
Abstract
Introduction
In this paper, we study the support needed by professional caregivers of those with dementia, and present a first step toward development of VIPCare, a novel application with the goal of assisting new caregivers at care-centres in interacting with residents with dementia.
Methods
A mixed-methods study including two questionnaires, two focus groups, and seven co-design sessions with 17 professional caregivers was conducted to (a) understand caregivers’ challenges/approaches used to reduce negative interactions with persons with dementia, (b) identify the existing gaps in supporting information for improving such interactions, and (c) co-design the user interface of an application that aims to help improve interactions between a new professional caregiver and persons with dementia. A pre-questionnaire assessed knowledge of smartphones and attitude toward technology. A post-questionnaire provided an initial evaluation of the designed user interface.
Results
Focus groups emphasized the importance of role-playing learned through trial and error. The layout/content of the application was then designed in four iterative paper-prototyping sessions with professional caregivers. An iOS/Android-based application was developed accordingly and was modified/improved in three iterative sessions. The initial results supported efficiency of VIPCare and suggested a low task load index.
Conclusions
We presented a first step toward understanding caregiver needs and developing an application that can help reduce negative interactions between professional caregivers and those with dementia.
Introduction
Professional dementia caregiver 1: “I have always explained that you walk into these doors, there are [30] residents…and you live in 30 different realities in a matter of 24 hours, so you have to figure out which one you are in.”
As quoted above by one of our participants, taking care of individuals with dementia introduces many challenges for professional caregivers. As dementia advances, those affected tend to lose the ability to make sense of their immediate environments, and often misconstrue events—including their own sense of who they are in that place and time, as despite cognitive decline, persons with dementia (PWDs) retain the sense of who they are, 1 and this sense is crucial to their wellbeing and quality of life. As cognitive memory of places, names, and roles fades, PWDs come to rely more heavily on the affective components of memory and their longstanding sentiments about the roles and identities that they have had in their lives. This means that people with dementia will often act like the person they feel they should be, not who others expect them to be in the situation at hand. 2 For example, a mother who has previously been a teacher may think that she is the teacher even when talking with her daughter. Therefore, she may expect her daughter to interact with her as if she was a teacher and to treat her with formal respect rather than love.
The family caregivers learn how to interact with PWDs over time, by changing their own roles and reactions according to who the person believes she/he is in the moment. However, interacting with PWDs may become a challenge for those without the shared history and daily contact of long-time family caregivers. Such people can include new professional caregivers at care-centers with multiple different residents and family members who see their affected loved one infrequently.
Providing care for PWDs in residential nursing facilities can be a demanding job with long hours and low pay. 3 Not only does it involve physical effort and direct personal care but a huge investment in emotional labour that often goes unrecognized. 4 Although professional caregivers have been shown to engage in many informal strategies to manage this work,5,6 they often lack important knowledge and prefer not to work with PWDs.7,8 Although models such as person-centred care 9 aim to address this, as Hung et al. 10 (2018) point out, many staff do not feel prepared to deliver this kind of care to PWDs. The current study seeks to understand how to provide technological support to newly placed nursing facility staff (i.e., professional caregivers) as they navigate the process of learning successful interaction with unfamiliar residents with dementia. To that end, we asked professional caregivers about experiences and challenges that they face daily, and asked what information can be important for new professional caregivers.
Prior research has shown that the most effective interaction strategies are based on the long-held self-sentiments and identities of the PWDs. To help professional caregivers quickly gain an understanding of the most effective interaction strategies based on the self-sentiments and identities of the PWDs, we draw on Affect Control Theory (ACT), a socio-cultural theory of affective interactions between people, 11 which can be a powerful predictor of humans’ behavior. Based on ACT, a psychological need to maintain consistency motivates people’s actions, emotions, and perceptions. In ACT, sentiments are represented using three dimensions (valence/evaluation, arousal/activity, and dominance/power), which can be fundamental to one’s interpretation of outcome of events on an emotional level. 12 Therefore, using this theory could be an effective approach to identifying behaviors and emotions that will align with the expectations of persons with dementia in specific situations, thereby reducing negative interactions.
Our longer-term goal is to develop VIPCare: an application that aims to help new staff (professional caregivers) at care-centers or visiting family members to learn how to interact successfully with the PWD for whom they care. The app will be tailored to the self-sentiments of each PWD (i.e., who the PWD feels she/he is) in a residential facility, as obtained through biographical interviews. 13 Based on those self-sentiments, the app will identify what identity the PWD is most likely to adopt when he or she is unable to make sense of their environment. Returning to our introductory quote, the app would train and assist the professional caregivers by helping them to identify the “reality” in which the PWDs are operating and providing cues about the approaches that can lead to successful interactions, when helping PWDs in Activities of Daily Living (ADLs). Such an application may help reduce the likelihood of negative outcomes of interaction, which has the direct goal of aiding professional caregivers in achieving their objectives more easily. It also may have the consequence of reducing anxiety of PWDs, thereby improving the quality of their lives.
To gain insights into what such an application would look like, we included in our interviews with professional caregivers’ questions about how an application should be designed and what information it should contain to successfully assist new professional caregivers. To ensure that the application would be successful, it is important to involve users (professional caregivers in this case) in the design process. This paper describes the first step in this process (prior to engaging persons with dementia): understanding the information that is important to include and the preferred design for this app from the professional caregivers’ perspective.
Background
Human-centered design emphasizes including users in the design process, or designing with them as opposed to designing for them. 14 Participatory design can ascribe agency to users, 15 empower them, 16 and provide researchers with more insights to create the successful/preferred product. 17 The methodology for the co-design process is usually selected according to the targeted users. For example, a recent study by Lazar et al. 14 suggested art therapy as a means to facilitating communication with individuals with specific health conditions (e.g., depression, dementia, and stroke).
If communication does not introduce a challenge but users have limited exposure to technology, paper-prototyping can be an effective approach to understand users’ needs. Paper-prototyping is a common approach for developing and improving design of user interfaces and is considered as a technique of usability testing, 18 or a method of brainstorming, designing, creating, or testing user interfaces, as defined by Snyder. 19 It is mostly appropriate for creating prototypes for interactive applications that mainly involve flat screens (e.g., mobile apps). 20 Paper-prototyping enables researchers to test the product with users before developing the product, to ensure that it meets users’ needs. 19 Iterative paper-prototypes can help ensure that users are involved in the process of developing the app and reduce likelihood of an outcome that does not meet users’ needs.19,21,22
However, as Snyder 19 points out, paper-prototyping is suitable for certain problems, such as conceptualization, learning about the workflow and necessary content, and understanding the preferred page layout and functionality of an application. However, it may not be ideal for assessing aspects of the application that require direct interactions with the application (response time, scrolling, colors, etc.). In these situations, the actual product needs to be tested. Therefore, we believe that a combination of paper-prototyping and co-design on an actual mobile app is ideal, as it enables us to learn about users’ needs and preferences about the contents/layout of the application, as well as test the other aspects that are more technical.
Multiple applications have been developed for people with dementia and their caregivers. For example, the “iWander” app 23 is created to monitor movements of a person with dementia and alert caregivers, enabling caregivers to monitor the person with dementia remotely. The “Care and Connect” application is also designed to rate public places on their dementia-friendliness, that is, how suitable they are for persons with dementia and their caregivers.24,25 Also, multiple applications are proposed and developed to monitor cognitive abilities of persons with dementia, to predict onset of dementia, 26 or to assess individuals’ risk or provide suggestions on how to decrease such risk. 27
Furthermore, many applications have been developed to improve social interactions of persons with dementia. For example, an app called “Ticket to Talk” was designed to stimulate discussions between younger people and older people with dementia (e.g., through a set of assorted media). 28 However, to the best of our knowledge, applications that are designed to train new caregivers—especially the professional staff who take care of multiple residents—to successfully interact with persons with dementia has seen limited attention.
Method
The study consisted of four parts: (a) a survey assessing professional caregivers’ experience of using smartphones, (b) two focus groups, (c) seven co-design sessions, and (4) pilot evaluations. All elements of this study involved only professional caregivers. Our caution in this development process is not undue, as many long-term care facilities require functional products to be tested, and it is more difficult to start prior to a lengthy design phase.
Procedure
Before focus groups and co-design sessions were conducted, a general survey was designed and disseminated at the dementia care wing of a long-term care facility. The residents of this facility include a range of older adults with and without disabilities, as this mid-sized long-term care facility offers a range of services, such as rehabilitation, assisted living, skilled nursing, and dementia care. The dementia wing—in which our studies were conducted—has staff that work only with residents with dementia, as well as a few “floaters” who work in multiple wings as needed.
Professional caregivers were asked to submit their responses to the surveys at their convenience. Two focus group sessions and seven co-design sessions were held afterward. The study was concluded by asking participants to respond to a questionnaire evaluating the final prototype.
Smartphone knowledge/usage survey
A survey was designed to assess professional caregivers’ knowledge and exposure to smartphones and smartphone apps, as well as their general attitude toward technology. The survey consisted of (a) general questions (e.g., Do you have a smartphone? If not, why did you choose not to have one?), and (b) The smartphone usage and attitude toward technology sub-scales from the Media and Technology Usage and Attitudes Questionnaire (MTUAS). 29 The smartphone usage questionnaire measures how often a user uses the smartphone for specific applications, for example, “read email on a mobile phone” or “browse the web on a mobile phone.” These questions were rated on 10 scales ranging from “never” to “all the time.” The attitude toward technology questionnaire evaluates users’ attitude toward technology by providing statements such as “I feel it is important to be able to find any information whenever I want online” and “I get anxious when I don’t have my cell phone.” These statements were evaluated on a continuous scale with 5 marks, from “strongly disagree” to “strongly agree.”
This survey was available for the staff members at the dementia wing and they were asked to put their anonymous responses in a provided box. It enabled us to better understand our sample and their familiarity with technology.
Focus groups
In the focus groups, our goal was to understand (a) professional staff’s everyday interactions with the residents, (b) the tasks they help the residents with, (c) the challenges they face daily, and (d) how they handle those challenges. Further, we asked what professional caregivers would expect from VIPCare (the app) and whether they believed that such application would be useful. The topics discussed in the focus groups were: 1. What are the different situations/interactions you have with residents? How do you handle them? 2. What are the tasks? What kind of tasks do you have daily? 3. How do you know how to deal with different residents? 4. If the resident does not listen to you, how do you change your action? 5. How do you train new staff to do all of these? 6. Who needs help learning to interact with people with dementia? Who do you think could use the app?
Thematic analysis was used to analyze the data from the focus groups. Themes were coded by hand, guidelines in 30 were followed for analyzing and reporting data. All the discussions in the focus groups were used (as the sessions were recorded), and were then coded for themes.
This step enabled us to understand whether there is a need for the app and who the potential users might be. All focus group sessions were audio recorded. One of the authors also took notes during the focus group sessions to ensure that we will not miss any important information.
Co-design sessions
After completing the focus group sessions and based on their outcome, we held a total of seven co-design sessions. In four of the sessions (6 participants), the participants were asked to design the application that they thought would be effective and efficient through paper-prototyping. Figure 1 shows an example of the setting. We used templates of iPhone or iPad and participants were presented with different tools such as sticky notes and examples of UI elements (e.g., search boxes, scrolls). In these sessions, participants decided on (1) the amount/type of information to be included in the app, (2) the way they want to phrase the instructions, (3) the tasks they would like to include in the application, and (4) the app’s design and the way they want to navigate through different screens. Example of the paper-prototyping setting. Templates of iPhone and iPad were printed in their actual sized (iPhone 8 and iPad mini).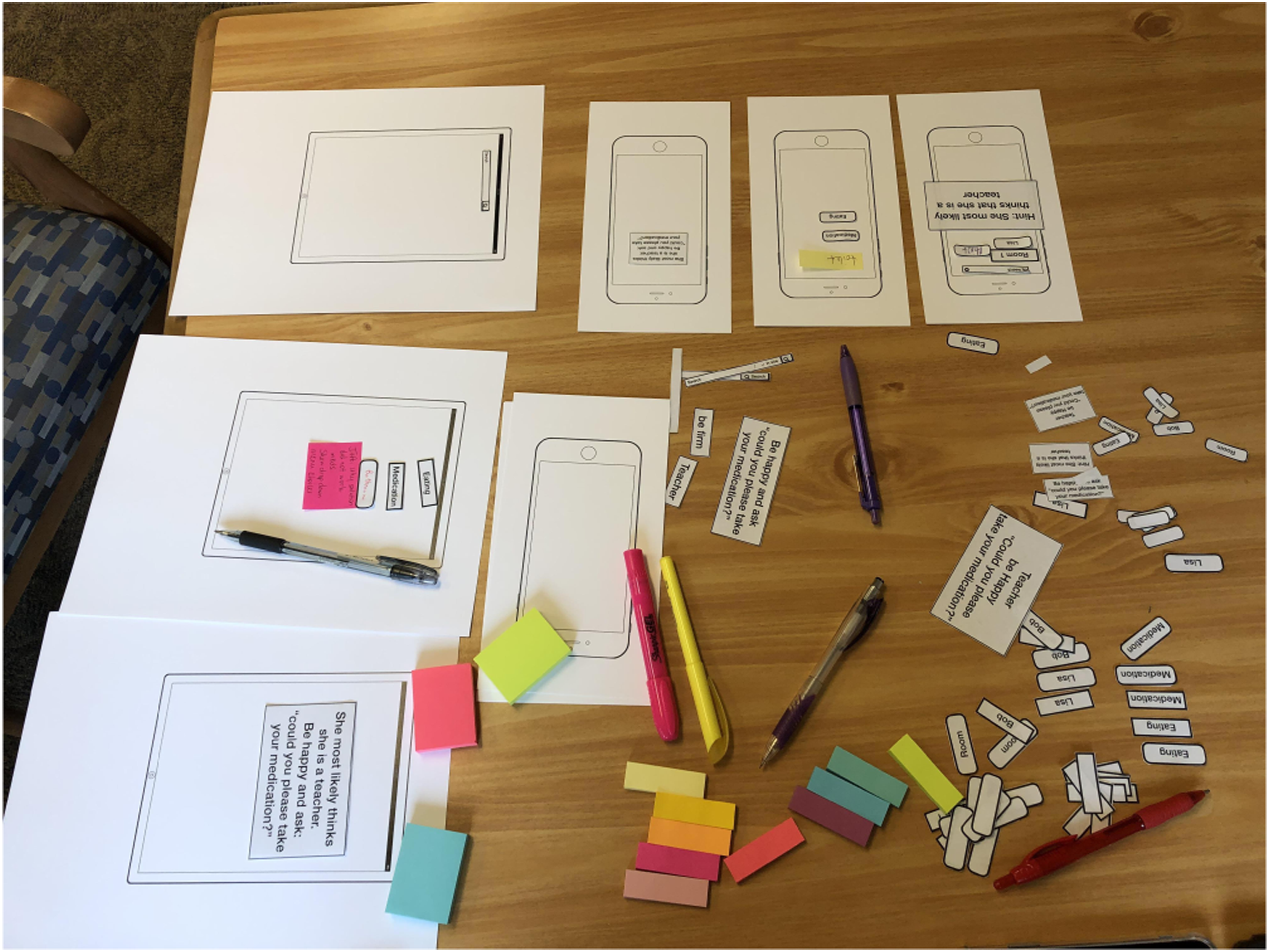
Paper-prototyping was used in the beginning because as Buxton argues, it is important to start with a method that enable us to “get the right design as well as get the design right.” 31 Because our participant group had a relatively lower exposure to technology, paper-prototyping was selected.
After the paper-prototyping sessions were concluded, the application was implemented and an iOS and Android-based app was created according to the outcome of the paper-prototyping sessions. The applications were then presented to the participants on an iPad mini* or iPhone XR† (depending on their preference), who tested it and suggested further changes. Changes were applied before showing the app to the participants in the next sessions. All decisions about the design (e.g., number of screens, navigation, visualization, type, and amount of information) were proposed by the participants. The researchers did not influence their decision-making and only asked questions that would motivate the participants to think further about different aspects of the application that might be important (how detailed the suggestions should be, what they want to see after pressing a button, etc.).
Initial evaluation of UI
The application was evaluated on different scales of NASA Task Load Index (NASA-TLX) 32 : mental demand, physical demand, temporal demand, overall performance, effort needed, and frustration level. Although the participants did not use the application to interact with the residents, they worked with the application in the real setting (while they were working in the center), and were assumed to imagine that they are assisting a resident while using the app.
In addition to the six NASA-TLX questions, we asked participants about another aspect of temporal demand: how time consuming they thought the app was. This is because professional staff at the care-centres are very busy helping multiple residents and we wanted to know whether they thought it would take them too much time to use the app. This questionnaire was used only as a pilot evaluation of UI to learn about possible changes that may be necessary to facilitate working with the app, which were not covered in the co-design sessions.
Both focus group sessions and co-design sessions were conducted at a table in the staff break room, located on the dementia wing of the long-term care facility. The initial evaluations were conducted where caregivers were the most comfortable, and in the majority of cases it was the dementia wing’s common area (dining room + living room, where residents were present).
Note that we focus on the design of the applications’ interface here, and how the suggestions are made and evaluating them are out of the scope of this article. We did not intend to evaluate the performance of the application through this primary UI evaluation, as the actual evaluation of the app would need additional sets of questions that are more specific and that evaluate both performance and suggestions of the app. Rather, here we asked the basic NASA-TLX questions to understand if we missed any feedback from the co-design sessions related to the UI, which the participants might have had difficulties to convey (or might not have paid attention to).
Participants
Due to the challenges involved in recruiting multiple professional caregivers in focus groups and co-design sessions (e.g., due to their work load and variable schedule), the studies were conducted onsite at the care center, which helped with increasing the number and diversity of the participants. A total of 17 participants were recruited (all female; two in 20s, three in 30s, and nine in 40s).‡ All participants were professional staff members (i.e., professional caregivers and one nurse) at the Long-term care facility, who worked fully or partially at the dementia care wing. All participants were experienced and were not new caregivers. As suggested by the long-term care facility, each participation added $10 to $30 (depending on the level of participation) to a shared fund, and all the participants were to decide how to spend it at the end of the study. Participants were recruited either between 3p.m. and 6p.m., or after 11p.m., when the residents required less assistance from the staff. Participants were divided into groups to help with different parts of the study based on their availability.
Focus groups and co-design sessions included a total of nine sessions with 14 participants: two focus groups with a total of five participants and seven Co-design sessions with a total of 10 participants (one of the participants in the focus groups also participated in one of the co-design sessions, and another participant joined both a paper-prototyping session and a session for co-designing on the app). Eleven out of 14 participants used and tested the app for an initial evaluation and responded to the evaluation questionnaire (four from focus groups, three from paper-prototyping sessions, one who also joined a paper-prototyping and a design on the app session, and three participants who were involved in co-design on the app).
Results
Our data includes (a) responses to the questionnaires and (b) audio recordings of the entire focus groups and co-design sessions, as well as the final outcome of the paper-prototypes.
Smartphone knowledge/usage survey results
A total of nine anonymous surveys were submitted. Eight participants indicated that they use a smartphone (5 android-based and two iOS) and one did not use any cell phone.
Summary of the results for MTUAS sub-scales. Ratings for Smartphone Usage questionnaire are out of 10. Other ratings are out of 5.


Participants’ ratings of MTUAS sub-scales. 95% confidence intervals are shown. Points show the values for each rating.
As compared to a survey of 942 participants conducted in 29 , our participants had a lower rating in all criteria, indicating that their smartphone usage was lower, they had both a lower positive and negative attitude toward technology (i.e., they were more neutral), had much lower anxiety levels and technology dependence, as well as a lower preference for task-switching. These results could, to some extent, inform us about the potential users of the app and help interpret their responses better. For example, less smartphone usage can lead to a higher “effort” and “frustration” levels in the NASA-TLX questionnaire. Lower level of multi-tasking can affect judgments of “mental load” and our measured “time consumption” criteria.
Focus group results
The groups discussed a variety of different tasks that they help residents with, which was inputted as the list of tasks in the application. The activities included, but were not limited to, feeding, administering medication, toileting, stimulating people to walk or watch TV, showering, shaving, talking, etc. They also discussed the challenging situations, such as when music being played is overstimulating or residents’ behavior changes during the day (e.g., due to sundowning
§
), which suggested that the app may need to consider the time of day for generating the suggestions. Most importantly, all participants indicated that they had learned how to interact with different residents through trial and error: “Some things that work for some people do not work for other people and you just have .. a lot of error until you start to figure out what works for them. So with a new person you just pull out all your tricks” “Let’s try this, nope, maybe this one, …it’s a lot of trial and error.” ‘When ‘Resident’ came, if he tells you something and you don’t know what he is talking about then he’ll get mad, …and then you talk to his daughter, and she is like, oh, he was a ‘occupation/role’ for his whole life, so he is the boss.
Therefore, information about participants’ past roles would be very helpful for professional caregivers. For example, it was mentioned by multiple people that when a new resident comes, they will learn about their personalities from their stories and will learn how to interact with them: “like X used to say all the time I used to live in south Lorraine and she would tell you how she is Serbian” said one of the participants. Another participant added “we had the people like the boss and ‘Resident’ used to work at a restaurant. They remember that stuff forever if they have done that for a long time”
Participants also emphasized and discussed in length the importance of role-playing (i.e., playing a role as if they were someone else, e.g., a daughter) when talking with different people: “We had a lady who we called grandma but she would call us granny…I would play like the granny role and say ‘grandma, come on, I have made this for you and then she’d like trust me” “…he is the boss …so a lot of time when he starts bossing people around, ‘cause he will go up to a table and like tell people where is this? where is that? and then he gets mad because they are not responding, so I started telling him that it’s lunch time, they are on the lunch break …they are allowed to have 30 minutes by law.” “I have always explained that you walk into these doors, there are 29 residents, and I make 30 cause one is coming, and you live in 30 different realities in a matter of 24 hours, so you have to figure out which one you are in.”
When a new professional caregiver joins the center, participants mentioned that they will try to convey information about residents’ behaviors “we will just tell them” … “they are gonna try to hate you, you might want to do it like this. If that don’t work, just come and get one of us cause we’ll know” [sic], and the approaches to interact with residents “do not give an open ended yes or no questions, cause you are gonna get a no every single time.”
Further, in response to who would benefit from the app, participants believed that the app would not only benefit new professional caregivers, but can be helpful for family members or people in the community, who interact with persons with dementia: “I think that would help people in the community, because a lot of people, especially when they are new, even after they are new for a while, they don’t know how to talk to the people.” “A lot of family members. Like it’s hard for them to understand all the cognitive changes that come along with dementia” … “or just how to talk to them.” … “You can’t go up to a loved one and say hey mom, don’t you remember me?”
Overall, the discussions in the focus groups had multiple outcomes: (a) we learned about the tasks and challenges that the application should consider in generating the suggestions. For example, participants mentioned that the instructions should never be in a yes/no question form. (b) Results emphasized the importance of role-playing and adapting interactions according to previous roles of the residents, which confirmed our hypothesis. Further, all participants liked the concept of the app and thought that it would be extremely useful, especially for family caregivers and new professional caregivers.
Co-design sessions’ outcome
Next, we held a total of seven co-design sessions with 11 participants. In four of the sessions (6 participants in total), the participants provided suggestions for design through paper-prototyping. In the remaining sessions, the application—VIPCare—was implemented and the participants provided feedback and discussed changes directly on the app.
Paper-prototyping
Most participants chose to go with an iPhone template over iPad. In each session, the participants worked on the prototype from the previous session and improved it.
Participants discussed multiple aspects of the design and compared alternatives. For example, for navigation, participants discussed whether they wanted to start with a person or a task (e.g., they may want to feed all residents at the same time and start by selecting task, or they may want to help the same resident with multiple tasks). They concluded unanimously that it would be better to start with a resident and navigate to tasks: “I like it where you click on a person, so, then when you are in there, you would have all the information for that person.”
Participants also suggested that inputting reactions as feedback in the application can be feasible: “facial expressions are usually pretty big,” “it’s pretty easy, normally easy to tell, like, if they are happy or ….” This feedback would be valuable as it can help with optimizing the suggestions. Further, sundowning was suggested to be included in the app, as it can affect residents’ behaviour. Contents and details of the information were also discussed (e.g., “so when you hit medication and it comes to this screen, we need more information here…”)
After four sessions of paper-prototyping, the last group did not have much to change in or add to VIPCare’s layout and indicated that the paper-prototype was reasonably good and met their expectations.
Figure 3 shows the final paper-prototype. Participants designed three screens with information about (1) residents, (2) tasks, and (3) instructions. They also included the information necessary for residents, and the way instructions should be delivered (e.g., the amount of information to include). Final prototype on paper.
Implementation of the app based on paper-prototypes
According to the outcome of the paper-prototyping sessions, a mobile app was developed. Only the user interface and an example of scenarios and instructions were included to test the UI, as opposed to the validity of the instructions. VIPCare was developed using React Native, a JavaScript/NodeJS framework. This framework was selected for its compatibility with both iOS and Android platforms. React Native uses XML page formatting and CSS-like styling. It supports asynchronous functions, which allows communication to server without having to use events and handlers.¶ Figure 4 shows the outcome. VIPCare V1, created according to the outcome of the paper-prototyping sessions.
Co-design on the Phone app
In three iterative co-design sessions (5 participants), the participants tested VIPCare and participated in co-design sessions on the app. They discussed possible changes in the design, (e.g., added tasks; added a button to indicate that the instruction worked). Each change was applied before showing the app to the next session’s participants. In the third session, the participants believed that the app was what they would want it to be and they could not think of any further changes.
Figure 5 shows the final design of VIPCare. The application has three screens: 1. Main screen, where the caregiver can search for and select a resident. Resident’s information such as nickname or background (e.g., information about sundowning, past identities, hobbies, and favorite food) will be displayed on this page, along with the name of the resident. Caregivers can search by room numbers, names, nicknames, or easily by scrolling and looking at the pictures to find a resident. 2. Upon selecting, a resident participant will see a list of the ADLs. The activities were suggested and completed by different participants to ensure that the list is comprehensive. The users can then choose the required activity. 3. After selecting an activity, participants will receive suggestions that are tailored for each specific resident and task, according to their past identities and emotional state.** The participants chose to see both a hint (the predicted possible current identity of the resident, e.g., Bob most likely thinks he is your boss) and a way of interaction (e.g., “Be respectful and say: please eat your food”). If the suggestion works, users will return to the second screen (upon request of the participants). Otherwise, a new suggestion will be generated according to the feedback received from the resident.†† Final design for VIPCare, changed according to the outcome of the three co-design sessions. A “worked” button is added, which will direct users to the second screen when pressed. More resident reactions and another task are suggested. Search based on room was added.

VIPCare was developed to have multiple colors/themes, so participants could choose the one they prefer, to ensure that the color of the app will not bias/affect its evaluation.‡‡ Figures 4 and 5 show two examples.
Initial feedback
Summary of the results for the NASA-TLX questionnaire sub-scales, the overall score, and the additional question about participants’ perception of how time consuming using VIPCare would be. All scores were on a scale of 0–100.


Participants’ ratings of the NASA-TLX sub-scales. 95% confidence intervals are shown. Points show the values for each rating. All scores were on a scale of 0–100, with 0 reflecting no mental, physical, and temporal demand, no effort, no frustration, and a high level of performance/success. 100 shows high mental, physical, and temporal demand, high level of frustration, high effort, and no success/very low level of performance. TimeExtra shows the extra question about how time consuming the participants thought VIPCare was.
Furthermore, the additional time-related question assessed participants’ perception of how time consuming the app is. Overall, this question received very low ratings, suggesting that it was not perceived to take too much time from the professional caregivers. Also, most of the participants indicated that they preferred to use VIPCare on a mobile phone that they can carry in their pockets, as opposed to a tablet.
Discussion
In this article, we presented caregivers and staff members’ experiences and perception of challenges involved in taking care of residents with dementia, as well as their opinion about the information that can help a new professional caregiver overcome these challenges. We then presented design of VIPCare, an application that aims to assist/train new caregivers of people with dementia, especially professional staff at care-centers, to learn faster how to work with each individual resident and have fewer negative/difficult interactions.
In a care center with multiple dementia residents, it becomes challenging to successfully assist different residents as each person may expect a specific behaviour from their caregiver. In this article, we conducted focus groups and co-design sessions with professional caregivers at a care center to understand their daily challenges and to co-design the user interface of VIPCare with the professional caregivers.
A survey before the focus groups assessed smartphone usage and attitude toward technology in this specific group. The results suggested less usage and a more neutral attitude toward technology as compared to a more diverse group of people. These results were informative for interpreting the initial evaluations of the UI and also suggested that paper-prototyping may be more appropriate to start the co-design sessions with. Further, focus groups emphasized the importance of role-playing when taking care of those with dementia. Multiple situations when caregivers acted as an employee, or as a daughter to successfully assist a resident with dementia were discussed, a skill that is only gained over time and by learning to understand each resident individually through trial and error. The outcome of the focus groups emphasized the positive impact of an application that can help new professional caregivers with the training process, that is, to learn faster how to work with each individual resident and have fewer negative/difficult interactions.
This study also provides support for the utility of Affect Control Theory as a means of modeling how PWDs respond to their environment. Based on the PWDs’ sentiments about the self and others (measured as good-bad, strong-weak, and active-inactive), we can assess likely responses to kinds of interactions using ACT. Such strategy helps accommodate the perceptions of the PWDs, rather than forcing them to interact in a situation that is not aligned with their expectations. This would empower professional caregivers by showing them the ways to adjust to “multiple realities”, and by reducing trial and errors in learning how to interact with the residents. Next steps in this research will evaluate whether training people to interact on the basis of PWD sentiments reduces unproductive interactions and negative PWD emotions.
The results of an initial evaluation of the application, which was co-designed through iterative sessions, supported efficiency of VIPCare and suggested a low task load index (which needs to be tested further in the future work). Higher ratings for Effort and Frustration, as compared with the other aspects of NASA-TLX, suggested adding a hint tab/button to provide additional guidance about how to use the application.
A unique feature of this study was our use of “in vivo” data collection to gain access to respondents that otherwise would not be able to participate in co-design. The variable week-by-week and 24-7 shift scheduling of a nursing facility make laboratory research subject to low turnout. We circumvented this problem with sessions scheduled on short notice at the facility during the slowest times of the day and night shifts. This format resulted in more diversity in our respondents, with even staff with limited transportation options able to participate. Clearly, the method sacrifices some standardization and reliability compared to laboratory conditions. However, it vastly increases validity, both by ensuring accurate representation in the co-design sessions of all those who will be using the app, and by having the process occur under the same circumstances in which the app will be used. For the purposes of our project, “in vivo co-design” had clear advantages in working with a difficult to reach participant population. It also enabled us to be present at the care-center and to observe (thus better understand) daily challenges and interactions. Many similar applications could benefit from this approach in the future, as it allows the researchers to include people who may not otherwise be able to participate in co-design sessions, focus groups, etc. (e.g., caregivers and other front-line workers).
It is important to emphasize that this study focused entirely on designing and implementing the user interface, and provided real examples of scenarios and instructions that the application will provide in the future. Subsequent steps in the project (future work) will implement dynamic suggestions, which will be personalized according to each resident and will be updated according to the users’ feedback. Future work will also evaluate the effectiveness of VIPCare and the dynamic suggestions with new groups of professional caregivers who were not involved in the current study, to better understand performance of VIPCare app in action.
Limitations
Our work had limitations. First of all, we had restrictions to have groups in specific lengths (30 min) and the group sizes varied based on the availability of the staff and their work load. Also, as we wanted to specifically recruit professional caregivers of those with dementia, we had access to limited number of participants. Further, as we wanted to keep the surveys anonymous to motivate staff to participate, we do not know which responses specifically belong to participants in each part of the study. Next, despite our best effort to minimize repeated participation, we had people who attended both focus groups and paper-prototypes, and one person who was involved in both co-design sessions (paper-prototype and app-evaluations). Lastly, evaluations with a different group of professional caregivers are needed in the future work to test the suggestions and evaluate the design of the application.
Conclusion
Impact of technology on lives of people with dementia and their caregivers have been investigated by many researchers. In this article, we study professional caregivers’ needs and propose initial design of a novel application—VIPCare—that aims to train and assists new staff members at care-centers, and improves their interactions with residents with dementia. Our mixed-methods study enabled us to understand the expectations from the app, how such app is perceived, and to co-design VIPCare with the users. Outcome of the focus groups emphasized the positive effect of such application and emphasized the importance of role-playing when taking care of people with dementia. This is a main component of the application: the application will have different roles and identities of the participants and suggest clues about interaction techniques that are emotionally aligned with the person with dementia. This application can help reduce negative interactions between professional caregivers and persons with dementia, and improve relationships and quality of lives.
Footnotes
Acknowledgments
We would like to express our profound gratitude to the staff, residents, and families of our research site for their kind cooperation and generosity in allowing us to do this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by American Alzheimer’s Association (AARG-NTF-18-564 603).