
Abstract
In response to the growing demand for robotic interventions to mitigate the profound physical strain experienced by caregivers during transfers, dual-arm robotic systems have emerged as a focal point of interest in the caregiving community due to their adaptability and versatility. However, the accuracy of existing human–robot mechanics model is insufficient, impacting the execution of transfer tasks. To enhance the model’s precision, an improved model is proposed, integrating hip torque identification. This proposed methodology involves the simplification of the human structure based on the kinematic attributes associated with the embrace of individuals by robotic arms and the subsequent computation of its inertial parameters. Accordingly, the application of D’Alembert’s principle is employed to analyze the impact of embracing motion, human posture, and the position of human–robot contact on the forces exerted on the human. This culminates in the establishment of a model. Considering the static indeterminacy predicament inherent in the model, a biomechanical data set is curated for the dual-arm transfer scenario. Leveraging this data set, a deep neural network utilizing multilayer perceptron is trained to accurately identify hip torque, thereby improving the model. Accordingly, a robotic transfer platform featuring dual arms is developed and trailed on six subjects with varying anatomical profiles. The results show that the constructed model has high accuracy. This study provides critical mechanics insights for dual-arm transfer tasks, offering potential application value in the field of nursing and rehabilitation.
Introduction
With the global population aging and the declining birth rate exacerbating, the scarcity of nursing personnel and the demand for high-quality nursing services have become increasingly prominent. 1,2 The efficient and flexible transfer of disabled elderly individuals has emerged as a significant concern in routine nursing practice. Conventional manual handling methods not only impose strain on the musculoskeletal systems of caregivers but also result in repetitive and arduous physical labor. 3,4
Caregiving robots have been acknowledged as pioneering solutions for addressing the challenges in the caregiving domain. 5,6 The bed-chair separated robot offers an indoor mobility solution for care recipients by integrating the design attributes of a wheelchair and a nursing bed. Nonetheless, the structure and cost of the robot impede its widespread adoption. 7 The single-arm transfer robots, while attracting attention for their simple structures and lower costs, fall short in terms of operational flexibility and multitasking capabilities. 8 Full-body wearable robots hold the potential to enhance caregivers’ carrying capabilities, but their technological maturity necessitates further enhancement. 9,10 The dual-arm nursing-care robot, designed for transferring care recipients between household appliances, is equipped with anthropomorphic arms and flexible movements. Hence, the research and development of this robot have attracted attention in nursing care. 11,12
The transfer assist robot developed by KIMM in South Korea, 13 RIBA and ROBEAR developed by RIKEN in Japan, 14,15 as well as RoNA developed by Hstar Technologies in the United States 16 have demonstrated potential advantages in nursing care. However, existing research has primarily centered on the robots’ structural design and operational mechanisms. In the field of human–robot mechanics model (H-R model), crucial for controlling the robot to complete transfer tasks, current research has not yet received adequate attention. Dual-arm transfer, as a non-grasping manipulation technique for multilinked objects, involves the robot interacting with the care recipient using the entire surface of its arms rather than just the end-effector. 17 While current research predominantly focuses on the manipulation of single-linkage objects using robotic arms, 18 further exploration of dual-arm transfer tasks is necessitated.
To control robots in completing transfer tasks, scholars have undertaken the abstraction of the human body into diverse linkage mechanisms, thereby formulating corresponding H-R model. Notably, Zyada et al. 19,20 employed a two-linkage mechanism and characterized contact pressure through a viscoelastic model, utilizing the Newton–Euler method for H-R model. However, this H-R model failed to account for frictional factors, thereby impinging upon the precision of control strategies and system stability. Building upon this, Jiang et al. 21,22 advanced the discourse by introducing the LuGre friction model, analyzing the equilibrium regions under frictional conditions. However, the pertinent research overlooked the mechanics attributes of the head-neck and lower leg, thereby amplifying operational risks. Similarly, Mehrez et al. 23,24 embraced a three-linkage mechanism and introduced the concept of a friction cone, employing the Lagrangian method for H-R model to explore the impact of frictional forces on balance. Nevertheless, their treatment of human joints as passive elements diverged from actual biomechanical principles. Conversely, Chen et al. 25 adopted a four-linkage mechanism under the premise of active joints, establishing a H-R model based on Newton’s second law. Nonetheless, their reliance on assumptions pertaining to friction and normal forces deviated from the actual mechanics of the human body. In an effort to refine this H-R model, Guan et al. 26 integrated real-time contact pressure measurement as an additional equation. While this enhancement bolstered H-R model precision, it necessitated the premeasurement of the cared-for individual’s pressure in all conceivable postures and human–robot contact positions. This process not only involved labor-intensive procedures but also increased the risk to the cared-for individual.
Therefore, in this study, an innovative approach was employed to integrate theoretical modeling of human–robot mechanics with hip torque identification, resulting in the construction of a H-R model that adheres to the human’s biomechanical properties. The human structure was simplified into a four-linkage mechanism, including the head-neck and lower limbs in its sagittal plane, and its inertia parameters were estimated based on transfer characteristics. By applying D’Alembert’s principle, a H-R model that accounts for friction and active joint factors was established. Addressing the static indeterminacy problem in the H-R model, human–robot biomechanics data sets for the dual-arm nursing-care transfer scenario was curated, and the multilayer perceptron (MLP) network 27 was employed to identify human hip torque, thereby improving the H-R model and significantly increasing H-R model accuracy. Moreover, an experimental platform for dual-arm robotic transfer was developed, and a series of experiments involving subjects of varying figures were conducted, yielding results that indicate a high level of accuracy in the H-R model. Finally, the research findings were summarized, and potential directions for further work were outlined.
Dual-arm nursing-care transfer robot structure
To address the issue of human–robot safety interaction during high-load transfer tasks, our research team has engineered a dual-arm nursing-care transfer robot characterized by a compact structure, high load-bearing capacity, and humanoid attributes. 11 The three-dimensional structure of the nursing-care robot is depicted in Figure 1(a), comprising a mobile chassis, a torso, and two robotic arms. The mobile chassis is equipped with McNamee wheels, endowing the robot not only with omnidirectional mobility but also with exceptional flexibility, enabling rapid localization and maneuvering in confined spaces, thereby significantly enhancing navigation efficiency and real-time responsiveness. The torso design is inspired by bionics principles and emulates the biological structure of the human body through the incorporation of waist and hip joints, thereby simulating human torso movements and conferring bionic left–right swinging and forward–backward pitching capabilities upon the robot. This design approach not only enhances the dynamic stability of the robot but also renders its interactions with humans more harmonious.

Dual-arm nursing-care robot: (a) three-dimensional model; (b) configuration of robotic joint DOF; and (c) physical rendering. DOF: degree of freedom.
The arm joints are equipped with 2R-coupled drives, and three such joints are connected in series to form a six-degrees of freedom (DOF) collaborative arm for the care robot. The schematic representation of the robot’s joint DOF configuration is depicted in Figure 1(b). This joint configuration allows for the superimposition of the output torque of two motors, thereby enhancing load-bearing capacity and joint stiffness. 28 In addition, the compact layout and sleek form-factor structure of the robotic arm endow it with a morphology akin to that of the human arm, thereby enhancing the bionic characteristics of nursing-care operations. This innovative design strategy effectively surmounts the challenges associated with the structural configuration, form factor, and load-bearing capacity of mobile nursing-care robots, thereby significantly enhancing their performance in practical applications. Figure 1(c) presents a physical rendering of the nursing-care robot.
Decomposition of human transfer movements
In the performance of a dual-arm transfer operation by the nursing-care robot, involving direct contact of its arms with the thighs and back of the care recipient, a comprehensive analysis reveals six fundamental phases, as presented in Figure 2: initial preparation, arm contact, stabilizing hold, postural adjustment, steady movement, and precise placement. These phases are derived from the emulation of human hugging actions. The study was conducted in accordance with the Declaration of Helsinki, and all participants provided written informed consent.

Design of human-like dual-arm hugging action in transfer tasks: (a) initial preparation; (b) arm contact; (c) stabilizing hold; (d) posture adjustment; (e) steady movement; and (f) precise placement.
As the robotic arms execute the transfer, the human body’s posture undergoes corresponding changes, inevitably resulting in changes to the human-robot contact force and the internal force exerted on the human body. An in-depth study into the influence of human body posture on these forces is necessary for understanding and optimizing the transfer actions of nursing-care robots. Upon analysis, it is identified that the cervical joint, hip joints, and knee joints predominantly impact the human body’s posture. To delve deeply into the correlation between force and human body posture, a simplified representation of the human body is constructed as a four-linkage mechanism interconnected by the cervical, hip, and knee joints on the sagittal plane, as depicted in Figure 3. This mechanism consists of a head-neck unit, upper body, thighs, and lower legs, with the cervical, hip, and knee joints serving as rotational joints linking the components. This simplified mechanism facilitates an intuitive analysis of the forces acting on the human body during arm transfer, thereby enabling the enhancement of the action control strategy of the nursing-care robot and the augmentation of transfer efficiency.
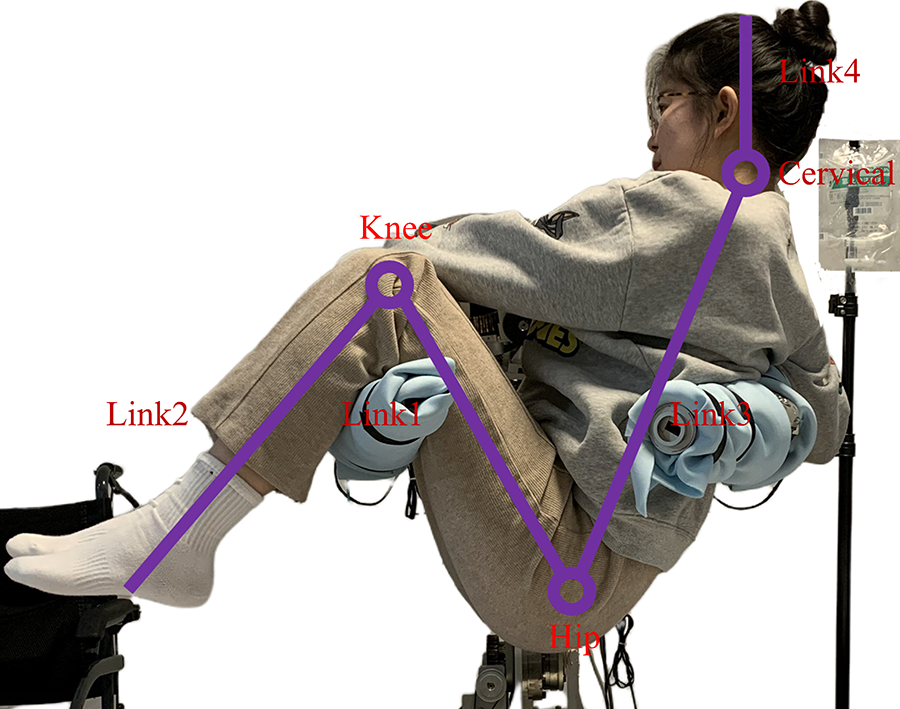
Four-linkage mechanism of the human body.
In modeling the kinematics and mechanics of human–robot systems, the direct measurement of the inertial parameters of the care receiver is beset by numerous challenges. In accordance with the guidelines stipulated in the national standard “Inertial Parameters of the Adult Human Body,” 29 this study undertook the computation of the inertial parameters, including mass, center of mass position, and moment of inertia, for a simplified four-linkage mechanism of the human body. The inertial parameters for each body segment were determined utilizing the following regression equation

where B 0, B 1, and B 2 represent the coefficients in the regression equation and can be obtained by referring to the national standard, respectively. X 1 and X 2 represent the height and weight of the human, respectively.
According to the national standards, the calves, feet, upper torso, lower torso, and arms are all identified as independent body segments. In the human structure simplified for the purposes of this study, the lower legs and feet were merged into link 2, while the upper torso, lower torso, and arms were merged into link 3. The computation of the inertial parameters for links 2 and 3 was undertaken, albeit the specific calculations are omitted herein due to spatial constraints.
Human–robot mechanics model
Throughout the process of robot transfer, the human–robot interaction force directly influences the control of the robot’s movements. These forces are determined by a multitude of factors, including the robot’s movement, the position of contact between the human and robotic arms, and human posture. To provide an accurate depiction of the force experienced by the care receivers, this study describes the human–robot system, conducts a kinematic analysis, and thus formulates the corresponding H-R model.
System description
The simplified mechanism of the human–robot system for transfer with robotic arms is delineated in Figure 4. In Figure 4(a), the inertia parameters for each link in the simplified mechanism of the human structure are presented. The distances from the hip to the centers of mass of links 1 and 3 are denoted as l 1b and l 3a, respectively. In addition, the distances from the knee to the center of mass of link 2 and from the neck to the center of mass of link 3 are represented as l 2b and l 4a, respectively. The mass, length, and moment of inertia for each link relative to its center of mass are indicated as mi , li , and Ji (i = 1, 2, 3, 4), respectively.

Simplified model of human–robot system: (a) inertia parameters for each link and (b) contact position and human posture.
Figure 4(b) illustrates a simplified mechanism of the contact position between the human and the robotic arms and the human body posture. The origin of the base coordinate system o 0-x 0 y 0 coincides with the rotation center of the hip, and its coordinate axis direction aligns with the world coordinate system Σ 0. The coordinate system oi -xiyi (i = 1, 2, 3, 4) of the link i is affixed on the link, and its origin is situated at the rotation axis of the link. With the world coordinate system Σ 0 as a reference, the position of the hip is denoted by (x, y). The angles between links 1 and 3 and the horizontal plane are represented by θ 1 and θ 3, respectively, while the angles between links 1 and 2, as well as links 3 and 4, are denoted by θ 2 and θ 4, respectively. In addition, the distances from the contact point between the robotic arm and the human thigh and back to the hip are expressed as d 1 and d 2, respectively. Therefore, the comprehensive positioning of the care receiver in the world coordinate system is achieved.
Theoretical derivation of the human–robot mechanics
The H-R model developed in this study is specifically designed for the “posture adjustment” phase. During this phase, it is assumed that the robot’s arms remain horizontal, resulting in the human experiencing primarily planar forces. In light of the potential nonequilibrium states that may be encountered by nursing-care robots during dual-arm transfer operations, this study employs D’Alembert’s principle 30 to establish a precise H-R model. The primary objective of this H-R model is to accurately capture the mechanics behavior during the transfer process and ensure its adaptability under quasi-static conditions (where both velocity and acceleration are zero), thereby enabling a comprehensive analysis of the mechanics behavior of the human–robot system throughout the operation.
To achieve an accurate H-R model, a detailed kinematic analysis of each link in the mechanism is essential. Based on the acquired motion parameters, the inertial forces acting on the links are computed. Considering that the simplified human mechanism exhibits a chain-like structure, this article relies on the kinematic iteration algorithm for chain structures 31 to conduct an in-depth analysis of a specific link (link 1), resulting in the determination of the angular and linear acceleration for link 1 as follows

where
Upon calculating the velocity and acceleration of link 1, an in-depth analysis of the inertial forces acting upon it was undertaken. This led to the derivation of the magnitudes of the tangential inertial force, normal inertial force, and inertial torque at the axis of rotation of the link, as presented below

Similarly, the magnitudes of the normal inertial forces, tangential inertial forces, and inertial torques acting at the axes of other links are denoted as
Following the determination of the inertial forces exerted on each link of the simplified human mechanism, the H-R model was modeled utilizing D’Alembert’s principle. This methodology involves treating the active forces, constraint forces, and inertial forces on each link as a system of forces in formal equilibrium. In the simplified mechanism of the human body, each link satisfies two force balance equations and one torque balance equation, resulting in a total of 12 independent equilibrium equations.
Considering the overall body segment as the subject of study, its force diagram is depicted in Figure 5(a). The care receiver maintains balance under the influence of their own body weight, the support forces exerted by the robotic arms on the thighs and back, and the virtual inertia forces applied to the axes of rotation of each link. Here, the support forces can be decomposed into normal forces Fi (i = 1,2) perpendicular to the contact surface and tangential forces fi (i = 1,2) along the contact surface. Based on the conditions for equilibrium of planar force systems, the following relationship is obtained


Force analysis of each body segment of the human–robot system: (a) overall body; (b) lower leg; (c) lower body; and (d) head and neck.
where




In the context of the isolated lower leg segment, the force diagram is presented in Figure 5(b). The lower leg maintained equilibrium through the counterbalancing of its intrinsic gravitational force, the virtual inertia forces introduced at the pivot point of the link, and the constraint reaction forces

Considering the lower body as an independent entity, its force diagram is depicted in Figure 5(c). The lower body sustained equilibrium through the relationship of its own gravitational force, the supportive forces exerted by the robotic arms on the thighs, the virtual inertia forces introduced at the pivot points of the lower leg and thigh, and the constraint reaction force

where


Shifting focus to the isolated head and neck segment, the force diagram is depicted in Figure 5(d). The head and neck maintained equilibrium through the counteraction of their intrinsic gravitational force, the inertia forces, and the constraint reaction force

In this study, the H-R model with a dual-arm nursing-care transfer robot was successfully formulated through the simultaneous equations (5) to (8). This H-R model adeptly illustrates the relationship among robot trajectory, human body posture, human–robot contact position, and human body force. To adhere to the safety prerequisites for the care recipients, the robot’s angular velocity and angular acceleration were both set to zero during the initial experimental phase to ensure the fluidity of the holding movement. Under these stipulations, the H-R model established in this study is utilized for static computation and offers potential solution strategies for subsequent dynamic analyses.
However, it should be noted that in the H-R model, there remain 13 unknown quantities, while only 12 independent equilibrium equations can be listed, thereby resulting in static instability in the system. Specifically, for the force analysis of the lower leg and head-neck body segment, six independent equilibrium equations can be listed, thus enabling the resolution of the internal forces
This observation unveils a critical problem: the determination of specific values for the internal force at the hip joint and the external force at the human–robot contact during hugging. If either of these values can be determined, the entirety of the force values on the human body can be completely resolved. Therefore, further research and data collection are necessary to address this issue and improve the H-R model.
Hip torque identification method based on deep neural network
In modern scientific and technological applications, sensor technology assumes a pivotal role. However, the direct measurement of friction force between humans and robots, as well as the internal force at the hip joint, presents formidable challenges. While the deployment of tactile sensors on the robotic arm offers a potential solution for acquiring human-robot contact pressure, it necessitates the prior measurement of the care receiver’s pressure in all conceivable postures and human-robot contact positions during the transfer process. This not only contributes to a time-consuming and labor-intensive process but also elevates the risks for the care receiver.
To effectively confront the aforementioned challenges, this study has undertaken the construction of a human–robot biomechanics data set for the dual-arm nursing-care transfer scene within a simulation environment. Accordingly, a deep neural network has been employed based on this data set to accurately identify the hip torque of different care receivers in various postures and human–robot contact positions, thereby bridging the gap in mechanics modeling and significantly mitigating the risk to the care receiver. This method transcends the limitations of traditional sensor technology and paves the way for a viable and efficient new approach to the research on H-R model with a dual-arm nursing-care transfer robots.
Data set construction
In the field of biomechanics and physiology, the AnyBody multibody mechanics modeling system has been utilized to provide a comprehensive human musculoskeletal model grounded in anatomical principles, 32 as depicted in Figure 6(a). In addition to offering preexisting models, this system affords researchers the capability to craft models tailored to specific requirements through the utilization of the AnyScript scripting language. 33 Notably, this system possesses the capacity to accommodate individual variations in skeletal structure and musculature, thereby offering a robust platform for the precise prognostication of internal loads imposed on the human body during routine activities. 34 This study is centered on the biomechanical response of the care recipient to the surrounding environment during the transfer facilitated by robotic arms.

Modeling process of the human–robot system: (a) human musculoskeletal model; (b) simplified robot structure; and (c) human–robot system.
To enhance the computational efficiency of the simulation and mitigate the impact of nonessential variables, the 3D structure of the nursing-care robot was streamlined using Solidworks. Accordingly, this simplified structure was converted to STL format to conform to AnyBody’s import criteria. After importing all the components, the robot model was reconstituted to ensure the relative part positioning and joint interconnection, as presented in Figure 6(b). Meanwhile, the relative positions of the robot and human were in a freely floating, separated state within the AnyBody. To establish a simulation model of human–robot contact, the relative positions were adjusted to ensure the robot’s arms to contact with the human’s back and thighs. Following this sequence of operations, the nursing-care robot was effectively integrated with the human, thereby enabling the construction of the simulation model for the dual-arm transfer, as illustrated in Figure 6(c). In the simulation model, the AnyScript scripting language was utilized to define a series of contact points on the robot arm’s forearm section as well as on the human’s back and thighs. By defining contact points at these locations and using the scripting language to constrain their relative positions, the human–robot contact is simulated.
In the current field of multidimensional pattern identification, a publicly accessible human–robot biomechanics data set for transfer tasks in nursing-care scenarios has been notably absent. Therefore, to bridge this gap and enhance the precision of H-R model, this study utilizes the AnyBody system to construct a human–robot biomechanics data set for the transfer nursing-care scene involving a dual-arm robot. Notably, the data set consists of 450 individuals with heights spanning from 155 cm to 180 cm, and appropriate weights are assigned to these virtual individuals according to the body mass index (BMI) classification standard of the national standard “Adult Weight Determination.” 35
These individuals are categorized into three groups, each consisting of 150 people, corresponding to the three BMI categories: underweight, normal, and overweight. Each individual comprises 6000 samples, each of which details the joint torques generated by the individual’ hip muscle groups to uphold bodily equilibrium at various human–robot contact points and body postures during changes in the robot arm position. In this study, samples are randomly selected from the three BMI groups in an 8:1:1 ratio to constitute the training, validation and test sets, with a segment of the data set labels presented in Table 1.
Transfer nursing-care task data set labels.

Network construction and key parameters
Considering the complexity of human–robot interaction forces in transfer tasks, especially the nonlinear variability of hip torque due to differences in subjects’ body types, human–robot contact points, and human postures, this study employs the MLP network to prognosticate the hip torque. The network consists of an input layer, three hidden layers, and an output layer. The input layer receives raw data, the hidden layers process the data through activation functions, and the output layer generates prognostications for hip torque.
In this study, the MLP network is instantiated employing the PyTorch framework and trained utilizing the aforementioned self-compiled data set. A normalization strategy is implemented to enhance the network’s identifiable precision before the network training started. This strategy obviates the dimensional influence of the data, thereby ensuring that the network can identify the interrelationships between features more accurately. To expedite the training process, the network and data are transposed onto the CUDA platform equipped with an NVIDIA GTX2070 graphics card, utilizing the GPU’s parallel computing capabilities to complete network training. Regarding the principal hyperparameters of the network, including the learning rate, batch size, and number of training iterations are encapsulated in Table 2 for the further optimization of the network’s performance.
Hyperparameters of the Deep Learning Network.

Identification results of hip torque
After 300 epochs of deep learning, the network for hip torque identification exhibited a mean absolute error (MAE) of 5.14e−3 and a mean squared error (MSE) of 4.83e−5 between the network’s identified and simulated values of the hip torque on the training set. On the test set, the network’s identified hip torque values exhibited an MAE of 6.75e−3 and an MSE of 6.42e−5 compared to the simulated values, demonstrating the network’s high accuracy and reliability in the task of hip torque identification.
To further analyze the network’s error characteristics, seven data points were randomly selected from the test set for a detailed error comparison (Figure 7), and the comprehensive data are summarized in Table 3. Considering the constraints of MSE in appraising the degree of network data fit, the coefficient of determination (R 2) was also incorporated in this study as a supplementary evaluation criterion. A high R 2 value denotes a commendable network fit, while a low value signifies a subpar fit, thereby evaluating the network’s fitting capacity by quantifying the proportion of the network’s output variance explicated by the network’s features. The formula for its computation is as follows

where
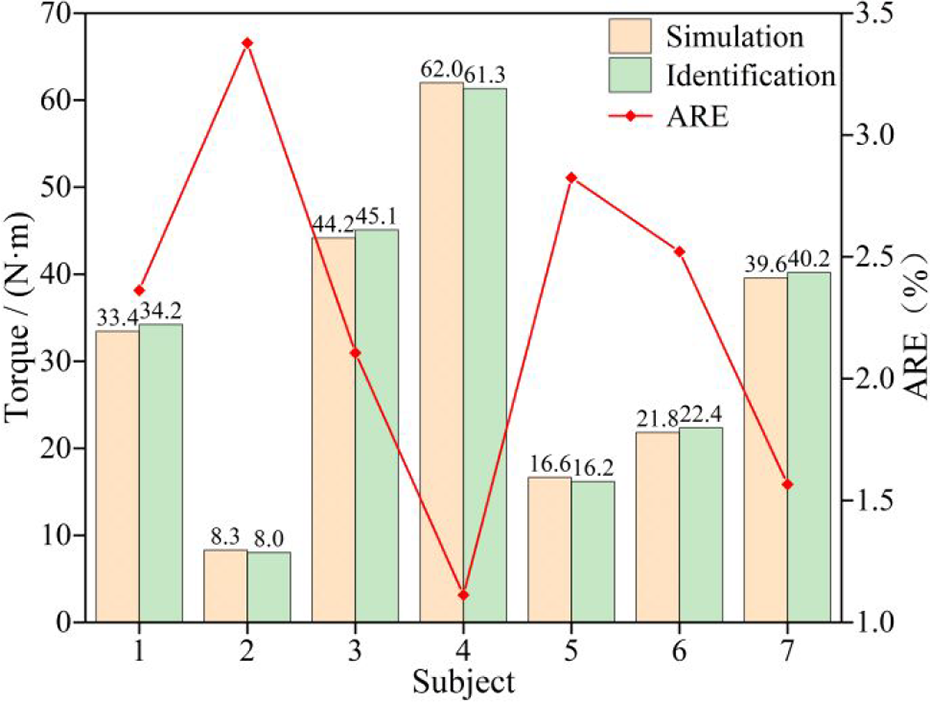
Comparison of hip torque identification values with simulation values.
Hip torque identification results at random sampling points in the test set.

From the seven randomly selected data points in the test set, it is evident that significant differences are present in the physical attributes, human–robot contact positions, and human postures of the subjects. The range of hip torque spans from 8 N·m to 70 N·m, and the average relative error (ARE) of the hip torque values identified by the network was consistently below 3.5%. The coefficient of determination R 2, as derived from equation (9), stands at 0.997, signifying the close correspondence between the network’s identified and simulated hip torque values. This attests to the efficacy of the deep neural network proposed in this article, which is founded on MLP, in establishing a precise nonlinear mapping relationship between hip torques and the characteristics of human posture and human–robot contact position. The network demonstrates robustness in accommodating individuals with diverse physical attributes, thereby affirming its practical utility in pertinent domains.
Validation experiment
The experimental segment of this study is dedicated to validating the hip torque identification method predicated on the MLP network and its impact on the precision of the H-R model with a dual-arm nursing-care transfer robot. Considering the inherent technical impediments in directly measuring hip torque, an indirect validation approach was embraced. Firstly, the MLP network was trained using a data set constructed in a simulated environment to prognosticate hip torque values. Subsequently, these prognosticated values were assimilated into the H-R model to compute theoretical pressure values in the subject’s back contact area of the human–robot interface. By comparing the pressure values prognosticated by the H-R model with the actual values measured by the experimental platform, this study comprehensively evaluated the precision of the H-R model and indirectly substantiated the efficacy of the MLP network in practical application scenarios.
Experimental scenario
To collect real-time pressure data in the contact area between the robotic arm and the care subject’s back during the transfer process, a comprehensive experimental platform was established (Figure 8). This platform comprised a custom-built dual-arm nursing-care robot, an OptiTrack motion capture device from Natural Point, and a high-precision pressure acquisition device from Tekscan. In addition, to assess the generalizability and adaptability of the trained MLP network when confronted with individuals of varying body sizes, six subjects with diverse body dimensions were recruited for the experiment, with detailed individual information provided in Table 4.

Construction of an experimental platform.
Information of experimental subjects.

The experimental setup phase included the calibration of the OptiTrack motion capture system and the Tekscan pressure sensors. For the OptiTrack system, five optical cameras were strategically positioned to cover the entire experimental area, and a calibration wand was utilized to enhance tracking accuracy. As for the Tekscan pressure sensors, calibration was accomplished by applying weights of varying magnitudes on the sensors and recording the corresponding electrical signals to establish a correlation between weight and signal, thereby ensuring measurement precision.
During the preparatory phase of the experiment, reflective markers were affixed to seven pivotal anatomical sites of the care recipient’s body (specifically, the ankle joint A 1, knee joint A 2, hip joint A 3, trunk A 4, shoulder joint A 5, neck joint A 6, and head A 7) as well as on the robotic arms, as depicted in Figure 8, to capture the nuances of human posture and the precise positioning of human-robot contact. In addition, tactile sensors were strategically deployed on the forearms of the dual-arm nursing-care robot to record real-time pressure data at the points of contact on the subject’s back during the transfer process. Accordingly, all the amassed data were transmitted in real time to a laptop for subsequent analysis.
During the execution phase of the experiment, the subjects were systematically lifted through the controlled manipulation of the robotic arms, with each subject being positioned at different contact points on their thighs and back, and the maintenance of a consistent human–robot contact position post-lifting. In addition, the posture of the care recipients was systematically changed by adjusting the positioning of the dual-arm nursing-care robot to lift the care recipients in accordance with various predefined maneuvers, thereby effectively mitigating operational risks.
Following the experiment, the amassed data, including human posture, human–robot contact points, and other pertinent characteristic parameters, were input into the trained MLP network to prognosticate the hip torque of the subject. This prognosticated value was subsequently integrated into the constructed H-R model to calculate the theoretical pressure values at the contact points on the subject’s back.
Throughout the course of the experimental procedure, the continuous operation of the motion capture and pressure collection devices ensured the real-time acquisition and documentation of contact pressure data at various postures and points of human–robot interaction. Notably, during the transportation phase of the experiment, the posture of subjects was precisely calculated utilizing data from body markers captured by the motion capture system. Elaborate methodologies and theoretical underpinnings for the computation of human posture can be referenced in the author’s previously published research. 26
Experimental results
To deeply analyze the accuracy and reliability of the H-R model formulated in this study, it was compared with the back-contact pressure values computed in our previous work, 25 with the objective of appraising the efficacy of each H-R model through the MSE between theoretical computations and empirical measurements. The veritable values of the experimental data were derived from empirical measurements on each subject. During the data processing phase, four sets of data were arbitrarily chosen from the measurements of each subject. Each set of data encompassed independent variables: the human–robot contact position, human posture, and human characteristic parameters; the dependent variable was the contact pressure on the back. These independent variables were input into the H-R model formulated in this study and our previous work to compute corresponding theoretical back pressure values, which are succinctly summarized in Table 5. Furthermore, to quantitatively analyze the deviation between theoretical computations and empirical measurements across this study and our previous work, a comprehensive MSE comparative analysis was undertaken, the results of which are presented in Figure 9.
Theoretical computations and empirical measurements contact pressure values on the back area under different postures and human-robot contact positions.

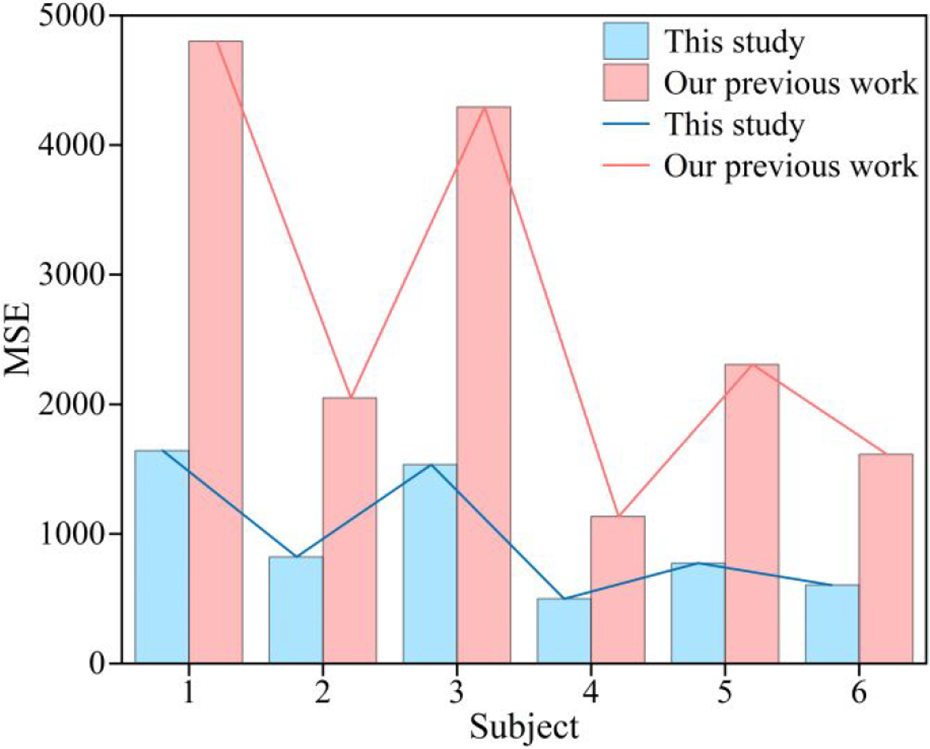
MSE comparative analysis between theoretical computations and empirical measurements across this study and our previous work. MSE: mean squared error.
In Table 5, a detailed comparison between theoretical pressure and actual measurement values was conducted, revealing that the contact pressure values calculated by the present H-R model exhibited a closer proximity to reality in comparison to our previous work, both at the level of individual data and in overall trends. In addition, the bar chart depicted in Figure 9 illustrates that the H-R model constructed in this study significantly outperforms our previous work in terms of MSE across subjects with different body types. This is because our previous work is primarily based on the assumption of dependency between frictional and normal forces. While this approach simplifies the complexity of human–robot contact friction to some extent, it also introduces significant errors in model construction. In contrast, this study employs a musculoskeletal model created with AnyBody, which is closely similar to the actual human body. This allows the H-R model to more accurately reflect the real mechanical behaviors of the human body and the human–robot interaction process, thereby achieving a smaller MSE between theoretical calculations and actual measurements.
Further quantitative analysis results show that compared with our previous work, the MSE of this H-R model is reduced by 63.71% on average. This result not only substantiates the model’s superiority in theoretical computations but also attests to its reliability in practical applications. The combination of findings from Table 5 and Figure 9 highlights the model’s sustained high accuracy and reliability across diverse combinations of human–robot contact positions, human postures, and human characteristic parameters. In addition, this demonstrates that the method of setting contact states in the simulation employed has proven to be effective.
Compared to our previous work, 25 which relies on the friction and normal force dependency assumption, this study significantly improves the model’s accuracy. Unlike the method in the study of Guan et al. 26 that required premeasuring contact pressure between humans and robots for supplemental equations, this study reduces reliance on extensive data collection, lowers the risk to care recipients from repeated measurements, and enhances the model’s generalizability. Therefore, the mechanics modeling method expounded in this study stands as a potent instrument for optimizing the design of nursing-care robot transfer actions, holding potential application value in the field of nursing and rehabilitation.
Conclusions
This study is centered on the modeling method of the H-R model for the transfer task of dual-arm nursing-care robots, with the overarching objective of enhancing the accuracy of modeling in robot-assisted transfer. The principal research results are as follows:
(1) This article introduces a novel modeling approach for the H-R model, where the human body is represented as a simplified four-linkage mechanism. This H-R model effectively captures the force experienced by the care receiver during transfer activities. It achieves this by taking into account the robot’s motion trajectory, the contact points between the human and the robot, the human’s posture, and the internal forces in the active joints.
(2) The study also presents the creation of a biomechanical data set specific to the human–robot system in a transfer nursing-care scenario. In addition, the MLP network for identifying hip torque is proposed. Utilizing this data set, a refined network has been developed to identify the hip torque in varying contact positions and postures of the human–robot interaction. This network addresses the issue of static uncertainty effectively, allowing the mechanics system to achieve a state of static equilibrium.
(3) Experimental validation of the H-R model’s accuracy and stability was conducted using a custom-designed experimental platform. However, the current H-R model exhibits limitations in handling individuals with larger body types, particularly failing to adequately consider the characteristics of obese physiques, suggesting the necessity for incorporating a more diverse range of human body characteristics in future H-R model enhancements.
A significant limitation of this study is that the current modal does not consider human body inclination as shown in Figure 2. Future research will address this by incorporating a more complex three-dimensional H-R model, and efforts will also be made to develop a more comprehensive data set to enhance the network’s identifiable precision. This will facilitate a thorough analysis of the force variations experienced by care recipients during different transfer phases. In addition, the current study lacks comprehensive testing in real-world scenarios. Future efforts will focus on exploring more robust modeling approaches to handle uncertainties and plan to simplify redundant data and equipment to enhance the system’s practicality.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by the Shanghai Science and Technology Program (grant No. 21511101701), the National Key Research and Development Program of China (grant No. 2021YFC0122704), and the National Natural Science Foundation of China (grant No. 11902110).
Research ethics and participant consent
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Fudan University (Approval Code: FE23118R; Approval Date: 4 June 2023). All participants provided written informed consent.