
Abstract
Affordable technology-assisted stroke rehabilitation approaches can improve access to rehabilitation for low-resource environments characterized by the limited availability of rehabilitation experts and poor rehabilitation infrastructure. This paper describes the evolution of an approach to the implementation of affordable, technology-assisted stroke rehabilitation which relies on low-cost mechatronic/robot devices integrated with off-the-shelf or custom games. Important lessons learned from the evolution and use of Theradrive in the USA and in Mexico are briefly described. We present how a stronger and more compact version of the Theradrive is leveraged in the development of a new low-cost, all-in-one robot gym with four exercise stations for upper and lower limb therapy called Rehab Community-based Affordable Robot Exercise System (Rehab C.A.R.E.S). Three of the exercise stations are designed to accommodate versions of the 1 DOF haptic Theradrive with different custom handles or off-the-shelf commercial motion machine. The fourth station leverages a unique configuration of Wii-boards. Overall, results from testing versions of Theradrive in USA and Mexico in a robot gym suggest that the resulting presentation of the Rehab C.A.R.E.S robot gym can be deployed as an affordable computer/robot-assisted solution for stroke rehabilitation in developed and developing countries.
Keywords
Introduction
Non-communicable diseases, especially cardiovascular diseases, are the leading cause of death and disability in the world. An increase in their prevalence often leads to higher incidences of stroke and consequently, an increase in the number of persons living with permanent disability due to stroke.1,2 Stroke is the leading cause of disability worldwide. Over 6.8 million adults live in the USA with disabilities due to a stroke, and by 2030, this number will grow by 4 million.3,4 Seventy-five percent of adults recovering from stroke have residual impairment in their limbs, with only about 25% achieving recovery with minor impairments, and only 10% achieving full recovery.5–7 Greater than 30% are unable to walk without some assistance and 26% remain dependent in activities of daily living. 8
The issues influencing rehabilitation outcomes are complex; some examples of these issues are poverty, increase in health costs, short length of stays, insurance limitations, and physical constraints on rehabilitation services (e.g. time).3,6 In low- and middle-income countries (LMIC), rehabilitation outcomes are worse since a disproportionate number of the population is without easy access to rehabilitation technologies, services and skilled clinicians.1,3,9,10 Improved stroke rehabilitation approaches can maximize the functional independence of stroke survivors discharged after inpatient and outpatient services and improve access to rehabilitation for low-resource environments in USA or other LMICs.
Our long-term goal is to develop and use affordable robot technologies to improve access to rehabilitation and ultimately improve the health and function of persons with persistent motor deficits due to a stroke in the USA and worldwide, especially in LMICs where more than 80% of those living with a stroke reside. Specifically, we desire to target stroke survivors who are diagnosed with hemiparesis, are living with severe to moderate motor function impairment, and are without easy access to rehabilitation. Research efforts are needed to develop cost-effective robot devices that can do the above and function in harsher environments characterized by extreme economic hardship (per country), intermittent energy and limited expert supervisors.
Our main approach to delivering rehabilitation has always promoted robot/computer-assisted motivating rehabilitation systems for stroke therapy. 31 We have proposed the use and development of mechatronic devices alone or within a suite of devices for upper limb stroke therapy. This paper summarizes lessons learned regarding the delivery of affordable and accessible stroke therapy in HICs and LMICs. We illustrate these lessons via the use of Theradrive, alone (TD-1),28–32 its development into a 1DOF Haptic Robot called Haptic Theradrive,36–38 a therapy gym in Mexico (TD-2),33–35 where Theradrive was one of six devices aimed at improving motor function after stroke. The paper then presents how a stronger and more compact version of the Theradrive is re-designed and leveraged in the development of a new low-cost, all-in-one robot gym called Rehab Community-based Affordable Robot Exercise System (Rehab C.A.R.E.S) with four exercise stations for upper and lower limb therapy. The prototype of the system is described along with strategies for control and new results from testing on exercise station 2. Finally, we discuss implications for deploying such a system in LMICs.
Background (lessons from delivery of affordable stroke therapy in USA and Mexico)
After stroke, residual motor function is often categorized into low, moderate and high motor function. For the upper limb, this categorization is typically influenced heavily by motor impairment scores derived from the upper extremity Fugl-Meyer (FM) Motor Assessment Scale. 41 A major design goal for robot therapy environments is to be effective and support rehabilitation with stroke survivors at all functioning levels. Design efforts, especially if the device is expected to be used in under-supervised environments such as in home and community rehabilitation settings, must consider appropriate devices, force feedback and controllers to maintain motor training, motivation and compliance. We illustrate three major insights gained using three versions of the Theradrive (TD-1, 31 TD-2, 50 and TD-3 37 ). Figure 1 shows the three versions of the Theradrive.
Affordable technology-assisted therapy using only commercial devices and games excludes severe strokes (TD-1)
Studies have supported the use of gaming devices such as the XBOX, Wii, or Nintendo GameCube as potential therapeutic devices that have demonstrated effectiveness in assessing and treating impairments in inpatient rehabilitation and home settings.20–22 Affordable therapy can be realized through the use of off-the-shelf force-feedback systems and using commercial games, but this method is not without drawbacks and limitations. For example, the original Theradrive (TD-1) was developed as an affordable stroke therapy system which used commercial force-feedback wheels and joysticks mounted on novel height adjustable frames to provide a therapy environment for the upper limb.28–32 Commercial gaming software as well as customized software called Unitherapy 39 enabled subjects to complete therapy tasks in several training modes, including unilateral steering in the front or on the side and bilateral steering utilizing the two steering wheels. 30 Therapy tasks consisted of subjects playing off-the-shelf driving games such as ‘Need for Speed’ or completing custom tracking tasks such as circle tracking or complex sine wave tracking. As subjects completed tracking tasks using the wheel, they experienced spring-like assistive or resistive forces on the wheel, where the magnitude of the force-feedback was proportional to the tracking error and the proportional gain was pre-adjusted according to a subject’s tracking ability.
To test the benefit of therapy with the commercial devices and games, 10 subjects were randomized to a group playing off-the-shelf games (fun tracking) and a group completing custom rote tracking tasks; each group completed 24, 1 h therapy sessions. 29 The group that played commercial games tended to performed better than the group that completed simple point-to-point tracking exercises, suggesting that game-based therapy is effective. This version of TD-1 proved most suited for subjects with moderate-to-high function. The low torque output of the 1-DOF commercial wheels and the non-adaptive force-feedback algorithm applied during therapy made it difficult for stroke subjects with low motor function due to severe hemiparesis to experience a great benefit. The wheels were unable to apply sufficient assistive forces for these users.
Affordable therapy delivered using multiple rehabilitation technologies for circuit training leverages limited therapists in LMICs (TD-2)
Stroke survivors in Mexico experience similar issues as those in USA and other high-income countries (HIC). They are also discharged from rehabilitation with residual disabilities and in need of access to services in the community. Unfortunately, in developing countries such as Mexico, a disproportionate number of the population is without easy access to rehabilitation services.9,40 Access is limited by: (1) economics: rehabilitation services and associated technologies may not exist outside of major urban areas and many times are not affordable by low-income patients; (2) training: skilled therapists and physiatrists are often not available in large numbers inside or outside of cities; and (3) technology: access to state of art rehabilitation technologies may be limited and gaining access may be too costly.
It was thought that a low-cost system such as Theradrive (TD-1) and the imagined use of it in the Computer/Robot-Assisted Motivating Rehabilitation Suite could be a potential solution to provide affordable rehabilitation in Mexico. The original Theradrive was subsequently recreated in Mexico and called the Mexican Theradrive (TD-2).33–35 The Mexican Theradrive was deployed in a robot gym.33,35 The robot gym offered therapy based on circuit training where patients could rotate to six stations under a clinician’s supervision; each station used a custom or commercially built robot/mechatronic rehabilitation technology. On four machines, subjects did activities of daily living (ADLs), cycling, or game-based visuomotor tracking tasks using the upper limb and on two machines, cycling and gait training using the lower limb. The robot gym enabled therapy to be provided for the upper and lower extremities of stroke patients in an environment where limited supervision is available. The multi-piece robot gym in Mexico occupied a large room and consisted of six rehabilitation technologies developed by a variety of manufacturers. The total cost of the multi-piece system was approximately 29,000 USD. 50 With the help of the six-station gym, a therapist would be able to treat 6 patients per hour and 42 patients per 7-h shift, resulting in a 3-fold increase in therapist productivity given the average treatment of 10 to 14 patients in a 7-h workday.
A pilot study compared the robot gym to standard therapy administered at the public rehabilitation healthcare center located in Chihuahua, Mexico. Patients in the standard therapy group experienced one-on-one manual therapy. Patients in the robot therapy group rotated through the six stations with an engineer and a therapist as supervisors who assist with set-up and use of the devices. 35 The robot gym needed only one clinician and one technician to support six patients during therapy together in a social environment. All patients had 24, 1-h therapy sessions for the upper and/or lower limb. Both the control group (CG) and robot group (RG) experienced a significant change in the FM motor scores for upper and lower limbs and the RG perceived the therapy received as more valuable and engaging. 50
This pilot study demonstrated that circuit training in the robot/technology gym was effective and was just as good as the control group. These results are supported by the literature. Buschfort et al. 19 showed that a suite of four simple robotic devices (from Reha-STIM) can provide effective seated ‘hands on’ therapy to acute and sub-acute patients (Arm Studio) inside the Charite’ Rehabilitation Hospital in Berlin, Germany. Arm Studio can deliver effective therapy to patients under the supervision of a single therapist. These efforts support the fact that simple rehabilitation robotics can be leveraged to improve rehabilitation outcomes11–13; however, most approaches are still not cost wise or feasible for LMICs.
Affordable therapy using 1 DOF haptic robots and games includes severe strokes (TD-3)
Lower-cost robot systems are being proposed for home and community rehabilitation settings such as Reha-Stim line of devices,23,24 TyroMotion’s Pablo®, 25 Hand Mentor Pro™ from Kinetic Muscle, Inc., 26 and Haptic Knob 27 among others. These systems are making inroads, but are still relatively expensive, use custom-games, and are not always strong enough for the most severely impaired stroke survivor.
The most severely impaired stroke survivors typically have arm impairments either due to flaccid arm muscles in which case they require maximum end-effector forces to move their limb or due to abnormal coupling of elbow and shoulder muscles in which case they generate large off-axis forces on the robot. The torque output of many off-the-shelf commercial force-feedback gaming wheels is low (e.g. 1.45 Nm for force-feedback wheels) and is unable to apply sufficient forces to support the impaired arm of severe strokes in either case.
The Haptic Theradrive was developed to overcome this limitation. The Haptic Theradrive with a custom crank arm is capable of applying torques stronger than the commercial force-feedback wheel (45 Nm versus 1.5 Nm)
37
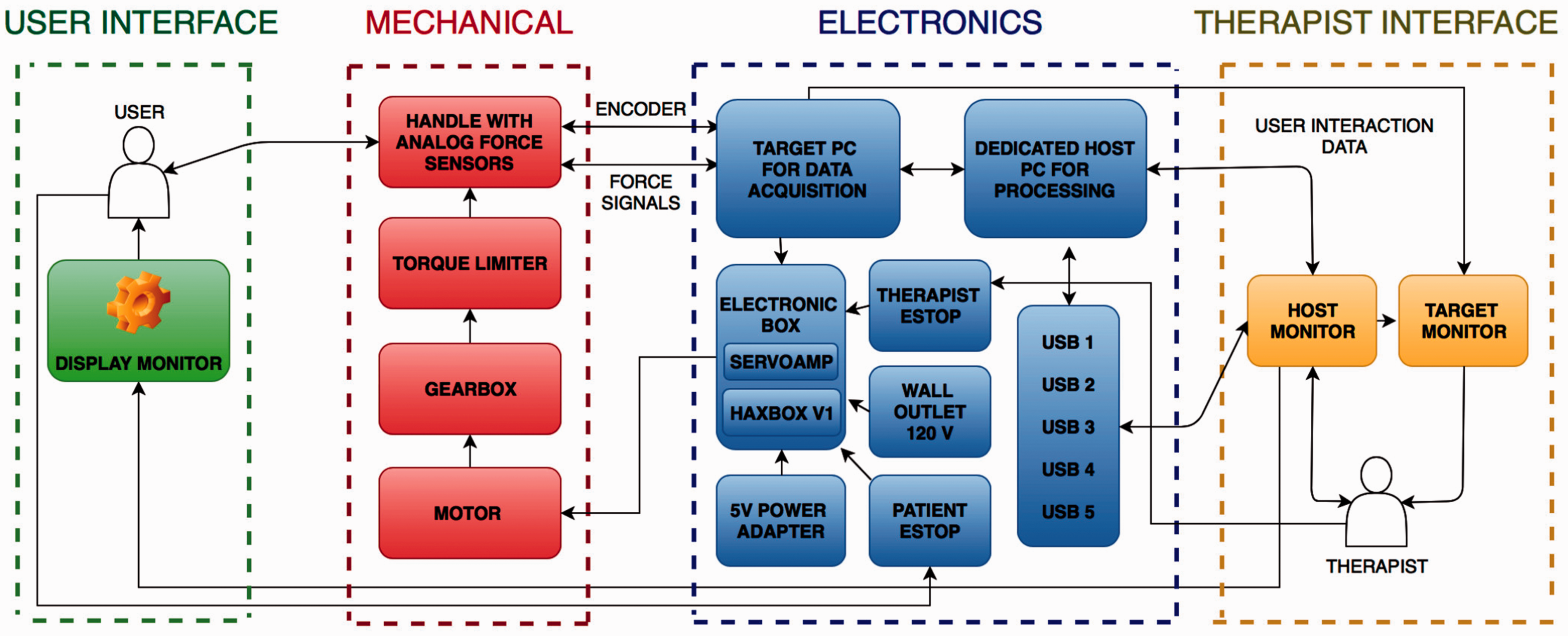
and is able to support the impaired arm of severe stroke survivors in either of the above cases. Due to stronger actuation, higher force assistance/resistance forces can be applied safely using a new compliant torque limiter. The control of the haptic robot uses an impedance-based controller, which uses position of the crank arm, custom load cell measurement of interactive forces on the handle, and knowledge of tracking performance to determine the force feedback experience on a tracking task (Figure 2). The controller can provide a zero-impedance mode, a static spring mode, or two adaptive control modes, which monitors patient performance and adjusts the spring stiffness to ensure that exercises are difficult but doable.44–46 The assistance/resistance of the haptic robot produced a significantly larger change in performance than that of the wheel since it is able to exert 30 times the torque of the wheel, and therefore can provide more assistance or resistance. The mechanical linkage of the haptic robot provides more support to subjects – sufficient for low-functioning subjects to be able to complete exercises. Pilot testing with the Haptic Theradrive
38
demonstrated its utility in providing adequate adaptive forces to move the impaired limbs of severely impaired stroke patients.
Theradrive (TD-1), Mexico Theradrive (TD-2), and Haptic Theradrive (TD-3). The Mexico Theradrive has a similar platform to TD-1. Note: Figure 1 used with permission from reference 37. Layout of Haptic Theradrive (TD-3)
Novel design of a compact robot gym with multiple exercise stations for affordable stroke therapy
Affordable robot technologies offer an enormous potential for improving health and function and decreasing the accessibility gap for low-resource environments both in urban and rural settings in LMICs.10,30 The pilot study results in Mexico suggest that we could potentially address issues of access to rehabilitation services in a cost-effective way in that a suite of low-cost systems of robot/computer-driven devices under limited supervision by clinicians could improve motor function of stroke survivors at a more cost-effective price ($29,000 USD). In Mexico, the estimated cost-ratio was calculated as cost per therapy which was $19.21 per hour considering traditional therapy as compared to $6.99 per hour for the rehab technology group leading to a 64% cost savings. 50 While this cost savings was significant and the cost of the six rehabilitation technologies was cumulatively much lower than many of the robot systems on the market, the World Health Organization (WHO) would still suggest that it is not sufficiently cost effective for most LMICs. The World Health Organization (WHO) promotes the adoption of “best buy” interventions for meeting healthcare needs in LMICs, which are cost-effective, affordable, feasible, and culturally acceptable. For Mexico, the WHO would suggest that a cost-effective rehabilitation intervention should range from a highly cost-effective solution of $9870 (GNI per capita for Mexico in 2014 calculated using the Atlas Method) to a cost-effective solution of $29610 (3× GNI per capita of Mexico). An intervention that costs more than 3×, the GNI per capita would be considered unreasonable. 56 Pertaining to this definition, the particular solution we deployed in Bustamante-Valles et al. 50 would be considered cost-effective. From the TD-2 deployment insights, we desired to develop a highly cost-effective affordable robot gym that can treat upper and lower limbs of stroke survivors within a smaller, more compact footprint at a cost much less than $9870. Since the robot gym concept in Mexico treated both the upper and lower limbs and resulted in improvements in both domains, we desire to retain the ability to effectively treat patients with low, medium and high motor impairment of the upper and lower limbs.
The design of a compact robot gym also meant redesign of the mechanical robots and a platform to provide multiple exercise stations. Our design process used a quality function deployment (QFD) approach, where end user needs are translated into functional needs, which are then further broken down into engineering requirements. 47 For example, the transportable requirement is a reflection of the end user’s needs, which functionally translates into a lighter system that can be moved easily. The engineering metric to evaluate meeting that functional need would be weight of the system and degrees of freedom of the robot base. Likewise, based on previous lessons learned, the redesign objective sought to improve each of the main mechanical system components to reduce its footprint, volume, weight, number of parts (and therefore the assembly/disassembly time) while minimizing costs and preserving the ability to safely include severely impaired persons in the treatment protocol. The following section sums up the target requirements for the multimodal, compact robot gym, which can deliver on the promise seen in Mexico, but at a more cost-effective price.
Functional requirements and proposed system
The functional requirements of a more compact robot gym system were the following:
Upper and lower extremity training using multiple robots: The system provides device stations that would allow task-specific training of the upper and lower limbs. Transportable: The device is easily transported from a place to another. It is easy to assemble and dismantle. Cost effective: The device is affordable in developing nations. The target price of the system is a maximum of $5000, which would be a about 6-fold decrease in cost. Given inflation and depreciation of the currency of many LMICs. This cost target may still be too much from the Mexico system. Maximize local resources: The system is constructed from the parts and materials that are locally available. This ensures sustainability in terms of construction of the device when the first generation device wears down or is damaged. Safe with minimum expert oversight: The system is safe to use with no or minimum number of experts on site. Haptic feedback: The robots are sensible to the users’ level of impairment and provide an adaptive controller that tailors the difficulty of exercises to the ability level of subjects. Regular feedback: The system records the user’s daily progress and outputs in a language that is understood by the users. This not only enables physicians to record the users’ progress over time but also could help the users see their progress. Gaming: The system uses commercial and custom games to maintain motivation in therapy. Multi-stations: The system provides the opportunity for one therapist to work with one or more patients simultaneously.
The proposed system has two components: the devices mounted in different orientations and the platform on which the devices are mounted. The result is a design and prototype of the robot gym system called Rehab C.A.R.E.S. Figure 3 shows two prototype versions (1(b) and (c)) – one with three commercial passive CARCI motion machines
63
and one with two commercial CARCI and the more compact, haptic Theradrive robot (TD-4 – upgrade from TD-3). The prototype has four stations (see numbers highlighted in Figure 1a) with machines that allow four patients to engage in progressive resistive exercise activities autonomously or semi-autonomously. The structure/platform is inspired by gait platform and designed to be easy to assemble, disassemble, easy to transport, robust and can be built with local resources. The first station is for shoulder movement (with three degrees of freedom), the second is for forearm pronation and supination, the third station will enable cycling of both the upper and lower limb, and the fourth station is the gait platform using a large pressure sensing balance board for gait and balance practice. The gait platform is embedded with three Wii boards that are arranged to accommodate a wide variety of patients with wide leg stance and stride lengths.
58
Subject’s center of pressure distribution is captured and mapped to the three Wii-board configurations for balance assessment, stepping and shifting posture assessment and practice.
59
(a–c) Current prototype version 1 with Haptic Theradrive and force sensing handle (yellow numbers = station numbers), 2bc: Actual and rendered drawing with four training stations. The first and second stations will work on range of motion and strength for the upper extremities including gross and fine movements. Stations three and four will work on gait and balance, where the person is secured to a harness. Wii boards are not shown.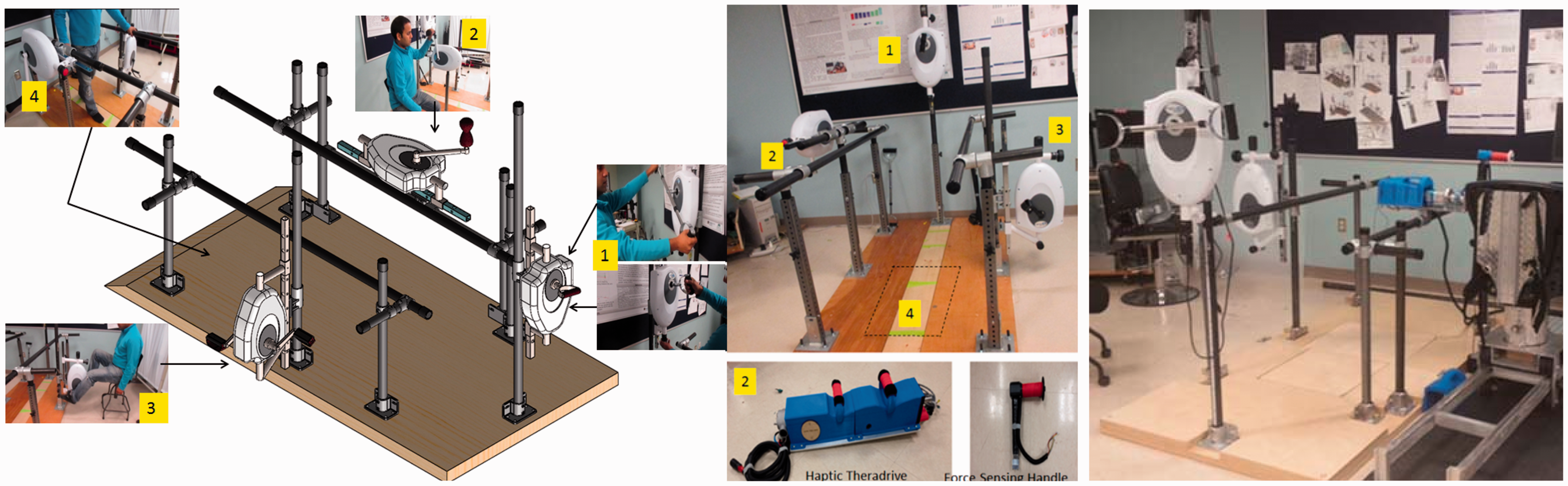
A passive CARCI can be replaced by a more compact version of the haptic Theradrive robot (Figure 3(c)), which provides adaptive force assistance or resistance as needed to keep the user training at a difficulty level appropriate for his or her level of function. All robots (passive or active) are one DOF devices fitted with position sensors and custom force handles. Signals are collected (via tablet PCs) and used to allow users to interact with PC-based commercial games as well as custom PC-based serious games
16
and tracking tasks. A variety of commercial games along with unity-based custom games developed internally can be used for therapy at each station.
59
The electronic components consist of several microprocessors and custom printer-circuit boards that drive the control architecture. Figure 4 details the flow diagram outline how the user and therapist interfaces are integrated with the mechanical and electrical architecture.
Schematic diagram of TD-4.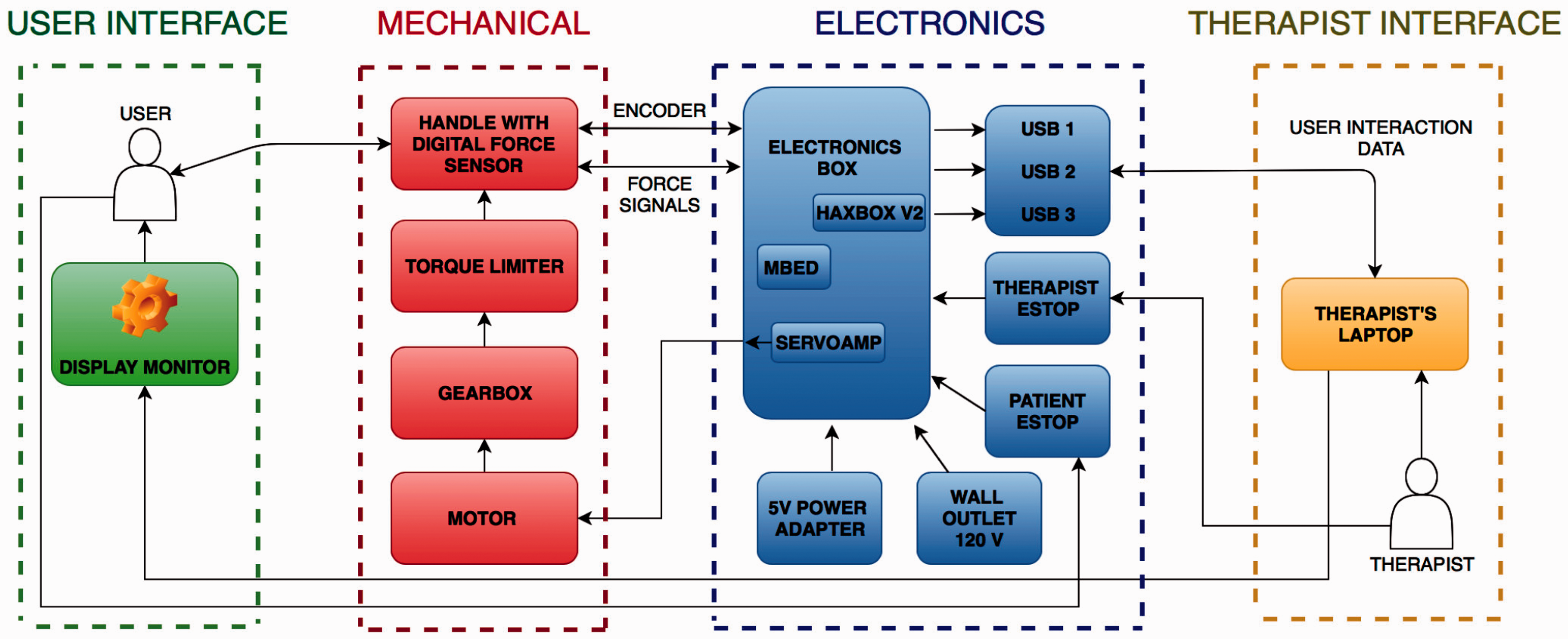
The new compact robot gym system currently costs about $5500 USD in materials and parts. The ultimate goal is to create a robot gym with three active robot exercise stations. This redesign represents approximately a 5.27-fold decrease from the robot gym concept deployed in Mexico which cost $29,000 USD, 50 and according to the WHO would be considered better than a highly cost-effective intervention strategy. If deployed in Mexico, the new compact gym would have a through put of about 4 patients per hour and 28 patients in a 7-h work day resulting in a 2× increase in therapist productivity.
Engineering development to fulfill functional requirements
Mechanical re-design
To achieve the robot gym system, the first major goal was to redesign the haptic Theradrive robot’s hardware and electronics to increase portability and ease of use within the context of a robot gym for rehabilitation in developing countries.
The new haptic Theradrive robot used in the robot gym (TD-4) was reduced in form factor, weight, cost and aesthetics resulting a more portable and maneuverable device. We achieved this in a variety of ways. For example, we increased portability by reducing the weight of the Haptic Robot by 25% without compromising its mechanical stability by replacing some mechanical parts with 30% infill 3D printed parts (built on the Makerbot Replicator 2). We increased safety and lowered cost by incorporating a more affordable, torque coupler which reduced robot length to 7.62 cm, increased tolerance to minor angular misalignment (6°) of the shafts, decreased assembly time, and reduced complexity of reassembling the robot once it is disassembled. The TD-4 robot is designed to accommodate a variety of end-effectors and transmissions to allow for 1DOF revolution in different planes. Up to three of these systems would be used in the Rehab C.A.R.E.S robot gym (Figure 3).
Electronics re-design
We reduced the complexity and cost of electronics and control system by replacing two PCs and the electronic box in TD-3 with a more compact electronic box, which encloses a much simpler data acquisition circuit for various sensors, sensor conditioning circuit, game interface circuit, a power supply and the low-cost microcontroller platform called MBED (Freescale).
48
The MBED takes care of the processing of the input from various sensors and sends the desired output to the robot for real-time control. We increased force measurement capability and boosted real-time processing of sensor signals by replacing the analog-based strain gauges with tactile digital sensors called Takktiles.
49
These low cost, tiny tactile sensors leverage the technology of MEMS barometers to deliver 1 g sensitivity, which provides a very accurate tactile feedback of the pressure applied by the user on the crank handle during tracking tasks. The Takktile sensors communicate via the Inter-Integrated Circuit (I2C) protocol, and the new system achieves much higher data transfer rates compared to the strain gauge system, thus allowing the impedance control scheme to provide a much smoother real time control. A dedicated graphical user interface that bundles together different parts of the therapy tasks such as the trajectory tracking task, gaming tasks, data logging, etc. and a TCP/IP-based centralized python server was implemented, taking care of the GUI and data logging and thus, removing the necessity for proprietary software such as MATLAB. This resulted in faster processing, which significantly improved time required for diagnosis and allowed for more time spent during therapy games rather than on set-up and data saving. Additionally, the path away from specific Matlab License allowed for a firmware architecture that is easily replicated. This will be particularly useful in creating economies of scale as the quantity of TD-4 developed goes higher. Figures 4 and 5 outline the new control flow for TD-4, which leverages the control algorithms used in TD-3. Overall, the TD-4 haptic Theradrive robot redesign resulted in a 25% reduction in cost for the robot (approx. $2500) and a 25% reduction in weight (from 14.4 kg to 10.8 kg). The weight and size of the TD-4 robot, coupled with the grip handles, make for easy set-up, lifting, and re-configuring of the system for front or side drive difficulty. A significant reduction in weight and length of TD-4 (compared to TD-3) increased portability, ease of set-up, and the ability of a skilled worker to safely lift, re-configure, and set-up the system multiple times in an 8-h work day.
64
Control scheme of TD-4.
The compact robot gym would consist of one or more TD-4 robots. In Figure 3(c), TD-4 is mounted on station 2.The controller would be implemented on each of the TD-4 robot exercise station where up to three robots could be used in the robot gym configuration in Figure 3. The electronics scheme would be augmented with microprocessors as needed to accommodate the additional robot units and the Wii boards’ data collection (Figure 4).
Validation of TD-4 on station 2 of robot gym
We tested four persons with hemiplegia due to a stroke on the TD-4, which is the haptic Theradrive station 2 (see Figure 6 in text – haptic theradrive in blue). All subjects gave informed consent and the pilot study was approved by the Human subjects ethics committee of the University of Pennsylvania. All strokes were cortical lesions. Subjects were evaluated for cognitive impairment using the Montreal Cognitive Assessment (MoCA),
61
for motor impairment using the FM Assessment test for upper limb41,64 and for gross reach and grasp function using the Box and Block test,
60
a measure suggesting some carryover to real life. After assessments, subjects used the Theradrive system for 12 sessions, 60 min each session to play game-based activities. The results of their clinical tests are presented in Table 1.
Station 2 with Theradrive – TD-4. TD-4 test station subjects.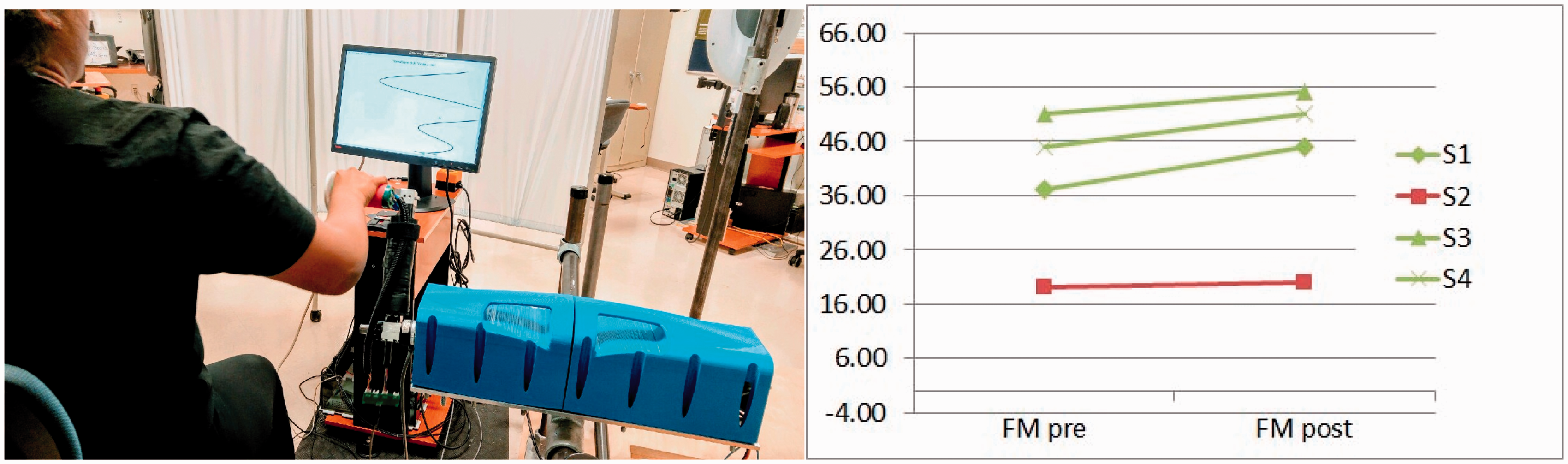

Testing results suggest persons with moderate functioning and mild cognitive function will respond to robot-assisted therapy using the Theradrive station within 12 sessions. Figure 6 shows station 2 with TD-4 and the results pre- and post- 12 sessions. Three of the four patients with stroke responded well to the therapy with the Haptic Theradrive station within 12 sessions and had an average six-point gain in motor function (FM-pre 44 ± 0.7 and FM-post 50 ± 5). One low functioning stroke survivors (FM-pre 19) and (FM-post: 20) only gained one point in motor control within the 12 sessions suggesting additional sessions may be necessary to see better outcomes. Correspondingly, the box and block test scores, which assess gross reach and grasp skills, improved for all except the low functioning subject. One stroke patient, S1, returned after one month and was retested. His upper limb motor control improved by another three points on the FM and his gross reaching and grasping tasks skills remained stable. 56 Further testing of Robot Gym with all stations is still needed.
Implications for usability of Rehab C.A.R.E.S robot gym
The clinical results suggest that TD-4 would be able to perform effectively as the active haptic robot at one or more of the exercise stations within the robot gym (Figure 3(c)). The improvements experienced by patients suggest that a minimum of 12 sessions (60 min each) would be needed per station and those with more severe impairments may need the additional treatments. In the Mexico study, low functioning subjects with FM upper limb motor scores that were less than 15 experience little or no upper limb motor improvements (+1 FM change) from their circuit training paradigm, while those that had baseline motor scores ranging from 17 to 51 saw greater than clinically significant increases (avg. +6.5 FM changes). Three of the four patient case studies on the TD-4 mounted on station 2 of the Rehab C.A.R.E.S Robot Gym experienced robust changes in half the exposure times (avg. +5 FM changes). The interventional protocol for the four stations, Rehab C.A.R.E.S Robot Gym would leverage the methods used in the Mexican study 50 where stroke survivors completed 24 2 h therapy sessions over six to eight weeks. Given this paradigm, one therapist could treat four patients by allowing each patient to experience 30 min of exercise on at each of four stations.
Discussion
We present one possible pathway towards developing affordable robots and mechatronic systems for stroke rehabilitation in developing countries. Early in our development work, we coined the phrase robot/computer-assisted motivating rehabilitation to describe our vision to create access to rehabilitation in resource-limited settings, 32 a concept and trend that have since been promoted and supported by other studies.16,19 We have evolved from using a commercial one 1 DOF mechatronic device as the exercise interface to using a stronger 1 DOF haptic robot as the exercise interface and finally to incorporating this robot into a compact suite of 1 DOF devices that can be used with custom or commercial games. The use of off-the-shelf commercial devices and games to provide therapy is viable but may lead to exclusion of more severely impaired stroke survivors and inappropriately tuned games. By developing simpler and affordable haptic robots and custom games with patient-centered adaptive control and games, more severely impaired stroke survivors can benefit at an affordable price. In LMICs, the provision of care focused on only the upper limb or the lower limb or on one disease state is often not practical. In collaborating with colleagues in Mexico, we were able to test the concept of using multiple rehabilitation technologies including an upper limb station for Theradrive in circuit training paradigm with six exercise stations which together provided both upper limb and lower limb exercise. The success of pilot testing led to the Rehab C.A.R.E.S robot gym platform, which offers a compact strategy for providing affordable robot therapy in high-, middle- and low-income countries.
In limited resource locations in the USA and in LMICs, accessibility issues are intensified, engineering resources are limited, infrastructure may be unreliable and skilled clinical help is scarce. The new compact robot gym can leverage low people resources for rehabilitation. We demonstrate that by using the haptic robot (TD-4) as a station, we can support the training of all levels of motor impaired stroke survivors, but training intensity and treatment intervention period may need to vary by baseline motor function. Using the haptic Theradrive alone or as one of the stations within the robot gym is an innovative solution that has the potential to augment the delivery of rehabilitation care in Mexico and other LMICs in a highly cost-effective way. Our resulting robot gym concept may increase rehab care clinicians’ productivity and efficiency by providing opportunity for one therapist (with possible assistance from one physical therapist assistant) to engage and simultaneously treat four patients using state-of-the art algorithms and robot-assisted strategies.
Future work on this system would involve deployment and test of the system within clinics in an LMIC and integration of these systems with mobile or tele-health tools already making inroads into these countries. 65 Mobile technologies such as cell phones and tablet PCs, new low power wireless communication protocols, and internet-enabled video communication (e.g. Skype) are readily available in LMICs.52,53 Mobile devices are being used for tele-monitoring and mobile health applications to monitor and track patients. Combining robot gym with accessible mobile technologies for telehealth offers an enormous potential for improving health and function and decreasing the accessibility gap for low-resource environments both in the USA and in LMICs.53–55 More efforts are needed to develop affordable robots for global health and rehabilitation.
Footnotes
Acknowledgements
We would like to extend our thanks to all the members of the Rehabilitation Robotics Lab in USA and Centro de Tecnología e Investigaciœn Biomedicina (CTIB) in Mexico. We acknowledge the Clement J Zablocki Veterans Administration for supporting the initial development of the Theradrive system at the the Marquette University mechatronics lab. We thank the Department of Physical Medicine and Rehabilitation, University of Pennsylvania. We also acknowledge the assistance provided by the Centro de Rehabilitación y Educación Especial (CREE)-DIF Chihuahua and its personnel, Dr. Yuridia Rufino and OT Amalet Aranda. We appreciate the collaboration of the senior research technicians in the CTIB, especially Erick Madrid. We are grateful for the participation and dedication of all the patients involved in this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the American Heart Association under the grant #0635450Z entitled “Robot-Assisted Motivating Rehabilitation after Stroke,” by departmental funds of the Physical Medicine and Rehabilitation of the Medical College of Wisconsin; the Mexican government grant# CHIH-2009-C02-127781 entitled “Gimnasio Robotica” and CONACYT I0015-225083.