
Abstract
Introduction
The successful integration of socially assistive robots in geriatric care settings hinges on the attitudes and opinions of healthcare professionals. This study explored their needs, expectations, and perceptions regarding robot use, including facilitating factors and barriers to implementation.
Methods
Twenty professionals participated in semi-structured interviews that covered topics such as robot applications, perceived value, acceptance criteria, prerequisites for deployment, ethical considerations, and design attributes. These interviews were analyzed using a deductive qualitative approach guided by the European Network for Health Technology Assessment model (version 3.0).
Results
Results indicated that professionals generally viewed robots favorably, noting their usefulness in various non-intimate tasks like meal assistance and toileting. Ease of use was identified as a critical factor for robot adoption in geriatric care. Furthermore, the necessity of educating all stakeholders and providing comprehensive training to professionals emerged as essential for successful implementation. The discussions also included financial and ethical issues related to the introduction of these technologies.
Conclusion
These findings will contribute to develop guidelines for designing and deploying socially assistive robots that align with the preferences and requirements of geriatric care professionals.
Keywords
Introduction
Globally, the aging population has led to a marked increase in certain age-related diseases, such as Alzheimer’s disease and related disorders, stroke, among others. 1 These conditions often result in a loss of independent functioning, necessitating daily support within specialized facilities like nursing homes, senior residences, and geriatric care units, or through home-based services such as home hospitalization, care, and assistance.
Providing effective and quality care to dependent older adults or those at risk of dependency represents a significant challenge, especially amidst a strained healthcare landscape characterized by nursing staff shortages, a limited number of general practitioners, and crises like the COVID pandemic. Consequently, it is crucial to innovate and develop approaches that maximize older adults’ independence and mitigate the impacts of age-related conditions, including cognitive impairments, sensory deficits, mobility issues, imbalance, and mental health disorders such as anxiety and depression. 2
Socially assistive robots (SARs) are engineered entities designed to engage socially (through speech, gestures, and behaviors) with users, serving various purposes including informational, therapeutic, recreational, educational, and logistical functions. Since the late 2000s, extensive research has explored the application of social robotics within geriatric care. 3 Some researchers argue that SARs offer a viable solution to the challenges posed by an aging population. 4 These tools have the potential to enhance the well-being 5 and the overall care of OAs in care facilities. 6 SARs could play the role of “coach” or facilitator, initiating personalized interactions to maintain OAs motivation to engage in physical and social activities, or for daily activities i.e., reminding to use eyeglasses or to take medication.7,8 SARs also offer promising possibilities for supporting caregivers in their tasks and alleviating their daily workload, in a highly strained organizational context. 9 In addition, SARs could be used to contribute to the educational effort needed to apply barrier gestures during epidemics (COVID-19 type). 10
SARs can adopt humanoid (resembling humans), animaloid (resembling animals) or machinelike designs. 11 Those designed for assistive purposes often resemble mobile platforms that can navigate in space. Some models incorporate screens to facilitate access to diverse services and content, including telepresence robots that allow individuals in different locations to communicate effectively. 12 Despite growing interest in SARs, their capabilities beyond therapeutic applications—such as providing information, orientation, entertainment, and practical support—remain underexplored. 13 Moreover, comprehensive analyses addressing the full spectrum of clinical, technical, social, organizational, and economic considerations in deploying robots within care settings are scarce.
In the ROBOTONOMIE project, a French research program, we aimed to develop a SAR system to support both, professionals working in geriatric institutions (i.e., nursing homes, long-term care units, etc.) in their tasks, and OAs who live in these facilities. This project intended to draw up a set of specifications covering the various technological functionalities to be developed for a SAR that could be used specifically in geriatric settings. In order to develop a solution adapted to the context in which it will be implemented, this work was based on a participative design methodology 14 for gathering user requirements, designing and then experimentally evaluating SARs use-cases. This kind of approach has been used in other studies in the field (social robots and geriatrics) that have demonstrated the interest of integrating relevant stakeholders, such as OAs and caregivers, for the definition of new conceptualizations and design guidelines for SARs.15,16
In the present study, we have investigated the expectations, needs and proposed use-cases for a SAR of professionals working in geriatric settings. Analyzing the perspectives and attitudes of these professionals is crucial for two main reasons: they are the prospective primary users of such robots, and their stance towards SARs significantly influences older adults’ acceptance of these technologies within care institutions, thus affecting their successful and meaningful deployment. 17
The study has also examined the facilitators and barriers to the implementation of SAR in these institutions. To understand these factors in the context of geriatric institutions, we used a multidimensional analysis model used in the field of Health Technology Assessment (HTA).18,19 This type of model makes it possible to systematically analyze the clinical, organizational, technological, economic, and legal issues associated with the implementation of a new technology in the healthcare field. This analytical framework makes it possible to assess the overall value of a healthcare technology (i.e. its properties, effects, and repercussions during implementation).
Methodology
Study design
This qualitative study was based on semi-structured interviews with healthcare professionals working in geriatric facilities (France) between June and October 2023.
Participants
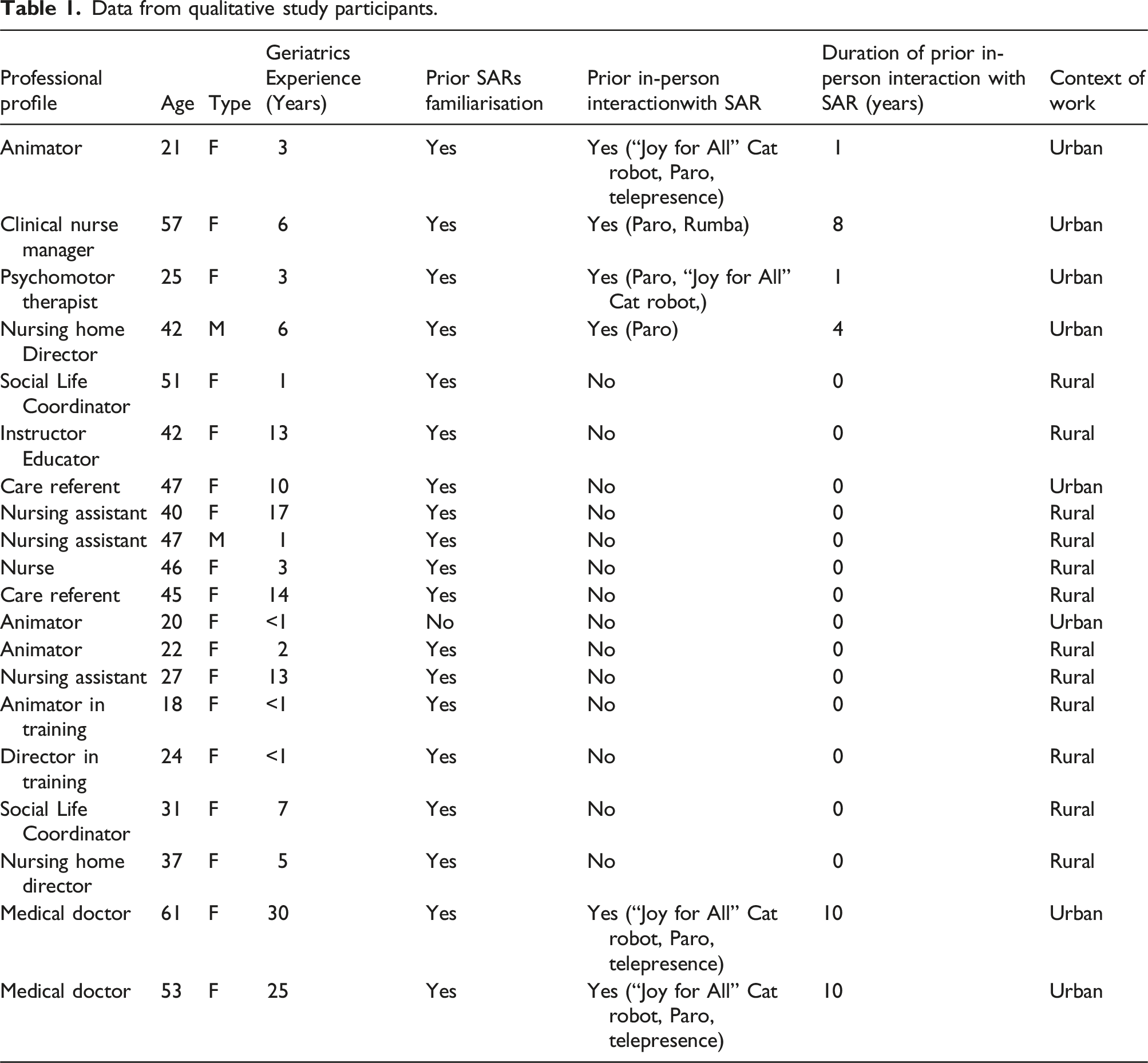
Data from qualitative study participants.
Ethical and regulatory aspects
Before the interview, participants were provided with both oral and written information outlining the study’s goals, associated risks, anticipated benefits, and their confidentiality rights. Each participant gave their oral consent and signed a consent form in two copies. The Paris Region Geriatric Hub Research Ethics Committee (CEGIF N° 2023–22) granted ethical approval for this study.
Material
Video material
To set the stage for the interviews, a video compilation was created showcasing various SAR applications with older adults. This visual aid enabled professionals to witness firsthand how real robots interact with actual users and to explore diverse robot designs. Featured applications of SARs included video conferencing, fall monitoring, motor and cognitive stimulation, entertainment (such as videos and games), logistics, teleconsultation, and delivery services. SAR models highlighted in the video material encompassed Cutti, Miroki, Geminoid F, Nao, Paro, Pepper, Ruby, Ubbo, Stevie, and Ubbo Vita.
Interview guide
Guide for the semi-structured interviews with geriatric care professionals.

Procedure
The interviews were facilitated by two researchers (SD, CH), who engaged with healthcare professionals, support staff, and management team members across each nursing home, conducting the sessions on-site. Interviews averaged 40 min in length (SD = 15), amassing a total of 800 min of dialogue. These conversations were recorded to ensure accurate transcription and analysis. The interview process was twofold: initially, participants were shown brief video demonstrations of SARs in operation. Following this visual introduction, the discussion moved to participants’ familiarity and prior experiences with SARs, guided by the structured interview format previously described.
Qualitative analysis
Professionals’ responses were categorized according to the European Health Technology Assessment model “EUnetHTA” (HTA Core Model® version 3.0) developed by the European Network of Health Technology Assessment. 20 This framework outlines a comprehensive method for evaluating the impact of health technologies, covering a wide range of aspects. Designed primarily to facilitate evidence-based decision-making through the systematic assessment of new health technologies, the model also serves research purposes, including data collection and analysis, provided its foundational principles are adhered to. 18
Evaluation areas of the EUnetHTA core model ® version 3.0. 19

To assess inter-rater reliability in coding the interviews, we employed a systematic approach involving two researchers (SD and ASR). Each researcher independently carried out a deductive thematic analysis of the interview content using the HTA Core Model® (version 3.0). The domains (level 1), subjects (level 2) and issues (level 3) of the EUnetHTA model, which correspond to a set of predefined codes, were used to guide the process of classifying and organizing the data in our study. In each interview, we first identified relevant data segments or an idea related to the various EUnetHTA domains (level 1). We then proceeded to an initial coding stage (i.e., labeling the data segments). We then analyzed the coded data (sentences or sets of statements) to classify them according to subject (level 2) and problem (level 3). We then performed the corresponding coding using the EUnetHTA nomenclature. A semantic approach was used to identify themes and codes using the explicit meaning of the data.
21
Following this, we compared the assigned codes to determine the level of agreement between the two raters. We calculated Cohen’s Kappa, a statistical measure that accounts for inter-rater reliability, resulting in a Kappa coefficient of 0.80. This value indicates substantial agreement between the two researchers. In instances where discrepancies arose, we facilitated discussions to resolve differences and refine the coding scheme as needed. This process ensured a consistent and reliable coding framework, thereby enhancing the validity of our study’s findings. Besides, some authors have previously emphasized the possibility of overlapping issues between topics in the HTA analysis. They have suggested to classify these overlapping issues in the most relevant topic section.
19
For the current study, the overlapping in the HTA coding was addressed by classifying each idea within the most or better fitting HTA dimension, topic and issue. During inter-rater discussions, this issue was formally addressed to ensure consistency and accuracy in the classification process. Figure 1 illustrates the process undertaken to address the issue of code overlapping. This type of thematic analysis using the EUnetHTA Core Model® framework, version 3.0 has been described in other studies.22,23 Process for addressing the HTA code overlapping issues.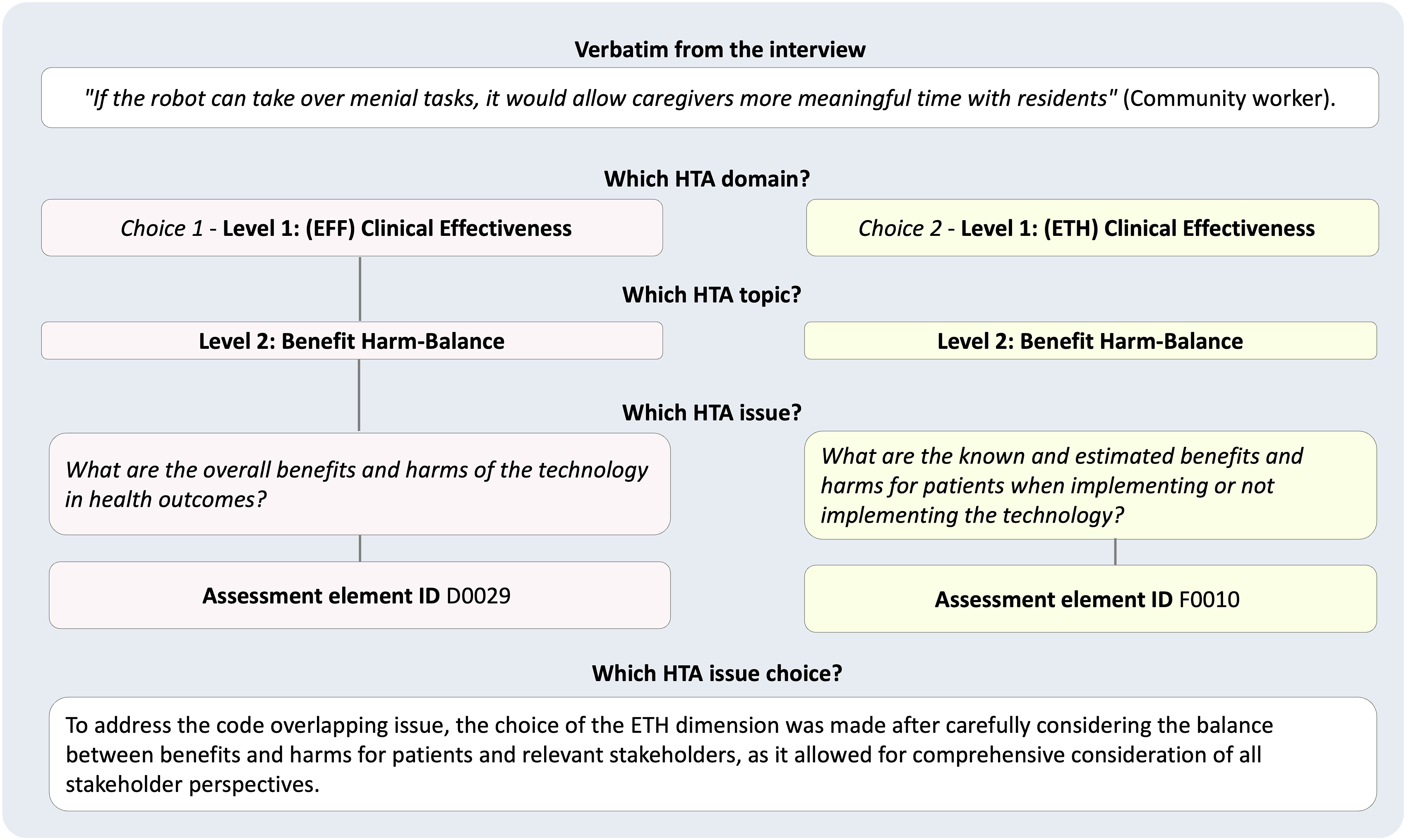
Finally, in order to explore how geographical context and prior exposure to robotic technologies influence professionals’ attitudes towards the integration of robots in elderly care, sub-analyses were conducted with the qualitative data, focusing on differences in professionals’ attitudes based on the context of work (urban or rural nursing homes) and on the level of previous experience with robots (familiarization or in-person interactions with robot) in their work settings. The analysis involved coding the verbatim responses according to these participant profiles, allowing for a detailed examination of how these factors impact perceptions and attitudes towards socially assistive robots in elderly care environments.
Results
Prior knowledge of social and assistance robots
Most of the professionals (19 out of 20, 95%) were acquainted with SARs, having encountered them in real-life scenarios (Table 1). For instance, the majority of participants had observed robots serving drinks or food to customers in nearby restaurants within their district. They had also watched documentaries and films showing how social robots could be used for patients and health professionals in medical settings. A subset of these individuals (6 out of 19) had in-person interactions with SARs. They had benefited from training in using robots, implemented interventions using these tools with residents and tested their impact on this population in the context of their work. One animator reflected, “We experimented with a small robot a few years back, and the outcome was quite positive, though we haven’t pursued it further since then.” One professional had no knowledge of robots, except a prior experience of watching some science-fiction films.
Qualitative multidimensional analysis using the HTA framework
In this section, the themes emerging from the qualitative analysis guided by the EUnetHTA conceptual framework are described. The themes are classified in each of the nine dimensions of the model, referring to the issue question and indicating the theme and the classification code of the EUnetHTA nomenclature in parentheses.
Dimension 1: Health problem and current use of technology (CUR)
What is the target population in this assessment? (Target population, A0007)
Professionals highlighted that SARs could serve all older adults within geriatric settings, with a special emphasis on individuals experiencing cognitive disorders, physical disabilities, and depression. Humanoid robots emerged as particularly fitting for those with significant neurocognitive disorders, like Alzheimer’s disease.
For which health conditions, and for what purpose is the technology used? (Utilization, A0001)
The professionals envisioned multifaceted roles for SARs, distinguishing several use-cases for direct care activities (i.e. tasks in which the resident is present): (a) Facilitating video conferencing to maintain connections with distant family and friends. (b) Disseminating information on nursing home events: “Imagine a robot navigating the hallways, reminding residents of their appointments or activities like, ‘Today at 2pm, don’t forget bingo is happening if you’re interested in joining…’ echoing the tradition of town criers” (animator). (c) Delivering items such as books, water, and meals directly to residents’ rooms. (d) Offering therapeutic and recreational engagements, including cognitive stimulation exercises and gentle physical activities. “Envision a mobile robot that could roam, playing music, cracking jokes, encouraging hydration, or facilitating video calls, addressing the gap in activity variety, especially crucial on weekends” (Nursing assistant).
Professionals also envisioned additional roles for SARs, including: • Broadcasting reminders for crucial daily tasks, like hydration. • Assisting residents in navigating the facility, whether finding their rooms or the location of activities. • Offering mobility support, especially for those in wheelchairs. “Imagine a robot guiding groups of residents, providing support for those with mobility challenges to lean on” (psychomotor therapist). • Facilitating the movement of residents within the facility, ensuring they can participate in various institutional activities or guiding visitors. • Performing nighttime surveillance in hallways to promptly address residents’ needs, medical emergencies, or falls, given the reduced staffing levels during these hours.
Furthermore, professionals noted the potential of SARs in indirect care activities that support the staff’s operational efficiency. Suggested applications included: • Facilitating communication among care teams by transmitting crucial patient information. • Enhancing telemedicine capabilities by bridging interactions between onsite professionals and remote healthcare providers. • Streamlining logistical operations, such as automating daily tasks like opening curtains, assisting in housekeeping duties, or contributing to the institution’s ongoing cleaning and disinfection efforts.
Each category of professionals imagined integrating the robot in tasks directly related to their roles, or delegating some of them to it. For the animators, the robot could act as a co-leader for collective activity sessions (e.g., explaining and repeating game instructions); for persons in charge of logistics, the robot could handle the transport and storage of objects; for care assistants and nurses, the robots could monitor the absence of falls and guide users (residents and accompanying persons) in the facility, as well as be used for telemedicine purposes.
Dimension 2: Description and technical characteristics of the technology (TEC)
What equipment and supplies are needed to use the technology? (Equipment and supplies needed to use the technology, B0009)
The robot’s appearance according to professionals
Professionals emphasized that the robot’s design should promote engagement with older adults and foster acceptance. “The Nao or Miroki model, resembling a small child, immediately piques the curiosity of residents,” (Psychomotor therapist). Yet, it’s crucial for SARs to be recognizable as robots: “It should echo human form but clearly distinguish itself as a robotic entity” (Clinical nurse manager). Preferred characteristics included a friendly and vibrant demeanor: “It should radiate joy with big, welcoming smiles” (Community worker). Ideal size recommendations varied from 60 cm to 160 cm to avoid intimidation and ensure stability: “A humanoid size would facilitate collaborative interaction” (Nursing assistant). Additionally, articulated limbs were suggested to enhance the human-like appearance.
Robot features and functions
Consensus among professionals highlighted the necessity for SARs to offer straightforward usage and programming through an intuitive interface. A suite of ergonomic considerations was delineated, including: • For visually impaired users, the robot should facilitate interaction via speech, featuring a clear and modifiable tone, the capability to reiterate instructions, and utilize speech mirroring natural human language. • Incorporating a screen to assist those with hearing impairments, allowing text-based communication. • Ensuring the screen presents information in an accessible format, accommodating visual impairments, and is mounted at an accessible height for wheelchair users. • Adjusting movement and speed to align with the physical abilities of users to prevent any intimidation or accidents: “Movement must be measured and deliberate to avoid startling the residents” (Director in training).
Robot behavior
Essential to its integration, the robot must exhibit politeness and a friendly attitude, respecting the privacy and personal spaces of residents. This includes announcing its presence when entering a resident’s room to maintain decorum: “It’s imperative the robot inquires before entering, demonstrating basic etiquette” (Psychomotor therapist). Interaction distances should be calibrated for comfort, engaging residents actively yet sensitively to avoid being perceived as forceful or invasive. Predefined behavioral scripts should empower users with the autonomy to engage or disengage at will. Moreover, the robot’s interactions should be dynamic, adjusting to the cognitive and emotional state of the residents: “Should a resident show signs of distress, the robot’s response should be to lower its tone and suggest a later return, evidencing an understanding of the resident’s mood” (Medical doctor).
What material investments are required to use the technology? (Equipment and supplies needed to use the technology, B0007)
Among the hardware aspects mentioned as essential for the use of SARs, the necessity for a reliable Wi-Fi connection within the institution was highlighted foremost. Adequate robot battery life is also critical: “Constantly needing to recharge the battery every 2 hours would be impractical for us” (Animator). Professionals emphasized the importance of technology interoperability and integration with the institution’s medical call system, “ensuring that in the event of a fall, the robot can immediately alert staff, enhancing its practicality and effectiveness” (Nurse). Furthermore, a robust maintenance system for the robot is required to address both software malfunctions and mechanical failures, such as bug fixes or physical repairs.
What specific facilities are required to use the technology? Equipment and supplies needed to use the technology, (B0008)
The adaptation of the physical environment for robot implementation was noted as a critical need to ensure effective usage: “The robot requires clear pathways, but obstacles like armchairs and other frequently used items in the facility can impede movement” (Social Life Coordinator). Adequate space was mentioned to be essential not just for navigation, but also for appropriately storing the robot when not in use.
What kind of skills and training characteristics are needed for the personnel using this technology? (Training and information needed to use the technology, B0013)
While some professionals believed that using the robot did not necessitate specialized skills—“An interest in robots and basic operational training should suffice” (Animator)—others highlighted the need for more specific skill sets to troubleshoot minor issues, including routine maintenance, loading procedures, and bug resolution. The deployment of robots employing advanced operational protocols, such as the Wizard of Oz technique, demands more sophisticated computer skills.
Dimension 3: Safety (SAF)
How safe is the technology in relation to the comparator? (Patient safety, C0008)
Ensuring safety for older adults
The integration of robots within care environments necessitates rigorous attention to safety considerations. Space management emerges as a critical factor to ensure robots navigate freely without posing fall hazards to residents. The robot’s stability and reliability are paramount, with a design mandate to eliminate any risk of toppling over a resident or presenting pinch points that could ensnare fingers: “The design must ensure the robot remains upright even when leaned upon, avoiding any construction that might pose a danger to residents” (Psychomotor therapist).
Psychological risks for the older adults
Concerns were raised about the potential for robots to induce anxiety in residents with cognitive impairment, who may perceive these machines as sentient beings: “Given the memory challenges some residents face, distinguishing a robot from living entities can be confusing, potentially leading to stress” (Clinical nurse manager). Additionally, there’s the concern of inadvertently setting residents up for frustration by suggesting activities beyond their capabilities: “There’s a delicate balance in ensuring activities facilitated by the robot are within the resident’s ability range to prevent feelings of inadequacy” (Psychomotor therapist).
Material risks for technology
Some professionals have pointed out that robots can be susceptible to mishandling or damage by users: «Alzheimer’s patients can be aggressive and poke people with their canes” (Nursing assistant).
Dimension 4: Clinical effectiveness (EFF)
What is the effect of the technology on generic health related quality of life (Health related quality of life, D0012)
Professionals anticipated that the robot could significantly enhance residents’ quality of life through various means. It has the potential to foster inclusion among residents, particularly benefiting those who may feel marginalized: “The robot can engage less active individuals, encouraging their participation within the community” (Community worker). By addressing and responding to residents’ needs more promptly—often exceeding the capacity of busy staff—it can alleviate feelings of loneliness: “Given our limited time, the robot could offer companionship, engaging in conversations residents are eager to have” (Nursing assistant). The robot might also serve as a confidential listener, offering a sense of comfort: “It’s possible that residents might share thoughts with the robot they’re hesitant to disclose to us” (Nursing assistant). Moreover, it could strengthen connections between residents and their families through video calls and play a critical role in cognitive engagement: “the robot can favor the stimulation of cognitive functions of the residents, such as memory and language and help the involvement of the person in the activity by encouraging the user to imitate it (the robot)” (Psychomotor therapist).
Dimension 5: Social aspects (SOC)
How do patients perceive the technology under assessment? (Patients ‘perspectives, H0100)
Professionals anticipate that residents will show initial curiosity and interest toward the robot, similar to their reactions to a new pet: “The robot would spark curiosity akin to a new animal presence. While some may initially keep their distance, their intrigue is expected to grow over time” (Animator). They predicted a gradual acclimatization to the robot’s presence, with residents valuing the non-intrusive company it offers. Nonetheless, perceptions of the robot are expected to vary widely: “Opinions will range from skepticism to outright enthusiasm, influenced by individual experiences and health conditions” (Community worker). A notable observation was the anticipated “ripple effect” where the acceptance and interest of one resident could influence others: “It’s fascinating to see how one resident’s engagement with the robot can pique the interest of their peers” (Instructor). Overall, there was optimism about residents embracing the technology, especially when its purpose and benefits are clearly communicated: “Our experience shows that residents can be incredibly receptive to new technology when its use is properly introduced” (Nurse).
What special points need to be communicated to patients to improve adherence to social and assistive robots? (Communication aspects, H0203)
Professionals emphasized the importance of providing clear and consistent explanations to residents to foster acceptance of robots. “Residents should be introduced to the robot gradually, understanding that it enhances care without supplanting the human touch” (Clinical Nurse Manager). They offered insights on effective information dissemination and training approaches: “Training might include interactive animations designed in an engaging manner, presenting the robot as a supportive aid rather than an unfamiliar entity” (Animator).
Dimension 6: Cost and economic evaluation (ECO)
What were the measured or estimated cost of the assessed technology? (Resource utilisation, E0009)
From the perspective of professionals, especially those in managerial roles, the expense associated with acquiring and maintaining most current robots poses a significant challenge to geriatric institutions’ budgets. “The financial outlay for a robot encompasses not only its purchase price but also ongoing maintenance, necessary institutional modifications for deployment, insurance, and further maintenance costs. These aspects require thorough financial assessment” (Director in training).
How does technology modify the need for other technologies and the use of resources? (Resource utilization, D0023)
Several participants suggested that robots could mitigate the impact of staffing shortages by taking over certain responsibilities. This technological intervention is poised to transform how resources, including human labor, are allocated within care settings. “Given our limited presence in resident areas, robots have the potential to offload some of our duties, allowing us to reallocate our efforts more effectively across the institution, possibly even rebalancing task distribution” (Animator).
Dimension 7: Ethical aspects (ETH)
What are the known and estimated benefits and harms for patients when implementing or not implementing the technology? (Benefit-harm balance, F0010)
Professionals recognized the robot’s potential benefits for both residents and staff. A significant advantage noted was the robot’s capacity for limitless engagement without judgment, contrasting with human limitations: “A robot offers an impartial presence; it won’t express displeasure, no matter how often it’s summoned” (Psychomotor therapist). Nevertheless, there was a strong consensus that the robot’s role should be supplementary, enhancing human care rather than replacing it. Tasks delegated to the robot should be those of lower human value-add, thereby freeing up staff to focus on more impactful interactions with residents: “If the robot can take over menial tasks, it would allow caregivers more meaningful time with residents” (Community worker). Direct care tasks, particularly those requiring empathy and physical contact, were emphasized to remain human responsibilities: “The concept of a robot managing feeding akin to a scene from a dystopian film is unthinkable” (Social life coordinator). The need for professional oversight was highlighted, whether for logistical support or therapeutic engagement, ensuring the robot’s integration doesn’t lead to impersonal care. This approach seeks to preserve the human essence of caregiving by leveraging robotic assistance judiciously.
Does the implementation or use of the technology affect the patient’s capability and possibility to use autonomy? (Autonomy, F0004)
Professionals underscored the importance of securing a resident’s consent prior to interaction with a robot and allowing them to dictate their level of engagement: “This includes respecting those who prefer solitude. The goal isn’t to force participation on individuals uninterested in engaging” (Community Worker). Some professionals highlighted the potential for robots to enhance resident autonomy by offering continuous availability. The robot could alleviate the conflict between personal autonomy, beneficence, and equity by supporting residents in making informed decisions (potentially through a simple, personalized choice algorithm), a luxury often unaffordable in institutional settings due to time constraints faced by caregivers: “For instance, a robot could daily present menu options to residents, empowering them with choices often constrained by the staff’s limited availability” (Medical Doctor).
Does the implementation or use of the technology affect human dignity? (Respect for persons, F0008)
The possibility of deceiving residents through the use of social robots was discussed. Comparing this to the experience with a doll, one professional observed: “We experimented with a doll, leading to mixed reactions from a resident who initially engaged with it as if sentient, only to later treat it indifferently. This fluctuation in perception raises concerns about the psychological impact, blurring the lines between object and entity” (Community Worker). The issue of potentially infantilizing residents with overly simplistic or childish interfaces was also brought up: “I have reservations about robots that utilize simplistic or juvenile interfaces, as it’s crucial to maintain respect and not diminish the adults we’re serving” (Community Worker).
Does the technology invade the sphere of privacy of the patient? (Respect for persons, F0101)
The concern about robots infringing on residents’ privacy was voiced: “Robots must be programmed to engage only with those residents who express interest” (Psychomotor Therapist). The critical importance of data security was emphasized, with apprehensions regarding the potential misuse of personal information relayed to the robot: “A paramount concern is the risk of espionage, with personal data being vulnerable to misuse by external parties” (Medical Doctor). There were also concerns about the potential for the robot to be compromised: “And the risk of the robot being hijacked? The threat of cyber-attacks remains a real and present danger” (Medical Doctor).
Are there factors that could prevent a group or person from gaining access to the technology (Justice and equity, H0012)
Professionals advocated for equitable access to the robot among all interested residents to avoid any sense of unfairness. As a concluding proposition, there was a call to establish guidelines for professional conduct and ethical robot use in geriatric settings: “A practice guide could be formulated to ensure ethical interactions by the robot, including seeking consent, adapting its communication style to the resident’s preferences, respecting privacy, and ensuring equitable engagement across the resident population” (Medical Doctor).
Dimension 8: Organizational aspects (ORG)
How does the technology affect the current work process? (Health delivery process, G0001)
Professionals viewed the robot’s integration as a boon to their operational processes, emphasizing its potential to streamline their duties and enhance resident care. By automating some routine tasks, the robot could significantly reduce the physical and cognitive demands on staff: “Automating tedious tasks would not only free up our time but could also alleviate the stress of our daily workload, fostering a more relaxed environment” (Nursing assistant). It was envisioned as a collaborator in activities, injecting energy and innovation into routine engagements: “A robot, capable of introducing music and movement into sessions, could revolutionize activity programming, acting as a dynamic co-facilitator” (Animator). The overarching sentiment was that robotic assistance, carefully and thoughtfully implemented, could bolster staff support without supplanting the human element: “Robotic support, when utilized judiciously, offers a significant augmentation to our resources, particularly in light of staffing constraints, enhancing our ability to deliver attentive care” (Director in training).
What kind of involvement has to be mobilized for patients and important others and/or caregivers? (Health delivery process, C0002)
According to professionals, the engagement of all stakeholders (managers, professionals, older adults (OAs), families) was deemed essential for the successful implementation of the robot in the institution. The facility managers played a pivotal role: “The management committee’s support is crucial; without their buy-in, efforts are futile. They must lead the initiative” (Community Worker). Staff involvement was also critical: “Respect and staff buy-in are key, given staff concerns about surveillance. It’s vital to communicate the purpose of these technologies upfront, clarifying that monitoring staff or tracking individuals is not the goal” (Community Worker). Residents needed to be informed and prepared for the robot’s introduction, and families were also integral to the process. Families’ reactions varied: “We have generally open families here. However, some residents have families that are more resistant, fearing that a robot caring for their loved one diminishes the personal touch” (Animator).
What kind of process ensures proposer education and training of staff? (Health delivery process, G0003)
Professionals emphasized the necessity of training on robot usage, including technical aspects, such as operation, charging, maintenance, or troubleshooting, as well as the key steps for the preparation and conduct of intervention sessions using the robotic mediation: “Staff require initial training followed by ongoing sessions to equip new hires with the knowledge to use the technology effectively” (Director).
How is the technology accepted? (Culture, G0010)
Many professionals shared positive anecdotes about robots, highlighting their potential to bridge gaps in care and education: “...a child who was ill could participate in class via the robot; such experiences are highly encouraging” (Social Life Coordinator). Some viewed the robot as a future coworker: “Collaborating with a robot is intriguing. It’s likely we’ll consider them colleagues eventually” (Nursing Assistant). However, concerns about job replacement were voiced: “The thought of being replaced by robots is unsettling” (Nursing Assistant). A gradual acceptance process was envisioned, starting with initial skepticism followed by familiarization and acceptance, driven by the robot’s appealing design and practicality. Professionals expressed a desire for real-life trials within the institution: “We’re eager to test these robots to observe their functionality and limitations firsthand” (Instructor); “Seeing and testing the technology myself is crucial for acceptance” (Social Life Coordinator).
What management problems and opportunities are attached to the technology? (Management, G0008)
Setting guidelines for robot use within the facility was highlighted as important, such as defining appropriate and inappropriate areas for its presence: “Robots might be better received in social areas than in private rooms” (Animator). Adjustments, such as keeping doors open for robot visits, were suggested. Ongoing evaluation of the robot’s impact was considered vital: “Post-implementation, we’ll need to assess what’s working, gauge satisfaction, and determine the technology’s utility” (Medical Doctor).
Dimension 9: Legal aspects (LEG)
What do laws/binding rules require with regard to the safety of the technology and how should this be addressed when implementing the technology? (Authorization and safety, I0017)
Professionals underscored the importance of addressing legal considerations when introducing SARs into geriatric care settings. The matter of liability, particularly in cases where a robot may inadvertently cause harm or damage, emerged as a significant concern. “The issue of liability, especially if a robot were to cause any harm, necessitates careful legal scrutiny. It appears that legal experts are beginning to explore these complex questions” (Medical doctor).
Comparative analysis of attitudes and perceptions of rural and urban nursing home professionals on socially assistive robots
A specific sub-analysis was conducted to understand the association between the context of work and professionals’ attitudes towards robots. This sub-analysis focused on comparing the views of participants working either in rural or urban nursing home settings. It examined differences in familiarity with robotic technologies, levels of acceptance, perceived barriers, potential benefits, and ethical concerns.
Urban participants demonstrated a higher level of familiarity with various socially assistive robots compared to their rural counterparts. Approximately 75% of urban participants could identify and describe advanced robots such as Pepper, Nao, and Paro, indicating a broader exposure: “We used Paro and later introduced Nao for activities with residents; they enjoyed these interactions” (Animator, urban). In contrast, only 50% of rural participants recognized basic robotic applications, often limited to simpler models like Paro or basic telepresence robots: “We are not familiar with these machines; it’s hard to say how useful they would be” (Nursing assistant, rural).
The acceptance of robots varied between the groups, with about 80% of urban participants expressing a positive attitude towards their integration into elderly care settings. They highlighted potential benefits such as reducing workload and providing companionship: “I find it positive; robots can help with tasks like serving water, reducing the workload for staff” (Clinical nurse manager, urban). Meanwhile, only 50% of rural participants shared this acceptance, often expressing reservations and a need for more evidence of the benefits before fully embracing the technology: “It’s difficult to imagine how these robots can really fit into our care routines here” (Care referent, rural).
Significant barriers to the use and deployment of robots in geriatric care settings were identified by both groups, though with different emphases. Around 60% of urban participants highlighted concerns related to the costs and complexity of implementing robotic systems, emphasizing the need for adequate training and support: “Training is essential; without proper introduction and ongoing support, these technologies can become more of a burden than a help” (Medical doctor, urban). Conversely, 70% of rural participants pointed out challenges related to digital literacy and the relevance of robots in less technologically advanced settings, often expressing concerns about the usability and potential replacement of human caregivers: “Our staff might struggle with these technologies; it could be overwhelming” (Social life coordinator, rural).
Both groups acknowledged the potential benefits of robots, with about 70% of urban participants seeing significant opportunities for enhancing care, particularly in social and recreational activities: “Robots like Miroki can help alleviate loneliness among residents, providing a form of interaction” (Medical doctor, urban). However, only 50% of rural participants expressed similar optimism, suggesting a more cautious and gradual introduction of robots to ensure proper adaptation: “We need to introduce these slowly, ensuring everyone is comfortable” (Nursing home director, rural).
Ethical concerns were prevalent across both groups, with approximately 65% of urban and 70% of rural participants voicing worries about potential dehumanization and privacy issues. Urban participants emphasized ensuring that robots complement rather than replace human caregivers: “The robot should not replace human presence; it should only assist, never replace” (Clinical nurse manager, urban). Meanwhile, rural participants focused on the importance of maintaining personal connections in caregiving: “It’s crucial that the personal touch in caregiving is preserved; robots can’t replace that” (Nursing assistant, rural).
The study also revealed a difference in approach to implementing robotic technologies, with 70% of urban participants advocating for a more experimental and gradual integration: “We should start with trials to see how well these robots integrate into our care routines” (Psychomotor therapist, urban). In contrast, 60% of rural participants preferred a cautious, well-planned approach to avoid overwhelming staff and residents: “A careful, step-by-step introduction is necessary; we can’t rush this process” (Instructor educator, rural).
Comparative analysis between professionals with in-person interactions of social and assistive robots and those only familiar with the concept
The analysis of professionals with in-person interactions with socially assistive robots versus those familiar only with the concept reveals distinct differences in knowledge and perceptions of the technology.
Professionals with in-person interactions demonstrated detailed knowledge of various robots, such as Paro, Nao, Pepper, and telepresence robots. They described specific functionalities, like video conferencing, physical assistance, and interactive games. For example, one professional mentioned, “The residents liked Paro and Nao, especially in activities like quizzes and movements” (Animator, in-person interactions). Conversely, those familiar with the concept but without in-person interactions often expressed cautious optimism, tempered by concerns about potential limitations and ethical issues. Some of these participants emphasized the need for proper support when introducing robots in geriatric care settings: “It’s important that we introduce these technologies slowly, ensuring everyone is comfortable” (Care referent, familiar with the concept)
Both groups raised ethical and practical concerns, but the nature and emphasis differed. Participants with in-person interactions were more focused on practical issues such as maintenance and the potential for robots to supplement but not replace human care: “It’s crucial that robots assist but never replace human caregivers” (Medical doctor, in-person interactions). Participants familiar with the concept, however, were more likely to express concerns about the broader implications of introducing robots into care environments. They worried about issues such as privacy, the potential for dehumanization, and the need for clear guidelines to ensure robots are used ethically: “There must be a line between the robot and ourselves... the robot should not overstep human roles or record private information” (Social life coordinator, familiar with the concept)
Summary of proposed robot specifications
Design specifications for a geriatric care social assistance Robot.

NB: *These two technical specifications are not yet feasible.
Summary of proposals for implementing interventions using social and assistive robots in geriatric facilities
Strategic framework for the implementation of SARs in geriatric care settings.

Discussion
The aim of this work was to analyze the needs and expectations of professionals working in geriatric facilities regarding the use of social and assistive robots, as well as the facilitating factors and barriers to their implementation in this context. For this work, we conducted interviews with 20 professionals with a variety of backgrounds and functions. The multidimensional EUnetHTA Core Model® (version 3.0) 20 was used to guide the analysis of interview transcripts.
Our results showed that professionals had a generally positive opinion and attitude towards robots. Nevertheless, they stressed a number of points that could hinder acceptance of these tools. In this section, we discuss the main facilitating factors, barriers and solutions described by professionals for the acceptance and implementation of social robots in institutions for older adults.
Facilitating factors for implementing SARs
Professionals’ knowledge of robots
Unlike the work by Mitzner et al.,24,25 where the professionals surveyed had little familiarity with robots, all the professionals (except one) in our study had knowledge about robots, and several had already used them. The positive attitude of the professionals towards robots in our study corroborates previous work,17,26 where professionals’ acceptance of robots correlated with their prior knowledge of these tools. Over the past 10 years, the development of social robots has enabled professionals to gain a better understanding of these tools, particularly their capabilities and limitations. We can therefore assume that professionals’ opinions of robots have become increasingly positive over time, as their knowledge of these tools has improved.
Satisfactory robot appearance
The first contact with the robot is crucial for the user’s acceptance of it. 27 Indeed, if the robot is unpleasant to the user, it may be immediately rejected. On the contrary, a pleasing appearance will increase the person’s commitment to the robot. A facilitating factor for robot acceptance by the professionals in our study was that the robots presented, particularly humanoid robots, satisfied them aesthetically. This result aligns with those in the literature,28–30 which showed that professionals preferred humanoid robots and judged them to be the most appropriate for older adults. Congruent with the literature, 28 the professionals asked for an interactive, expressive, and friendly robot. A size smaller than human, between 120 and 150 cm, already recommended in the literature,28,30,31 was suggested by the professionals in our study.
Use of robots for direct and indirect care in the institution
Overall, the professionals held a very positive view of robots, believing that these tools could enhance residents’ quality of life by promoting interaction, stimulating them, and reducing isolation. This finding is consistent with various studies in the literature.17,29,32 Furthermore, the professionals noted that robots could alleviate their mental and psychological workload.32–34
Professionals believed that robots could be useful for various purposes across different situations. For direct care, in alignment with existing literature, they cited applications such as video conferencing with loved ones, especially family,22,29,31,35 falls monitoring and prevention,35,36 assistance with orientation, 36 and provision of recreational activities like dancing, listening to music, games, reading, 36 as well as physical exercises, cognitive stimulation, task reminders, or information alerts,30,36,37 mobility assistance, 35 companionship, 36 and patrolling with monitoring for possible falls in corridors. For indirect care, the professionals in our study, similar to those in previous studies,17,32,35,36 believed that the robot could assist them in their work, particularly for simple, repetitive, and routine tasks that are physically and psychologically demanding, such as logistics assistance, cleaning, and disinfection. Previous works have indicated that professionals hoped robots could aid with additional tasks such as transporting patients, acting as translators for non-native speakers, or providing support during aggressive incidents involving residents or families.26,32 However, professionals in our study did not express these latter needs.
Motivating professionals
Unlike the professionals interviewed in previous studies who feared that robots would replace them and lead to job loss,28,33,36 participants in our study had few concerns about this issue. In fact, they viewed the robot as a work-assistance tool to which they could delegate repetitive and constraining tasks defined and controlled by them. Some suggested, in a positive and spontaneous manner, that the robot could serve as a colleague. This perspective is comparable to that observed in the study by Vänni and Salin. 32
Other facilitating factors for robot implementation included the professionals’ interest in the robots and their desire to test them quickly in real-life scenarios they had envisioned. This positive attitude of professionals towards robots could also facilitate a positive ripple effect on residents and their families. We cannot rule out the possibility that professionals’ interest in robots reflects a novelty effect, and that this interest might diminish when they are confronted with them in real-life, as mentioned in previous work. 38
Barriers to implementing SARs
The professionals have raised a number of issues that could constitute technical, human, organizational, and ethical barriers to the implementation of robots. They have also suggested solutions to these issues, which we will discuss below.
Technical factors
For the professionals in our study, as observed in previous studies,33,36 the robot’s usability was a critical point. The robot had to be easy to use for both residents and professionals. This aspect was particularly described in the Almere model, 39 which stipulated that the robot was much more likely to be accepted if it had good usability. The technical challenge is likely to be all the greater, as the professionals in our study noted that the robot needed to be able to adapt to residents’ sensory (hearing and visual) and physical (mobility disorders, residents in wheelchairs) impairments. The professionals wanted the robot to be interactive, use language effectively (i.e., to understand and express itself clearly), and be able to adapt to residents' cognitive or behavioral disorders. The desire to personalize the robot according to the abilities and needs of older adults has already been expressed in previous work.30,37
Regarding the risks mentioned by the professionals, the risk of a fall caused by an assistance robot jostling a patient could only be mitigated by using a stable robot with satisfactory navigation capabilities within the institution’s environmen28,36t. Nevertheless, professionals in our study preferred a mobile robot, unlike those in the study by Salichs et al., 28 who preferred an immobile robot for fear that it might jostle residents.
For professionals, all residents could benefit from SARs. However, it seemed necessary to take precautions when offering a robot to residents with severe neurocognitive disorders. These individuals may not understand the nature of the tool and consequently feel anxious when interacting with it. The psychological risk of inducing anxiety by using a robot in a resident with major neurocognitive disorders could be limited by having a good knowledge of the person and by testing the effects of the interaction between this person and the robot, if the person gives consent.36,40–42 Furthermore, it was perhaps preferable to avoid using mobile assistance robots in units where patients with major neurocognitive disorders were wandering around. This is the reason why the professionals in the study by Salichs et al. 28 preferred an immobile humanoid robot.
Human factors
Professionals in this study believed that residents’ opinions on robots might vary. Some residents might easily accept the robots, while others could be reluctant. According to participants, any initial concerns about implementing SARs in the institution would likely dissipate as residents gradually became accustomed to their presence. Residents would be interested in the robot, curious to test its functionalities, and satisfied with its presence in the institution. Specifically, they would value the ability to summon the robot to request services repeatedly without fear of being intrusive. The professionals' confident anticipation of an overall positive resident response to the implementation of a robot in a geriatric institution aligns with previous findings in the literature.32,36
Participants also considered that some professionals and families might be reluctant or even hostile toward the implementation of SARs in the institution. However, they believed that familiarity with these technologies, combined with group influence, could positively impact robot acceptance. The phenomenon of individuals becoming interested in a technological tool due to group influence —particularly by other professionals, residents, or families—has been extensively described in the literature and is a known determinant of product adoption in the UTAUT model. 43
In line with the literature, the professionals in our study emphasized the importance of a collegial decision-making process involving all stakeholders, especially management, for the implementation of a robot.33,44 Informing all parties (professionals, residents, and families) about the robot’s presence and its operational methods41,42 and training professionals in the use of the tool were identified as crucial for its successful integration into the institution. 33
Organizational factors
Although professionals believed that robots could reduce their workload both physically and psychologically, they also expressed concerns that implementing robots could burden them with new tasks, such as preparing the robot before use, cleaning it after use, and maintaining it. This concern aligns with the observations of other authors,17,41,42 who noted professionals’ worries about their ability to effectively use a robot if they lacked adequate resources and time. Consequently, participants in this study emphasized the need for sufficient human resources and long-term technical support to facilitate the implementation of the robot in the institution. 44
Furthermore, as noted by Vanni et al., 32 professionals believed that the implementation of robots in their institution should be carried out in stages. Participants in this study insisted on the importance of simultaneously informing all stakeholders and repeatedly training professionals in the use and maintenance of robots. The significance of educating all stakeholders has also been highlighted in other studies. 33 Interestingly, Wang et al. 44 proposed a five-step implementation scheme called “Easy to Use Tool Start,” which includes sharing the team’s experiences and successes, organizing the implementation schedule step-by-step, addressing the team’s difficulties, repeating the training, and providing technical support to the team. Similarly, Haubold et al. 45 suggested several steps for implementing a robot in an institution, starting with assessing the impact of a robot on planning, workflow management, and staff training, and proceeding with strategic, ethical, and human considerations to ensure a well-rounded implementation strategy.
Ethical aspects
Unlike the professionals in the study by Frennert et al., 33 who perceived the presence of robots in an institution as a threat to the quality of care, participants in our study believed that robots could enhance residents’ care. However, they raised several concerns.
The risk of dehumanizing care due to the presence of the robot was acknowledged by our participants and has been previously discussed in the literature.28,33,35,46 Thus, as described by Mitzner et al.,24,25the professionals in our study preferred that the robot be used for physically demanding or routine tasks, but not for tasks directly related to the resident’s health or requiring physical contact. In line with various authors,24,25,28,34,35 participants in this study were hesitant to use the robot for hygiene care and feeding assistance, believing these tasks, which require physical touch, should remain human responsibilities26,32 or, at minimum, be performed in the presence of a human. 34 Establishing a clear division of tasks between the robot and professionals could mitigate the risk of dehumanization. Usage scenarios, including where and how the robot would operate, need to be predefined by professionals and regularly reassessed.
In this context, robots remain tools at the disposal of professionals, utilized based on the purpose and ethics behind their use. In a situation where the time available for care per resident is increasingly scarce, it is essential to free up professionals’ time as part of an “Ethics of Care” approach. 47 To preserve this ethical framework, a team analysis involving residents’ representatives of the potential tension between the ethical principles of nonmaleficence, beneficence, autonomy of decision-making, and equity must be conducted on the most personalized scale possible. 48 Enhancing residents’ empowerment, by providing them with support and opportunities to make their own choices considering their capacities, is seen as a major ethical lever. 49
The risk of robot intrusion into personal privacy noted by our professionals has also been documented in the literature.28,36,37,44 To address these ethical concerns, our participants proposed drafting guidelines for good practice in the use of robots. This approach aligns with the good practice recommendations by Niemelä et al., 31 who advocated for a set of rules for using telepresence robots in institutions, developed collaboratively by residents, families, and professionals.
Regarding SARs, the risk of misleading residents, for example, by causing them to believe the robot is a living entity, was discussed. This corroborates findings by Koh et al.,41,42 which highlighted differing views between philosophers and field professionals on this issue. Philosophers have considered the potential deception of residents by robots as a significant ethical concern,46,50 whereas field professionals have noted the benefits and advocated for residents’ autonomy in perceiving the robot either as a living entity or an inanimate object. Our study, like those of Koh et al.,41,42 recommends training professionals in best practices for using SARs, followed by establishing a mechanism within the team to reflect on ethical questions that may arise during robot-mediated interventions.
Economic factors
Consistent with the literature, our participants, particularly the directors, noted that the high cost of robots could significantly hinder their acquisition and integration into the facility.41,42 They indicated that they would be more likely to accept the high cost if, following a health economics evaluation, the robots proved to provide a return on investment by freeing up nursing time. These professionals expressed a desire for more detailed information on the cost-benefit ratio of robots, particularly those designed as mobile assistance platforms.
Comparison of attitudes and perceptions between rural and urban professionals on socially assistive robots
The comparison between urban and rural settings revealed that urban participants had greater familiarity with robotic technologies, likely due to better access to advanced resources and educational opportunities. This disparity highlights the need for targeted initiatives to increase awareness in rural areas, where exposure to such technologies is limited. Urban participants’ higher acceptance rates can be attributed to their frequent interactions with robots, making them more open to integration. In contrast, rural participants displayed caution, emphasizing the necessity of building trust and demonstrating clear benefits before adopting these technologies.These results corroborate those by previous authors51,52 who showed that the people living in urban areas, especially big cities, were more comfortable about the idea of robots assisting older adults with respect to those living in rural contexts.
Significant challenges related to the acquisition, use, and adoption of robotic technologies were noted across both groups, particularly concerning costs, complexity, and digital literacy. These challenges are more pronounced in rural settings due to limited resources and infrastructure. Addressing these issues requires not only financial investment but also comprehensive training and ongoing support to ensure effective utilization of robotic tools. The cautious optimism among rural participants compared to the enthusiasm in urban areas indicates differing readiness levels, suggesting the need for a phased, tailored approach to introducing these technologies.
Ethical concerns about dehumanization and privacy were prevalent, underscoring the importance of ensuring that robots complement rather than replace human caregivers. Both urban and rural participants stressed the necessity of maintaining personal interactions in caregiving, highlighting a shared priority across settings.
The differing attitudes toward implementation—urban participants’ openness to experimentation versus rural participants’ cautious approach—reflect varying risk tolerance and resource availability. This suggests that a one-size-fits-all strategy is inappropriate. Instead, a nuanced approach, considering the specific needs and contexts of each setting, is crucial for the ethical and successful integration of robotic technologies in elderly care. Overall, these findings underscore the importance of a context-sensitive strategy to address the unique challenges and opportunities present in different geographical areas.
Comparison between professionals with in-person interactions with social and assistive robots and those only familiar with the concept
The comparison between professionals with prior in-person interactions with socially assistive robots and those familiar only with the concept highlights the critical role of hands-on experience in shaping positive attitudes and detailed understanding of these technologies. The experienced group showed greater enthusiasm and knowledge, which aligns with findings that direct interactions with robotic systems enhance understanding and acceptance. 53 This group’s familiarity with practical aspects such as user interface and maintenance underscores the importance of experiential learning in fostering a comprehensive understanding of socially assistive robots’ capabilities and limitations.
Furthermore, the cautious stance observed among those familiar only with the concept, particularly regarding ethical concerns, reflects broader societal apprehensions about the integration of technology in caregiving. The literature supports this, noting that ethical considerations like privacy, autonomy, and the potential for dehumanization are significant barriers to the adoption of social robots in care settings. 54 These concerns highlight the necessity of transparent guidelines and ethical frameworks to ensure these technologies enhance, rather than detract from, the quality of care.
The emphasis on the need for training and support among the experienced group points to a practical understanding of the challenges associated with adopting new technologies. Comprehensive education and ongoing support are crucial for the successful integration of socially assistive robots, as supported by recent studies highlighting the need for structured training programs to prepare caregivers for working with these technologies. 55 This need for training is less emphasized among those familiar only conceptually with these robots, suggesting a gap in awareness of the practical challenges involved.
These findings underscore the importance of targeted interventions, including hands-on training and clear ethical guidelines, to address the concerns of both groups. A nuanced approach, incorporating both experiential learning and ethical considerations, is necessary to bridge the gap between theoretical knowledge and practical application, ultimately improving the quality of care provided to elderly populations.
Study limitations
This work shows some limitations. Previous research has indicated that women and men perceive technology differently. Therefore, it can be assumed that such gender differences in opinions would also exist among healthcare professionals. However, this assumption cannot be verified due to the significant gender imbalance among the participants in our study. Consequently, it is difficult to draw conclusions based on individual opinions, especially considering that only two men were included in our work.
Dividing the total group of participants into smaller professional subgroups—based on their work context (urban or rural nursing homes) or prior experience with robots (familiarization or direct interaction)—resulted in each subgroup consisting of only a few individuals. As a result, no definitive conclusions or generalizations can be drawn from our findings regarding the differences between urban and rural participants, or between those with prior in-person interactions with social robots and those who are only familiar with them. To gain a clearer understanding of the differing opinions among these professional groups, a study with a larger sample size would be necessary.
The professionals mentioned few barriers to the implementation of robots in their institution. It is possible that the professionals did not disclose all the potential barriers they envisioned concerning their own institution to the researchers.
Contribution of the study
Our work has provided insightful contributions to the analysis of facilitating factors and barriers to the implementation of SARs in a geriatric care institution and has enabled us to suggest a number of solutions to alleviate the problems that arise during their implementation. We gathered the opinions of professionals with diverse roles (caregivers, logisticians, and management) concerning SARs primarily used with older adults. We interviewed professionals in various contexts: in urban areas (in two different regions) and in rural areas. Another contribution of our qualitative study was to conduct a multidimensional analysis of professionals’ needs and expectations of social robots, using the EUnetHTA Core Model® (version 3.0). 20 This method allowed us to examine all the factors associated with the implementation of social robots in institutions for older adults from multiple perspectives comprehensively. As noted by Vandemelebroucke et al., 56 the use of an HTA assessment model is particularly useful for conducting a comprehensive assessment that includes the medical, economic, safety, social, and ethical dimensions of health technologies.
Although the professionals were not able to interact with the robots during the project, most of them were already familiar with them. Thus, the presentation of the project videos enabled them to express their opinions and expectations of the robots (suggesting numerous use cases), and to describe the facilitators and barriers to their implementation in institutions in depth.
Conclusion and outlook
This study explored the needs, expectations, and perceptions of healthcare professionals regarding socially assistive robot use, including facilitating factors and barriers to implementation in geriatric care settings.
The outcomes indicated that healthcare professionals generally viewed robots positively, recognizing their usefulness in a variety of non-personal care tasks. Ease of operation was identified as a critical factor for successful robotic integration in elderly care. Additionally, the importance of educating all stakeholders and providing comprehensive training for professionals was emphasized as essential for effective implementation. Discussions also addressed the financial and ethical considerations associated with the deployment of these robots.
The findings also provided insights into how the work context influences the adoption and integration of robotic technologies in elderly care, revealing distinct challenges and opportunities faced by professionals in these different geographical areas (urban and rural). The analysis also showed that in-person interactions with socially assistive robots significantly enhances professionals’ knowledge and positively influences their perception of these technologies. In contrast, those familiar with the concept but lacking hands-on experience are more cautious and focused on potential challenges and ethical issues. These differences underscore the importance of providing comprehensive training and support to all professionals in care settings, ensuring they are well equipped to work with these technologies and address the concerns of residents and families effectively.
This study also emphasizes the critical importance of co-construction with users when introducing a new tool that involves changes in practices within a geriatric care institution. This work will enable us to formulate recommendations for the design of SARs that meet the needs and expectations of users, particularly professionals. In our subsequent efforts, we plan to conduct co-design workshops with professionals and residents from geriatric care institutions. These workshops will focus on creating and testing prototypes for various activities and services that the robot could offer. These include cognitive games, assorted services (such as delivering a bottle of water or the newspaper), and reminders of the institution’s scheduled activities (menus and entertainment activities). Additionally, tests will be organized for guiding and monitoring individuals using the robot. The next phases will involve the evaluation of the final prototypes and the observation of the robot’s repeated usage and its functionalities during co-construction workshops with all stakeholders.
Footnotes
Acknowledgement
We would like to thank professionals from nursing homes (Vigne Blanche in Gevrey, George Sand in Chenove, and Annie Girardot in Paris) and long-term care units at Broca Hospital (AP-HP, Paris) for agreeing to take part in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Vyv3 Bourgogne group and the Caisse des Dépôts.
Guarantor
ASR.
Contributorship
MP and ASR researched literature and conceived the study. SD, IS, HL, MP, CH were involved in protocol development, gaining ethical approval, participants recruitment and data analysis. ASR wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.