
Abstract
Objectives
The Ponseti method has led to vast improvements in outcomes for infants born with clubfoot deformity, but challenges with compliance during the bracing phase of the protocol remain. Unilateral braces promise higher compliance but often have led to unacceptably high recurrence.
Methods
We have developed a novel unilateral brace for clubfoot deformity that strategically applies patient-specific, anatomically-targeted forces to the lower limb to maintain correction. We retrospectively reviewed the cases of 26 patients with minimum follow-up of 24 months. The data were analyzed for recurrence rates, caregiver-reported compliance, and differences in Pirani score, dorsiflexion, abduction, hindfoot eversion, and resting rotation between initial and final follow-up.
Results
Most patients (N = 23, 88%) were compliant with the bracing protocol. Two patients showed recurrence of deformity (8%). There were statistically significant improvements in Pirani score, dorsiflexion, abduction, hindfoot eversion, and resting external rotation. A subset of patients with sub-optimal correction at baseline showed improvement in all parameters across the course of bracing.
Conclusions
This novel unilateral brace for maintenance of clubfoot correction after Ponseti treatment demonstrates rates of recurrence rates and caregiver-reported compliance at 2 years of follow up that are comparable to outcomes with traditional bilateral foot abduction orthoses.
Introduction
The Ponseti method is the international gold standard for correction of idiopathic clubfoot.1–3 The Ponseti method has four stages: serial manipulation, a specific technique of cast application, percutaneous Achilles tenotomy, and finally the use of a foot abduction orthosis (FAO) to maintain the correction of the deformity. 4 The FAO has traditionally been made of open-topped shoes connected by a rigid bar, which hold the feet in external rotation and dorsiflexion. 5
If the protocol is adhered to correctly, recurrence of deformity requiring surgical intervention occurs in about 12% of patients.6–8 However, parental compliance with the bracing protocol is a challenge, with non-compliance ranging from 8 to 49%.6,8–11 Non-compliance can result in recurrence rates as high as 48% 6 ; it is a stronger predictor of recurrence than severity of the deformity at birth. 12
In order to improve compliance, several groups have created unilateral orthoses purported to achieve the same outcomes as the FAO, but with improved patient comfort. Several of these attempts resulted in improved compliance but unacceptably high rates of recurrence, ranging between 31% and 83% recurrence of deformity.13–15 However, two recent studies described unilateral braces that achieved outcomes comparable with the traditional FAO. Specifically, Adachi et al. demonstrated a unilateral brace with 13% recurrence and 95% compliance across 5 years of follow-up 16 and Berger et al. demonstrated a unilateral brace with 14% recurrence and 91% compliance across 7 years of follow-up. 17
Comparison of unsuccessful and successful unilateral braces reveals that it is not sufficient for a unilateral brace to simply hold the foot in its corrected position; this results in high recurrence. 15 Rather, direct application of abduction and dorsiflexion forces to the appropriate areas of the foot is required for successful maintenance of correction.16,17 Additionally, the brace must have an anchor point above a flexed knee in order to correct tibial torsion; an ankle foot orthosis is not sufficient.5,13,18
Despite the potential that a carefully designed unilateral brace holds for achieving both high compliance and low recurrence, only the two studies mentioned above have described successful unilateral braces. Therefore, our group has developed a new brace that meets the criteria for a successful unilateral orthosis, the Dynamic Torsional Knee Ankle Foot Orthosis (DTKAFO). The goal of this study was to describe the DTKAFO and present the results of a retrospective study of 26 patients who have used the DTKAFO for a mean follow-up of 30.1 months.
Methods
Description of the patient cohort
Between 2015 and 2020, 112 patients (154 clubfeet) were treated for bracing with the DTKAFO at Cunningham Prosthetic Care in Saco, Maine after casting according to the Ponseti method19,20 (Figure 1). All patients and their orthopedic teams were based at various locations throughout the continental United States. The 112 cases were reviewed as a retrospective cohort study. This study was approved by the Messiah University Institutional Review Board, protocol 2017–059. Flowchart describing the patient cohort and selection process. FAO+DTKAFO indicates patients who used a foot ankle orthosis before switching to the dynamic torsional knee ankle foot orthosis (DTKAFO). DTKAFO indicates patients who began using the DTKAFO directly after casting.
Nine patients were excluded because they had non-idiopathic clubfoot. Of the remaining patients, 26 patients (34 feet) had a minimum follow-up with Cunningham Prosthetic Care of 24 months and were included in this study. Mean follow-up was 30.1 months (range: 24–40 months). Mean age at follow-up was 3.0 years (range: 2.3–4.5 years). No patients were lost to follow-up. All patients had been treated according to the Ponseti method prior to presentation.
Of the 26 patients, 16 patients (22 feet) had used a foot abduction orthosis (FAO) under the supervision of another provider for bracing prior to switching to the DTKAFO. Use of the FAO was discontinued at the initiation of DTKAFO treatment. This cohort is referred to as FAO+DTKAFO. The most common reasons for switching reported by parents were distress or discomfort of the child in the FAO, sleep issues in the FAO, and/or desire for their child to use an orthosis that did not restrict use of the unaffected limb. Period of prior use of an FAO ranged from 1 week to 9 months, (mean: 3.9 months). All FAO+DTKAFO patients used the DTKAFO for at least 24 months (range: 25–40 months), supporting an assumption that bracing outcomes observed in this cohort can be attributed to the DTKAFO rather than to initial use of the FAO. The remaining 10 patients (12 feet) began bracing with the DTKAFO immediately following casting. This cohort is referred to as DTKAFO.
Baseline characteristics of patient groups.
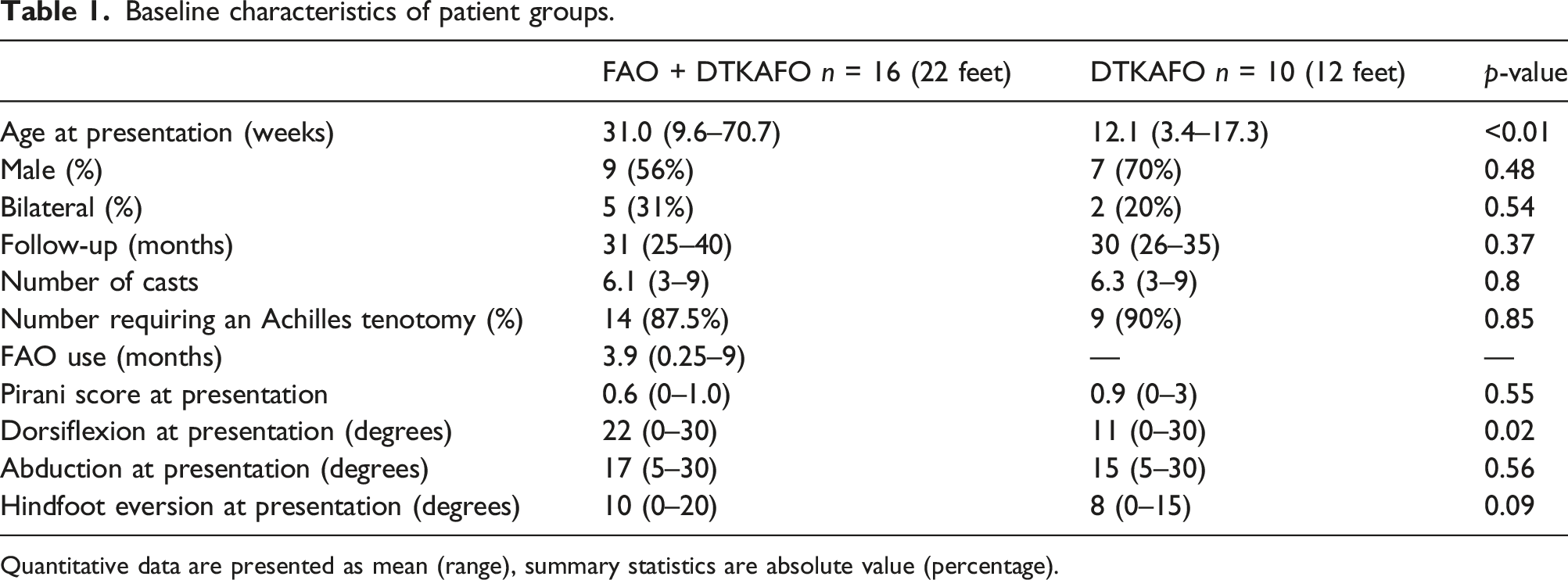
Quantitative data are presented as mean (range), summary statistics are absolute value (percentage).
Measurements
Patients were evaluated at Cunningham Prosthetic Care for Pirani score and range of motion of the foot and ankle at the initial visit and at all in-person follow-up visits. Pirani scoring was accomplished following standard protocols. 21 Per the Pirani system, values greater than zero indicate sub-optimal correction. 21 Dorsiflexion of the ankle was measured relative to the axis of the anterior tibia by passively dorsiflexing the ankle with the knee flexed at 90°. Forefoot abduction was measured relative to a bisector of the calcaneus by holding the hindfoot stable and rotating the forefoot laterally in the transverse plane. Hindfoot eversion was measured relative to the lower one-third of the leg by holding the ankle stable and everting the heel. External resting rotation was measured by visualizing the foot from the plantar aspect aligned with the axis of the tibia with the knee in 90 degrees of flexion, a bisector of the heel was compared with the axis of the femur to assess the relative angle of rotation in the transverse plane.
The dynamic torsional knee ankle foot orthosis
The DTKAFO is made from 4- to 6-millimeter-thick polypropylene with low-profile steel and aluminum fasteners, a plantar spring-steel strip (0.028–0.042 inch thickness), hook-and-loop straps, and foam padding (Figure 2). The DTKAFO consists of three molded thermoplastic components: the thigh component, the helix component, and the foot component. The dynamic torsional knee ankle foot orthosis (DTKAFO). A. Patient wearing the DFKATO. B. Frontal view of the DTKAFO. 1) Helix component, 2) Midfoot hook-and-loop fastener strap C. Transverse superior view. 3) Thigh component, 4) Thigh hook-and-loop fastener strap D. Transverse inferior view. 5) Foot component, 6) Stainless steel bar.
The neutral position of the DTKAFO is 90o of knee flexion, 40° of forefoot abduction, 10° of dorsiflexion, and 15° of hindfoot eversion. These parameters are adjustable by the clinician based on the patient’s presentation. Due to the flexibility of the polypropylene, the patient is able to move the limb away from the neutral position, but meets increasing resistive force as he does so. The spring steel is stiff, reinforcing the brace along the axis of the plantar surface of the foot, while still allowing some motion as described below. By the combined forces of the polypropylene and the spring steel, the DTKAFO acts to restore the foot to the neutral position, which is the fully corrected position specified by the Ponseti protocol. 22
The thigh component of the DTKAFO is secured around the patient’s thigh proximal to the femoral condyles using an inelastic, padded strap. The thigh component is attached to the helix component distal to the lateral condyle via metal fasteners that can be adjusted along the vertical axis to accommodate increasing leg length of the patient.
The helix component is a spiral of plastic that travels around the tibia circumferentially and ends at the heel cup, which completely surrounds the posterior calcaneus. The heel cup is attached to the plantar surface of the foot component via the spring steel bar.
The DTKAFO is sized to each patient such that the axial length of the helix is half an inch shorter than the tibial length. Therefore, when the DTKAFO is donned on a patient, the helix is stretched and untwisted slightly in order to secure the thigh component proximal to the condyles of the knee. Thereby, the donned brace exerts an abductive rotational force and a compressive axial force which creates a simulated ground reaction force as the “spring” of the helix seeks to return to its neutral position. Details of the forces exerted by the DTKAFO are presented below and in Figure 3. Design of the DTKAFO. A. Superior view of the DTKAFO showing abductive force (1), talar counterpressure force (2), and external rotation force (3). B. Medial view showing dorsiflexive pressure (4), dorsiflexive force on the distal calcaneus (5), and molding of the heel cup to prevent heel slip (6). C. Posterior view showing eversion pressure on the subtalar joint (7) and heel valgus (8).
The rotational and axial forces are delivered from the helix to the foot component via the stainless-steel bar. The abductive rotational force is directed to the medial aspect of the first metatarsal. The elastic midfoot hook-and-loop fastener strap applies a medially-directed counterpressure on the head of the talus to counter the cavovarus aspect of the deformity and encourage abductive range of motion of the forefoot. The knee is held in a flexed position, allowing the rotational force to work without over-pressurization of the hip joint.
The axial compressive force of the distracted helix acts on the plantar surface of the midfoot and forefoot through the plantar forefoot section to dorsiflex the talocrural joint. Anatomical contouring of the proximal foot component corresponding to the proximal longitudinal arch applies an upward force on the plantar aspect of the distal calcaneus to aid dorsiflexion at the subtalar joint. The rear portion of the heel cup curves around the upper part of the posterior surface of the calcaneus, preventing the heel from slipping out of the brace.
The inferomedial portion of the heel cup is molded and padded in such a way that it applies pressure at the posteromedial calcaneus to rotate the calcaneus into eversion at the subtalar joint. The talus, navicular, and cuboid follow the calcaneus into abduction. The calcaneus is stabilized by the heel cup, which is molded to hold the calcaneus in valgus. Further stability of the calcaneus and midfoot is encouraged by the hook-and-loop fastener strap that wraps gently around the midfoot. The midfoot strap is not needed to keep the foot in the brace; rather, the distracted helix exerts an upward and medial pressure that cradles the foot within the foot component.
Following assessment of the severity of the deformity and measurement of the patient’s limb, the DTKAFO is customized to address the patient’s presentation. The thickness of the polypropylene and the width of the helix are calibrated to provide the appropriate level of rotational force. The spring steel cross-section and the angle of dorsiflexion are calibrated to provide the appropriate level of dorsiflexion force. Padding is provided to focus the necessary forces on the forefoot and on the proximal medial and lateral arches.
Treatment regimen
All patients were followed by an independent orthopedist. Each patient’s orthopedist directed the course of treatment with the DTKAFO, including determining when treatment should be concluded. Treatment began with a 7-days period of initialization that gradually increased the time in the orthosis until the appropriate amount of time was reached, based on the patient’s age (see Supplement Material for details). The DTKAFO was prescribed for full-time use (23 h per day with a 30-minute break in the morning and evening) until the child demonstrated pull-to-stand activity. Then increasing time out of brace up to 6 hours per day was allowed for active play. When the child was ready to begin ambulating, brace wear was reduced to nights and naps. The DTKAFO is designed to allow for multiple adjustments to accommodate growth during usage. Many of these can be accomplished by the parent when directed to do so by the orthotist.
It was important that the patient’s caregiver gained comfort in putting the brace on their child in the clinic. Therefore, the caregiver was instructed in proper donning of the brace. The caregiver’s proficiency was evaluated at a follow-up visit 24 h after the initial visit. Caregivers were given clinic contact information and instructions on how to manipulate the foot to demonstrate range of motion and how to take a series of four specific, informative photographs. These photographs were used to supplement SkypeTM consultations with a Cunningham Prosthetic Care clinician if the caregivers had questions or concerns about brace use or fit. Patients were followed by Cunningham Prosthetic Care at 1 week after initial fitting, at 1 month after this, and then at two-to-three-month intervals until treatment was concluded. Follow-up visits were conducted either in-person at Cunningham Prosthetic Care or via SkypeTM. For in-person follow-up visits, measurements were taken by the orthotist. For SkypeTM follow-up consultations, measurements were taken by the clinician based on photos of the parent or caregiver positioning and/or stretching the foot according to specific instructions provided by the clinic. These measurements were visually confirmed by the orthotist during the SkypeTM follow-up consultation. Clarification on any unclear measurements was achieved by deepening the detail and level of instruction during SkypeTM consultations as necessary.
Non-compliance was defined as incomplete adherence to the bracing protocol, defined as decreased wear time or incorrect brace wear. Decreased wear time was defined as any deviation from the protocol-recommended wear time and was documented at each follow up based on verbal reporting by the parent or caregiver. Incorrect brace wear was evaluated by the treating provider and documented at each follow-up based on how the brace was donned.
Statistical analysis
For baseline patient characteristics, quantitative data were reported as mean (range) and qualitative data were reported as absolute and relative frequencies. Data violated the assumption of normality according to Shapiro Wilks test. Comparisons between FAO+DTKAFO and DTKAFO group baseline characteristics were made using Mann Whitney U test and Chi-square test for binomial data. Comparisons between baseline and final follow-up for dorsiflexion, abduction, hindfoot eversion, and resting external rotation were made using pairwise Mann Whitney U tests. Comparison of relative change across parameters was made using Kruskal-Wallis test with follow-up Mann Whitney U tests. Statistical significance was considered at p < 0.05. All statistical analyses were performed using R 4.0.2 (R Foundation for Statistical Computing, Vienna, Australia).
Results
Outcomes
Clinical data on the 26 patients.

Compliance
Non-compliance with the DTKAFO was self-reported by the caregivers of three patients (12%). Two of the non-compliant patients were Case 1 and Case 13, as mentioned above. The caregiver of the third non-compliant patient reported a period of decreased brace wear time when the patient was aged 15–20 months. However, the caregiver resumed adherence to the treatment protocol in the next 7 months of treatment (patient age 20–27 months). This patient did not experience recurrence of deformity.
No patients experienced skin blistering or skin breakdown during use of the DTKAFO. Mild erythema was observed in several patients at the medial aspect of the first metatarsophalangeal joint, at the interphalangeal joint, and at the lateral thigh and calf where the de-rotational counter force is applied. When erythema occurred, patients were advised to temporarily reduce wear times until the inflammation subsided, which took on average approximately 2 weeks.
Analysis
Pirani score, ankle dorsiflexion, forefoot abduction, and hindfoot eversion were compared between the baseline and final follow-up for each patient in the cohort, with the final follow-up defined as the latest visit recorded in the data set, since many of the patients had not yet concluded bracing. All groups were non-normal according to Shapiro-Wilks test.
Pirani score was significantly reduced at final follow-up compared to baseline, from 0.5 to 0 points (p = 7.6*10−9) (Figure 4(A)). Dorsiflexion, forefoot abduction, and hindfoot eversion were significantly increased from 17 to 23° (p = 1.7*10−12), 16–21° (p = 1.0*10−9), and 9–13° (p = 1.4*10−9), respectively (Figure 4(B)). External resting rotation was significantly decreased from 20 to 5° reflecting the change from post-casting resting rotation to an appropriate anatomical resting position at conclusion (p = 0.008). Comparison of patient data at baseline and final follow-up. A. Pirani score comparison. B. Dorsiflexion, forefoot abduction, and hindfoot eversion range of motion, and resting external rotation comparison. N = 34 feet. Data presented as median ± standard error of the mean. * indicates p<0.05 between baseline and final follow-up.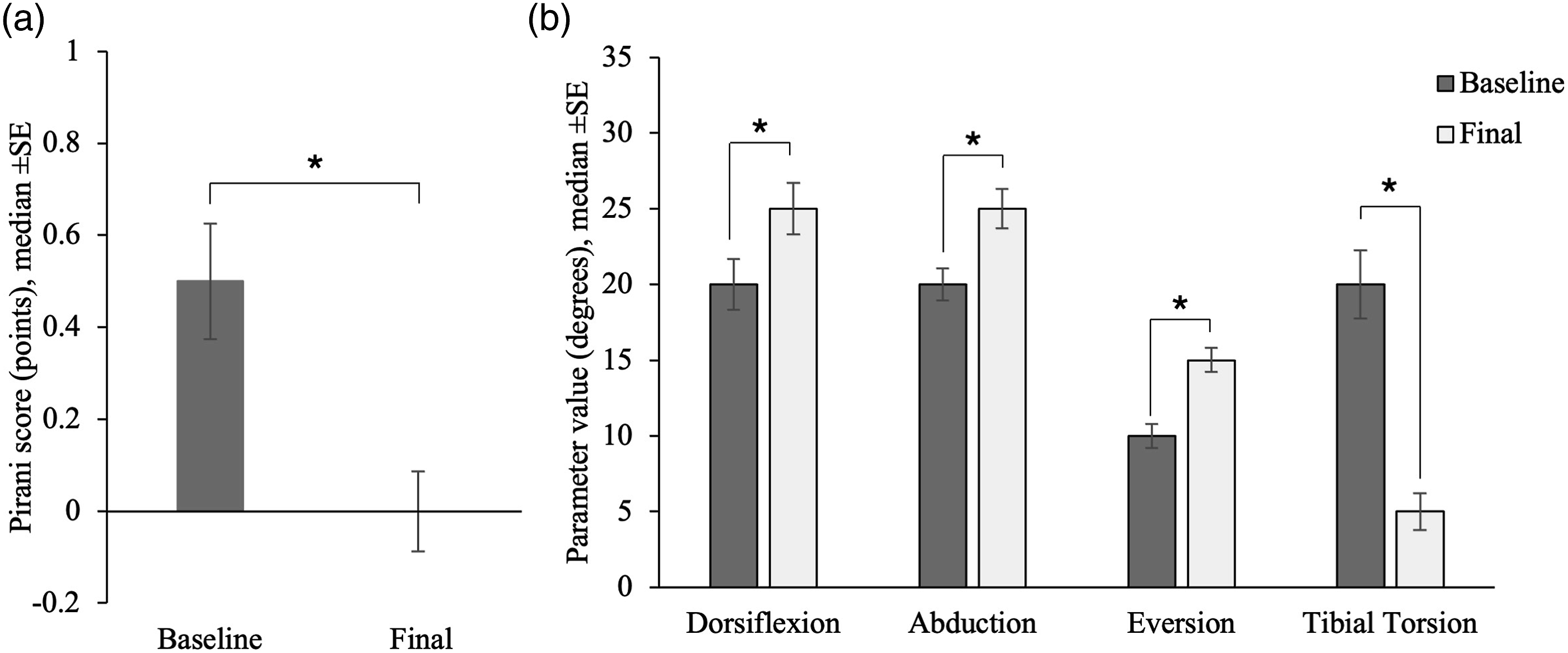
In order to assess the influence of the statistically significant difference in dorsiflexion at baseline between the FAO+DTKAFO and DTKAFO groups, we analyzed each of these groups separately. The FAO+DTKAFO and DTKAFO groups had a median gain in dorsiflexion of 5.0 ± 4.3 and 5.0 ± 5.4°, respectively. Both were statistically significant increases, indicating that both groups were similarly influenced by the DTKAFO despite differences in dorsiflexion at baseline.
Change from baseline to final follow-up for feet sub-optimally corrected at baseline.

All parameters showed improvement from baseline to final follow-up (Figure 5). There was no significant difference in normalized gains across parameters. Pirani score and eversion showed the greatest gains, with 100% median normalized gain in both parameters. This indicated that in these parameters, the median improvement across the course of treatment was equal to 100% of the patient’s deficit at baseline, bringing them to optimal correction at final follow-up. Normalized gains in feet that were sub-optimally corrected at baseline.
Discussion
The most significant finding of this study is the high caregiver-reported compliance (88%) and low recurrence (8%) achieved with our novel unilateral brace, the DTKAFO. The 88% caregiver-reported compliance demonstrated herein is comparable to the strongest results from studies utilizing a traditional FAO, which range from 92% compliance at best 10 to 51% at worst. 23 Similarly, the 8% recurrence shown here is comparable with the lowest recurrence results from recent FAO studies of similar follow-up periods. 10 It is well known that compliance and recurrence are linked, 24 which explains why the strong compliance reported here was accompanied by low recurrence of deformity.
Further, in the majority world where clubfoot is most prevalent, compliance can be difficult due to the cultural stigma against physical deformity, which makes the bulky appearance of the traditional FAO particularly challenging for parents. Cultural pressure against the wearing of an orthosis has been reported in sub-Saharan Africa,1,25 South America,26,27 and India 28 among others. The slim, unilateral design of the DTKAFO makes it an appealing option for parents in the majority world who wish to complete the bracing protocol discreetly, thereby reducing the stigma against their child and likely improving compliance.
Our group has recently begun investigation of implementation of the DTKAFO at the African Inland Church CURE International Hospital in Kijabe, Kenya, to explore the use of the DTKAFO in the cultural context of East Africa. We note that there are some challenges related to fabrication of the DTKAFO in this setting. First, the quality of available materials can be variable, particularly the polypropylene sheets and the spring steel. Second, orthotists require special training in the fabrication of the DTKAFO, but this is the case even for the more commonly used Steenbeek brace. These challenges may be overcome as the DTKAFO is more commonly used or if it is able to be mass-produced. Our group is investigating the feasibility of 3D printing and injection molding as strategies for mass production.
One of the most common reasons given for non-compliance in non-majority world patient populations is inconvenience.23,24 Indeed, the connecting bar of the FAO makes simple childcare tasks like changing a diaper or buckling the child into a car seat more difficult. These issues are alleviated by the DTKAFO’s unilateral design and could in part explain the high caregiver-reported compliance rates shown in this study. There may also be some selection bias due to the fact that parents who seek out the DTKAFO have done so because they are particularly committed to finding a unilateral brace for their child. Therefore, these parents may represent a segment of the population that is more likely to comply with any bracing protocol.
We report statistically significant improvements in Pirani score, dorsiflexion, abduction, and hindfoot eversion. We speculate that this is because the unique and dynamic design of the DTKAFO results in a gentle, persistent stretch being applied in all three planes during wear, causing the brace to act as if it is an extension of the casting process in which the orthopedist gently stretches and molds the foot into the corrected position over a series of casts.
It is important to note that our study has several limitations. First, we used no severity classification system because 62% of our patients (N = 16) were treated previously with an FAO for 1 week to up to 9 months and only began use of the DTKAFO as a second type of treatment. We know from parent report the number of castings performed, but we do not know the precise number or type of manipulations. Notably, we see no significant differences between groups at presentation, except for age and dorsiflexion, which were both higher in the group previously treated with an FAO. All patients were treated with the DTKAFO for at least 24 months, in contrast to the relatively short time periods of FAO use (mean of 3.9 months), supporting an assumption that bracing outcomes observed in this cohort can be attributed to the DTKAFO rather than to initial use of the FAO. In addition, we detected statistically significant improvements in Pirani score, dorsiflexion, abduction, and eversion between the beginning and end of DTKAFO treatment across the patient cohort. This suggests that patient outcomes are directed by the DTKAFO.
Second, our sample size is 26 patients, which is comparable to similar studies in the literature,13,15,16,18,29 but does restrict our ability to generalize these findings. It is our goal to utilize these findings, which are from a retrospective cohort, to inform the design of a larger-scale prospective study of the DTKAFO in partnership with hospitals in the majority world.
Third, our mean follow-up was 31 months, which is comparable to the literature,8,30,31 but some studies report that recurrence in patients using unilateral orthoses becomes apparent only with longer-term use. 14 However, two recent studies of unilateral orthoses have shown good results (<15% recurrence) with follow-up periods of five 17 and seven 16 years. Therefore, these results are useful as an early outcome that may or may not be predictive of long-term results with the DTKAFO unilateral brace.
Conclusions
The DTKAFO represents an innovative approach to the bracing phase of clubfoot treatment after Ponseti casting. The helix design applies a regime of targeted forces to precise anatomical locations on the patient’s lower limb. The results presented here demonstrate that in a group with a minimum of 2 years of follow-up, using the DTKAFO for bracing results in 88% caregiver-reported compliance and 8% recurrence with statistically significant improvements in range of motion of the patient’s foot and ankle.
Supplemental Material
Supplemental Material - Two-year retrospective cohort results on use of a dynamic unilateral brace for treatment of clubfoot: Can compliance and prevention of recurrence both be achieved?
Supplemental Material for Two-year retrospective cohort results on use of a dynamic unilateral brace for treatment of clubfoot: Can compliance and prevention of recurrence both be achieved? by Emily J Farrar, Michelle Lo, Luke Groothoff, Jerald Cunningham and Joseph Theuri in Journal of Rehabilitation and Assistive Technologies Engineering
Footnotes
Acknowledgements
We acknowledge the invaluable contributions of America Cervantes, Rebekah Forshey, Tim Howell, Luke Redcay, Scott Reichenbach, and the teams at HopeWalks and CURE Clubfoot Kenya.
Author’s Note
Jerald Cunningham reports that he is directly employed full-time by Cunningham Prosthetic Care, the company that is the primary manufacturer and distributor of the Dynamic Torsional Knee Ankle Foot Orthosis (DTKAFO).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.