
Abstract
Introduction
Individuals with acquired brain injury may find it difficult to self-manage and live independently. Brain-in-Hand is a smartphone app designed to support psychological problems and encourage behaviour change, comprised of a structured diary, reminders, agreed solutions, and traffic light monitoring system.
Aim
To evaluate the potential use and effectiveness of Brain-in-Hand for self-management in adults with acquired brain injury.
Methods
A-B mixed-methods case-study design. Individuals with acquired brain injury (n = 10) received Brain-in-Hand for up to 12 months. Measures of mood, independence, quality of life, cognition, fatigue, goal attainment, participation administered at baseline, 6 and 12 months. Semi-structured interviews conducted with acquired brain injury participants (n = 9) and healthcare workers (n = 3) at 6 months.
Results
Significant increase in goal attainment after 6 months use (t(7) = 4.20, p = .004). No significant improvement in other outcomes. Qualitative data suggested improvement in anxiety management. Contextual (personal/environmental) factors were key in influencing the use and effectiveness of Brain-in-Hand. Having sufficient insight, appropriate support and motivation facilitated use.
Conclusions
Brain-in-Hand shows potential to support acquired brain injury, but further work is required to determine its effectiveness. Context played a pivotal role in the effectiveness and sustained use of Brain-in-Hand, and needs to be explored to support implementation.
Keywords
Introduction
Acquired brain injury is a heterogeneous condition resulting in cognitive, emotional and behavioural impairments,1–3 which are often difficult to predict and make long-term rehabilitation challenging. Acquired brain injury is the leading cause of death and disability in young adults 4 and over one million people live with the long-term consequences of injury.5,6 Acquired brain injury can have a detrimental impact on quality of life, limiting independence and restricting participation in daily activities.7,8 Individuals often find it difficult to self-manage their condition, meaning they rely on others to support them in daily activities. 9 A lack of self-awareness, defined as ‘the inability to recognise deficits resulting from one’s injury’, 10 may impact on a person’s ability to self-manage and set appropriate goals. Self-management is important as people with acquired brain injury need to be able to recognise their limitations and make informed decisions, without the support of others. 11
The multifaceted nature of acquired brain injury means that rehabilitation interventions need to be individually tailored. Although many smart technologies exist to support some problems experienced following acquired brain injury, such as cognitive impairment, there is insufficient evidence to support the use of personal smart technologies for improving clinical outcomes in this population. 12 There are also multiple known challenges of implementing such interventions in complex settings like the UK National Health Service (NHS). Some of the barriers faced when implementing these technologies include resistance to change from traditional practice among therapists 13 and the translation of knowledge from technology developers to clinicians. 14 There is a need for effective rehabilitation interventions that support independent living and self-management post-injury, which can be tailored to different needs and settings. With anticipated growth in the number of hospital admissions, alongside increasing social care costs, interventions need to focus on reducing societal pressure and health and social care reliance.
Brain-in-Hand is a smartphone application (app) that has been implemented in autism and mental health settings. Brain-in-Hand supports users by providing a structured daily routine for tasks and problem situations (see Figure 1 for summary). The technology was specifically engineered to support the management of persistent emotional and behavioural problems such as anxiety and depression - commonly seen in people with acquired brain injury. Users are able to self-monitor problems (e.g. anxiety, fatigue) using a traffic light system. Any activity is sent from the app to an online ‘cloud’ in real time, which can be reviewed by the user and nominated mentor(s) (e.g. treating occupational therapist). Schematic of Brain-in-Hand system, from planning to data monitoring.
The aim of this study was to evaluate the potential use and effectiveness of Brain-in-Hand for adults with acquired brain injury. The specific objectives were to: 1. Identify barriers and facilitators to Brain-in-Hand use. 2. Determine whether Brain-in-Hand use was associated with improved outcomes related to goal attainment, mood, functional independence, quality of life, cognition, fatigue and participation. 3. Evaluate the acceptability of Brain-in-Hand from the perspective of people with acquired brain injury and healthcare workers after 6months’ use.
Methods
A mixed methods A-B case design was used. Participants were recruited across three UK NHS sites and local charities for people with acquired brain injury between July 2016 and March 2017. Ethical approval was granted by NRES Committee East Midlands Nottingham 2, reference number 16/EM/0141. Participants with acquired brain injury were recruited by one author (JK). The initial approach was from a member of the NHS usual care team – e.g. an occupational therapist, or by a charity volunteer. Participants with acquired brain injury were also identified and approached by independent sector therapists, solicitors and case managers. Potential participants were informed of all aspects pertaining to their participation in the study (quantitative and qualitative data collection methods). For those interested, a visit was organised (face-to-face or over the phone) with the researcher, who took written informed consent.
Participants were both people with an acquired brain injury and healthcare workers. People with a brain injury were included if they were: (1) between 18 and 65 years of age; (2) diagnosed with an acquired brain injury; (3) at least 3 months post-injury/stroke; (4) had a smartphone and were competent at using it, and (5) had at least one problem as a result of their acquired brain injury that potentially limited their functional independence. People with communication difficulties resulting from acquired brain injury (e.g. severe aphasia) with no support from a relative or carer were excluded, as this may have limited participation in study activities such as setting up the device and the interviews. Healthcare workers were eligible to participate if they were treating or supporting a person with acquired brain injury (e.g. occupational therapist, support worker) who was participating in the study, and consented to participate.
As this was a series of case studies, no power calculation was performed. We aimed to recruit up to 15 people with acquired brain injury to take part in the case studies; a number considered sufficient to reach data saturation, 15 as enough information would be obtained to inform the design of a subsequent study (e.g. feasibility trial). Given the in-depth nature of case studies, a sample size of at least five is recommended. 16
Assessment schedule.

HADS: Hospital anxiety and depression scale; NEADL: Nottingham extended activities of daily living; MSNQ: Multiple sclerosis neuropsychological screening questionnaire; CIQ: Community integration questionnaire; GAS: Goal attainment scaling; FAS: Fatigue assessment scale; EQ-5D-5 L: EuroQol 5-dimensions 5-levels.
Measures were chosen, which were reliable, valid, and easy for participants to complete, thus minimising participant burden. The intention was to capture information about impairments and functional limitations that Brain-in-Hand could potentially support, as its use in acquired brain injury was largely unknown prior to the study. The Nottingham Extended Activities of Daily Living was chosen because it indicates competence with activities of daily living and was short, thus limiting participant burden.
At least two goals relevant to each participant were set at baseline using Goal Attainment Scaling. 23 Potential goals were discussed with the participant’s treating occupational therapist (if applicable) prior to, or during the baseline session to ensure goals were relevant and attainable. Goals were then identified by the participant and discussed with the researcher (JK). Patient-stated goals were recorded and converted into SMART (Specific, Measurable, Achievable, Realistic, Time-bound) goals. Where necessary, the researcher (JK) contacted the treating therapist to clarify the patient goals. Goals were reviewed for attainment at 6 and 12 months post-intervention. This method was chosen as goals could be weighted to reflect importance, and attainment scores calculated across the study period using a spreadsheet. 23
Semi-structured interviews were conducted with participants with acquired brain injury and healthcare workers at 6 months since beginning to use Brain-in-Hand. Data were collected on acceptability of Brain-in-Hand, and barriers and facilitators to use. Interviews were audio recorded and transcribed. Example interviews questions are shown in Appendix 1.
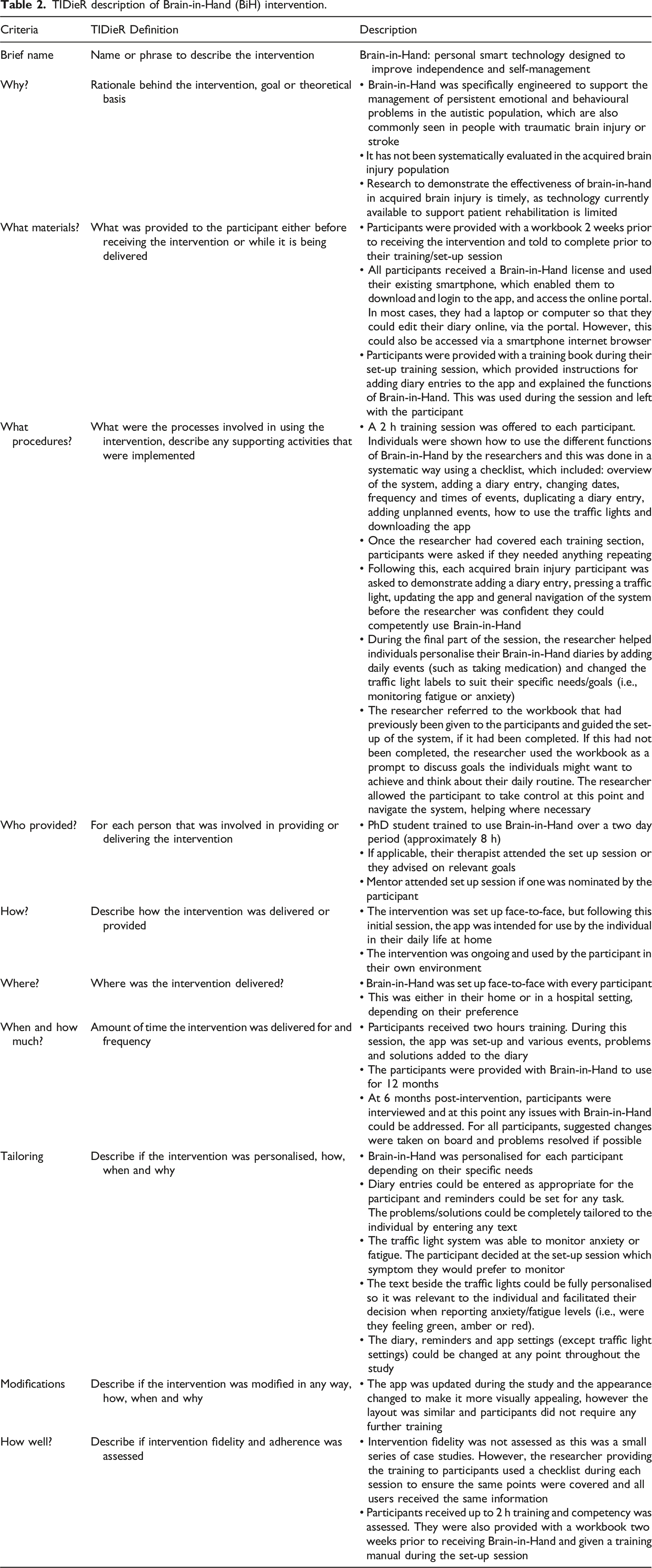
TIDieR description of Brain-in-Hand (BiH) intervention.
Quantitative data were analysed to present the perceived change in mood, functional independence, fatigue, cognition, quality of life, goal attainment and participation for participants with acquired brain injury measured using questionnaires. The suggested clinical cut-off scores were identified from published sources.25–27 Difference in scores for individual cases, mean averages across cases and mean differences were statistically analysed. For parametric tests, mean averages and standard deviations were presented for comparison between the questionnaire measures with associated p values. Overall response rates and completeness of questionnaires returned were assessed. All analyses were completed on IBM SPSS version 22.0 and GraphPad Prism version 6.0.
Interview data were analysed thematically using the Framework approach
28
to elucidate factors influencing the effectiveness of Brain-in-Hand and the barriers and facilitators to its use, and acceptability. The coding matrix was informed by the Behaviour Change Wheel
29
and International Classification of Functioning, Disability and Health (Figure 2).
30
Summary of International Classification of Functioning, Disability and Health (ICF) components for acquired brain injury (ABI).
The International Classification of Functioning, Disability and Health was chosen for its focus on functioning and disability, and personal and environmental contextual factors (Figure 2), which are important to understand the use and acceptability of a smartphone app like Brain-in-Hand. Each component can interact with another component in two directions, meaning that any intervention affecting one area can potentially affect outcomes in another. The International Classification of Functioning, Disability and Health provides a common language for reporting the qualitative findings. In the context of acquired brain injury, it has facilitated the identification of barriers and facilitators of interventions and enabled the exploration of effect on functional states (impairments, limitations, and restrictions). The Behaviour Change Wheel suggests that behaviour change is dependent on three components: capability, opportunity, and motivation. As Brain-in-Hand is intended to influence behaviour change, the Behaviour Change Wheel seemed a logical choice for the interview topic guide. It was also used successfully to identify barriers and enablers to Brain-in-Hand use in a previous study. 31
Interview transcripts were coded independently by two authors (JK and AW). Data were analysed using NVivo (QSR International Pty Ltd). Codes were compared and collated into themes. Findings were triangulated with the authors, people with acquired brain injury, and healthcare workers to enhance validity of findings.
A convergence coding matrix 32 was used to synthesise and integrate the quantitative and qualitative data. Themes across both datasets were searched for agreement and disagreement between the two methods. The synthesised data were coded according to their complementarity, disagreement or silence.
Results
A total of 14 people were recruited to the study, 10 were adults with acquired brain injury and three healthcare workers (two occupational therapists and one support worker) (Figure 3). A summary of the acquired brain injury participants’ characteristics is shown in Table 3. Recruitment diagram. Summary of acquired brain injury participant characteristics. alower score indicates a negative outcome. blower score indicates a positive outcome. HADS: Hospital Anxiety and Depression Scale; NEADL: Nottingham Extended Activities of Daily Living; EQ-5D-5L: EuroQol 5-dimensions 5-levels; CIQ: Community Integration Questionnaire; MSNQ: Multiple Sclerosis Neuropsychological Screening Questionnaire; GAS: Goal Attainment Scaling; FAS: Fatigue Assessment Scale; SD: standard deviation; OT: Occupational therapist; NP: Neuropsychologist; PT: Physiotherapist; SLT: Speech and language therapist; NC: Not completed. Red coloured numbers indicate probable clinical impairment/presence of the outcome in question (i.e., anxiety, depression, cognitive impairment).

Quantitative findings
Summary of quantitative data collected at baseline, 6 and 12 months post-intervention.

ameasures where a higher score indicates a positive outcome.
bmeasures where a lower score indicates a positive outcome.
HADS: Hospital Anxiety and Depression Scale; NEADL: Nottingham Extended Activities of Daily Living; EQ-5D-5L: EuroQol 5-dimensions 5-levels; CIQ: Community Integration Questionnaire; MSNQ: Multiple Sclerosis Neuropsychological Screening Questionnaire; GAS: Goal Attainment Scaling; FAS: Fatigue Assessment Scale; SD: standard deviation, CI: confidence intervals. ***paired t-test, significant difference in scores (p < .05).
Example goals set using Goal Attainment Scaling (GAS).

Participants Goal Attainment Scale scores increased significantly between baseline (mean = 37.21, SD = 0.76) and 6 months (mean = 53.9, SD = 11.02); t(7) = 4.20, p = 0.004) (Figure 4, Table 4). Although there were no significant changes in any other outcome measures, there was a mean decrease in Multiple Sclerosis Neuropsychological Screening Questionnaire scores between six months and 12 months post-intervention (mean change = −3.75, SD = 8.50, CI –10.85 to 3.35). Mean Goal Attainment Scale (GAS) scores with interquartile range and range at baseline, 6 months and 12 months post-intervention.
Some negative scores were reported, including a mean decrease in Community Integration Questionnaire scores between baseline and 6 months (mean change = −3.38, SD = 7.23, CI –9.42 to 2.67), indicating an initial reduction in participation. There was also a mean decrease in Nottingham Extended Activities of Daily Living scores between baseline and 6 months (mean change = −0.75, SD = 3.66, CI –3.81 to 2.31).
Qualitative findings
An overarching theme of context was identified as a key influencer of Brain-in-Hand use and effectiveness. We define context as an individual’s situation, or factors involving the person and the surrounding environment. 30 Within this, four main themes were identified. Having appropriate support (set up, monitoring and goal identification/revision), motivation and self-awareness appeared to facilitate Brain-in-Hand use.
Insight and self-awareness
Insight emerged as a common theme running through the interviews. Analysis highlighted the need for people with acquired brain injury to have a level of self-awareness for Brain-in-Hand to be useful. Individuals who have some insight and self-awareness are often more able to self-monitor and self-correct behaviour. Participants who had insight into their limitations tended to have more realistic expectations of Brain-in-Hand and how it could help them. They were also more aware of when they needed to change behaviours and amend goals, or use the app to change their routine (e.g. taking more rests in the day to manage fatigue). After using Brain-in-Hand for 6 months, one participant became more aware of his anxiety and recognised that he needed to manage this better. By using the app, this person appeared to gain greater insight into when he became anxious and developed ways to control these feelings: Yeah, it’s [using the Brain-in-Hand traffic lights] made me face up to that I have got like an anxiety problem because it’s not linked to any kind of depression or anything like that… yeah and this [Brain-in-Hand] reminds me all day that I need to be mindful. (Participant 5, male, traumatic brain injury)
However, one therapist suggested that even when individuals have a level of insight, they might not know when to press the appropriate traffic light. Some acquired brain injury users might struggle to recognise symptoms of fatigue or anxiety, which makes it difficult to monitor when these ‘red’ episodes (i.e. highly fatigued/anxious) appeared most frequently. The occupational therapist mentioned that one barrier to Brain-in-Hand use and its effectiveness and might be users’ inability to recognise or acknowledge their symptoms: I think for our patients, I think they’re trying desperately not to press that for ‘I’m struggling’, we wanted them to press it [Brain-in-Hand traffic lights] for fatigue, but again you’ve still got an insight issue for am I fatigued or do I want to press this button. Erm they’re trying to prove to themselves that they can cope, they don’t want to press the button [red traffic light]. (Participant 11, occupational therapist)
Some individuals may have found it hard being honest with themselves when rating their fatigue/anxiety levels and accepting that they have a problem.
Support and training
Interviews revealed that ongoing support and training would be beneficial for Brain-in-Hand users. Training for healthcare workers was highlighted by occupational therapists as an important facilitator to provide them with the knowledge and explore potential uses of Brain-in-Hand for supporting their patients. Appropriate support was also a key facilitator to the effective use of the intervention. One participant chose his wife as his Brain-in-Hand ‘mentor’. Although initially useful for self-monitoring, the participant admitted he was not honest when monitoring his fatigue levels as the study progressed. This meant that he was not using the traffic lights appropriately and therefore not benefiting from this component of the app: I don’t want to let Kim know that I am struggling, but Kim doesn't really see that I am struggling erm and as she's my wife more than anything else I don't want to let her think I am struggling too much because she will probably dump me…so there is a fear of upsetting… maybe it should be somebody else other than Kim so I get support from another angle without Kim needing to be worried. (Participant 2, male, acquired brain injury)
Participants highlighted the need for frequent contact with the Brain-in-Hand support team (based within the company) to ensure the app was working correctly and to prompt them to think about things they were struggling with (e.g. diary entries). Linking back to the theme of insight, some people may not have the self-awareness to ask for help when the app is not working. This was identified as an issue for a number of participants; several did not ask for help when they needed it. One participant forgot her password that was set during the initial training session and failed to request support. As a result, she did not use Brain-in-Hand for several weeks.
Motivation to use the app and change behaviours
Many participants admitted to lacking motivation and some recognised that this affected their use of Brain-in-Hand. Reduced motivation impacted on the effectiveness of Brain-in-Hand and goal attainment. Some individuals were motivated to maintain Brain-in-Hand use, as they were achieving goals and could see the benefits. One person said the app was like having a friend, which motivated him to use it, as it was an opportunity to think about how he was feeling: Well at the start it was a bit of a friend really, erm and yeah it was nice to have it pop up on my phone how are you feeling because it was making me think how I was feeling at the time. (Participant 5, male, traumatic brain injury)
The impact of reduced motivation was evident for some individuals who did not frequently use the traffic light system and lost interest over the 12-months intervention period. There was also a connection between unachieved goals and demotivation.
Technology
Participants identified a number of barriers to use and potential improvements for Brain-in-Hand, which might facilitate its use in the acquired brain injury population. Most participants mentioned that being able to edit the app on the smartphone or smart device would improve accessibility. The current system only allowed users to update reminders on the online portal rather than their phone - which was a barrier to those with memory impairment who needed to be able to access the diary ‘on-the-go’. Others felt that the reminders needed follow-up notifications to ensure they had completed a task. One participant who was using the app to manage fatigue, spoke about reminders for rests. That’s the other thing as well, when you, when it says rest, you complete it, but you, you're pressing rest you've completed your rest before you have your rest. So then if something comes up and stops you from having the rest when you've had your reminder to have your rest, say like a phone call comes through or a client phones you up, then you've failed to have your rest. (Participant 2, male, acquired brain injury)
One participant struggled to act on instructions he received by phone. His support worker had noticed that the phone reminders did not work for this person who needed direct instructions: But if it’s like a reminder that’s not, it’s not a direct instruction, it doesn’t seem to have the same effect, like James said he’ll think ‘oh, I’ll do that in 10 min’ and then he’s forgotten, erm which brings me onto my next bit that it needs to follow that up. (Participant 13, female, support worker)
The support worker also discussed the need for follow-up reminders on the app to check that users had actually completed a task. Other participants discussed the need for tasks to have a start and finish, especially if tasks were related to activities that could be completed immediately. Users found the traffic light monitoring system to be the most useful part of Brain-in-Hand, although a few people preferred the reminder function.
Data convergence
Convergence coding matrix.

The outcome measures did not capture all of the potential benefits of Brain-in-Hand that were mentioned in participant interviews. The data were discrepant on one aspect – anxiety. The quantitative data showed no improvement in mood (measured using the Hospital Anxiety and Depression scale) across participants, however some individuals qualitatively reported the benefit of using Brain-in-Hand for anxiety management, suggesting that the app (specifically the traffic light monitoring system), was improving anxiety levels. Quantitative measures of independence/functional outcomes did not significantly improve across participants, however for six individuals, the Nottingham Extended Activities of Daily Living score did increase. This complemented the qualitative data, finding that some participants felt empowered after using Brain-in-Hand and other felt they had regained independence by prompting them to complete daily tasks, such as taking their medication and doing therapy exercises.
In addition, the converged data suggested that support was important to all participants, in terms of motivation, but also ensuring they could troubleshoot any technical issues. After the 6 months interview, contact from the researcher became less frequent and support was effectively withdrawn (even though participants were encouraged to contact the research team at any time). At this point, Brain-in-Hand usage dropped and task completion decreased, suggesting that ongoing support was important to encourage participant use. The change in usage is shown in Figure 5. The qualitative data supported this, as participants consistently highlighted the need for support, to help with technology problems, motivate them to continue using the app, and talk them through updating their diary, reminders and solutions. Data exported from the Brain-in-Hand app showing the change in usage over time.
Discussion
The data obtained from each participant provided valuable information about the potential uses of Brain-in-Hand for individuals with acquired brain injury and identified technological improvements necessary for implementation in this population. Overall, Brain-in-Hand helped participants set and achieve goals and, in some cases, facilitated self-management.
Personal and environmental (contextual) factors, such as insight and self-awareness, relationships, environment, support and services, determined the extent of use, and need to be considered when implementing Brain-in-Hand, or similar interventions. Context, plays a pivotal role in the effectiveness and long-term use of Brain-in-Hand. It is clear that such contextual factors (insight, ongoing support, training, motivation, technology) need to be considered and appropriate for the acquired brain injury user, if Brain-in-Hand is to work in this population; an idea which was reflected throughout the interviews. This is something that should be considered when implementing smart technologies and the infrastructure surrounding the use of such technologies (i.e. the context in which it will be delivered) needs to be better understood before they can be effectively implemented.
Although a lack of engagement and motivation are common issues when implementing smart technologies like Brain-in-Hand, it appeared that additional support and self-awareness may improve compliance in the acquired brain injury population. Unrealistic goals and lack of motivation can result from impaired self-awareness or lack of insight, 33 which means that this group of individuals could benefit from additional support when setting goals and using such technologies. This highlights the need for training in goal setting for those involved in setting up the app for use, or the need for involvement of the therapy team, where rehabilitation is ongoing.
Convergence coding facilitated the synthesis of quantitative and qualitative findings, and offered greater insights into the data than individual analysis.34,35 Where data did not completely converge, it offered complementary information about the key themes and provided context to the quantitative outcomes. As there was no clear change on most quantitative measures (other than a significant increase in goal attainment), it appeared that Brain-in-Hand had been largely ineffective. However, convergence of data highlighted potential reasons for poorer outcomes, such as the impact of life changes (e.g. relationship breakdown, general lack of motivation), which were not specifically linked to Brain-in-Hand.
The convergence of data also emphasised environmental (e.g. support, training) and personal barriers (e.g. insight, motivation), that need to be addressed prior to implementation of Brain-in-Hand in a healthcare setting. Barriers included appropriate support in terms of technological troubleshooting, but also support for the individual to help with goal setting and monitoring app usage (e.g. a therapist reviewing patient usage and changing reminders/problems within the diary). This is a barrier that needs addressing prior to implementation and could be provided by the company or a relevant charity (currently provided by the National Autistic Society for Brain-in-Hand users with autism), and/or the treating therapist who could provide ongoing monitoring and motivation.
Additional barriers were lack of motivation, inability to identify a personal need for the technology (i.e. poor insight). Although this may be a challenging barrier to overcome, a potential solution ahead of a feasibility study would be to test the technology under optimal conditions (e.g. on specific individuals who had insight into the impact of their injury on functioning and wanted to work towards achieving relevant goals). Adequate training was also important for patients and clinicians, to ensure users were aware of the app functions and how they could use them effectively; a lack of structured training for clinicians was a barrier to use. Before moving to a trial, a training package will need to be developed to ensure that healthcare workers (e.g. rehabilitation therapists) understand the potential uses of Brain-in-Hand, the software and how to support users. This study suggested that the support provided to Brain-in-Hand users was as important as the app itself. Although set-up sessions were provided to acquired brain injury participants in this study, further development to this training package would need to be carried out ahead of a feasibility trial.
Convergence of mixed methods data was important to understand more about who Brain-in-Hand could potentially support and suggest potential outcomes to be measured in a future feasibility study (such as goal attainment, self-awareness, fatigue or anxiety). Individuals recruited to a future study would need to be aware of the impact of their injury and impairments, such that they could set relevant goals and recognise the need for Brain-in-Hand.
The findings of this study suggest that technologies like Brain-in-Hand can be divided into two components (Figure 6): the ‘Big T’ (context) and the ‘small t’ (content). The ‘small t’ refers to how the technology actually works (i.e. its nuts and bolts). It includes the physical components of Brain-in-Hand - smartphone app and online portal. The ‘small t’ can be thought of as the intervention ‘content’ and the device that individuals will use. Without addressing barriers associated with this part of the technology, it would not be as effective and sometimes not work at all. Barriers include losing the smartphone, the app not working correctly, losing login details and having no access to a computer to edit the Brain-in-Hand app. The ‘Big T’, is the system as a whole. As with the content of the intervention, the context is equally important and if barriers associated with this are not addressed, the technology will be less effective or not used. The ‘Big T’ refers to many interacting components that can either hinder or facilitate successful implementation. Context not only refers to the environment, but also the personal factors such as motivation, insight and capability. Therefore, researchers should consider both when designing and evaluating interventions. Representation of the two elements necessary for the long-term implementation of technologies like Brain-in-Hand.
One of the main issues associated with the use and effectiveness of the app is adequate support for users, something which is already provided for Brain-in-Hand users with autism. A 1-year subscription for such users includes 4 h of personalised planning and set-up support sessions, access to Brain-in-Hand software and on-demand remote support from a Response Service (following the press of a red traffic light), which is provided by the National Autistic Society. A potential solution to ensuring adequate support is available for acquired brain injury users is offering a response service via a brain injury charity (e.g. Headway, UK Acquired Brain Injury Foundation), or by a support worker, however this would require additional funding and training. Another solution would be to embed Brain-in-Hand in specialist NHS rehabilitation and support (including out of hours support) funded by the NHS. Brain-in-Hand has the potential as an adjunct to NHS rehabilitation particularly as the online cloud enables a healthcare worker, such as an occupational therapist, to see what their patient is experiencing in real time and how (or if) they are managing. This may lead to revised support or rehabilitation strategies, rather than trial and error approaches, which often rely on patient self-reporting over time; this is particularly challenging for patients with memory problems.
The idea of context and content has been corroborated by other researchers, highlighting their importance in implementation36–38 and influencing rehabilitation outcomes, 39 and are some of the known challenges and barriers to implementation.14–16 However, there is limited evidence supporting the interaction between the ‘Big T’ and the ‘small t’, with many studies focussing only on the environmental context (i.e. setting) rather than the intervention as a whole (i.e. environmental, personal, and technological factors).
One of the main strengths of the study was the A-B case design, which enabled a more in-depth exploration of the data collected from each individual. This design was chosen to understand more about who could benefit most from Brain-in-Hand following acquired brain injury to inform the design of a future trial. This study sits between the theoretical development and the feasibility/pilot phases of the Medical Research Council framework, 40 which are concerned with developing the underlying programme theory for, and identifying the underlying mechanisms of the intervention. Although some participants withdrew, which may have been due to the length of the study and a lack of ongoing support, we saw the 12-months study duration as a strength rather than a limitation because it offered insight into the use of Brain-in-Hand in clinical practice over time and its potential for failure if users were unsupported and goals not reviewed. The integration of methods and the use of convergence coding to determine whether findings converged with or diverged from each other was a further strength, providing insight across cases and findings. It not only highlighted the challenges faced when evaluating complex rehabilitation technologies like Brain-in-Hand but was useful in identifying participant selection criteria, potential outcome measures and issues to address in training and set up for a future trial.
The study has limitations. This was a small study where we aimed to recruit participants with a range of injury severities and breath of problems so that we could identify who (and what impairments) might benefit from using Brain-in-Hand. This was a strength but also a weakness, because the sample was small and heterogenous with no specific focus or similar baseline characteristics, thus a broad set of outcome measures were required. There were minimal changes in the majority of outcomes, which may have been related to the insufficient sensitivity of the measures used (i.e. unable to detect relevant change), the lack of similarity among participants, or a lack of effectiveness of the intervention. The short training period provided to participants in line with the usual practice for Brain-in-Hand (users with autism receive 2 h training) may not have been enough for the acquired brain injury population.
In a future study, participants may benefit from shorter and more frequent sessions over the first 4 weeks, to reinforce learning and facilitate their understanding of its context in everyday life (i.e. how can it help them achieve goals, why do they need to use it, why is the potential of Brain-in-Hand for them long term). This would also provide an opportunity to troubleshoot issues as they arise, thus ensuring users understand all components of the app.
Conclusion
Brain-in-Hand did not appear to benefit all people with acquired brain injury who had impaired insight, or poor motivation, however we did note improvements for some individuals. The findings suggest that Brain-in-Hand is more helpful for individuals who have insight into the difficulties presented by their impairments (even if they aren’t aware of the extent of them), and individuals with cognitive impairment that require Brain-in-Hand to support planning and decision making. There was also a clear benefit of Brain-in-Hand to improve goal setting and attainment in these individuals. People who reported an improvement in cognitive function, set memory and planning related goals at baseline, suggesting that Brain-in-Hand might be useful for reminding and structuring daily routine. The main barriers to implementation were linked to a lack of or inappropriate support/training, lack of motivation to use Brain-in-Hand, a lack of insight and self-awareness to set realistic goals and identify a personal need for Brain-in-Hand, and technical problems preventing participants from using the app. It is important that both the content and context of interventions like Brain-in-Hand are consistently reported by researchers, so that technology can progress and common barriers avoided. Both the content and context are pivotal to the success of such interventions; however, contextual factors require greater focus during the early stages of implementation research.
There appears to be a potential use for Brain-in-Hand to support this population, however the wider context and infrastructure may be limiting its success. Although, this study sheds light on some the issues Brain-in-Hand could support, further work needs to be conducted to better understand the potential uses of such technology in acquired brain injury.
Footnotes
Acknowledgements
The authors would like to acknowledge the support of Brain in Hand Ltd. throughout this research, for providing app licenses for all participants, and providing technical support to the researchers and participants where necessary. The authors would like to acknowledge the support of the staff at the recruiting sites and participant identification centres in conducting this research. We would also like to thank all participants for taking part in this research.
Author Contributions
JK contributed to the main writing of the paper, with additional input from all authors. JK and AW conducted all interviews. Qualitative data analysis was conducted by JK and AW, then reviewed by KR and RdN. Quantitative data analysis and synthesis of data was conducted by JK. All authors critically reviewed the final version of the manuscript for publication. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JK was a PhD student at the time of conducting this research, funded by a Hermes Fellowship, the University of Nottingham and Brain in Hand Ltd.
Guarantor
JK is the guarantor and corresponding author.