
Abstract
Introduction
Conflicting evidence exists regarding the effects of knee orthoses on proprioception. One belief is that pressure applied by orthoses heightens kinesthetic awareness and that this affects balance. This study aimed to investigate the effects of two different orthosis designs on kinesthetic awareness and balance in healthy individuals.
Methods
Twenty individuals (13 women) participated in this case series study. Each was tested wearing 1/no orthosis, 2/soft elastic orthosis and 3/non-elastic jointed orthosis. Pressure under orthoses was recorded. Kinesthetic awareness was investigated by testing joint position sense and threshold to detection of passive motion. Balance was tested using a modified sensory organization test.
Results
Non-elastic jointed orthoses applied the greatest pressure to the knee. With non-elastic jointed orthoses, threshold to detection of passive motion was significantly poorer for pooled results (p = 0.02) and when the start position of the knee was 70° (mean threshold = 0.6°, 0.6°, 0.7° for no-orthosis, elastic and jointed-orthoses; p = 0.03). No major differences were observed in JPS or balance and correlation between proprioception and balance was poor.
Conclusions
There may be a limit to the amount of pressure that should be applied to the knee joint by an orthosis. Exceeding this limit may compromise kinesthetic awareness.
Introduction
Knee orthoses are commonly prescribed for a variety of conditions, including osteoarthritis, 1 cruciate ligament deficiencies, 2 stroke 3 and as a prophylactic measure in non-injured groups. 4 The primary goals when prescribing a knee orthosis are often cited as pain reduction, increased stability and improved joint control. 5 It has been suggested that improvements in stability and joint control associated with the use of knee orthoses are associated with enhanced joint proprioception 5 and can enhance balance performance.6,7 Evidence to support this is however inconsistent.
A proprioceptor can be broadly defined as a receptor that facilitates conscious sensations. This includes the sense of limb position, limb movement, tension or force and balance. Kinesthesia is the term used to refer to sensations of limb position and movement. 8 Information from the proprioceptive senses are crucial for kinesthetic awareness and play an important role in both motor planning (feedforward mechanisms) and adaptation to effect performance (feedback mechanisms). 9 Reduced proprioception may lead to a multitude of functional problems, including increased postural sway, 10 decreased balance and an increased risk of falls. 11 The mechanisms underlying proprioception have been debated extensively and it is generally accepted that joint receptors, muscle spindles, Golgi tendon organs and cutaneous receptors all play a role to varying degrees.9,12
Due to its complex nature, there is no single measure that captures all aspects of proprioception. 9 Several tests have, however, been identified to quantify kinesthetic awareness on a functional level. These tests typically make the distinction between two proprioceptive functions, detection of static position and detection of motion. 9
The extent to which knee orthoses influence kinesthetic awareness is unclear. While some report improved joint position sense or detection of motion, in healthy individuals and in those with a pathology,6,13–15 others report no such effect.16–18 In a recent systematic review and meta-analysis, Ghai et al. 19 concluded that joint stabilisers, including orthoses, have a positive effect on kinesthetic awareness at the ankle but neglible effects on postural stability. In contrast, the systematic review performed by Sugimoto et al., 20 focusing on orthotic use after ACL reconstructions, found insufficient evidence to support the statement that orthoses have a positive effect on joint position sense at the knee. Few studies related to knee orthoses have incorporated multiple tests of kinesthetic awareness, with the majority choosing to report only joint position sense.6,14,20 Application of multiple tests of kinesthetic awareness within a single study may provide a greater understanding of the mechanisms by which a knee orthosis affects kinesthetic awareness and is recommended by Herrington et al. 15 who demonstrated that there is limited correlation between detection of static position tests and detection of motion tests.
Improvements in kinesthetic awareness alone are unlikely to have major implications for individuals unless they are correlated with improvements in functional performance. A limited number of authors have investigated the relationship between kinesthetic awareness and functional performance and results are generally inconclusive. Birmingham et al. 6 and Kuster et al. 7 indicated that knee orthoses enhance both kinesthetic awareness and balance. Some authors report improvement in kinesthetic awareness with no improvement in balance.21,22
Little is understood of the physiological mechanisms that are influenced by the application of an orthosis. While some suggest that pressure applied to the joint via an orthoses stimulates somatosensory pathways that are processed through reflex loop mechanisms,23,24 others suggest that skin, muscle and other joint receptors are affected by the orthotic pressure and that this has an effect on kinesthetic awareness. 25 Simoneau et al. 26 provided evidence to support the role of cutaneous feedback in proprioception by demonstrating improved joint position sense and detection of motion when a single strip of tape was applied over the ankle joint. This suggests that shear forces applied to the skin through the application of tape may be influencing kinesthetic awareness.
While specific physiological mechanisms influencing proprioception remain unclear, it is likely that the design of an orthosis may influence their function. This could be achieved by manipulating the amount of pressure applied to the soft tissues and joint capsule via an orthotic device or through shear forces experienced at the interface of the skin and the orthosis.
The aim of the present study was to determine if knee orthosis design is associated with levels of kinesthetic awareness and balance performance in a group of able-bodied adults and to explore if there is a correlation between kinesthetic awareness and balance performance. It was hypothesized that application of an orthosis designed to apply increased pressure to the soft tissues and joint capsule would be associated with heightened kinesthetic awareness and that this in turn would correlate with improved balance performance.
Materials and methods
Subjects
An a priori power calculation was performed to determine appropriate sample size using previously published JPS data by Herrington et al. 15 The results indicated that approximately 20 participants would be required to detect a statistically significant difference (p < 0.05), with a statistical power of 0.8 and a true difference between the groups of 0.6°.
Twenty healthy individuals (13 females) participated in the study. Participants volunteering were required to be over the age of 18 and were recruited through pamphlets that were placed on notice boards at Jönköping University. Prior to the study, each potential participant was requested to complete a questionnaire about past injuries and current levels of pain in their bodies. They were excluded if they; reported ever having sought medical attention for a problem with their knees, reported known problems with their balance, or reported having experienced pain within the past three months in their ankles, knees, hips or back. Participant details are presented as supplementary material. Informed written consent was obtained from all individuals prior to testing and all procedures were approved by the regional ethics committee in Linköping, Sweden (Dnr 2014/439-31).
Participants took part in a single testing session of approximately 2 h in duration. Testing involved two validated tests of proprioception and a standardized test of balance, described in detail below. All tests were performed under three randomized orthosis conditions including; no orthosis (control), soft elastic orthosis (Selection Knee Minor, CAMP Scandinavia AB, Sweden) and a non-elastic jointed Orthosis (Elcross CAMP Scandinavia AB, Sweden) (see Figure 1). To investigate the relationship between pressure applied to the limb and proprioception, interface pressure measurements were recorded when participants were fitted with the soft elastic and non-elastic jointed orthoses.
(a) Selection knee minor, CAMP Scandinavia AB; (b) Elcross CAMP Scandinavia AB, Sweden (photos reproduced with permission of Camp Scandinavia AB).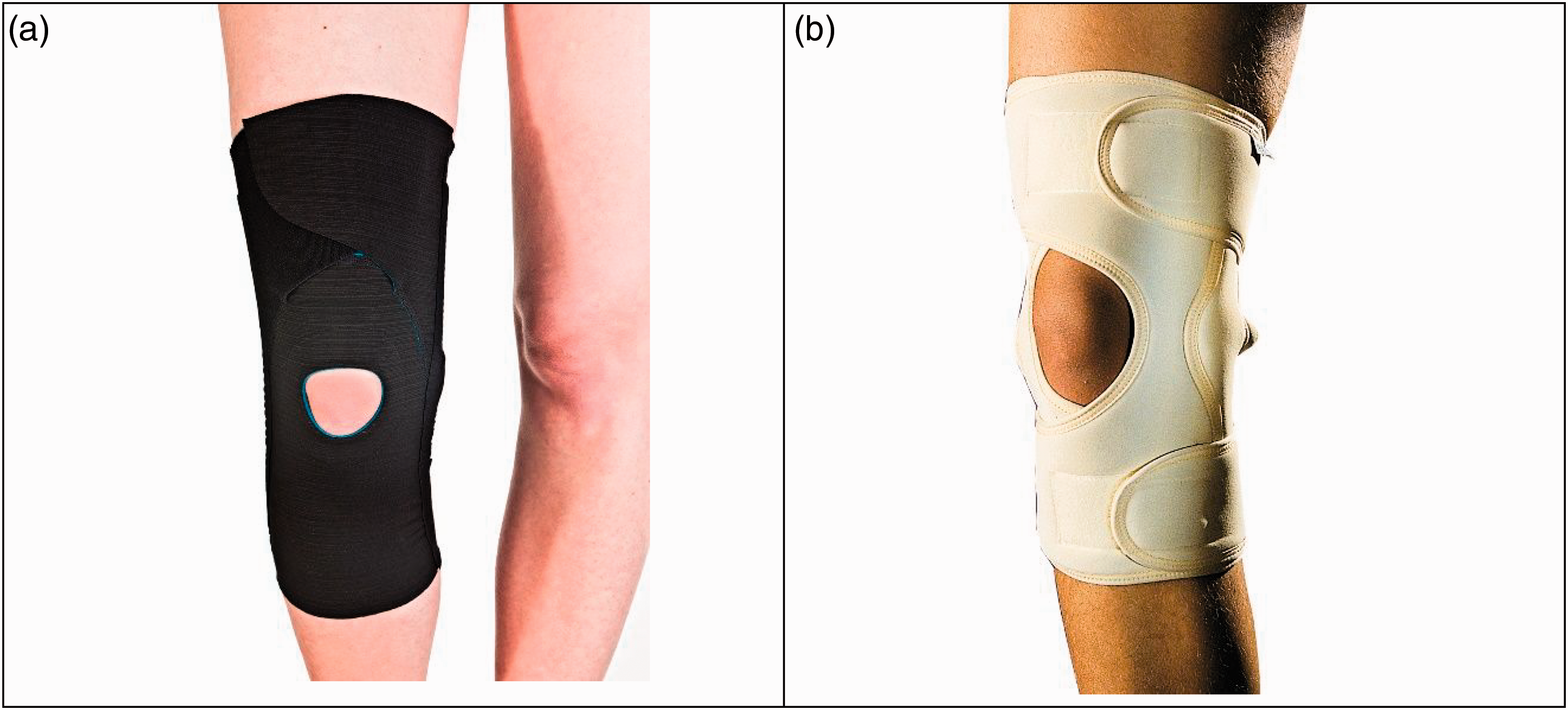
Testing equipment
Interface pressure was evaluated using a Pedar Pliance system (novel GmbH, Munich, Germany). This system has previously been demonstrated as a reliable tool for measurement of low interface pressures under garments used in the management of burns. 27 Data were captured at a frequency of 50 HZ using four capacitance pressure sensor arrays (novel GmbH, Munich, Germany). Each sensor had a sensing area of 40×40 mm and contained 16 sensors. The pressure range for these sensors is between 3 and 200 kPa. Sensor arrays were positioned under the orthoses, medially and laterally at the level of the knee joint (mid-joint line) and on the anterior surface of the distal thigh and anterior surface of the proximal tibia. Sensors were attached to the skin using double-sided tape and calibrated prior to applying the orthoses.
Proprioceptive tests were conducted using an isokinetic dynamometer (Isomed2000, D&R Ferstl GmbH). Raw voltage signals representing the angular position of the dynamometer and a pulse from a synced trigger device were collected using DASYlab software (Measurement Computing Corporation, USA) at 100 Hz. Raw signals were exported to Visual3D (C-Motion, Inc., Germantown, MD) where post-processing was conducted, including conversion from raw voltage to angular position and low-pass filtering using a zero phase-lag eighth-order Butterworth filter with a cut-off frequency of 4 Hz.
Testing protocol
Interface pressures
In test conditions involving application of an orthosis, pressure measurements at the skin-orthosis interface were conducted immediately after the appropriately sized orthosis was fitted by a certified orthotist and according to manufacturer instructions. Participants always wore the orthosis on the right leg. Pressure measurements were recorded during a 10 s period as the leg was passively held in full extension and then as the participant remained seated and moved their leg from full extension to full flexion during three repetitions. During remaining tests, the pressure sensors were disconnected from the Pliance system but not removed from under the orthosis. Mean pressures (kPa) and peak pressures (kPa) over all loaded sensors from all four sensor arrays (calculated with the frames and the sensors that were loaded), for the three repetitions, were extracted for analysis.
After pressure measurements were recorded, kinesthetic awareness and balance tests were conducted in a systematic order (JPS, TDPM and mSOT) with a 2 to 5-min pause between each of the tests. Kinesthetic awareness tests lasted approximately 15–20 min per condition, while the mSOT was approximately 6 min per condition. Participants were offered additional rest time, though none requested this.
Tests of kinesthetic awareness
Kinesthetic awareness was examined using two standardized tests; joint position sense (JPS) and threshold to detection of passive motion (TDPM). Reliability of each test has been reported.28–30 Both tests were performed with participants seated upright in the isokinetic dynamometer (ISOmed 2000, D&R GmbH, Germany) with their anatomical knee joint aligned with the mechanical joint of the dynamometer and their distal leg strapped to the limb support pad of the dynamometer arm. Throughout testing, subjects wore earmuffs and blackout glasses to suppress auditory and visual cues associated with movement of the dynamometer.
The JPS test began with participants positioned in 90° of knee flexion. Upon test initiation, the arm of the dynamometer actively extended the participants leg at an angular velocity of 10° per second and stopped at one of two randomly assigned reference angles; 50° and 75° from full extension. Olsson et al. 31 have indicated that reliability of JPS is maximized if test angles are maintained within 40–80° of knee flexion. The leg was held at the reference angle for a period of 5 s before returning at the same angular velocity to 90° of flexion. After a further 5 s, the leg was again actively extended, this time to full extension. During this final occasion, each participant was requested to indicate, using a handheld trigger, when they felt that their leg reached the original reference angle. Each reference angle was repeated three times in a randomized order. Variables that were exported for analysis were: mean absolute error between the reference angle and the angle when the trigger was pressed. Data were averaged for the three trials performed at each reference angle.
Detection of passive motion testing began by first moving the knee to one of two predetermined start angles; 50° or 70° from full extension. There is no consensus regarding appropriate target angle to use in this test so angles were selected to approximate those used in previous studies. After a period of time, between 1 and 10 s, movement was initiated, and the dynamometer arm began slowly moving the leg into either extension or flexion at an angular velocity of 1° per second. Participants were requested to press the handheld trigger at the first moment sensed that their leg was moving. Each start angle was repeated three times while moving the leg into flexion and three times while moving the leg into extension (12 trials in total). The order of testing was randomized for every participant. The angular difference between the start angle and the angle recorded at the point the participant pressed the trigger was extracted for analysis.
Modified sensory organisation test
The modified sensory organization test (mSOT) was conducted while participants stood upright on a Pro Balance Master (NeuroCom International Inc., Oregon, USA). This system incorporates a force plate that is capable of rotating about a single axis and has been described in previous work.32,33 When performing the mSOT, participants are requested to stand as still as possible with their hands by their sides for a period of 20 s. The test includes four sensory conditions which are each repeated three times. These include: (1) stable support surface with eyes open, (2) stable support surface with eyes closed, (3) unstable support surface with eyes open (achieved using a foam cushion and by allowing the force plate to freely to move about its pivot point) and (4) unstable support surface with eyes closed. Reliability of the mSOT has been established in previous work. 34 Data were averaged across the three trials within each sensory condition. A custom program was used to calculate the mean velocity of the centre of pressure (CoP) under each of the standing conditions. A detailed description of the equation used to calculate this variable is presented elsewhere. 33
Data analysis
Statistical analysis was performed using IBM SPSS statistics (version 21). Data were examined for violations of normality using the Shapiro–Wilk test. As normality was violated (p < 0.05), Friedman’s analysis of variance was used to compare means across orthosis conditions. When significant differences were observed, post hoc comparisons were performed using the Wilcoxon signed-rank test. Spearman's rank correlation coefficient was used to examine the relationship between proprioception and balance with proprioception data from all three test conditions correlated again velocity data extracted from the mSOT. The critical alpha level was set at 0.05 for all analyses.
Results
Interface pressure
Median values and confidence intervals (CI) for pressure recorded under each orthosis, soft elastic orthosis (elastic) and non-elastic jointed (jointed) in the extended position (left side of table) and during the flexion/extension movement (right side of table).

Note: p-values indicate results of Wilcoxon signed-rank test.
All units in kPa.
Proprioception
Median absolute error and confidence interval (CI) for joint position sense data.

Note: p-values indicate results of Friedman’s ANOVA.
All units in degrees (°).
Median error and confidence intervals (CI) for threshold to detection of passive motion.

Note: p-values indicate results of Friedman’s ANOVA.
*Statistically significant differences (p < 0.05). All units in degrees (°).
Post hoc analysis revealed differences between the two variables marked with ‘a’.
Post hoc analysis revealed differences between the two variables marked with ‘b’.
mSOT
Median scores and confidence intervals (CI) for balance variables.
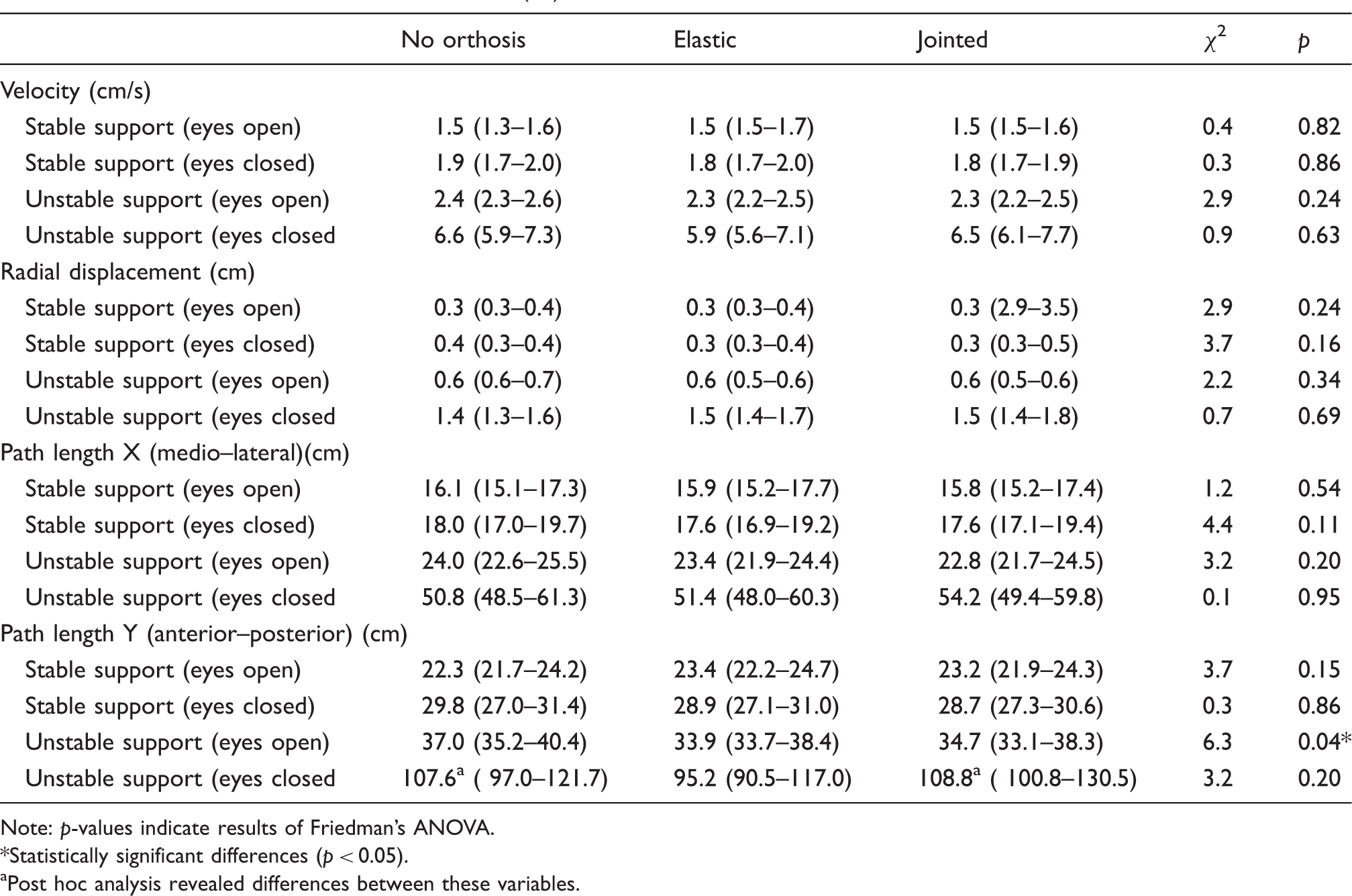
Note: p-values indicate results of Friedman’s ANOVA.
Statistically significant differences (p < 0.05).
Post hoc analysis revealed differences between these variables.
Correlation analyses
Correlation between measures of proprioceptive acuity and balance (velocity of the CoP).

Statistically significant differences (p < 0.05).
Discussion
Results of the present study were found to be contrary to our hypothesis, which proposed that application of an orthosis would be associated with heightened kinesthetic awareness and that this in turn would correlate with improved balance performance. In the sample of healthy adults recruited for this study, increased pressure was not found to be associated with heightened kinesthetic awareness. In fact, for the total data set and the non-elastic jointed orthosis condition, which applied the greatest amount of pressure, results were significantly poorer in the detection of passive motion test. No significant difference was observed between the control condition or either of the orthosis conditions in tests of joint position sense. The only balance variables were affected by orthoses was path-length of the CoP in the anterior/posterior direction. There was a weak positive correlation between results on the detection of passive motion test (start angle 50°) and velocity of the centre of pressure but no significant associations were observed between joint position sense data and velocity of the centre of pressure. The most interesting finding related to this study is an indication that excessive pressure applied around the knee joint may compromise kinesthetic awareness.
There is currently little understanding of the underlying mechanisms by which orthotic devices may contribute to proprioception. One proposed mechanism is the compression they provide, 15 which presumably differs between specific orthosis designs. While several authors have investigated the effect of altering orthosis design on proprioception,13,16 the present study is the first to quantify relative pressure applied by different orthotic devices and to investigate potential associations between pressure, proprioception and balance. In this study, pressure was reported by extracting the maximum pressure recorded during a testing sequence and by calculating the median pressure for each sequence.
Joint position sense is a commonly accepted test of proprioception which evaluates a subjects’ ability to reproduce previously established joint angles. Our study has not demonstrated any significant difference in joint position sense when comparing either of the two orthosis conditions to a no orthosis condition. Results are consistent with Hosp et al. 35 and Torres et al. 36 who compared joint position sense in healthy women wearing kinesiology tape to a no-tape condition. In contrast, Herrington et al. 15 reported that application of an elastic sleeve in a sample of 12 healthy individuals led to a 23% improvement in joint position sense. In a group of 64 healthy individuals, Van Tiggelen et al. 37 demonstrated that a patellofemoral orthosis also significantly improved of joint position sense. Van Tigglen et al. also demonstrated that a deficit in proprioception induced via fatigue can be eliminated with the use of an elastic knee orthosis. Previous studies demonstrating positive results for orthoses in relation to joint position sense appear to use similar protocols to the present study. Target angles utilized by Herrington et al. 15 were not reported, while Van Tiggelen et al. 37 utilized one target angle of 45°. Our study utilized two target angles (50 and 75°). Herrington et al. utilized delays and a movement velocity that were identical to the present study, while Van Tiggelen et al. had a slightly longer delay when presenting the target angle.
Boerboom et al. 29 have demonstrated that the detection of passive motion test is more sensitive in detecting small changes in proprioception as compared to tests of joint position sense and, in our study, it was this test that demonstrated a significant difference between the jointed orthosis and no orthosis conditions. The jointed orthosis condition exhibited poorer results when analysing combined data from all detection of passive motion tests and when the start position for the test was set at 70° moving into flexion. These results are in contrast with previous work which has reported either no effect,16,17 or a positive effect36,38 in detection of passive motion with the application of an orthotic device or tape.
It is likely that the deterioration in detection of passive motion observed in the present study was a result of orthosis design and the excessive pressure applied by the jointed orthosis. Our results suggest that application of too much pressure by an orthotic device may compromise proprioception rather than facilitate it. It is important to recognize, however, that the pressure measurements in the present study were quite rudimentary and data presented represent the maximum and median pressure over the testing period. The methods applied in this study did not make it possible to accurately identify the flexion angle of the knee for specific frames of data in the pressure measurement files. Given the observed results, it seems important to further investigate the association between pressure applied to the knee and proprioception by synchronizing pressure data with kinematic data. Bottoni et al. 16 reported no difference in detection of passive motion in 20 healthy individuals fitted with 1/ an elastic jointed orthosis and 2/ a knee sleeve. In this study, two starting angles of 60° and 30° were used in detection of passive motion tests. These starting angles are not too dissimilar to the starting angles of 70° and 50° used in the present study. While pressure under the orthoses was not reported by Bottoni et al., both orthosis designs incorporated elastic materials which would be comparable to the elastic orthosis used in the present study. Although no significant results were reported, it is interesting to note that the greatest error was observed for the jointed orthosis at a starting angle of 60°.
The relative effects of orthoses on balance in the present study demonstrated only one significant difference which was related to path-length of the CoP in the y plane, with the no-orthosis condition reporting greater values. No differences were observed in any of the other variables (velocity, radial displacement and path-length in the x plane). Results can be contrasted to Birmingham et al. 23 and Kuster et al., 7 who demonstrated a significant reduction in total path-length of the centre of pressure when wearing an orthosis. Both these studies included individuals who had undergone ACL reconstructions, while subjects in the present study were healthy individuals with no known condition that may affect balance. It is likely that individuals with pathological conditions affecting balance would derive more benefit from the application of a knee orthosis.
The relationship between proprioception and functional performance is of interest in sports injury prevention, sporting performance, falls prevention and rehabilitation in general. Proprioceptive feedback from the ankle has been well established as a key mechanism in balance control. 39 The contribution of proprioceptive feedback from the knee on balance appears to be less well established. Our results did not demonstrate a clear relationship between proprioceptive feedback from the knee and balance outcomes. Only a few other studies involving knee orthoses or taping have attempted to investigate the relationship between proprioceptive feedback from the knee and functional outcomes. Risberg et al. 17 presented moderate to low correlations between detection of passive motions tests, with and without knee orthoses, and two knee function outcome measures. Birmingham et al. 23 demonstrated that application of a knee orthosis significantly improved balance by reducing path-length of the centre of pressure and anteroposterior variation of CoP but the authors did not find a significant relationship between proprioception and balance in individuals who had undergone an ACL reconstruction.
Use of healthy subjects with inherently good proprioception is an obvious limitation of the present study and limits clinical generalisation of results. Given that orthoses are sometimes prescribed as a prophylactic measure, together with the fact that previous research has reported significant effects of orthoses and taping on kinesthetic awareness in healthy subjects, we do consider this to be a relevant group to investigate. A further limitation related to this paper is the limited sample size which may have reduced the power of the study and increases the likelihood of type-II error.
The time between application of the orthosis and testing of proprioception was less than 10 min in the present study and may be a limitation in the study design as participants had little time to familiarize themselves with the orthosis. Little is known of the effects that orthosis accommodation times may have on kinesthetic awareness. However, Torres et al. 36 did demonstrated that immediate benefits of kinesiology tape on knee proprioception remained the same after 24 h, suggesting that increasing the accommodation time would not have affected our results.
Pressure measurement made in this study was rather rudimentary. While they give an indication of relative pressure applied by each orthosis, lack of data related to knee kinematics or torque required to move the joint for each orthosis condition does not allow us to analyse how the pressure profile of each orthosis design may differ as the knee moves into flexion. This would be recommended in future studies. Furthermore, pressure measurements were taken prior to tests of proprioception and not simultaneously. While the orthosis was not removed between pressure measurements and tests of proprioception, we cannot guarantee that the orthosis did not move or loosen between the tests.
A further limitation is the ecological validity of the tests used which have been called into question by several authors. 40 These authors argue that both detection of passive motion and joint position sense are far removed from normal daily activities. The benefit of both methods however is that proprioceptive information from the foot is minimised as the ankle/foot complex is unloaded. 14
Results from the present study indicate that orthosis design, including choice of materials is likely to influence proprioceptive feedback and should be considered by health professionals involved in the prescription of devices. Of importance is the fact that an orthosis constructed from a stiffer material, applying greater pressure to the knee, may have a negative effect on proprioception. While results from our study suggest that the relative effects are minimal and the clinical effect in healthy individuals is unknown, it will be important to investigate if the negative effects are exaggerated in individuals who have reduced proprioception due to a pathological condition. This would provide clinicians with an additional patient-indicated criterion for orthosis selection which reduces any potential risk for further injury as a result of orthosis design.
Conclusions
Orthoses design was found to significantly affect kinesthetic awareness, as measured through detection of passive motion. Interestingly, the orthoses design which applied most pressure to the limb had a negative effect on proprioception. None of the orthoses tested in this study had effect on balance performance.
Supplemental Material
Supplemental material for Effects of knee orthoses on kinesthetic awareness and balance in healthy individuals
Supplemental Material for Effects of knee orthoses on kinesthetic awareness and balance in healthy individuals by Nerrolyn Ramstrand, Terje Gjøvaag, Inger Marie Starholm and David F Rusaw in Journal of Rehabilitation and Assistive Technologies Engineering
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by a travel grant from Erasmus+ (staff mobility in higher education).
Guarantor
NR.
Contributorship
All authors were involved in development of the protocol as well as data collection and analysis. NR wrote the first draft of the manuscript and all authors reviewed and edited the manuscript.
Acknowledgments
The authors would like to thank all individuals who participated in this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.