
Abstract
In this review and meta-analysis, we aimed to investigate the effect of spine orthotics in osteoporotic patients. The relationship between osteoporosis, osteoporotic vertebral fractures (OVFs), and age-related hyperkyphosis has made this effect unclear. We believe that taking participants’ conditions into consideration may help to alleviate this controversy. The electronic database includes Web of Science, PubMed, Cochrane Library, Medline, and ClinicalTrials.gov. For English language literature was searched up to March 2023, and 34 articles were included in the review and 15 article had sufficient quality for meta-analysis based on the methodology quality index. There was no significant effect found from using either rigid or soft orthoses alone during the acute phase of one level (OVFs). Both semi-rigid and weighted orthoses have shown a positive significant effect on thoracic kyphosis angle and back extensor muscle strength in osteoporotic or older hyperkyphotic patients. The results of this review indicate that using a soft or rigid orthosis alone does not have a superior effect in the acute phase of one-level (OVFs) compared to not using an orthosis. However, using a semi-rigid or weighted orthosis in osteoporotic or hyperkyphotic older adults with or without (OVFs) can benefit thoracic kyphosis angle, back muscle strength, and balance.
Keywords
Introduction
Changes in spine biomechanics 1 related to aging, osteoporosis, osteopenia, and postmenopausal hormonal changes in the older population, especially in women 2 Causes Asymmetrical load transmission of the intervertebral disc. 3 The spine-bent postures will provoke age-related hyperkyphosis or osteoporotic vertebral fractures. 4 While Hyperkyphotic older adults, 1.7 times more than older adults without hyperkyphosis face with future OVFs 5 ; The exact cause-and-effect relationship between age-related hyperkyphosis and OVF is not clear.
The prevalence of hyperkyphosis in the elderly population is 20% to 40%, varying between men and women, 6 and for osteoporotic vertebral fractures, 20% to 24%, varying between races. 7 Hyperkyphotic posture negatively impacts the quality of life, pulmonary and physical function, increasing the risk of falls, fractures, and mortality. 8 Osteoporotic vertebral compression fractures, reported as risk factors for age-related hyperkyphosis. 8
Approximately 67% to 75% of OVFs are without clinical symptoms,9,10 and only 10% of OVFs need hospitalization, 11 so conservative interventions are a priority for patients. Surgical and non-surgical interventions 12 like Percutaneous vertebroplasty, kyphoplasty, orthotic interventions, and analgesic drugs are prescribed for painful OVFs. Also, an equal effect on pain in 1-year follow-ups was reported for both. 13 Invasive and non-invasive methods seem to have advantages and disadvantages.14–16
Back extensor muscle strength (BES) and proprioception deficits as the functional and structural modifiable factors 8 and OVF as a preventable factor 17 were targeted by conservative interventions like orthotics, physiotherapy, exercises, and tapping18–20 in age-related hyperkyphosis condition. Orthotic interventions have been used for decades to decrease age-related hyperkyphosis or improve flexed posture in kyphotic patients and protect the spine of people with OVF during the healing period, and meta-analyses evaluated different interventions.19,21,22 Orthoses are conservative interventions that, in some designs, showed a remarkable effect on trunk muscle strength and kyphosis angle.23–25
However, controversy about using orthotic intervention in the osteoporotic population exists. Most of the studies in this field, inattentive to the relationship between age-related hyperkyphosis and OVF, omitted data about previous OVFs or thoracic kyphosis angles to include patients in a study about age-related hyperkyphosis or OVFs in the acute phase solely. Indeed one-third of hyperkyphotic older adults have at least one OVF, and subdividing these patients by inclusion criteria, which happened in previous reviews, cannot help us distinguish the effect of orthosis in osteoporotic patients.26–28 Although some Meta-analyses results showed no impact of orthotic use in age-related hyperkyphosis 19 in comparison with other interventions, articles report significant improvements.23,25 Otherwise, some meta-analyses showed controversy about orthosis benefits in pain, functional ability, and union duration in the acute and sub-acute phases of OVF21,29,30 and neglected the structure, function, and design of an orthosis. Explaining the design, function, and target population of spinal orthotics in osteoporotic patients may change our expectations of an orthosis and define the proper manner of use of a spinal orthosis in osteoporotic patients.
The point is that orthotics in this field have different designs, goals, and roles. Therefore, defining the types, function, manner of use, wearing time, and describing the best choice based on patient characteristics may alleviate inconsistency about orthotic interventions in the osteoporotic elderly population. So, this systematic meta-analysis review aims to investigate the effect of orthotic interventions in osteoporotic patients based on the syndrome.
Methods
This systematic review and meta-analysis were designed and presented based on the instructions for preferred reporting in the systematic review and meta-analysis guidelines (PRISMA).
Eligibility criteria
In this review, studies that inspect the effect of orthotic interventions on pain (as a visual analog scale or part of a questionnaire), quality of life (any questionnaire about the physical and mental situation of patients), spinal function (any questionnaire or radiographical evaluation that explore physical function of the spine), OVFs anterior body compression ratio, intervention duration (includes bed rest duration or length of hospitalization), re-fracture (new OVFs that happened during follow up), Kyphosis angle (regional or global), Trunk flexor and extensor muscle strength, physical functioning (clinical tests like timed up and go or forward reach test), balance (through the center of pressure or sensory organization tests), gait spatiotemporal parameters, and plantar pressure were included from English language journals. The inclusion criteria were: (1) osteoporotic or age-related hyperkyphotic human participants with or without OVFs; (2) randomized or non-randomized prospective clinical trials with or without a control group; (3) specifying the type of orthosis used. Studies were excluded if they had healthy subjects or didn’t report any quantitative results. Additionally, non-English-language articles were excluded.
Search strategy
Search strategy table.

Study selection
All articles obtained by the search were imported to EndNote X9 (Thomson, Reuters, Carlsbad, CA), and one reviewer (FK) extracted duplicate or cross-references. Then the abstract of each article was evaluated independently by two reviewers (FK and MA). Disagreements between two investigators referred to consensual choice. A tertiary investigator (AB) is involved if there isn’t consent.
Data extraction
Reviewers (FK and MA) extracted details from the included article about the author, publication year, characteristics of participants, including mean age, sex, number in each group, type of syndrome, concomitant disorders and drugs, bone mineral density level, and features of the study such as design, aim, type of interventions (Orthosis and other interventions that were used in comparison with orthosis), all outcome measures with numerical reports, including variables describing the level of fracture improvement and duration of improvement, variables representing hyperkyphosis improvement, and variables describe Balance and gait parameters. Means and standard deviation for Anterior vertebral body compression fracture (AVBCP), Oswestry disability index (ODI), Thoracic Kyphosis angle, Back extensor muscle strength, sensory organization test (SOT), and gait speed for calculation of effect size extracted. The effect size was reported as the standardized mean difference (SMD) with a 95% confidence interval. These data were used for a meta-analysis of outcomes reported with different units and to compare the effect of orthotic types on variables and syndromes. If the reported data wasn’t based on the mean or Standard deviation, the study was excluded from the meta-analysis but still in review.
Methodological quality assessment
The Modified Downs and Blacks quality index (QI) tool is used for assessing the quality of methodology of all admitted studies by inclusion criteria. The QI tool is a checklist with 27 questions. This tool can evaluate Randomized controlled trials (RCTs) and non-randomized trials in four domains, including reporting via the first 10 questions, external validity via the following three questions, internal validity via questions 14 to 26, and power via the last question. The test-retest reliability (r = 0.88), inter-rater reliability (r = 0.75), internal consistency (KR-20 = 0.89), and criterion reliability (r ≥ 0.85) of the QI were reported. 31 None of the QI items were changed, and the total score of this tool was 28 due to one of the items that scored up to two points. Reviewers (FK and MA) assessed each article independently using the QI tool, and any discrepancy was resolved in the consensus meeting, and disagreements were referred to the third investigator (AB). Differences and a 95% confidence interval were determined.
Data analyses
Quality of included studies to meta-analysis.

Results
Study selection
The document’s title and abstract were evaluated according to inclusion criteria, and a context investigation for the final selection was conducted based on the review strategy. Discords were solved by consensus. A number of 4293 titles and abstracts were imported into EndNote X9, and after removing duplications and irrelevant items, 50 studies were evaluated in full text. Eight items due to insufficient data about orthotic intervention,16,32–38 two objects due to having different languages,39,40 two objects for including healthy subjects,41,42 one item with the qualitative design,
43
one entity with the case series design,
44
and two items for unclear results45,46 were excluded, and 34 studies remained into this systematic review (Figure 1), that fifteen of them included to the meta-analysis (Table 3). Flowchart depicting studies for the systematic review and meta-analysis. Type of orthosis used in acute phase of OVFs.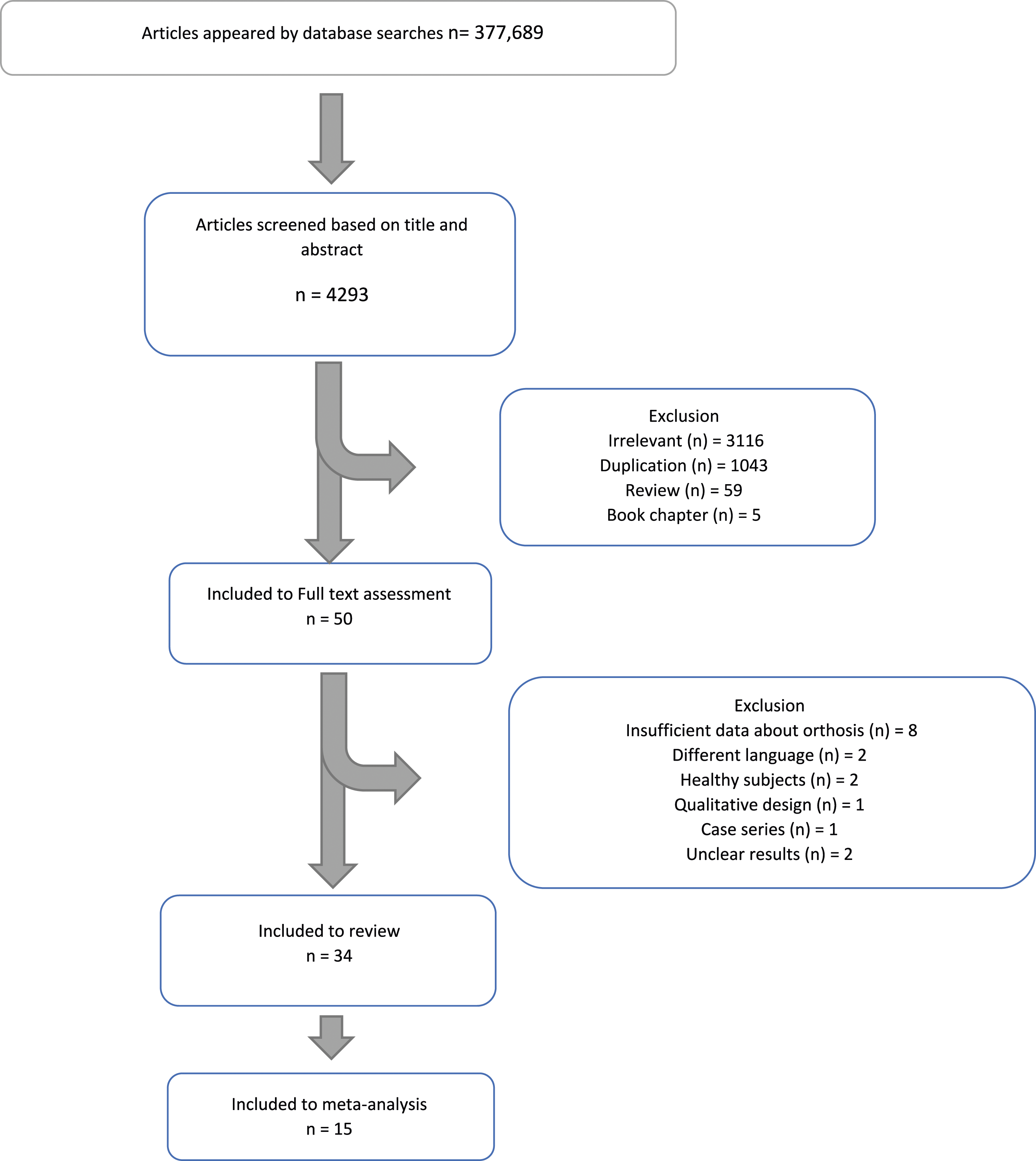

Study characteristics
Eight prospective non-randomized clinical trials, four future randomized clinical trials, and one case-control study with OVF patients in the acute phase (OVFs that happened in the last month), Two prospective randomized controlled trials, one prospective crossover study, and two trials with patients in the non-acute phase of OVFs (that happened in the last 6 month), six prospective randomized control trials, and four non-randomized clinical trials are included in this review. Besides, five trials assessed changes immediately after using an orthosis and compared them with the same patients without an orthosis, which were named “immediate effect” studies in this review. Orthoses designs were TLSO (Thoracolumbosacral orthosis), TLO (thoracolumbar orthosis), plaster jackets, three-point pressure, soft, Semi-rigid, and weighted with different names like PTS (posture training support), 47 WKO (weighted kypho orthosis), 48 DHB (Dynamic Hyperextension Brace), 49 or rucksack type orthosis. 46
Quality assessment of included studies
Downs and black scale scores for included randomized controlled trials to systematic review.

Downs and black scale scores for included studies to review that evaluated immediate effect - red numbers choose based on consensus.

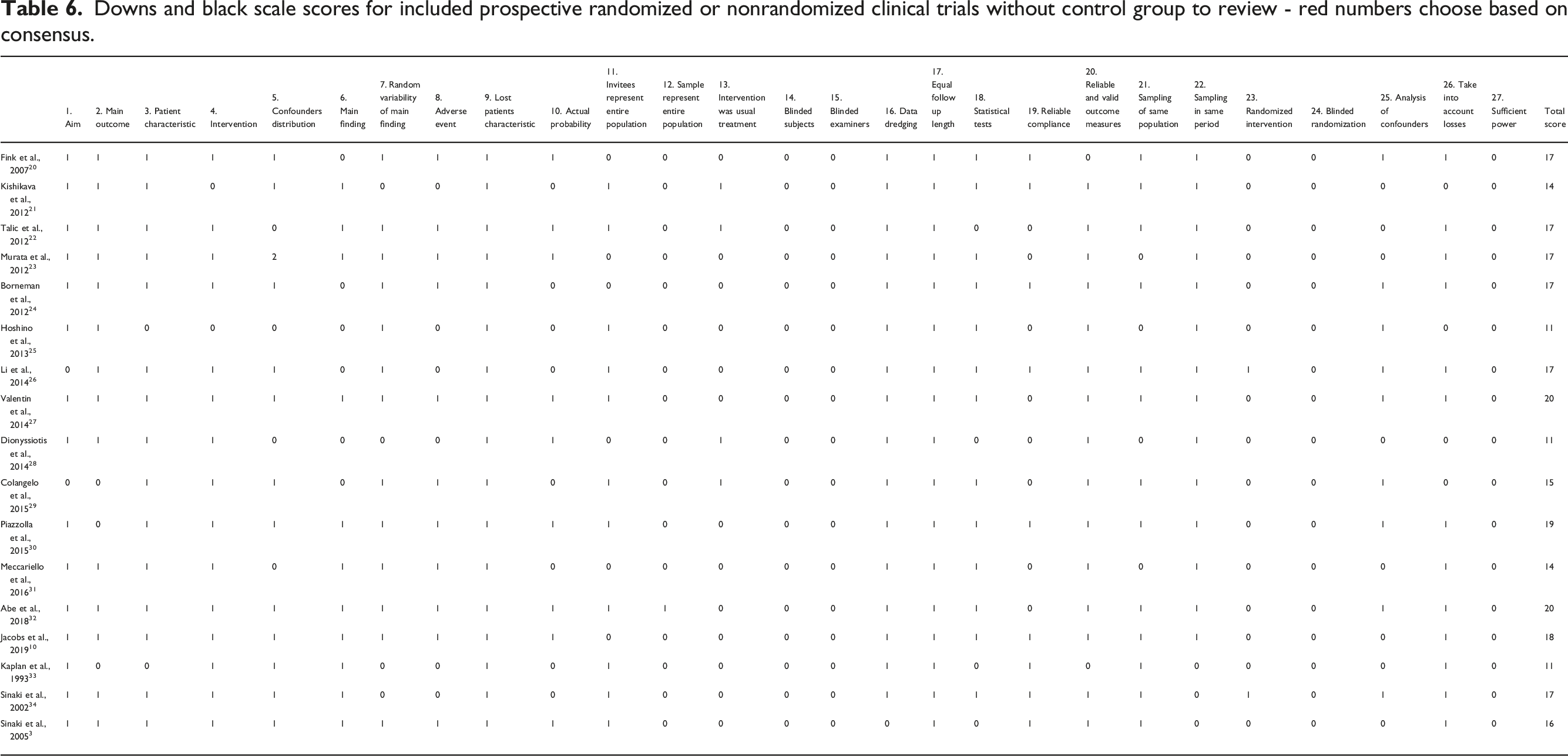
Downs and black scale scores for included prospective randomized or nonrandomized clinical trials without control group to review - red numbers choose based on consensus.
Effects of orthoses in osteoporotic patients (with or without hyperkyphosis or OVFs)
Orthotic interventions type
Traditional classification of orthotics may cause ignorance of dynamic or static effect of orthosis on spine. Considering the details of each orthosis in this review, we categorize them into four groups: movement restrictor designs, soft designs, semi-rigid designs, and weighted designs. Explanation of details, goals, and the manner of use for each orthosis design mentioned in the discussion (part 4.5).
Orthoses used in the acute phase of OVFs
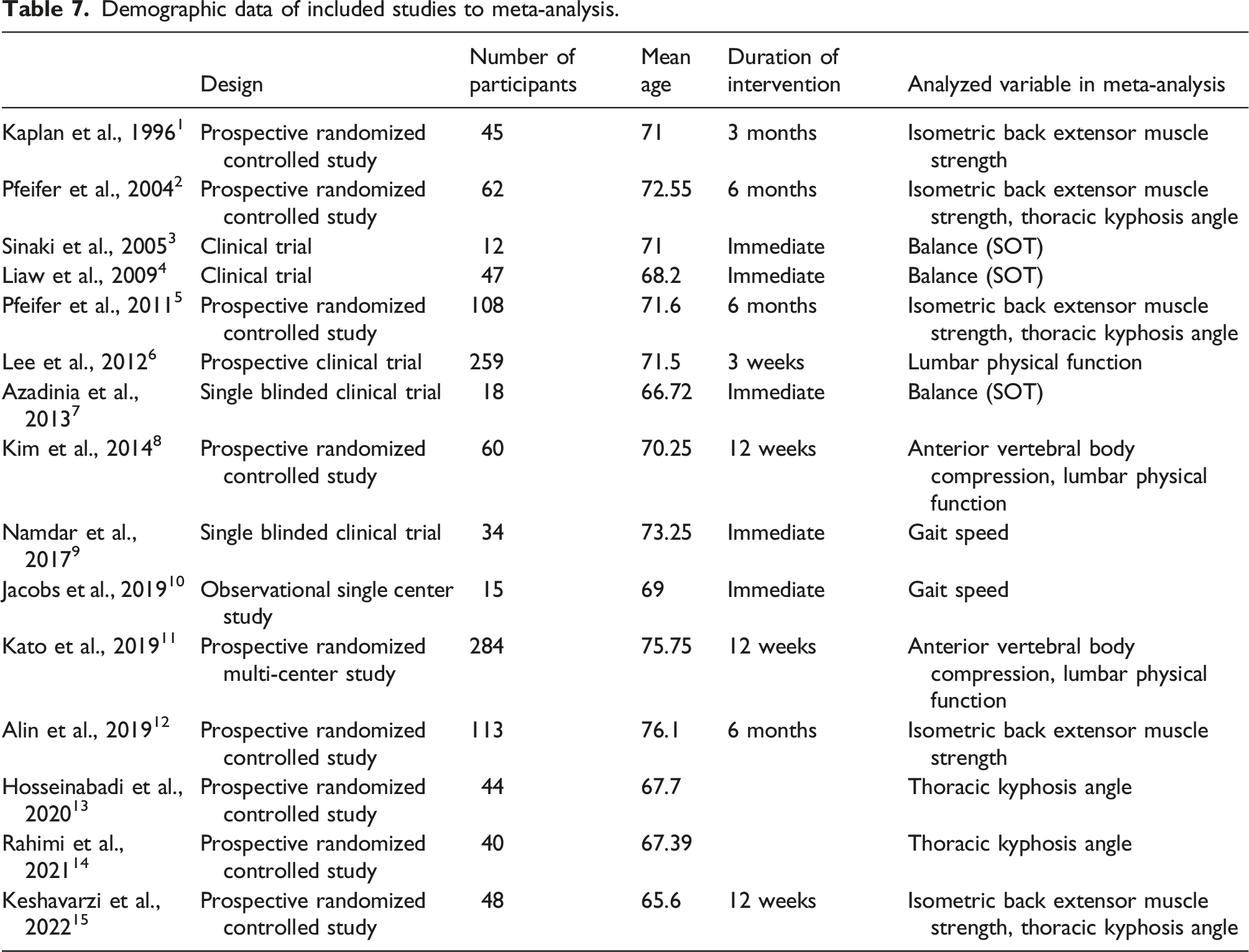
Demographic data of included studies to meta-analysis.
Orthoses were used in acute phase of OVFs.

The typical outcome measures in this part were the collapse rate of the anterior and posterior portions of the vertebral body, bone union rate or status, pain, number of refractures, and ODI scores. Additional outcome measures are detailed in (Table 8). As mentioned, we could enter three of the 13 articles in the meta-analysis with more than one group and report enough data after the intervention.13,52,53 Due to high heterogeneity (p = .000, I2 = 92.638, and Tau2 = 0.579), samples were sub-grouped based on groups in the study. Meta-analysis showed a significant difference between rigid TLSO and no orthosis (SDM = −2.401, p = .000, and CI = 95%) and inflexible TLSO and soft back orthosis (SDM = −2.640, p = .000, and CI = 95%) for ODI score (Figure 2) (Kim/Kato/Lee). Meta-analysis showed no significant difference between the effect of rigid or soft orthosis and no orthosis group for anterior body compression ratio (Figure 3). The VAS after the intervention was only reported in three articles; two of them used orthotics as a part of conservative intervention after approximately 1-month of bed rest with no control group,13,52,57 so the results weren’t solely the effect of orthotics. In 1961 patients, through 13 articles, 44 refractures happened in follow-ups in conservative groups, and 25 related to articles that exclusively used orthosis without rest or other interventions.50–54,58,59 Also, refracture in 10 cases and cement leakage in 24 patients were related to other interventions reported.13,50 Adverse events reported for the sole use of orthoses without rest were soreness, hernia, and pulmonary disease.56,59 4 of 13 studies had single-level OVF inclusion criteria,14,52,53,56 and one reported a fusion of vertebral bodies adjacent to OVFs.
54
Effect of orthosis on oswestry disability index in OVF patients. Effect of orthosis on anterior body compression ratio.

Orthosis in OVFs happened in the recent 6 months
Orthoses were used in OVFs happened in recent 6 months.
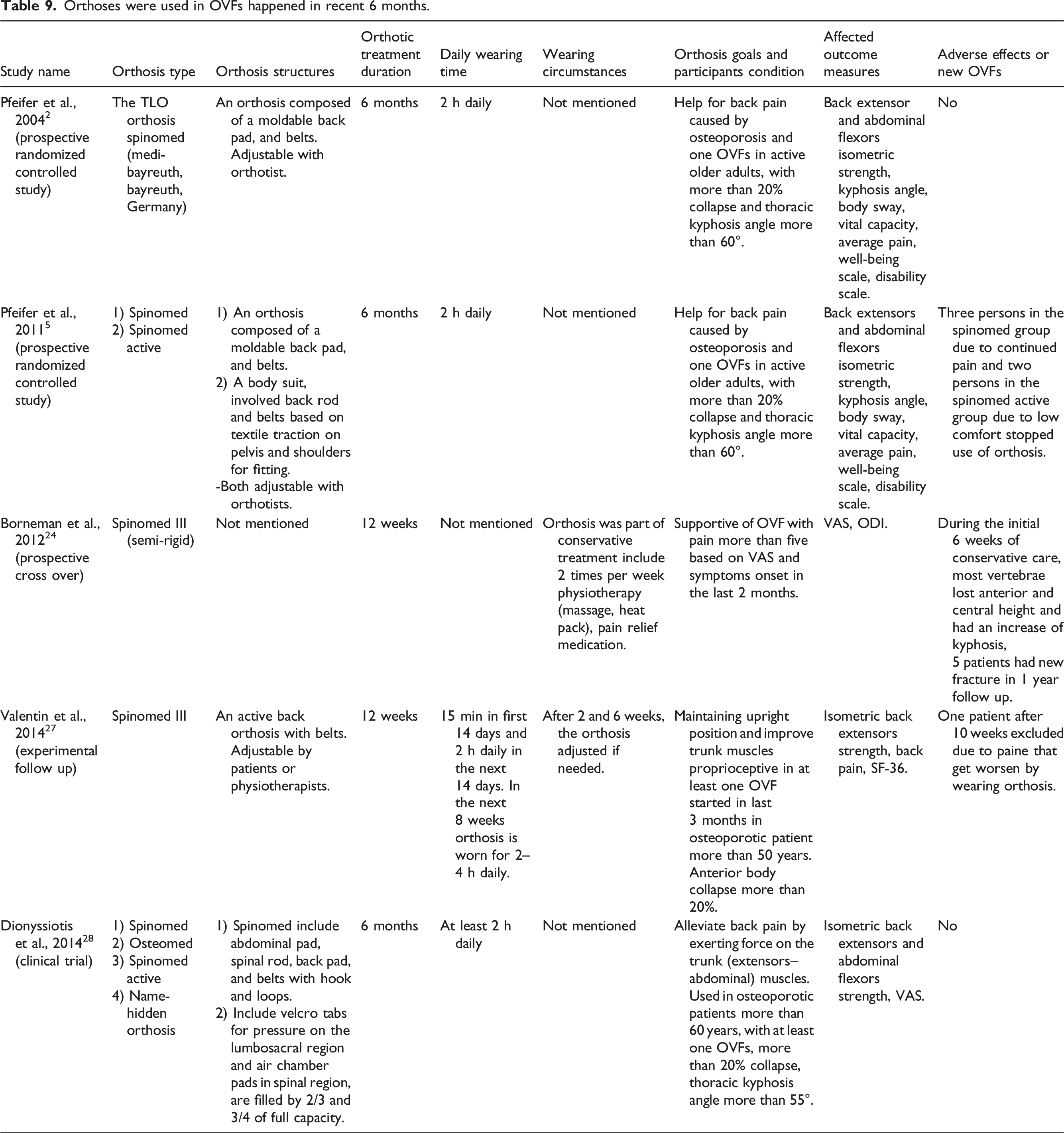
Three articles reported after intervention outcomes that one of them was excluded due to low methodological quality 60 and the remaining articles were related to each other 64 and had high quality with incontrovertible improvements in patients’ conditions.61,63 In these two articles, the mean pain of participants and their ability to extend and flex their trunk for muscle strength evaluation tests show that most of the participants weren’t in the acute phase of OVFs, so these two articles were included in the meta-analysis with the following articles that measured comparable variables.
Orthosis in hyperkyphotic patients with or without OVFs
Orthoses were used for hyperkyphosis or back extensor muscle strength improvement.

Thoracic kyphosis angle
The orthosis type used in the age-related Hyperkyphosis group was (Spinomed) in five articles, (semi-rigid TLO) in one article, (Elderly spinal orthosis) in 1 article and (DHB) in 1 article. Six articles mentioned orthosis manner of use. Five out of six used a semi-rigid orthosis 2 h daily for 12 weeks and one used a weighted orthosis named DHB. The DHB orthosis wore 12 h daily for 1 year.
Four of the 11 articles23,25,65,66 and two articles in part (3.5.2)61,63 assessed the thoracic kyphosis angle, but only five of these studies were included in the meta-analysis due to enough data for analysis.23,25,61,63,66 Another study had enough data on thoracic kyphosis angle, but this study’s orthosis type differed from TLSO-type orthosis.
49
The heterogeneity was (p = .000/I2 = 92.322/Tau2 = 1.253). So, the data is sub-grouped based on groups in articles. Meta-analysis showed significant differences between corrective exercise (accommodated every 2 weeks based on each patient’s condition) compared with ESO orthosis + exercise (SDM = −2.022, p = .000, and CI = 95%) and significant differences between corrective exercise (accommodated every 2 weeks based on each patient’s condition) compared with spinomed + exercise (SDM = −1.629, p = .000, and CI = 95%) and significant differences between semi-rigid TLO orthosis in 3 months compared with no orthosis as a control group (SDM = −1.316, p = .000, and CI = 95%) (Figure 4). One study in this group excluded the thoracic kyphosis angle meta-analysis graph due to heterogeneity.
23
Two studies had patients with OVFs,61,63 and three had pains between three and 6 VAS points.61,63,66 In four studies,23,25,61,63 orthoses were compared with no intervention. Other outcome measures related to balance, functional ability, back muscle endurance, and proprioception showed a significant relationship with kyphosis angle improvement, which wasn’t entered in the meta-analysis due to variety and the inability to compare. Effect of an orthosis on thoracic kyphosis angle.
Back extensor muscle strength
Three of the nine articles in this part (Table 10) and two articles in part (3.5.2) measured back extensor muscle strength and had more than one group entered the meta-analysis.24,25,61,63,65 Due to heterogeneity (p = .000, I2 = 92.784, and Tau2 = 1.216), data subgroups depend on reported groups. There were significant differences between PTS versus no orthosis (SDM = 1.645, p = .000, and CI = 95%), PTS versus conventional TLSO (SDM = 6.532, p = .000, and CI = 95%), conventional TLSO versus no orthosis (SDM = −2.633, p = .000, and CI = 95%), spinomed versus no orthosis (SDM = 1.566, p = .000, and CI = 95%), spinomed active versus no orthosis (SDM = 1.802, p = .000, and CI = 95%), and semi-rigid TLO versus no orthosis (SDM = 2.571, p = .000, and CI = 95%) (Figure 5). One study compared equipped exercise with spinomed, and no orthosis showed no significant differences.
65
The intervention duration in three studies was 6 months,61,63,65 in one study was 4 months,
24
and in one study was 3 months.
25
Three studies had hyperkyphosis inclusion criteria,25,61,63 and two had patients with pain and OVFs in the last 6 months.61,63 Effect of an orthosis on back extensor muscles strength.
In one article a WKO orthosis wore 1 h daily for 4 weeks and in another article, WKO wore 2 h daily only during activity for 4 weeks.48,67 One study used PTS 8 h daily while up and about for 16 weeks. 24 Five articles used Spinomed orthosis for different durations between 3 and 12 months, two to 4 h daily.60–63,65 One study used a semirigid TLO orthosis 2 h daily for 12 weeks. 25
Immediate effects of orthoses in osteoporotic patients
Orthoses were analyzed their immediate effect.

Sensory organization test
Three articles that used the Neurocom system and reported SOT test data before and after orthosis were included in the meta-analysis.67,70,71 There was heterogeneity (p = .000, I2 = 87.594, and Tau2 = 1.200). Therefore, a subgroup analysis was conducted. Significant differences in the comparison of WKO versus no orthosis (SDM = −1.442, p = .001, and CI = 95%), PTS versus no orthosis (SDM = 1.704, p = .004, and CI = 95%), and spinomed versus no orthosis (SDM = 1.628, p = .002, and CI = 95%) indicated. There were no significant differences between spinomed versus PTS and Knight Taylor versus no orthosis in the SOT test (Figure 6). Two articles had hyperkyphosis as inclusion criteria,67,70 and one study’s participants had OVFs.
71
Two studies reported LOS test data that evaluated directional control and reaction time and showed no significant difference between the orthosis and without orthosis conditions.70,71 Effect of an orthosis on sensory organization test (SOT).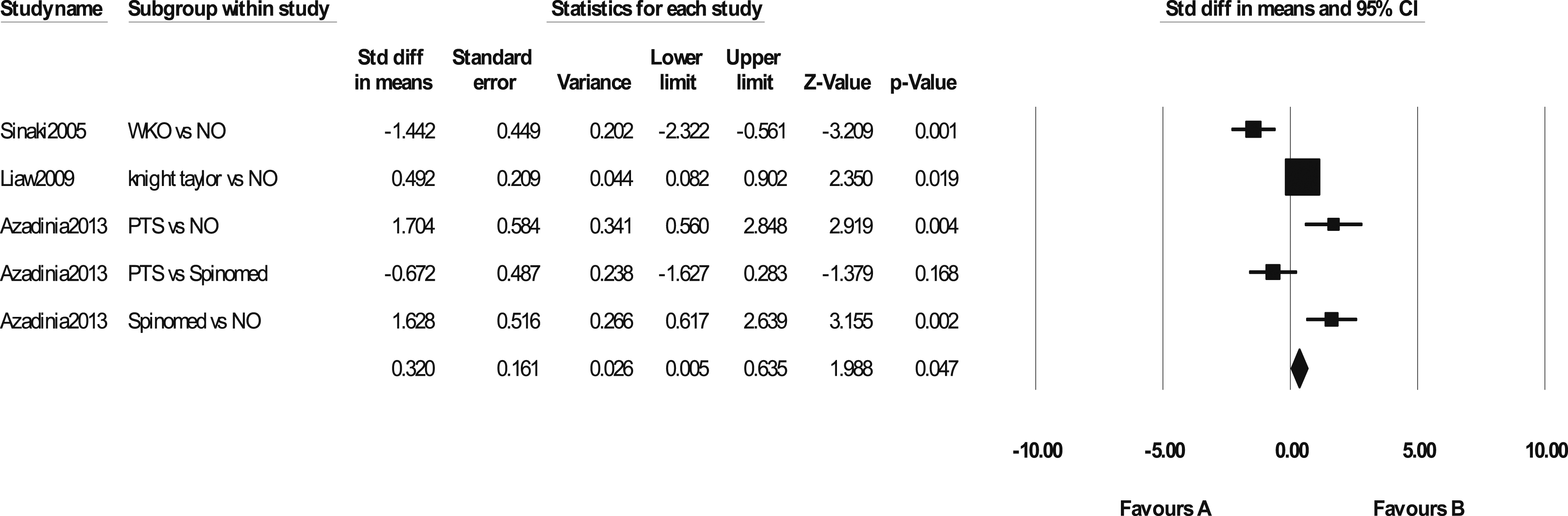
Gait parameters
Two articles measured spatiotemporal gait parameters before and after orthosis use in both first use and long duration after using orthosis,51,67 and one other article measured walking speed.
72
Walking speed was measured in two studies,51,72 entered into a meta-analysis, and there were no significant differences between the orthosis and no orthosis groups immediately (Figure 7). Immediate effect of an orthosis on walking speed.
Discussion
Quality
While four articles got more than 20 points on the QI scale,52,53,61,63 about six Articles with a quality score of less than 15 were excluded from the meta-analyses.47,58,60,68,69,73 The lowest scores, respectively, related to Internal validity confounding (selection bias) include random allocation, concealing the allocation of participants and evaluators, and reporting or evaluating confounding factors. Internal validity bias includes blinding and undefined sample sources. External validity includes distribution of confounding in the sample and treatment of most patients, reporting, and power-providing sample size calculation.
Even though 13 articles randomized intervention assignments and five concealed them from patients and examiners,24,49,53,70,72 the randomization still weakens the included studies’ quality. Some studies were multi-central,52,58 and some did not describe the source of the included participants.15,51,52,54,56,60,68,69,74 While blinding patients about orthosis is impossible, blinding them about the type of orthosis via placebo orthosis, 69 blinding examiners about the intervention group23–25,52,53,75 is possible. Only three studies reported the proportion of the sample to the source.14,52,53 11 articles reported power based on the primary outcome measure of effect size.13,23–25,52,53,61,63,65,70,72 A part of quality deficiencies relates to the nature of orthotic interventions that are usually optional and not the intervention for most patients. The score of the quality scale in two studies with the largest sample size52,58 decreased because they had a multicentral design. Considering reports from various studies mentioned in results, it is crucial to prioritize the evaluation of adverse effects in orthotic studies. Results of the QI score showed that 27 points on this scale are achievable in studies with orthotic interventions. Incomplete reports of results data and details of the method, more than the absence of randomization and blindness, made included studies to review inappropriate for the meta-analysis. In any trial, data before and after intervention always shows effectivity but without correlation of these data, the effect can’t compare with other studies in meta-analysis.
The design of some studies fails to distinguish the effect of physiotherapy or training from the effect of orthosis.14,15,49,55,66,75 There is evidence indicating that the impact of physiotherapy on healing during the acute phase of osteoporotic vertebral fractures (OVFs) 76 and supervised training on kyphosis angle 19 is greater than what is reported in studies on orthotics. Comparing exercise with orthoses using precise methodology can lead to different results. 65
Effect of orthoses in the acute phase of OVFs
Vertebral body compression ratio and Lumbar function quality were the most frequent variables reported in the studies included in this part of the review. Two studies, which only involved one level OVF participants, included in the meta-analysis based on quality score52,53 showed no significant difference in the anterior vertebral body compression ratio between patients who used orthoses and those who did not. One of these studies had a control group with no brace, and the baseline score of the ODI in this group was lower than that of two other groups with orthotic intervention, 53 mentioned in a review before. 21 So, it seems a full-time use of an orthosis in one-level acute phase OVF patients has no harmful effect on lumbar function based on the ODI scale score. Reported data for pain wasn’t enough for inclusion in the meta-analysis. 53 Besides participants have different sensitivity to analgesic drugs that aren’t measurable, 13 so pain assessments had a not enough quality to compare. Also, existing and prescribed orthoses only protect the spine from inadvertent flexions and movements that may hurt the spine again and cause pain. Evaluation of the effect of orthotics on pain debating when control group patients are conscious about body movements that may cause more pain. Orthoses can alleviate the pain of the fracture and improve healing if it has stimulators. 76 On the other hand, in most studies, orthosis wearing was full-time. Full-time immobilization of the spine for 3 months 24 or a long period of bed rest has irreversible effects on older patients’ lifetime, which increases the risk of disability and mortality.77,78 Any intervention that can help them ambulate independently in a shorter time after OVFs is a priority, and long durations of bed rest 79 or long duration of rigid orthosis wear is not the choice in unnecessary cases like one-level OVFs. If orthotic treatments are chosen, soft or semi-rigid designs while walking may eliminate adverse effects.
Conservative treatment in five studies includes physiotherapy or targeted muscle training14,15,55–57 and only two studies explained the details of the training. In this review, we excluded any studies that did not provide detail about the type of orthosis. These criteria may lead to the exclusion of studies that focus on training or physiotherapy.
Effects of orthoses in OVFs happened in the last 6 months
The inclusion criteria in the studies may significantly influence the outcomes. Five studies recruited osteoporotic patients who had OVFs in the last 6 months15,60–63 and two of them got the highest quality score of the QI tool in this review, showing the effectiveness of Spinomed in pain relief and kyphosis angle and trunk muscle strength and body sway improvements61,63 However, there is some debate around these findings because the exact age of the vertebral fractures was not reported in these studies61,63 and the ability of patients to contract muscles for strength tests may influenced by the nature of their fracture pain that is improving during the time. Also, participants of these studies61,63 had thoracic kyphosis angles higher than 60° in baseline evaluation. There is a relation between thoracic kyphosis angle and back muscle strength. 8 Patients with Hyperkyphosis probably had lower trunk muscle strength. It can be one of the reasons for the inability of other studies to prove their61,63 results. By the way, the results of these two articles confirm that wearing Spinomed according to the manner of use (2–4 h daily) is a beneficial treatment for osteoporotic patients with VAS pain score of fewer than five points that had one level OVFs in the last 6 months and Hyperkyphosis that affirmed before. 30 Orthoses with spring-like bars meet both the needs of movement limitation and moveability for patients and demonstrated a semi-rigid orthosis17,25 revealed significant improvement. In all studies, orthosis wearing time was 2–4 h daily.
Effect of orthoses in osteoporotic and hyperkyphotic older adults
There is a relation between back muscle strength, number of OVFs, degree of hyperkyphosis, and the number of falls in older adults.6,8 So, the prevention of OVFs and hyperkyphosis should be targeted. 80 The strength of back extensor muscles and thoracic kyphosis angle are vital variables that can prohibit osteoporotic vertebral fractures and falls in older adults. Based on this evidence, some orthoses are designed to improve spinal muscle strength and decrease kyphosis angle in osteoporotic patients.
Effect of orthoses on kyphosis angle
The thoracic kyphosis angle was measured in six studies before and after orthotic intervention.23,25,49,61,63,66 Two of them were not included in the meta-analysis due to heterogeneity or involving participants with new osteoporotic vertebral fracture (OVF).23,49 Based on the meta-analysis results, it was found that exercises designed by a specialist and tailored to each patient’s condition, with changes every 14 days, are more effective in reducing the thoracic kyphosis angle compared to orthosis and constant exercise. 66
A previous meta-analysis compared the effect of Spinomed orthosis with other conservative treatments, mostly different types of exercises, on kyphosis angle in patients of various ages. 19 Only one study compared two orthoses plus constant exercise with developing exercise based on patient condition. In Jenkins and colleagues’ study, only two studies of Pfeifer61,63 with osteoporotic patients experiencing pain due to OVF were included. Other studies in this part had no pain or OVF. Semi-rigid backpack-type orthoses, with no exercise, were found to have a significant effect on decreasing kyphosis angle in hyperkyphotic seniors compared to a control group with no treatments. This effect may be due to the periodic realignments of spring-like spinal bars and two-layer elastic stomach pads that increase abdominal pressure. 25
The number of studies that used an orthosis in age-related hyperkyphosis or osteoporosis isn’t sufficient to judge their effect on the thoracic kyphosis angle compared with other type of conservative treatments. 19 It is suggested that mixing exercise with an orthosis should be examined in a meta-analysis with groups that have exercise only, orthosis only, exercise and concomitant orthosis, and a group without any treatments, especially in a study that employs a crossover design for ethical reasons.
Effect of orthoses on back extensor muscles strength
According to a meta-analysis, PTS, Spinomed, and semi-rigid backpack-type orthoses showed a notable positive impact on back extensor muscles when compared to no intervention. Two studies48,67 were not included in the meta-analysis because they did not report a control groups or correlation between before and after the intervention.48,67 Additionally, one study that compared Spinomed with equipped exercise and no orthosis 65 showed no significant effect on none of the interventions. In this study, the thoracic kyphosis angle was not reported and hyperkyphosis was reported via flexible ruler index. The same orthosis in patients with OVFs happened in the past 6 months with a Kyphosis angle of more than 60°, and pain after the same intervention duration showed significant improvement in trunk extensor and flexure muscle strength.61,63 The decrease in thoracic kyphosis angle may be related to changes in back muscle structural variables. 8 Another study found that the use of a semi-rigid orthosis improved thoracic kyphosis angle in patients without pain and osteoporotic vertebral fractures (OVFs) within 3 months, leading to significant improvement in back muscle strength. 25 Some patients may prefer to keep using orthosis for more than 3 months, 43 but there is no evidence for the more beneficial effect of orthosis for longer-duration use. 61
Only one study compared the effect of Weighted orthoses on back muscle strength with a control group 24 and one compared thoracic kyphosis angle. 49 Kaplan et al. compared conventional TLO with no orthosis and PTS orthosis group in which only five participants were in the TLO group. Based on five patients’ data in this study, movement limitation with a soft TLO with complex inlays in osteoporotic patients makes back muscles weaker. 24 The Weighted orthoses were developed to improve posture and strengthen back muscles in osteoporotic patients. One study compared the effect of these orthoses on back muscle strength with a control group, 24 and another study compared the thoracic kyphosis angle 49 while both group participants had spinal extension training simultaneously.
Effect of orthoses in osteoporotic or hyperkyphotic patients on gait and balance
Effect of orthoses on dynamic balance
Three studies evaluated the effect of orthoses on dynamic balance in patients with hyperkyphosis, osteoporosis, or both.67,70,71 Orthoses types were a weighted orthosis (PTS, WKO),67,70 a semi-rigid orthosis (Spinomed), 70 and a movement restriction design (Knight Taylor). 71 Effects of initial and after 4 weeks of orthosis use on sensory organization test (SOT), 67 and the effect of one-time use of the orthoses on directional control and reaction time were reported.70,71 Osteoporotic patients with pain due to recent OVFs with a Knight Taylor orthosis compared with no orthosis showed a decrease in overall directional control and no significant differences for SOT and reaction time. 71 Besides, patients had increased average stability, percentage of ankle strategy and decreased average velocity of the center of gravity target sway, and a lower frequency of falls. 71 Another study compared the effects of a weighted orthosis (PTS) and a semi-rigid orthosis (Spinomed) in hyperkyphotic older adults and showed that both orthoses had a significant positive impact on SOT tests compared with no orthosis condition. Still, there were no significant differences in directional control or reaction time. 70 One study showed improvement in the SOT test after 4 weeks of 1 h’s daily use of WKO plus speed program exercise in osteoporotic hyperkyphotic patients. 67 It needs to be made clear whether the balance tests in this study were conducted with or without an orthosis.
Effect of an orthosis on static balance
One study analyzed the effect of the one-time use of three different TLSOs on hyperkyphotic older adults’ center of pressure (COP) displacement velocity. 68 Results showed an increase in the anteroposterior mean velocity of COP displacement, respectively, for rigid TLSO, soft TLSO, and semi-rigid TLSO and an increase in the mediolateral mean velocity of COP displacement for soft TLSO, rigid TLSO, and semi-rigid TLSO. 68 Mohebi et al. compared COP displacement velocity between Hyperkyphotic patients with or without osteoporosis and a healthy young group. Higher COP displacement velocity for anteroposterior displacement in hyperkyphotic patients versus the young group and higher velocity for mediolateral displacement in osteoporotic patients versus the young group were reported. 81 So, it seems a semi-rigid TLSO is a better choice than a rigid and soft TLSO in static balance, as a study reported a larger average, anteroposterior COP range in faller elderly that experienced hard damages after a fall compared with non-faller elderly. 82 Sinaki et al. showed hyperkyphotic patients have a more mediolateral and less Antero-posteriorly center of mass displacement compared with healthy older adults. 67 It can show that this population balance system tends to decrease anteroposterior displacement, and can lead to harmful falls. Fall prediction based on one variable of static balance is not possible. 83 Pfeifer et al. reported a decrease in body sway Velocity after 6 months of using spinomed as a semi-rigid orthosis.61,63 The Foot pressure of osteoporotic patients immediately after wearing a semi-rigid orthosis showed a pressure decrease in the forefoot region. 42 COP trajectory can be more explicator of elderly falls by variables like Sway area per unit time and anteroposterior and radial mean velocity. 84
Effect of an orthosis on gait spatiotemporal parameters
Three studies measured spatiotemporal gait parameters,51,67,72 and two of them included meta-analyses.51,72 Cadence improved after using a weighted and semi-rigid orthosis, but there was no significant difference in first-time or long-duration use of the orthosis on spatiotemporal gait parameters.51,67
Orthosis designs, goals, and manner of use
The design of each orthosis reflects the goals of the orthosis and the expectations of the medical profession. With respect to the effect of an orthosis on joints’ range of motion (ROM) and muscles’ electrical activations (EMG), 85 The orthoses’s designs transformed the logic of movement inhibition to movement restriction and also movement motivation in some situations. 63 As orthoses’s designs progress, our outlook on spinal orthotics in osteoporotic or age-related hyperkyphotic patients will be changed. In this part we have a look on the effect of different design of orthosis and the thru manner of use for each orthosis.
Semi-rigid designs
Orthoses made from spring-like or plastic uprights fitted into elastic or non-elastic soft structures like polychloroprene fabrics, elastic, and non-elastic fabrics that are enclosed by hook-and-loop fasteners. With this explanation, some of the orthoses used in articles as soft orthosis is a semi-rigid orthosis. 52 Spring uprights allow some flection while keep its constant alignments. The wearing time and manner of use ignored in some studies 15 and adverse effects that reported in one study may relate to manner of use. In this study, semi-rigid orthosis wore in sitting and standing positions and the exact wearing time during the day is not clear 56 The true manner of use for this type is, 2–4 h daily during simple upright activities.
Weighted designs
This orthosis consists of a non-elastic rucksack or backpack with 0.2 to 1 kg weights positioned at a specific distance from the scapula’s inferior angle and adjacent to defined vertebrae. The position, number of weights and wearing time varied across different studies. The PTS orthosis is used in patients with osteoporosis, kyphosis, scoliosis, etc. 47 Some studies reported the effects of WKO orthosis on back extensor muscle strength in osteoporotic patients with 4 h of daily use, 24 while others reported the impact of PTS on hyperkyphosis with 1-h daily use combined with an exercise program during activity. 67 11 studies utilized a weighted orthosis, with two not meeting the inclusion criteria.44,46
Movement restrictor designs
Five types of rigid spinal designs body jacket (full body orthosis made from two pieces of plaster or thermoplastic or sometimes made from one-piece lighter thermoplastics with an anterior opening design that covers Thoracolumbosacral region and shoulders), rigid TLSO (anterior opening thermoplastic and cover the Thoracolumbosacral regions but not shoulders), Taylor (steel rods shaped base on body size, covered with soft materials and restrict flexion, extension and lateral bending of the trunk), three-point pressure orthoses (steel bars making force on the sternum, pubis and back to restrict flexion and extension and some amounts of lateral bending of trunk mostly named Jewett or CASH or C35 orthosis), rigid TLO (light anterior opening thermoplastic and cover the Thoracolumbar regions), were commonly used in patients with vertebral fractures 86 and were used in some studies for osteoporotic vertebral fracture patients too.
Soft designs
These types are made from polychloroprene fabric or elastic or non-elastic fabrics and may include some plastic bars used for orthosis shaping. Some restrictions are due to increased abdominal pressure and the length of shoulder straps. The coverage of soft orthoses commonly is a thoracolumbar or lumbar region. Some designs have shoulder straps covering the thoracic region. Some designs may include different parts like air chambers of Osteomed. Commonly wore full-time.
Discussion summary
Only four high-quality studies are not enough to compare orthotic interventions with other treatments. In some studies, it is impossible to distinguish the effect of orthosis from other conservative treatments. Comorbidities are an important aspect of any research. The included studies reported comorbidities as a baseline distribution to show normality or excluded participants with comorbidities via inclusion criteria. It’s not possible to evaluate the effect of comorbidities on the result of intervention. We suggest that future studies consider common comorbidities such as diabetes, osteopenia, and progressive degenerative joint diseases in different groups.
The high-quality studies in the acute phase of vertebral fractures had single-level fracture inclusion criteria, which limited our results to single-level vertebral fractures. After the acute phase and 6 months post-fracture, back extensor muscle strength and the kyphosis angle improve in individuals with over 60 degrees of hyperkyphosis and less than five-point pain with a semi-rigid brace. The kyphosis angle and back muscle strength can improve in osteoporotic patients who do not have vertebral fractures or are not in the acute phase of fractures with weighted or semi-rigid orthosis.
The orthosis effect on dynamic balance is well defined, but static balance can be evaluated with variables representing the balance situation. The number of studies assessing walking parameters is insufficient for discussion. Any type of orthosis has a prescription and manner of use that should be considered for utilization.
Limitations and future directions
In this study, we aimed to investigate the true effect of spinal orthotic interventions in osteoporotic patients. However, due to low methodological quality or lack of reported data, our meta-analysis is based on less than 10 articles, which limits the strength of our conclusions. We found that only one of three studies in the acute phase of osteoporotic vertebral fractures (OVFs) had a control group, and one of them was a multicenter study. Other studies in this group used orthosis combined with other treatments, making it difficult to isolate the effect of the orthotic intervention. We recommend that future studies use better methods, including control groups with no treatment or separable groups with enough reporting of results. Additionally, we encourage future studies to report correlations between before and after intervention data, as these correlations are critical for evaluating the effectiveness of interventions and allow for comparisons with studies that have no control group.
Conclusion
This systematic review and meta-analysis propose that using soft or rigid orthoses solely has no beneficial effect on interventions in the acute phase of OVFs compared with no orthoses in one-level fractures. Besides, using semi-rigid or weighted orthoses in osteoporotic or hyperkyphotic older adults with or without OVFs significantly affects thoracic kyphosis angle, back muscle strength, and balance improvements.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.