
Abstract
Aim
Intense training of arm movements using robotic devices can help reduce impairments in stroke. Recent evidence indicates that independent training of individual joints of the arm with robots can be as effective as coordinated multi-joint arm training. This makes a case for designing and developing robots made for training individual joints, which can be simpler and more compact than the ones for coordinate multi-joint arm training. The design of such a robot is the aim of the work presented in this paper.
Methods
An end-effector robot kinematic design was developed and the optimal robot link lengths were estimated using an optimization procedure. A simple algorithm for automatically detecting human limb parameters is proposed and its performance was evaluated through a simulation study.
Results
A six-degrees-of-freedom end-effector robot with three actuated degrees-of-freedom and three non-actuated self-aligning degrees-of-freedom for safe assisted training of the individual joints (shoulder or elbow) of the human arm was conceived. The proposed robot has relaxed constraints on the relative positioning of the human limb with respect to the robot. The optimized link lengths chosen for the robot allow it to cover about 80% of the human limb’s workspace, and possess good overall manipulability. The simple estimation procedure was demonstrated to estimate human limb parameters with low bias and variance.
Discussion
The proposed robot with three actuated and three non-actuated degrees-of-freedom has a compact structure suitable for both the left and right arms without any change to its structure. The proposed automatic estimation procedure allows the robot to safely apply forces and impose movements to the human limb, without the need for any manual measurements. Such compact robots have the highest potential for clinical translation
Introduction
Robot-assisted rehabilitation of arm function, in chronic stroke patients, has been found to be as effective as intensity matched conventional therapy for reducing impairments.1–3 However, the growing demand for rehabilitation services cannot be met through one-on-one therapist-administered intense training protocols. Technological tools that improve access, and efficiently deliver such services are vital for establishing sustainable service and care pathways. Robots are one such technology that can physically interact with participants to allow graded intense training of various sensorimotor functions. However, the infiltration of robots into routine clinical practice has been poor. This is primarily due to their high cost-to-benefit ratio, limited features, and bulky nature, especially in the case of arm robots. There is a need for fresh approaches to designing arm rehabilitation robots that can address some of their current shortcomings to improve their potential for commercial translation and eventual clinical acceptance. This work presents a different approach toward robot-assisted arm rehabilitation focusing on individual joint training, unlike most existing arm robots that are designed for coordinated multi-joint arm training.
There is some evidence in the current literature supporting the hypothesis that individual joint training is not inferior to coordinated multi-joint training. A study by Milot et al. used the BONES robot to administer multi-joint and single-joint training in moderately impaired chronic stroke participants, and found that both groups showed improvements in both motor function and impairments. 4 Interestingly, they did not find the multi-joint training to be superior to the single-joint training approach. Although only a pilot study with 20 participants, this finding is also supported by other evidence in the literature. Schaefer et al. found that training on a single activity of daily living (ADL) generalized to untrained tasks in chronic stroke participants. 5 The study by Fluet et al. investigating robot-assisted upper limb (UL) training showed that training the arm and hand together as a functional unit was no different from training the arm and hand separately. 6 A study on healthy individuals by Klein et al. found that individual training of parts of a complex movement resulted in slightly better learning and retention. 7 These results support the idea of developing a simple, compact, and cost-effective robot for training individual joints, rather than developing one for coordinated multi-joint arm movements. This is the primary objective of the current work, which focuses on the development of a robot for assisted training of two degrees-of-freedom (dof) of the shoulder or elbow joint.
Although exoskeleton robots are well suited for supporting and assisting individual joint movements,8–13 the strict constraints of alignment of joint axes between the robot and the human can complicate their design and use. On the other hand, end-effector robots have structures that are independent of that of the human limb.14–17 They have significantly fewer constraints on the location and the orientation of the human joint with respect to the robot, thus making it much easier to interface a human limb with the robot. Given these advantages, we chose to implement an end-effector based approach for the proposed robot for training individual joints.
Conventional end-effector robots for arm rehabilitation are attached to the human limb at the hand, where they apply interaction forces to impose arm movements. Such an approach cannot be used to impose movements at an individual joint of the arm as this human-robot closed kinematic chainI is under-constrained. An end-effector robot for training a specific joint will need to be directly attached to the human limb segments that is anatomically connected to the joint of interest (e.g., upper-arm for the shoulder, and forearm for the elbow). In order to ensure that the robot imposes precise and safe movements and forces/torques to the human limb, it is essential for the robot to be aware of the details of the human limb’s kinematic chain and its parameters. Current end-effector robots do not take into consideration the details of the human limb’s kinematic chain.
To this end, we present a 6-dof end-effector robot AREBO (
Design of AREBO’s kinematics chain
The objective was to develop a compact, portable robot for training movements of individual joints of the human arm (shoulder and elbow), which can be used for both the left and right arms without requiring any change to the robot’s structure. Furthermore, we also wanted to avoid the need for precise positioning and orientation of the patient with respect to the robot, which can be difficult and time consuming with severely affected patients. These design requirements can be fulfilled by an end-effector type robot, the type chosen for designing AREBO.
Consider the human limb with a joint (e.g., shoulder joint) located at the origin of a reference frame

where,

Depiction of a human-robot closed-loop kinematic chain where the movements of the human limb are to be assisted by the robot.
To simplify the process of connecting the robot to a human limb, the robot must not strictly constrain the location and orientation of the human limb with respect to the robot, i.e., no strict constraints on
Human limb’s kinematic chain
We assume the human shoulder joint at

Details of the human limb’s kinematic chain. The human limb considered in this work is a two or three dof chain with the structure shown in the figure. The third dof is optional.
The Denavit-Hartenberg (DH) parameters for the human limb are shown in Figure 2. The position and orientation of

where,
AREBO’S kinematic chain
We are only interested in assisting the shoulder flexion/extension and shoulder abduction/adduction movements of the shoulder joint with the robot in the current application. This movement assistance can be accomplished by applying forces orthogonal to It must The robot needs precise The robot must
An appropriately designed 6-dof robot can achieve any arbitrary position and orientation within its workspace. To apply a force in any arbitrary direction at the robot’s endpoint in 3 D space, we need at least three actuated dof for the robot. The remaining three dof can be unactuated, allowing them to self-align to any arbitrary orientation of the human limb


Details of the proposed robot’s kinematic chain. The robot has 6 dof arranged in the particular manner shown in the figure. This allows the robot to achieve a range of positions and orientations within its reachable workspace. The first three dof (shown in dark gray) are actuated, while the rest three dof (shown in light gray) are passive self-aligning joints.
Human-robot closed kinematic chain
A closed-loop kinematic chain is formed when AREBO is connected to the human limb, such that the frames

We assume that the orientation of

The first three joints of the robot shown in a darker color in Figure 4 are the actuated joints, while the rest three (shown in a lighter shade) are unactuated. These sections are shown separately in Figure 4 to demonstrate the different roles of the two sections. The actuated section is responsible for applying appropriate forces on the human limb, while the unactuated section helps in self-aligning the robot’s endpoint
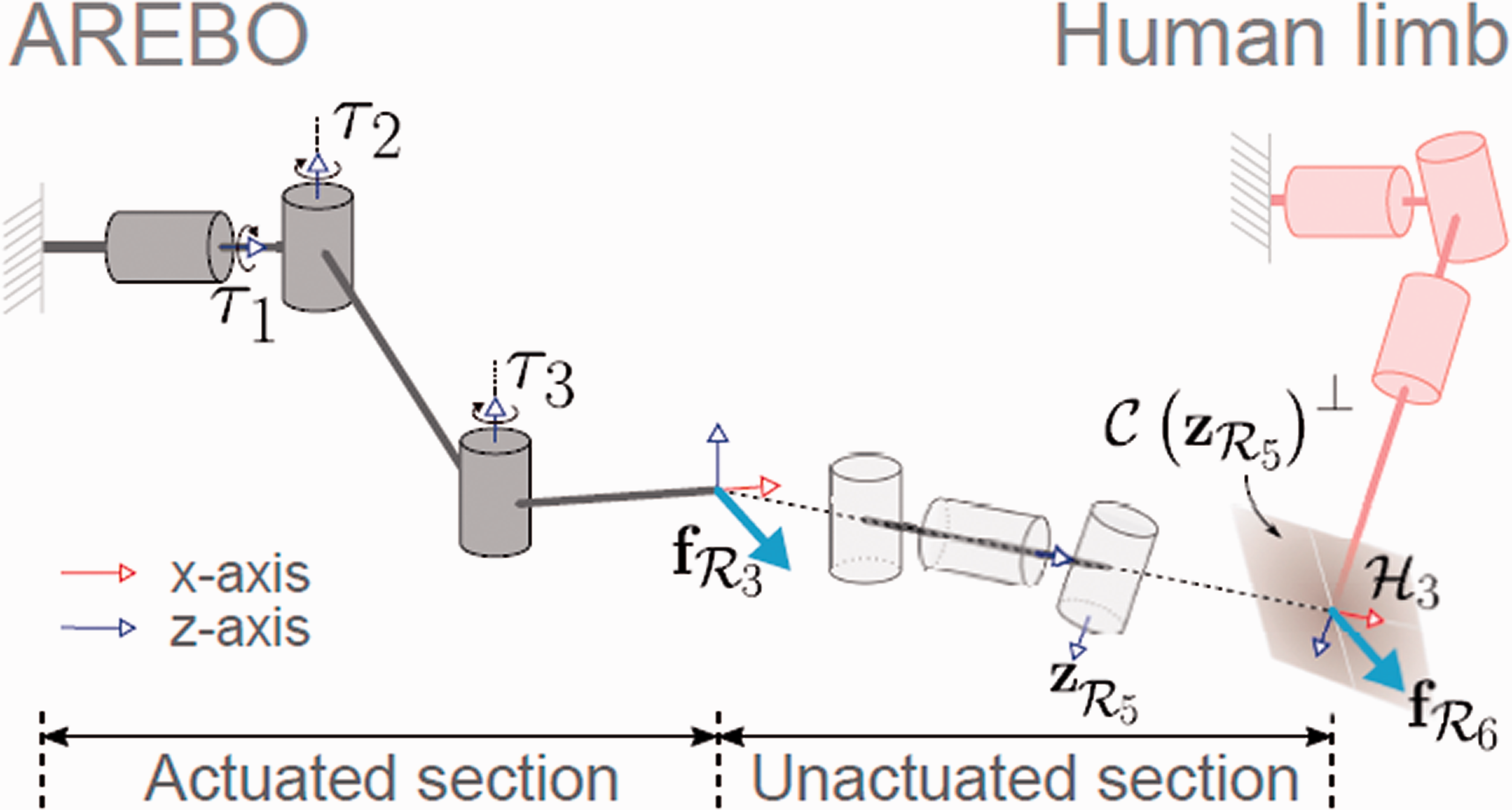
Detailed depiction of the human-robot closed kinematic chain, along with the interaction force applied by the robot on the human limb. The endpoint force
When the robot and the human limb are connected

where,


Except for the cases where
Identification of human limb parameters
In the human-robot closed kinematic chain, the planning and control of the human limb’s movements require information about the location of Can a given desired human limb configuration For any reachable human limb configuration
Assuming that we know
Given that AREBO allows some freedom for the user to sit with respect to the robot (Figure 7) and can accommodate upper-limbs of different sizes, the values of


We have assumed earlier that

The unknowns in the above equation are
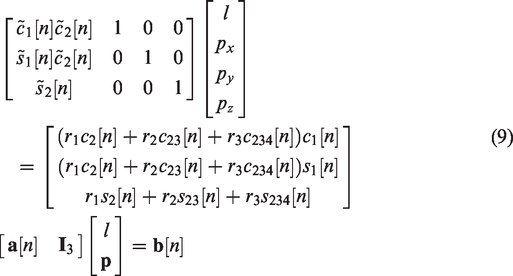
Combining the equations for all n,
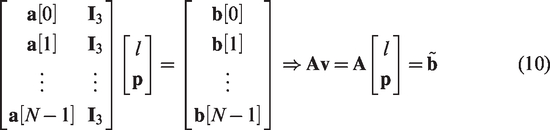
If

Methods
In this section, we describe the optimization of the robot link length parameters and the simulation analysis of the algorithm for estimating human limb parameters.
The first step in the physical realization of AREBO is the choice of its link lengths r1, r2, and r3. These link lengths will determine the robot’s workspace and its overall manipulability. The individual endpoint workspaces of the robot

When the endpoints of the human limb and robot are attached together, i.e.,
We wish to allow a range of possible values for the parameters l and Maximize Wa (or Maximize the ability of the robot to apply forces orthogonal to the human limb.
These two objectives can be combined into a single objective function






Optimization of robot link lengths
The optimization of the robot link lengths was carried out numerically through a brute force search over a set of parameters values for
Set of parameter values for the robot and the human limb used for the robot link length optimization program. There are a total of 484 robot parameter sets

Choose values for the robot link lengths:
Choose values for the human limb length and location:
Compute the set of all possible joint configurations for the human limb
Compute the workspace
If all possible human limb parameters have been searched, then go to Step 6, else go to Step 2.
Compute the two objective functions
If all possible robot parameters have been searched, then go to Step 8, else go to Step 1.
Find the optimal robot link parameters as the value of the 
We assumed
Simulation analysis of human limb parameter estimation
The algorithm for estimating the human limb parameters described in ‘Identification of human limb parameters’ section was evaluated using simulated movement data. Twenty different random parameter sets were generated from uniform distributions for px, py, pz, and l of the human limb.

The human and robot joint angle data from the simulated calibration procedures were used to estimate the human limb parameters; 50 different estimates for the 20 different sets of human parameters were estimated. The performance of the estimation algorithm was evaluated by computing the distribution of estimation errors for the four parameters.
The code used for robot link length optimization and the analysis of the limb parameter estimation are available for download; refer to online Appendix B for details.
Results
In this section, we present the results from the robot link length optimization and the simulation analysis of the human limb parameter identification algorithm.
Optimization of robot link lengths
The results from the robot link length optimization procedure are shown in Figure 5 in the form of heatmaps as a function of two robot link parameters; the first two rows correspond to the individual objective functions

Heatmaps depicting the values of the objective functions O1, O2 and O as a function of the different robot link lengths. These plots show that workspace O1 and force ratio O2 are conflicting objectives, and the resulting overall objective that weighs both O1 and O2 equally is shown in the bottom row.

The values of normalized workspace O1 and force ratio O2 for the optimal robot link lengths, for the different possible parameters for the human limb (from Table 1).

CAD models of a realization of AREBO and the depiction of its use for assisting the different movements of individual joints. (a) When connected to the upper-arm, the robot can assist shoulder flexion/extension and shoulder abduction/adduction by applying forces orthogonal to the upper-arm. (b) When it is connected to the forearm, SIER and EFE can be assisted by applying forces orthogonal to the forearm. It should be noted that this approach for assisting SIER is safer and more comfortable than by providing tangential forces on the upper-arm. 18 The two CAD models in (a) and (b) demonstrate the relative freedom a participant has in sitting with respect to the robot.
Identification of human limb parameters
The results from the analysis of the human limb parameter identification procedure are shown in Figure 8. The true value of the parameters is 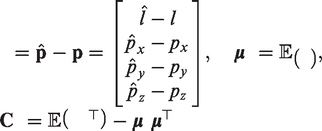

Errors in human limb parameter estimates for two different measurement noise
Figure 8 shows histograms of the estimation error in the different parameter estimates for two different noise levels in the joint angle measurements. As expected, lower measurement noise results in estimates with smaller bias and variance. The sample mean and covariance of estimation errors are shown below the plots in Figure 8 for both noise variances. The limb length has the largest absolute bias and variance among the four parameters, and also appears to be underestimated for both levels of measurement noise. The parameter pz has the lowest absolute bias and variance, which also appears to be underestimated. The other two parameters px and py have intermediate bias and variances, and these are overestimated. pz is least correlated to the other parameters. The other three parameters appear to be slightly correlated.
Discussion
The paper presented the kinematic design of a 6-dof robot – AREBO – capable of assisting movements of individual human joints. The proposed design can assist up to two dof of a human joint while ensuring the safe application of assistive forces on the human limb. The optimization of the robot’s link lengths, maximizing an objective function consisting of the human limb’s workspace and the robot’s ability to apply forces in safe directions, was presented. The paper also presented a simple algorithm for continuously estimating the kinematic parameters of the human limb using the joint angles of the robot and the human limb.
Based on the existing evidence and further assuming that robot-assisted therapy is as effective as dose-matched conventional therapy, the ultimate goal of rehabilitation robots is to deliver substantial doses of intense therapy at a small cost to the healthcare system. Realizing this goal requires compact, cost-effective devices that can be easily deployed even in space-constrained healthcare settings and patients’ homes while offering superior benefit-to-cost ratio to the user. AREBO presents a minimalistic solution for an arm robot by using three actuated and three passive dof, while offering several useful features that boost its potential for clinical adoption. AREBO has a very compact and portable structure making it suitable for small clinics and even patients’ homes. The reduced number of actuators also makes the overall bill of materials low compared to that of a fully actuated robot. Many recent work targeting robotic mechanisms for the shoulder joint have relied on clever design with active control to ensure suitable alignment to the shoulder joint axes.12,13,19,20 From the perspective of assisting just two dof of the human limb, AREBO’s self-aligning passive joints remove the need for active alignment, thus simplifying the control of the human-robot interaction. The end-effector design of the robot’s structure allows it to be used for both the left and right arms without any change in its structure. Without such a feature, a clinic would require dedicated devices for the left and right arms, which is an undesirable solution. The robot can be used for training one or two dof at either the shoulder or the elbow, as shown in Figure 7. Shoulder flexion/extension and shoulder abduction/adduction can be trained with the design shown in Figure 7(a). It should be noted that even though we can only train shoulder flexion/extension or abduction/adduction when the robot is connected to the upper-arm (Figure 7(a)), it does no restrict internal/external shoulder rotation movements. A participant can still make unassisted internal/external shoulder rotations while still connected to the robot, which is ensured by the three passive dof of the robot. Assisted training of the shoulder internal/external rotation dof can be done by connecting the robot to the forearm (Figure 7(b)), which can also be coupled with the elbow flexion-extension. It would be safer and more comfortable to carry out assisted shoulder internal-external rotation by applying forces on the forearm.
18
Another important feature of AREBO is the relaxed constraint on the patient’s relative position with respect to the robot. This feature is of significant practical value, as this has the potential to drastically reduce setup time for patients with more severe impairments or in a wheelchair. This ease in setting up the device translates to improved usability and can save time for the clinician when using the robot with multiple patients during a day. This reduced constraint in seating the patient and variations in human limb size between patients result in variations in the human limb’s workspace that can be supported by the robot, and also its manipulability. However, as long as these parameters are within a reasonable range specified in Table 1, the robot with optimized link lengths has an excellent workspace and a good manipulability. The optimized robot can cover, on average, 80% of the human limb’s workspace, and for about 60-70% of the points in the robot’s joint space, it is “easier” to apply a force orthogonal to the human limb.
The proposed algorithm for human limb parameter estimation allows AREBO to automatically estimate the location of the human joint with respect to the robot, and the length of the human limb, both of which are required for the complete specification of the human-robot closed kinematic chain. This can be done with a short calibration procedure (5 s long). The current results show that with the level of noise expected from rotary sensors, the human limb parameters can be estimated with relatively small bias and variance. There has been prior work on estimating human limb posture when connected to an exoskeleton robot,
21
and to plan the robot’s trajectory for a given human limb trajectory.
18
However, the authors are unaware of any prior work on estimating the location of the human joint and limb length using the human and robot joint kinematic data. One of the assumptions made by the proposed algorithm is that the human limb parameters are fixed over time. It is reasonable to assume that limb length does not change over time, but the same cannot be assumed about the limb’s location. For example, when the robot is connected to the upper-arm (as shown in Figure 7(a)), trunk or scapular movements will result in the translation of the glenohumeral joint. Thus, it would be ideal if the estimation can be implemented using data from the recent past in a recursive form with the following assumptions: Human limb length does not undergo any change over time. The location of the human limb does not undergo a drastic change in the window of data used for the estimation process.
Based on these assumptions, the recursive estimate at time n can be posed as multiple objective minimization problem,
We finally point out the limitation of AREBO’s simplicity gained at the expense of training coordinated multi-joint movements, i.e. the inability to perform assisted training of multi-joint movements possible with exoskeleton robots such as BONES, 10 ArmIn, 8 etc. From the neurorehabilitation perspective, the current evidence indicates that simple single-joint training is as effective as complex multi-joint training. 4 The study by Milot et al. showed that both single and multi-joint training with BONES resulted in improvements in both sensorimotor impairments and function. 4 About 75% of the participants in this study had an equal preference for both single-joint and multi-joint training with the robot. 4 There is also evidence for the transfer of training effects to untrained ADL, 5 which can be extrapolated to the possibility of single-joint training generalizing to complex multi-joint movements. Furthermore, single-joint exercises are an important component of training protocols in patients with severe sensorimotor impairments in impairment oriented training.23,24 These studies and the practical advantages of AREBO make a strong case for developing and evaluating the clinical usability and efficacy of such simple, compact robots for arm neurorehabilitation. If found to be therapeutically effective, such robots have the best potential for clinical translation and widespread adoption.
Conclusion
The paper presented the kinematic design and optimization of a compact 6-dof robot for individual joint training of the human arm. The proposed robot uses three actuated dof and three passive self-aligning dof keeping the overall structure of the robot simple and cost-effective. The proposed robot allows significant freedom in terms of the seating of a patient with respect to the robot, can easily accommodate arms of different sizes, and can be used for both the left and right arms without any change to its structure. The paper also presented an approach for automatically tracking the kinematic parameters of a human limb attached to the robot, which can be used by a robot controller to impose the desired movements to the human limb.
Footnotes
Declaration of conflicting interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Sivakumar Balasubramanian and S Sujatha.
Contributorship
SB, SG, and SS conceived the initial ideas for the robot and its design. SG and SB explored various potential designs for the robot. SB carried out the optimization of the robot link lengths. SB, SG, and JSM worked on the estimation algorithm and its evaluation through simulated data. SB prepared the first draft of the manuscript with help from SG and JSM. All authors reviewed the manuscript. SB and SS oversaw the activities of the project.
Acknowledgements
The authors thank Mr. Aravind Nehrujee, Mr. Samuel Elias, and Mr. Sathish Balaraman for their help in building and rendering the 3D models for the robot.
Note
I. A kinematic chain is an assembly of rigid bodies that are interconnected through a set of joints to allow constrained movements with respect to each other. A closed kinematic chain is one that forms loops and every link is connected through two joints to two adjacent links.