
Abstract
Introduction
Some children with autism spectrum disorder (ASD) have difficulties with transitions that may lead to problem behaviours. Although the use of technologies with children with ASD is receiving increasing attention, no study has looked at their effect on transitions in activities of daily living. This study aimed to document the feasibility of (1) using two intervention technologies (NAO humanoid robot or wearable haptic device) separately to facilitate transitions in occupational therapy sessions for children with ASD and (2) the method used to document changes.
Methods
Using a single case reversal (ABA) design, two children with ASD were randomly assigned to one of the intervention technologies (humanoid robot or haptic bracelet). Each technology was used as an antecedent to stimulate the start of transitions in eight intervention sessions at a private occupational therapy clinic. Data concerning the time required for transitions, child’s behaviours during transitions at the clinic and mother’s perception of the child’s performance in transitions at home were analysed graphically.
Results
When using technology, both children’s behaviours were appropriate, quick and relatively stable. Also, both mothers reported improved perceptions of their child’s performance in transitions.
Conclusions
This exploratory study suggests no detrimental effect of using these technologies.
Introduction
The prevalence of autism spectrum disorder (ASD) has increased in recent decades. 1 According to U.S. data, the current prevalence of ASD in 8-year-old children is estimated to be one in 59. 1 ASD is characterised by impaired social interactions and communication, repetitive behaviours and limited interests. 2 Repetitive behaviours are manifested in rigid, non-functional rituals that can make transitions between activities difficult. 2 Transitions are defined as ‘moves from one activity to another’ 3 (i.e. finishing one activity and starting another). The exact reason why individuals with ASD have difficulties transitioning from one activity to another is unclear. These difficulties may be due to a greater need for predictability 4 or challenges in understanding what activity will come next. 5 For some children with ASD, their difficulties with transitions may be manifested in problem behaviours such as non-compliance, tantrums, physical and verbal aggressions, even self-mutilation. 6 Considering that transitions occur in up to 25% of preschool and elementary school children’s daily time, 7 children with ASD experiencing such difficulties may present reduced functional autonomy and develop a dependency on support from adults (teachers, therapists and parents) to remain task-oriented and adhere to transition times.8,9
One of the strategies to facilitate transitions discussed in the scientific literature is manipulating ‘antecedent events by introducing stimuli that set the occasion for performance’. 3 More specifically, strategies involving visual and auditory cues 10 are primarily used to encourage the child to start transitioning. Firstly, the use of auditory strategies, such as asking children with ASD to ring a bell at the end of their transitions, enables them to self-initiate the strategy, lessens the need for support from adults by reducing the instructions given to the children and increases appropriate behaviours. 3 In addition, children with ASD reportedly present relatively strong visual-spatial abilities that make the use of visual strategies, such as pictograms, visual schedules and timers, promising tools to facilitate transitions in this population. 11 These cues enable children to anticipate transitions by reducing the time allowed and lessening problem behaviours.10,12,13 However, children may become dependent on auditory and visual strategies, which makes removing the cues more difficult and the effects hard to generalise to other environments or other transitions in day-to-day life.10,12 For example, the two children in the case study by Dettmer and colleagues 12 wanted to continue using visual supports to facilitate transitions and had tantrums when these supports were removed. Therefore, it would be interesting to explore alternate ways to assist the transitions of children with ASD that could help to generalise what is learned to other tasks and contexts, without constantly depending on the aid used to teach the children to execute their transitions.
Use of robots with children with ASD
Considering that children with ASD show an intrinsic interest in technology,14–17 the use of humanoid robots with this population is receiving increasing attention. 18 Effects reported in the literature include reducing stress in communication interactions, 19 improving eye contact, taking turns, divided attention and imitation,14,19,20 reducing repetitive and stereotyped behaviours and improving language and joint attention. 21 Although more and more studies are targeting the use of humanoid robots with people with ASD, the meta-analysis conducted by Costescu and colleagues (2014) reveals that evidence of actual benefits remains thin (moderate effects of robot-enhanced therapy on behavioural outcomes). 18 In 2016, Begum and colleagues also reported that despite great promise, research on the use of robotics to optimise interventions with people with ASD ‘has made minimal progress’. 22 Also, recent studies looked specifically at the impact of a humanoid robot on social and communication skills,13,18–24 omitting other core difficulties faced by people with ASD, such as transitions between activities.
Use of wearables with children with ASD
Other technologies increasingly used in paediatric rehabilitation include haptic devices. 25 Haptic devices are incorporated into various consumer products available on the market. 26 For example, some common simple haptic technologies are used in pagers, cellular phones and joysticks. In most cases, they take the form of a tactile response through vibrating. 26 Few studies have documented the use of vibration with children with ASD although the sense of touch, including vibration, is 10 times more effective in social interactions in this population than verbal cues or interpersonal contact. 27 Among the few studies that have been done, vibration cues were used to improve social initiations.28,29 and optimise the attention of children with ASD to their teachers or current activities. 30
Despite the increasingly frequent use of technologies with children with ASD, no study has looked at their effect on transitions in activities of daily living (ADL). Therefore, the aims of this study were to: (1) document the feasibility of using two intervention technologies (NAO humanoid robot or wearable haptic device) separately to facilitate transitions in occupational therapy sessions for children with ASD, and (2) explore the feasibility of the method used to document potential performance changes in transitions of children with ASD.
Method
Design
This pilot study employs a single case reversal (ABA) design with two participants. In single case design, the outcome variable (here: transition time) is measured repeatedly within and across different conditions of the independent variable (here: intervention technologies) to determine whether a causal relationship exists between use of the technology and transition times. 31 More specifically, the ‘reversal’ design involves the pre-intervention situation (phase A) followed by the introduction (phase B) and withdrawal (phase A) of the intervention to compare transition times for each case. 31
Two children with ASD completed 14 personalised occupational therapy sessions over an 11-week period. The first three sessions took place before introducing the technology (phase A). Eight sessions were then completed with each participant using one of the technologies, that is, humanoid robot (phase R, for robot) or haptic bracelet (phase B, for bracelet). Three final sessions were held after withdrawing the technology (phase A).
Participants
To participate in the study, the children had to (1) have been diagnosed with ASD, (2) be between 4 and 7 years of age, (3) speak French and (4) have difficulty in transitions as reported by their parents.
The two participants were recruited using a purposive non-probability sampling method. The child psychiatry clinic at the Centre hospitalier universitaire de Sherbrooke (CHUS), where the diagnosis of ASD had been made, sent letters to families who had a child who met the eligibility criteria to inform them of the study. Parents interested in participating were invited to contact the research team for more information. Free and informed consent was obtained at a meeting with the research team. The research protocol was approved by the ethics committee for health research with humans at the CHUS Research Centre.
Anthony (fictitious name)
Five-year-old Anthony lives with his parents and two-and-a-half-year-old sister, who does not have any known developmental difficulty. His mother has a professional diploma while his father, who had language delays and memory problems, finished grade 9. According to Anthony’s developmental history, he began speaking late. The first suspicions of ASD began before age one since Anthony did not respond to his own name. He started daycare when he was about 2 years old. The diagnosis was made at age five by a child psychiatrist, backed by an interdisciplinary team and standardised tools (ADOS). At recruitment, the mother reported significant difficulty in Anthony’s ADL transitions at home (overall performance of 15% on a visual analogue scale [VAS]). During the occupational therapy sessions, Anthony’s goals were to develop the ability to dribble a ball and to work on fastening his clothes (buttons, zippers, laces).
Sophie (fictitious name)
Four-year-old Sophie is non-verbal. She lives with her single mother, sisters aged 12 and 13 and brothers aged 4 and 10. Her younger brother is known to have ASD and attention deficit hyperactivity disorder (ADHD), and her older brother also has ADHD. Her mother completed grade 9 and is a full-time mother. Sophie’s psychomotor skills developed late (crawled at 12 months and walked at 18 months), and she was still not toilet-trained at the time of the study. The first suspicions of ASD began at the age of 18 months since Sophie did not talk and spent her time swinging. The diagnosis was made by a child psychiatrist at age 3½ when she started at a family daycare. At recruitment, the mother reported moderate difficulty in Sophie’s ADL transitions at home (overall performance of 37% on a VAS). During the occupational therapy sessions, Sophie’s goals were to develop the ability to use a pencil and to become more autonomous in getting dressed.
Apparatus
Sequence of activities and scripts used to announce transitions.

aCommon activities considered for analysis.
The wearable haptic device was a bracelet worn on the forearm just above the wrist that emitted vibration cues. It consists of a Pico VibeTM (307–100) vibration motor from Precision Microdrives calibrated to generate a displacement of about 15 dB − defined as the comfort zone 32 − within the range 150–250 Hz. The wearable haptic device was calibrated on the child at a preliminary meeting in the clinic to determine the operating mode to use with the child. In the calibration session, three different safe frequencies (minimum, median and maximum allowed by the vibrating device) were tested on Sophie with three trials for each frequency. Each trial included the three frequencies, which were presented in a different order from one trial to the next. Since Sophie is not verbal, the research team targeted the mode in which, in addition to tolerating the bracelet, Sophie showed verbally or non-verbally that she liked (such as by smiling) the vibration cues from the bracelet at the minimum frequency. During the trials at median and maximum intensity, Sophie’s face became serious and she tried to pull the bracelet off her forearm. During the intervention phase, the haptic bracelet was activated before the therapist gave the child the verbal instruction. Once again, another adult seated in the opposite corner of the room used computer software to activate the vibration when the child was supposed to listen to the next instruction from the occupational therapist to start transitioning to the next activity. The occupational therapist’s instructions were the same as NAO’s prerecorded scripts (see Table 1).
Procedures
The participants were randomly assigned to one of the intervention technologies, that is, humanoid robot or haptic bracelet. Each technology was used in eight intervention sessions at a private occupational therapy clinic. For this study, the therapy sessions were free for the participating families. They lasted no more than 1 hour each and were all structured the same way, with six activities in the following order: (1) undressing (remove winter clothes), (2) therapeutic activities related to the specific objectives for each child, (3) hand hygiene, (4) snack, (5) other therapeutic activities and (6) dressing. Since the children had different therapeutic goals, the therapeutic activities were different for each child and also changed over time in order to remain motivating and a ‘just right challenge’ for the child. Examples of therapeutic activities included playing ball games, playing with playdough, tying shoes, tying buttons, drawing, dressing up, etc.
Each intervention technology was used as an antecedent to stimulate the start of the transition. Three variables were collected: time taken to transition, child’s behaviours during transitions and performance in transitions at home. Two of the variables (time taken and child’s behaviours) were measured in each of the 14 intervention sessions in the clinical setting while data for the third variable (performance in transitions at home) were collected from the parents only in the first and last sessions.
The 14 occupational therapy intervention sessions for each child were videotaped. The videotapes of the 28 sessions were viewed by the research team to extract the data after the fact. Of the six activities that structured the intervention sessions, four were used throughout the therapy to evaluate the children’s performance in transitions. Since the therapeutic activities varied for the same child during the follow-up period and also differed from the other child’s in order to meet their personalised intervention objectives, these activities were not studied. However, they were relevant in giving meaning to the children’s presence in therapy, and also a benefit of participating in the study. Thus, the four activities studied were: (1) undressing, (2) hand hygiene, (3) snack and (4) dressing.
To facilitate the data analysis and ensure standardisation across the sessions, the research team wrote the script that the occupational therapist or NAO used to announce each transition. The different transition times were then defined based on the standard script used in all the intervention sessions.
Transition times in the clinic
Following Sainato et al.’s definition of transition as a change ‘from one activity to another’, 3 the research team subdivided the transitions into two main periods, namely initiation (T1: time between when the therapist gives the instruction and travel is initiated) and time travelling to the next activity (T2: time between when travel is initiated and the end of the child’s travel). For this study, the transitions to each of the four activities studied were divided into two periods, resulting in a total of eight transition periods analysed for each intervention session. Transition times were analysed using visual analysis and improvement rate difference. The visual analysis highlighted clinical change (and not statistical change) based on changes in variability, slope, level and trend between adjacent phases.33,34 More specifically, according to Jacobson et al., a clinically significant change is defined as follows: ‘the client moves from the dysfunctional to the functional range during the course of therapy on whatever variable is being used to measure the clinical problem’. 35 Also, improvement rate differences (IRD) were calculated for each of the eight transition periods for both children. IRD is defined as the difference between the improvement rate in the treatment phase (percentage of data points that exceeds all data points in the treatment phase) and the improvement rate in the baseline phase (percentage of data points tied with or exceeding any data point in the treatment phase). 36 Two average IRDs were also computed for each participant, indicating the average level of improvement for T1 (initiation time) and T2 (travel time) separately for each child.
Behaviours of the children in transitions in the clinic
Using a behavioural grid with three components (participation, avoidance and refusal), the participants’ behaviours were scored for the four activities in each time period (T1 and T2). Scores were assigned as follows: (1) ‘participation’ when the child adopted a positive attitude (i.e. no ‘avoidance’ or ‘refusal’ behaviours), executed the task immediately after the instruction, started the new activity or needed only one reminder; (2) ‘avoidance’ when the child exhibited at least one of the following behaviours: needed more time, needed more than one reminder, negotiated verbally, switched back and forth between the new and the previous activity, grumbled, talked excessively between the transition or detoured before going to the new activity; and (3) refusal’ when the child had one or more of the following behaviours: negative verbalisations (‘I don’t want to’, ‘No’, etc.), aggressive behaviours (e.g. throwing things, hitting, spitting, biting or scratching someone), self-mutilation behaviours (e.g. hitting or biting themselves), tantrums (e.g. crying, yelling), engaging in a ritual, continuing the initial activity, moving to a different activity or running away. The behaviours associated with the transitions were analysed descriptively using the behavioural grid. Frequencies and percentages were calculated for each transition separately for the three pre-intervention sessions, eight intervention sessions and three follow-up sessions (post-intervention).
Performance in transitions at home
In the first and last occupational therapy sessions, the mothers’ perceptions of their child’s general performance currently in transitions at home were recorded on a VAS. The VAS has been described as a useful tool to measure a variety of subjective phenomena. 37 Although the VAS had not been validated or used previously to evaluate mothers’ perceptions of their child’s performance in transitions at home, the VAS has been used a few times to rate the perceptions of mothers with children with ASD, including concerning their sleep problems or behaviour problems.38,39 As recommended in the literature, 37 the VAS used was a 100-mm horizontal line with a right angle stop at each end; the left end was labelled ‘No participation in transitions’ and the right ‘Full participation in transitions’. The VAS was scored by measuring the distance in millimetres from the left end, giving a score out of 100 mm. The VAS results were then analysed descriptively by comparing the pre-intervention score with the post-intervention score for each child.
Results
Feasibility of using intervention technologies
Anthony and the humanoid robot
Anthony was randomly assigned to using the humanoid robot to facilitate transitions during the intervention sessions. Anthony and his mother came as scheduled to a private occupational therapy clinic for 14 intervention sessions over an 11-week period, including eight sessions with the humanoid robot.
Transition times in the clinic
Overall, transition times (T1 and T2) for the four activities were quick. For the initiation time (T1), even before introducing the humanoid robot, Anthony had quick stable times between 0 and 4 s from the outset. Hence, when the humanoid robot was introduced, no improvement was noted. On the contrary, IRDs showed a negative effect of NAO on initiation time (average IRD = −81%). When analysing the graph in Figure 1, variability is observed in the data collected between sessions 4 and 11. Anthony might take over 40 s to start the travel after hearing the instruction from NAO five times (15%) out of 32 observations (8 sessions × four transitions = 32 travel times during phase R). The post-intervention results are once again very quick and stable, which are comparable to the observations before the intervention. Initiation time (T1 Anthony).
Concerning the travel time (T2) illustrated in Figure 2, the introduction of the humanoid robot did not have a significant impact on the speed of Anthony’s travel to his hand hygiene and snack tasks; times during phase R (intervention with the robot) are similar to the pre-intervention and post-intervention times (IRDs between −30% and −38%). However, two changes were observed in Anthony’s travel time when introducing NAO. First, his travel time toward undressing was much longer the first time he saw the robot (session 4), but went back to normal in the following sessions. This was because the robot walks slowly and Anthony was waiting for him during transitions. Also, a trend towards extending the travel time was noted before the dressing task from session 4 onward (IRD = −100%). This slowdown in executing the travel was also maintained during the post-intervention phase. When comparing the two A phases (pre-intervention and post-intervention) when no intervention technology was used, the travel times before dressing in the post-intervention sessions were greater than all the times in the first three sessions before the humanoid robot was introduced. Travel time (T2 Anthony).
Behaviours in transitions in the clinic
Frequencies of Anthony’s behaviours during transition times T1 and T2.

Performance in transitions at home
In the first intervention session, Anthony’s mother reported an overall performance of 15/100 in ADL transitions at home. At the end of follow-up, she reported an overall performance of 67/100 in Anthony’s transitions at home. Thus an improvement of 52 points (on a scale of 0–100) was observed between the first and 14th occupational therapy session.
Sophie and the haptic wearable device
Sophie was randomly assigned to using the haptic wearable device to facilitate transitions during the intervention sessions. Since she is non-verbal, the operating mode chosen for the interventions, after the haptic device was calibrated, was when Sophie smiled and kept the bracelet, which corresponded to the minimum vibration frequency of the device.
Sophie and her mother came as scheduled to a private occupational therapy clinic for 14 intervention sessions over an 11-week period, including eight sessions with the haptic bracelet on her forearm just above her wrist.
Transition times in the clinic
In general, Sophie’s transition times (T1 and T2) were quite quick for all four activities. More specifically, initiation times (T1) were quick (<15 s) and stable for three of the four activities before the haptic device was introduced (phase A), namely undressing, snack and dressing (see Figure 3). Only the initiation time toward hand hygiene was more variable and tended to increase during the first three occupational therapy intervention sessions, but not in phase B. During phase B (intervention with the haptic bracelet), quick and relatively stable times were observed for the eight sessions and all four activities. Nevertheless, the average IRD (−49%) revealed no significant improvement in phase B. Finally, these quick times were maintained after withdrawal of the haptic device, except that it took Sophie more time to initiate travel to hand hygiene in the first post-intervention session (session 12). This did not persist in the last two sessions. Initiation time (T1 Sophie).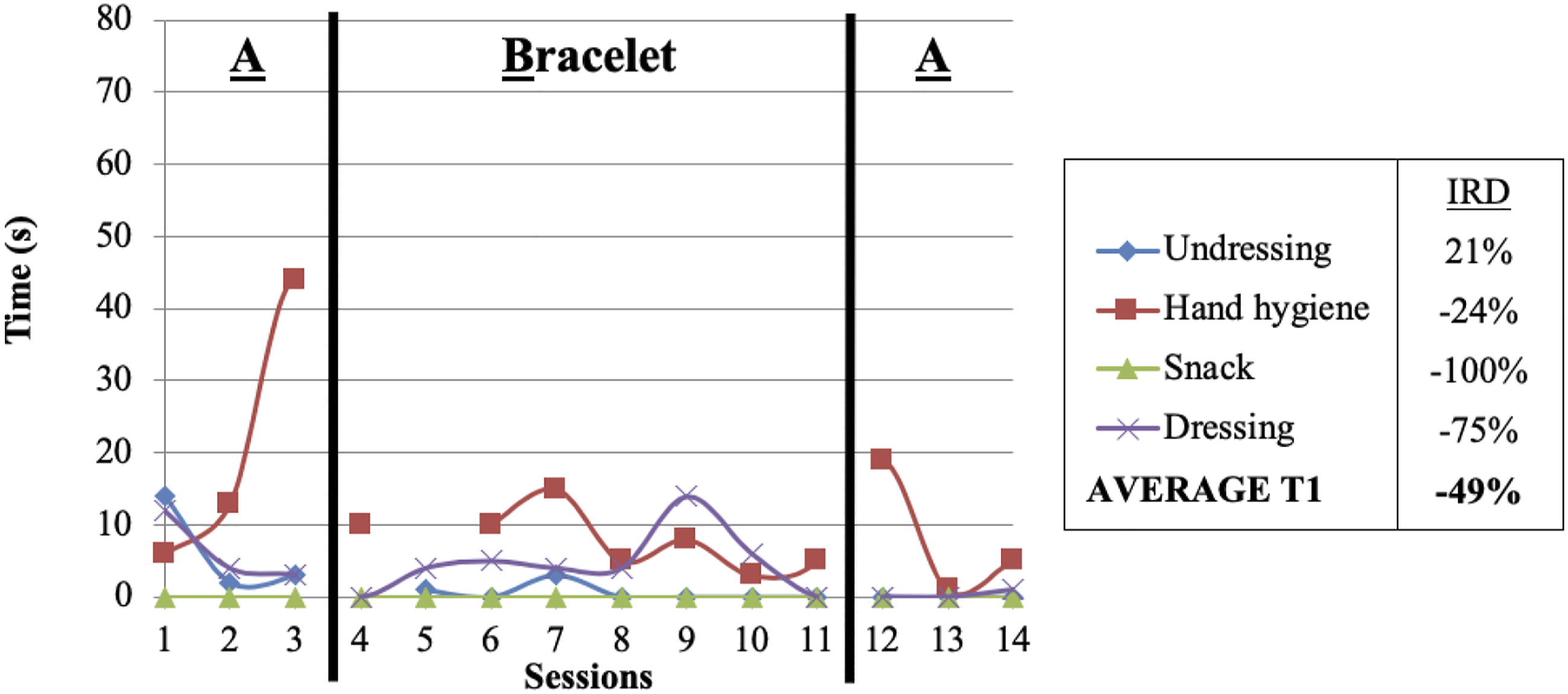
For travel time (T2), substantial variability was noted right from phase A in Sophie’s travel time to all activities: undressing (range: 23–30 s), hand hygiene (range: 24–79 s), snack (range: 19–33 s) and dressing (range: 28–60 s) (see Figure 4). Also, in phase A, three of her four activities showed a natural tendency to decrease travel time (undressing, hand hygiene and snack). For these three activities, Sophie’s tendency to accelerate travel times was maintained when the device was introduced in phase B (undressing IRD = 100%; hand hygiene IRD = 21%; snack IRD = 8%) and withdrawn at the end of the intervention (phase A). For travel time to dressing, this continued to vary greatly in phase B (IRD = −67%), making it impossible to identify a trend. In each session, Sophie seemed preoccupied during this transition and checked that her mother was following her, which potentially increased the time needed to complete the transition. Despite that, travel times to dressing increased slightly when the haptic bracelet was withdrawn (phase A). Travel time (T2 Sophie).
Behaviours in transitions in the clinic
Frequencies of Sophie’s behaviours during transition times T1 and T2.

Performance in transitions at home
According to Sophie’s mother’s VAS, Sophie’s overall performance in transitions at home increased by 26.5 points, from 37/100 in session 1 to 63.5/100 in session 14.
Results
Feasibility of the method used to document changes
Transition times in the clinic
Transition times were calculated after the fact using software to view the videotapes and add markers at key points in the transition. Since a prerecorded script was used for NAO or the occupational therapist to announce the transitions, the start of the transitions was easy for the research team to identify. Three markers were used for each activity: (1) end of the verbal instructions given by NAO or the therapist, (2) initiation of travel by the child, and (3) end of the child’s travel. Thus the time between markers 1 and 2 was the initiation time (T1) while the time between markers 2 and 3 was the travel time (T2). In short, the definition of transition times, the videotapes, the viewing software for affixing markers and the protocol used for the interventions made it possible to quantify the performance in transitions through accurate transition times that were reproducible from one session to the next.
Behaviours in transitions in the clinic
The grid for documenting the children’s behaviours in transitions in the clinic was used to describe the children’s performance. As reported in Anthony’s results, this qualitative aspect can help to understand unusual transition times.
In addition, documenting the children’s behaviours indicated the acceptability of the two intervention technologies. The analysis of the data on the children’s behaviours showed that the haptic device was particularly well accepted by Sophie, who displayed fewer avoidance and refusal behaviours with the device than before the bracelet was introduced.
Performance in transitions at home
A VAS was used at the beginning and end of the intervention to document changes in the mothers’ perceptions of their child’s performance in transitions at home. This scale collected subjective quantitative data from the mothers to assess if what the children had learned was generalised to their real life. Generalisation to real-life settings is unquestionably an important element to explore in more detail in similar studies.
Discussion
The results of this study show that it is feasible for occupational therapists to use a haptic device or humanoid robot with children with ASD to stimulate skills other than social and communication. In fact, when using technology to facilitate transitions between activities, both children’s behaviours were appropriate, quick and stable.
Contrary to what was initially reported by the mothers (documented on the initial VAS), the children had little difficulty in transitions right from the first intervention sessions (phase A without technology). Quick transition times in phase A also explain the negative IRDs reported in this study. In fact, it was difficult, if not impossible, for Sophie and Anthony to improve their transition times because of their speed at baseline. Nevertheless, the participants maintained their quick initiation times (T1), except for Anthony when travelling to the dressing task, where the time increased during the sessions with the humanoid robot and decreased after it was withdrawn. This was because Anthony continued his previous activity, even after being instructed to go and get dressed. The times required for travel (T2) varied from one session to the next with the humanoid robot, especially since Anthony repeated NAO’s instructions and was distracted by NAO’s movements. As for Sophie, she maintained or decreased travel times (T2) when using the haptic device, except for travel to the dressing activity. The times for that activity continued to vary from one session to the next since she often waited for her mother to follow her, although this did not seem to be related to the presence of the haptic device. It is possible that the presence of the humanoid robot was so attractive that it was distracting, and much more so than the haptic device; this would limit the ability to produce the expected changes in speed when travelling between two activities in the humanoid robot’s presence. 20 In contrast, even though touch perception may be different in children with ASD, using adapted tactile or haptic technologies, such as the haptic bracelet, may be helpful for people with ASD. 40
Although no previous study looked at using a humanoid robot or haptic device to improve transitions in children with ASD, the present study showed promising results. In fact, trends from this study suggest that the vibration cues (haptic device) or a strategy using simplified visual and auditory cues (humanoid robot) could be used as a communication method to facilitate transitions in children with ASD. In addition, this exploratory study showed no detrimental effect of using these technologies. Despite encouraging results for both technologies, the haptic bracelet was less distracting for Sophie than the robot was for Anthony. More research is needed to investigate potential benefits of using a haptic device or humanoid robot to facilitate transitions in children with ASD. To test this hypothesis, future studies should have a larger sample, longer follow-up and fewer distractions during the intervention sessions.
This study has some significant limitations. Firstly, the VAS data collection method presents several potential biases. For example, the pre- and post-intervention measures were recorded on the same sheet. Thus, in the post-intervention evaluation, the mothers could see the rating they had chosen in the first evaluation. Considering a social desirability bias and knowing that the mothers wanted to see improvements in their child’s transitions, it is likely that they scored their final perception higher and overestimated the actual improvement they observed. In addition, it is not possible with the VAS to characterise the changes perceived by parents. Hence the generalisation of potential gains made in the clinic should be explored in greater depth using, for example, interviews with parents, a tool that captures parents’ perceptions of performance in greater detail (such as the Canadian Occupational Performance Measure), 41 or videotapes of transitions at home.
Also, the children’s initial level of difficulty with transitions may have been overestimated by their mothers. Despite the effort to recruit children with difficulties during transitions, both participants performed relatively well during the pre-intervention phase (phase A) (i.e. appropriate behaviours and relatively quick transition times). Given their good performance during the pre-intervention phase, the two participants may not have been representative of children who could benefit the most from this type of intervention, which limits the likelihood of observing a clinical improvement in transitioning from one activity to another. Knowing that a predictable and structured environment reduces problem behaviours,42,43 the appropriate behaviours initially obtained in the transitions may also be because the therapy was delivered in a structured context with few environmental distractions, which could have had an impact on the quality of the transitions.
Finally, since this is a case study, the results cannot be generalised to other children with ASD; hence the need for other studies looking at the same topic with a greater number of participants. Also, it would be interesting to try these two intervention technologies in the child’s real life, such as at home, where there are environmental distractions. In addition, considering that transition is defined as a change ‘from one activity to another’, 3 it would be a good idea to consider both the activity that must end as well as the activity about to begin to determine if the child’s difficulty occurs when an activity ends or a new one begins. For example, a measure of the time it takes for a child to stop the current activity could be added to future research protocols.
Conclusion
The aim of this study was to explore intervention technologies that had never been used before to improve the transitions of children with ASD. Despite its limitations, this study determined that an NAO humanoid robot and a haptic bracelet could be used as communication methods to facilitate transitions in ADL in this population without any detrimental effects. In the presence of one or other of these intervention technologies, the children in this study generally maintained a quick transition time or improved their time slightly. However, the haptic device seemed less of a distraction than the humanoid robot, particularly when travelling, where some avoidance behaviours were associated with the robot’s presence. Furthermore, both mothers reported improved perceptions of their child’s performance in transitions, confirming the potential of these intervention technologies to facilitate transitions in real life situations. Future studies should be conducted in children’s own living environment and with more participants. It would also be interesting to include a more in-depth evaluation with parents to better document changes in the real world.
Footnotes
Acknowledgements
We wish to thank Marc-Antoine Pelletier, MSc, Eng, electrical engineering student Alex Salvail, and multimedia technician Jérémie Lamoureux Bélair, all of whom collaborated in developing and programming the haptic device. We also thank Timothy D. Gifford of MOVIA Robotics for his assistance with operating and programming the NAO humanoid robot.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.