
Abstract
Gait retraining in people with musculoskeletal and/or neurological impairments requires sustained dedicated efforts by the patient and the rehabilitation therapist. Various technical approaches have been proposed and utilized to improve the effectiveness of training interventions. Among the most promising approaches is the provision of real-time feedback information to the patient, which has been used with success on treadmill-based interventions in the past. We are describing a mobile visual feedback system that is intended to work in the user’s everyday-life environment. The data are captured by a small mobile load cell, processed in a wearable computer, and displayed to the user via smart-glasses. Preliminary testing of the initially selected feedback variable stance/step ratio (i.e., the duration of a step’s stance phase in relation to the overall step’s duration) confirmed that data quality is sufficient for purposes of generating feedback information and that the chosen variable is responsive to changes in gait symmetry. The presented work may inform future studies and developments on the topic of mobile visual feedback for gait rehabilitation.
Introduction
Gait deviations are frequently observed as a symptom in patients with musculoskeletal and/or neurological impairments. They are very prevalent among people with lower limb loss, where they can be mostly attributed to the inevitable differences between sound and prosthetic leg. For users of lower limb prostheses, gait deviations can be the cause and the symptom of gait instability, falling and fear of falling, overuse injuries, and impaired mobility.
However, gait deviations and the associated acute and chronic medical problems are not limited to individuals with lower limb loss, and gait retraining has the potential to benefit a great number of patients beyond this population. Due to the range of possible underlying pathological conditions1,2 and the wide spectrum of individual coping strategies, gait deviations manifest themselves in a variety of forms. These include fairly minor bilateral asymmetries of step pattern or arm swing, as well as severe favoring of one leg over the other with associated compensatory trunk and arm motions.
It has been (inconclusively) debated which level of asymmetry constitutes a pathological gait deviation,
3
since it was found that even healthy able-bodied people present gait asymmetries either because it is functional to utilize legs differently or because of laterality (limb dominance). Accordingly, the prevalence of gait deviations can only be roughly estimated based on the known prevalence of some underlying conditions. So it is known that every year about 795,000 Americans suffer a stroke,
4
1.4 million are diagnosed with traumatic brain injury,
5
and 185,000 undergo major limb amputation. A study from 2007
6
estimated that among US adults, nearly 27 million have clinical osteoarthritis …, 711,000 have polymyalgia rheumatica, 228,000 have giant cell arteritis, up to 3.0 million have had self-reported gout in the past year …, 5.0 million have fibromyalgia …, [and] 59 million have had low back pain in the past 3 months
Untreated, gait dysfunction can become chronic, even after the underlying pathology has been addressed. Physical therapy for gait retraining is therefore commonly prescribed to patients recovering from stroke, limb amputation, or other pertinent conditions. Such training typically comprises, in addition to strengthening and range-of-motion exercises, a number of therapy sessions. These sessions are typically spaced out over several weeks in which the therapist observes the patient’s gait and provides corrective feedback. While generally effective, this approach is very time- and personnel-intensive, which often necessitates a limitation on the duration of such provided training. After the cessation of training sessions, and even in between training sessions, patients are at risk of reverting to their abnormal gait pattern, especially in cases where the treated gait deviation has manifested itself over long periods of time already. To mitigate this risk, patients may be advised to continue practicing in front of a mirror which provides a simple form of visual feedback.
More sophisticated approaches that have been proposed include augmented sensory feedback, which has been reported to improve dysfunctional lower extremity impairments and related gait patterns including in those with lower limb loss 11 : The patient walks on an instrumented treadmill, while stationary gait analysis equipment generates pertinent gait data that are displayed to the patient via a computer screen in real time. A common criticism of these previous studies is based on the associated expense and tightly controlled laboratory conditions. These circumstances may limit translatability of the approach to realistic clinical environments, as the required equipment (instrumented split-belt treadmills), gait analysis personnel, and time are often unavailable in clinical settings.
More recently, mobile data collection and feedback systems have been utilized to overcome some of these shortcomings. One such approach is based on an array of wearable accelerometer sensors, attached to trunk, legs, and arms of the user, a processing unit, and an in-ear speaker that provides standardized verbal feedback corresponding to the gait deviation that is detected by the sensors. 12 Notable limitations of providing feedback in that manner are that the voice commands may be perceived as interfering with regular communication, and—importantly—that the specificity of the commands is not conducive to effective motor learning. By obeying commands such as “increase right step length!”, “swing arms!”, or “tighten your hip muscles!”, the user focuses on the internal mechanisms of proper gait. It has been shown that providing an external instead of internal focus of attention yields better motor learning success.13,14
Overall goal of our research is to design a system that provides real-time mobile visual feedback (RTMVF) for gait training. The feasibility of such a system is currently being investigated in a cohort of people with lower limb loss, a population that was selected because use of limb prostheses is often associated with gait deviations and because the mechanical limb provides an ideal platform for the necessary sensor equipment. Even though people with limb loss make up only part of the overall population with gait deviations, they offer unique opportunities to test and refine the technology before it will subsequently be applied more generally. We describe here the development of the system components, the selection of meaningful feedback variables from the available sensor output, and the initial validation of the measured and processed gait data.
Methods
The RTMVF system was developed utilizing commercially available and/or previously validated componentry (Figure 1). Gait data source is a prosthesis-integrated load cell (i-Pecs, RCT Electronics, Dexter, MI) capable of measuring precisely kinetic gait variables in lower limb prostheses. The device is semi-permanently installed as part of the load-bearing structure of the limb prosthesis connecting to the rest of the device using standard adapters. Ground reaction forces and moments of force data can be collected up to 850 Hz and transferred wirelessly or by cable connection to a laptop computer for further processing. In order to provide visual feedback to the patient, a wearable head-up display (M300, Vuzix, West Henrietta, NY) was used. These “smart glasses” contain, positioned at the fringe of the user’s normal field of view, a small-sized display, the contents of which are retrieved from the computer via Wi-Fi or Bluetooth connection.15,16 The display has a resolution that is comparable with small computer screens, yet its position and intended purpose in our context advises against the conveyance of very complex visual information.
Mobile gait feedback system in use. PC: personal computer.
Connectivity between the different components is currently realized using cable connection between load cell and laptop computer, and Bluetooth to the smart glasses. In this configuration, the lightweight computer is being carried in a pouch on a waist belt by the user.
Feasibility of the system was evaluated using the feedback variable “Stance/step time ratio,” (i.e., the duration of a step’s stance phase (From initial ground contact to toe-off) in relation to the overall step’s duration measured from one initial ground contact to the next initial ground contact on the same side). This parameter correlates with some typical gait deviations in lower limb prosthesis users, and it lends itself to easy capturing by lower cost, prosthesis-independent sensor equipment for potential translation into the clinic and/or adaptation for different patient populations. Stance and swing components of step cycles were derived by an algorithm that analyzed various components of the axial force curve (the sensor’s Fz is roughly equivalent to vertical ground reaction force in an external coordinate system 17 ) to determine the appropriate crossings of a 15 N and 100 N threshold (Visual Studio Community 2015). For examining the sensor data graphically and quantitatively, different strategies were tested to harden the algorithm to outliers and measuring artefacts. 18 Timing parameters were established to help the algorithm detect transition steps and turns as non-representative steps for gait analysis and feedback purposes.
A target window of stance/step ratio was established between 0.59 and 0.63, resulting in three discrete output states: Too short stance phase (below 59% of step cycle), desirable stance phase (59%–63%), and too long stance phase (above 63%). The three states were represented by different feedback colors, displaying a red (for too short stance phase), green (desirable stance phase), or yellow (too long stance phase) screen to the user. The most accurate calculation of stance phase duration with respect to the total step cycle requires the entire step cycle in question to be timed. This makes the feedback information available only after a given analyzed step is completed. Accounting for this inevitable latency, the validity of the system in generating feedback variables was investigated in a small sample of steps.
Inclusion criteria for this test were use of a trans-tibial prosthesis for ambulation, absence of acute or chronic health conditions that would affect prosthesis use, and ability to walk without aids for at least 30 min. Demographic data and mobility score (PLUS-M 19 ) were recorded. The test participant was equipped with the RTMVF system and a waist-worn “mobile gait lab” (G-Walk, BTS Engineering, Milan, ITA) and was asked to traverse in self-selected walking speeds repeatedly across a 30 -m level walkway. Step phase durations were extracted from the G-Walk data to serve as the validation standard for the respective variables computed from the prosthesis sensor data by our algorithm. Gait symmetry index, a proprietary variable output by the G-Walk software, was recorded as well and correlated to the i-Pecs derived stance/step ratio in order to investigate its appropriateness as feedback variable for gait training. The variable is a composite index that is based on acceleration and gyroscope data through the step cycle. An index of 100 signifies perfect symmetry between the left and the right step with respect to ground contact forces, trunk tilt, and temporal parameters. Bivariate correlation analysis was conducted using IBM SPSS Statistics (Version 24).
Results
The participant was a 61-year-old female, weighing 58.5 kg and 1.49 m tall, who had been using trans-tibial prostheses for 12 years and had a PLUS-M score at the 79th percentile.
A total of 67 steps were analyzed. Correlation between RTMVF step ratio data and reference data was strong, with a Pearson correlation coefficient of R = 0.813 (p < 0.001).
Correlation between variables stance/step ratio and overall gait symmetry index (Figure 2) across eight data collection sessions was strong as well (R = 0.735), indicating that the feedback variable is a good proxy for the primary outcome of interest.
Correlation between stance/step ratio (the feedback variable) and overall gait symmetry. RTMF: real-time mobile visual feedback.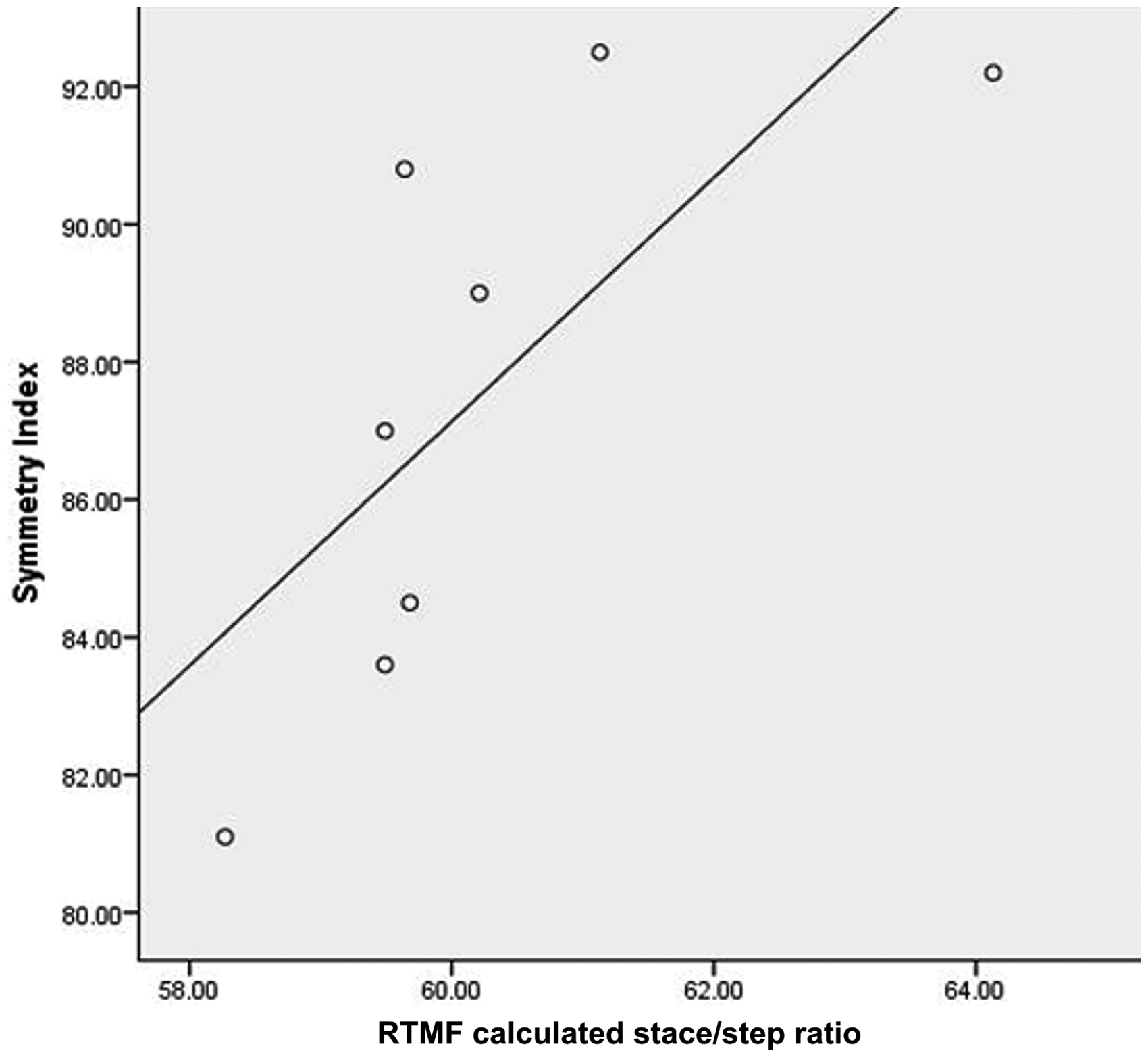
Latency of feedback was less than 1 s and was not perceived as problematic by the test subject. The test suggests that a patient can be fitted with the system in about 30 min, most of which time is required for the installation of the load cell into the prosthesis structure.
Discussion
Findings suggest that our system measures step cycle components with sufficient validity. None of the analyzed steps was classified improperly, and deviations between the two utilized data capture systems did on average not exceed 66 ms or 10.2%, a discrepancy that can be deemed acceptable and may be attributable to the difference in generating kinetics data based on accelerometry (G-Walk) and strain gages (i-Pecs). This leaves the slight delay in displaying the feedback information that is owed to the processing of load cell gait data, as potentially the most relevant difference to treadmill-based feedback systems for gait training. Whether the mobile feedback may still be considered “quasi real-time,” and may thus allow the assumption that the function mechanism of the tested methodology is in principle comparable to more conventional approaches, should be tested in a larger scale study.
Our pilot data collection illustrated the advantages of providing real-time visual feedback with a mobile system, in terms of efficiency, clinical applicability, and representativeness of data. Once the short preparations, involving attachment and calibration of the equipment, were concluded, collecting gait data on a substantial number of steps required not more time than the participant spent taking those steps. One person was able to administer the test session, as the patient was able to walk safely and in her regular fashion without being notably encumbered by the wearable equipment. The environment in which the training and data collection can occur is very realistic, as the system can be used on most any indoor and outdoor walking surface, including slopes, stairs, and uneven terrains. Even though only one simple variable was extracted and analyzed for the current study, more of the sensor’s raw data (3-axial forces and moments) may prospectively be harvested to refine the detection of gait deviations and to inform better feedback displayed to the patient. Previously reported findings 11 suggest, for instance, that providing feedback on the peak vertical ground reaction force can improve stance symmetry.
Some of the limitations of our approach have been addressed in earlier development stages. We initially considered a number of commercially available wearable head-up displays, including the Google glass system (Google, Mountain View, CA) and the Recon jet (recon instruments, Vancouver, BC), before implementing Vuzix M100 and M300 smart glasses (Vuzix, West Henrietta, NY) in our prototype. Battery life of the head-up display is currently the limiting factor, along with transmission lag time, though without affecting the commonly allocated 1-h time frame for gait therapy sessions.
Our single subject pilot study did not allow investigating which modifications to the algorithm may be needed on an individual basis. It may be assumed that other users require slightly different feedback information, depending on the severity of their gait deviation and their ability to make the prescribed corrections. Such users may, for instance, benefit from adjustments to the size and location of the “target window” for the proper stance/step ratio.
Findings of the current study are anticipated to provide the groundwork for subsequent research and development with the goal of effectively supplementing traditional therapist-based gait retraining. By expanding patients’ exposure to gait therapy interventions beyond the limited sessions with their therapist, training effects should onset swifter and should be better sustainable. As habitual gait deviations can cause further secondary orthopedic issues in the musculoskeletal system and as learning theories, though not previously widely implemented in this rehabilitation population, suggest “dependency” on feedback can become a deterrent to motor learning, the optimal frequency and duration of this type of treatment should be further investigated.
In conclusion, a mobile gait analysis and feedback system hold promise for enhanced gait retraining approaches in people with lower limb loss.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by a Milbank Grant from the Foundation for Physical Medicine and Rehabilitation and and a PInCh (Pitt Innotion Challenge) award from the University of Pittsburgh.
Guarantor
GF.
Contributorship
Both authors researched literature, conceived the study, and developed the protocol. KK lead system development and testing, including IRB approval application, subject recruitment, and data collection/analysis. GF wrote the first draft of the manuscript. Both authors reviewed and edited the manuscript and approved the final version of the manuscript.