, 109 children with a total of 162 idiopathic clubfoot participated in the study. During follow-up, the patients were routinely examined by two pediatric orthopedic fellows and evaluated by a single dedicated medical team comprising one senior pediatric orthopedic surgeon (JBV), one orthotist (FYZ), and one physical therapist (LMG).
After casting corrections, the patients were assigned to receive the traditional D-A brace or unilateral clubfoot brace (UNIC-Brace) without pre-established selection criteria. Both types of orthoses were provided by the institution without financial costs to the caregivers.
Comprehensive instructions and training were provided to parents and caregivers on managing both types of orthoses. The recommendation was to use the orthosis 23 hours per day until the onset of crawling, and subsequently only during nighttime and daytime naps. Additionally, mothers were trained by a physical therapist to manipulate the feet of the child at home when the child was not wearing orthoses. Patients were scheduled for monthly assessments in the first 2 months and every 3-4 months thereafter. During follow-up, the families were questioned regarding the orthosis, reporting ease, difficulties, and instructions on usage. The equipment was examined periodically to assess the need for replacement. Progress of correction was evaluated through clinical appearance, flexibility, and alignment of the foot as well as Pirani score. The Pirani score is used to measure the severity of foot deformities. The scale assesses three criteria for the hindfoot and three for the midfoot. A maximum of six points indicates significant deformities, while a score of zero represents a fully corrected foot. 20 When any recurrence of the deformity was identified, radiography was performed, and the patient underwent new serial casting. After foot realignment, the same orthosis used before the relapse was utilized again.
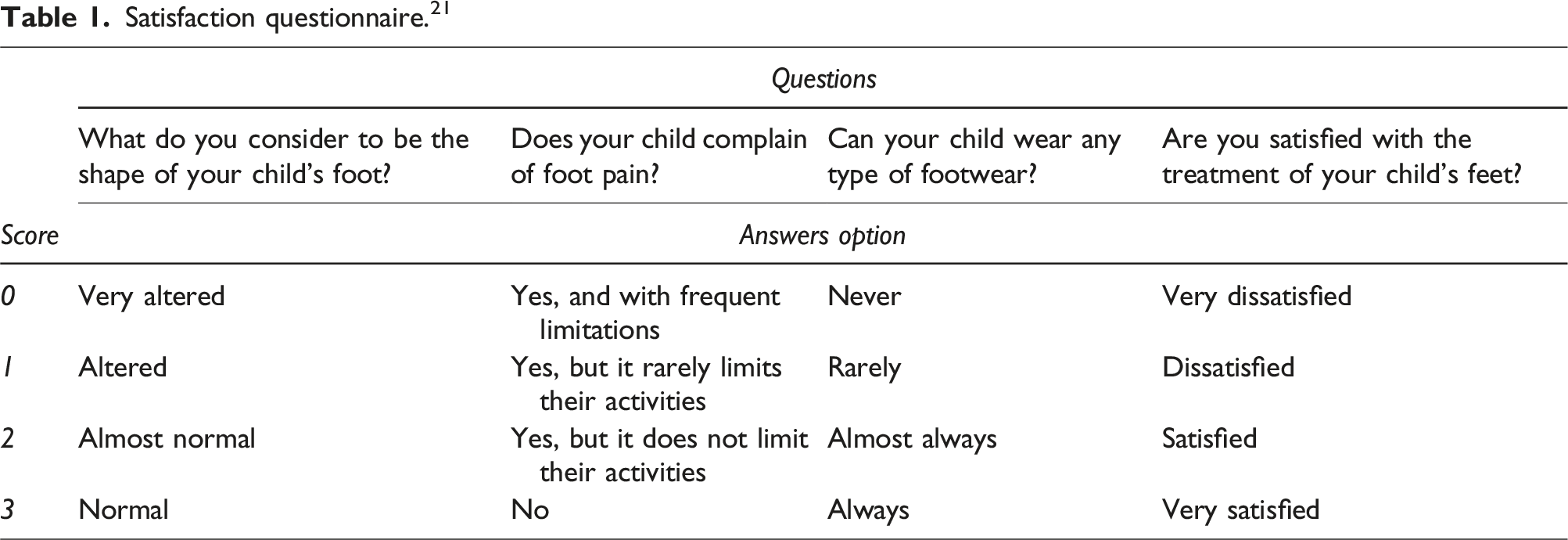
Non-compliance was defined as irregular use 14 or complete discontinuation of bracing. Failure was defined as the recurrence of a deformity requiring a new series of casting or surgical intervention. 21
Satisfaction questionnaire. 21
Grouping
Two groups were established based on the type of orthosis as follows: group 1, (Double Abduction brace (D-A brace) comprising children who used the traditional double abduction orthosis as conceptualized by Denis Browne and recommended by Ponseti4,5 and group 2 including users of the novel UNIC-Brace for testing.
Statistical analysis
Using the SPSS statistical package (Statistical Package for the Social Sciences, USA), numerical variables were compared between the two groups using an independent sample t-test. 23 Assumptions of normality and homogeneity of variances were assessed using the Shapiro-Wilk test. Variance homogeneity was examined using Levene’s test. 24
Six t-tests were performed for the six numerical variables to compare the groups and p- adjust for to prevent FDR (false discovery rate). 25 To compare qualitative variables for occurrence frequencies, the chi-square test 26 was employed, which generated p-values. A 95% confidence interval was used to construct graphs of significant quantitative variables.
Results
After applying the inclusion and exclusion criteria and time span, 109 patients out of 206 patients (162 feet) were included and distributed as follows: 51 children (75 feet) in the D-A brace group and 58 participants (87 feet) in the UNIC-Brace group (p = .037) (Figure 2). Summary of the overall study progress.
Patient´s characteristics at baseline.

The mean number of new braces provided during the follow-up period was 6 in the D-A group and 7 in the UNIC-Brace group. The total cost of each D-A brace and UNIC-Brace was US$160 and US$100, respectively. Therefore, the total cost during the 3-year treatment was approximately US$960 for the D-A brace and approximately US$700 and US$1,400 for the UNIC-Brace in unilateral and bilateral clubfoot cases, respectively.
Final results.
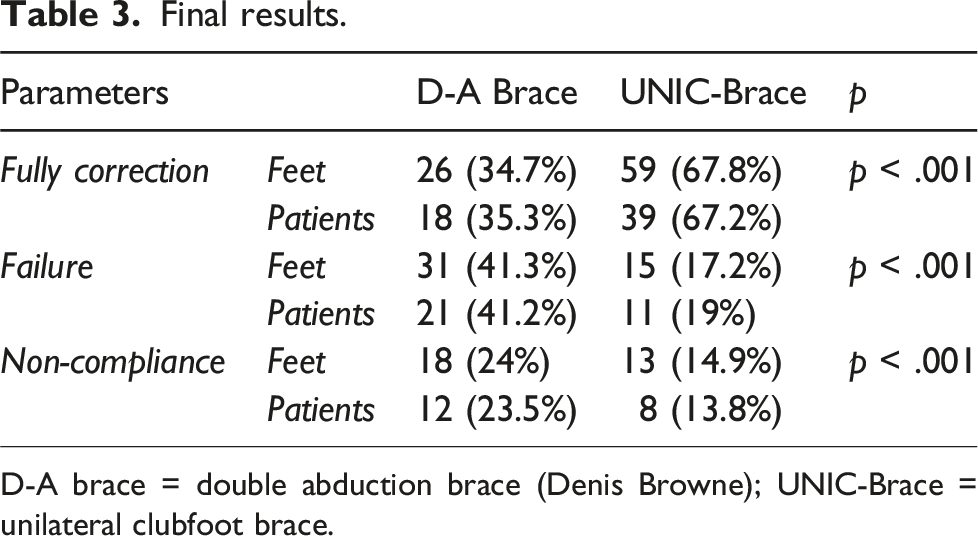
D-A brace = double abduction brace (Denis Browne); UNIC-Brace = unilateral clubfoot brace.
Questionnaire of satisfaction results. 22

*Good = normal foot and very satisfied family; **Regular = almost normal foot, satisfied family; ***Poor = Altered or very altered foot, dissatisfied family with the treatment.
Discussion
Ponseti recognized that congenital clubfoot intrinsically tends to recur and emphasized the importance of using the D-A brace to prevent relapses. 1 A systematic review has revealed that approximately 30% of 2206 children treated for clubfoot experienced a relapse. 3 In addition to this inherent propensity for relapse, 11 the recurrence rate increases with poor adherence to bracing programs.4,9,27–29 Many factors may contribute to poor adherence to orthotic use, such as cultural stigma, financial challenges, parental belief that correction has been achieved, and concerns regarding aesthetics and discomfort.2,30,31 Moreover, these challenges may intensify in low-income areas and regions with limited education. 30
Strategies have been proposed to enhance commitment to brace use, focusing on educating parents and healthcare professionals and ensuring effective communication.2,32,33 However, challenges persist in achieving optimal compliance with bracing protocols, reinforcing the need for continued research and innovative approaches to manage orthosis adherence. 34 The D-A brace restricts movement caused by the binding of the lower limbs, leading to difficulties in breastfeeding, transporting, and child caring. Therefore, unilateral orthoses have emerged as an attractive option. However, the primary limitation of such orthoses is their low effectiveness. In 2011, Janicki et al. 35 tested a standard ankle foot orthosis (AFO) and reported that it was inadequate in preventing recurrence. Other studies have documented similar outcomes using different models of unilateral braces.15,29,36 A recent review has concluded that the evidence supporting the use of unilateral limb orthoses to maintain clubfoot correction is insufficient. 3 Conversely, good results and better adhesion have been reported with specially designed unilateral braces.16–19 However, some models may have additional features that increase costs, thereby limiting their widespread use in developing countries.4,14 This aspect is critical because, globally, approximately 100,000 children are born annually with clubfoot, 80% of whom live in low- and middle-income countries. 30
This study outlines the development of an efficient brace that stands out for its reproducibility in standard orthopedic offices and affordable prices. The model has unique features, including knee movements and specific foot positioning in slight dorsiflexion and abduction, coupled with support over the lateral aspect of the talus. This design replicates the final position of the foot during Ponseti casting. Foot abduction aligns with Ponseti’s philosophy by promoting stretching of the medial soft tissues, an aspect that is crucial for preventing recurrence.1,35 Moreover, the brace includes two flaps enveloping the femoral condyles, ensuring stability and preventing the leg from rotating within the brace. This innovative combination of features enhances the effectiveness of clubfoot correction, making it a promising option in orthopedic care. Based on the administered questionnaire, the families expressed higher satisfaction with the unilateral orthosis model compared with the other model. A lack of parental or caregiver support is important as it may lead to irregular attendance in routine assessments, potentially leading to the abandonment of follow-up care. However, this orthosis immobilizes the ankle, which may contribute to calf muscle atrophy, a concern considering the pre- existing muscle abnormality in clubfoot. 4
One strength of this study is that we established a control group represented by patients treated with the traditional D-A brace in the same period and under similar circumstances as the test group, thus allowing a reliable analysis. However, we only reported short-term results. To date, the recurrence rate of clubfoot over time has not been determined, making it challenging to establish a definitive follow-up period for determining outcomes. In 2017, Sangiorgio et al. 37 analyzed timeline relapses in corrected clubfoot using a survivorship analysis. They have reported that the incidence of relapse was approximately 30% at 2 years, increasing to 45% at 4 years, and further to 52% at 6 years. By contrast, Agarwal et al. 3 observed that relapses tended to slow over time.
Additionally, consensus regarding the criteria for evaluating treated clubfoot is lacking. Some studies utilized scoring systems,17,19,36 whereas others considered clinical attributes such as plantigrade foot, deformities, flexibility, gait, and ease of fitting shoes. 35 Each system has strengths and limitations. In this study, Pirani scoring was applied to ensure the homogeneity of the two populations at treatment initiation and to monitor the progress of correction during the casting phase. However, when interpreting the final outcomes, we relied on clinical criteria 35 and caregivers’ opinions. Many authors do not incorporate radiographs in early evaluations because of inconsistencies in the various angles drawn on radiographs compared with normal ranges and anatomical deformations. 3 Nevertheless, radiographic examination can be valuable for studying the shape of the talar dome. This is an iatrogenic deformity arising from forced dorsiflexion caused by an inadequate plaster casting or orthosis.15,38
Although this study’s experience with the UNIC-Brace has been favorable, a weakness of the study was that patients were not randomly assigned to the groups; instead, the choice of brace depended on the available model at the time of the initial indication. In cases where both types of orthoses were available, some parents may have preferred a specific model. A randomized study comparing dynamic orthosis with a traditional brace would accurately assess the outcomes. Moreover, some bias favoring the new orthosis may have existed owing to the non-blinded evaluation.
Nevertheless, the study findings suggest that compared with the traditional D-A brace, the tested brace emerges as a promising alternative to traditional boots and bars for managing clubfoot. However, further mid- and long-term follow-up studies are needed to confirm these findings.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.