
Abstract
School psychologists and counsellors are increasingly asked to support children and families in navigating healthy screen use. Excessive screen use among children is a growing concern, associated with adverse health outcomes. While family involvement is crucial, the effectiveness of family-based interventions for managing screen use remains unclear. This review synthesised global evidence on family-based interventions for managing screen use in children and adolescents (5–18 years). A comprehensive search across eight databases (Jan 2000–Nov 2024) identified 45 interventions (62% were school-based), examining screen use duration, content, context, and interactions. Random effect meta-analysis showed a reduction in total screen time (SMD = −0.11, 95%CI [−0.20, −0.02]); however, there were inconsistent effects for other outcomes (television, computer, and gaming time). Intervention component analysis and qualitative comparison analysis was conducted on 15 effective interventions of high quality. Six out of 17 components demonstrated high consistency, including individual-focussed (classroom lessons, educational resources, interactive activities, and content building children’s knowledge, awareness, and digital skills) and family-focussed (informative materials and parent education) components. Findings showed school-family partnerships are particularly effective in promoting healthy screen use and in empowering both children and caregivers, with direct implications for the preventative and consultative roles of school psychologists and counsellors.
Introduction
Globally, most school-aged children and adolescents exceed recommended daily screen time limits, with prevalence of excessive use across age groups and countries (Qi et al., 2023). Screen time refers to the total duration spent on electronic devices such as smartphones, laptops, and television, whereas screen use encompasses the diverse range of activities enabled by these devices such as watching television, studying online, or using social media (Kaye et al., 2020). Discretionary or recreational screen use describes leisure-based engagement on screens that is not related to work or education, often passive or sedentary in nature (Celis-Morales et al., 2018; Tremblay et al., 2017). Depending on the purpose, discretionary screen use may be beneficial or detrimental when excessive, affecting young peoples’ physical health, mental well-being, and academic outcomes (T. Sanders et al., 2024; Stiglic & Viner, 2019).
School-based psychologists and counsellors are playing an increasingly central role in supporting children, adolescents, and families to develop and maintain healthy screen use practices. Recognising the negative effects of excessive screen use, various interventions, and strategies to regulate and balance childrens’ screen use have been implemented across home, school, community, and digital settings. These interventions primarily focus on behaviour change, aiming to reduce screen time, minimise problematic use, enhance media literacy, and promote healthy behaviours using techniques like goal setting, self-monitoring, shaping knowledge, and social support mechanisms (Jones et al., 2021; Krafft et al., 2023; Oh et al., 2022). Among these, school-based interventions are popular, as schools serve as key implementation sites, providing targeted support through classroom education, counselling, and peer learning opportunities (Friedrich et al., 2014; Throuvala et al., 2020).
Family engagement is also crucial, with evidence showing the positive influence of household rules, parental behaviours, role modelling, and monitoring in reducing screen time (Arundell et al., 2020; Marsh et al., 2014; Minges et al., 2015). Despite growing autonomy in adolescents, families are uniquely placed to regulate adolescent media use at home, where most of the recreational screen use happens (Ding et al., 2024). However, the majority of existing interventions remain school-based, with limited to no family engagement. Even when family involvement is present, its extent varies, ranging from active participation (e.g. parent-child media use plan (Moreno et al., 2021)) to passive involvement (e.g. merely receiving educational materials (Apisitwasana et al., 2018)). Given the central role of parents in shaping adolescents’ daily habits and regulating media use, there is scarcity of evidence on whether family-based interventions are effective in managing screen use in school-aged children and adolescents (Marsh et al., 2014).
Existing systematic reviews and meta-analyses have identified effective interventions aimed at reducing screen time among children and adolescents across a broad age range (0–18 years; Jones et al., 2021; Krafft et al., 2023; Wu et al., 2016). While these reviews provided valuable evidence, including age-stratified estimates (Jones et al., 2021), they lacked a dedicated focus on the distinct developmental needs of school-aged children and adolescents. Screen use in children under 5 years is largely shaped by parental control, early learning contexts, and developmental needs (Mallawaarachchi et al., 2024). In contrast, school-aged children and adolescents engage in diverse forms of digital media and experience peer and school influences, highlighting the need for a review focussing exclusively on this age group.
While reducing screen time has been well-researched, interventions for addressing broader aspects of screen-based behaviours are understudied for this age group (Reeves et al., 2020). Specifically, a comprehensive approach to managing screen use goes beyond limiting duration, it considers the content (what is being consumed), context (purpose or settings), and interaction (level of engagement) with screens (Griffith et al., 2024; Kaye et al., 2020; Reeves et al., 2020). For instance, the Canadian Paediatric Society (2019) emphasises the need for interventions promoting healthy screen use by not only managing screen time, but also encouraging meaningful digital engagement, positive role modelling, and proactive monitoring for signs of problematic screen use.
Additionally, many interventions adopted a multicomponent approach, combining several strategies simultaneously. A previous systematic review identified study characteristics and behavioural techniques such as goal setting, feedback, and planning as effective in reducing screen time for children aged 0 to 18 years; it also noted that interventions shorter than 12 weeks could still achieve significant reductions in screen time (Jones et al., 2021). However, existing studies often evaluate the overall effectiveness of these multicomponent interventions without assessing the contributions of individual components independently (Krafft et al., 2023). This makes it challenging to determine precisely which strategies or combinations of strategies yield the most substantial effects (Krafft et al., 2023). Identifying key components of interventions is critical for designing targeted, scalable, and effective programmes that maximise impact and minimise resources (Jones et al., 2021). At present, there is limited evidence on which specific components are likely to be effective, particularly within the context of family-based interventions for managing discretionary screen use.
To address these gaps, the present review evaluated the effectiveness of family-based interventions in managing discretionary screen use among school-aged children and adolescents (5–18 years). This work adds value compared to previous reviews in three key ways. First, it focusses specifically on interventions with family engagement, acknowledging the importance of caregivers in shaping adolescent screen behaviours. Second, it takes a multidimensional approach, considering studies that address not only screen time, but also challenges related to content, context, and interactions, including problematic behaviours and risky engagement. Third, it undertook a qualitative approach combining intervention component analysis (ICA) and qualitative comparative analysis (QCA) to identify components that were both effective and consistently present in successful interventions (Suen et al., 2023). Therefore, this review seeks to address: What is the effectiveness of family-based interventions in managing discretionary screen use among school-aged children and adolescents, and which components are consistently associated with successful outcomes? The findings will inform the design of future evidence-based strategies to promote healthy screen use in school-aged children and adolescents.
Method
The current systematic review was registered with the International Prospective Register of Systematic Reviews (PROSPERO #: CRD42023414857). The review was conducted and reported according to the Preferred Reported Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (Page et al., 2021). For this review, family-based interventions were considered as studies that involve family members or parents or caregivers of children or adolescents. We included studies where family members participated at any level, ranging from passive (e.g. receiving newsletters or information leaflets) to active involvement (e.g. attending parent sessions or directly supporting adolescents). Because family factors including parenting practices and engagement is a key determinant of children’s media use, interventions with any level of parental involvement were considered family-based, regardless of settings (X. Liu et al., 2024).
Search Strategy
A systematic search of studies was conducted across eight electronic databases: PubMed, Web of Science, Scopus, EMBASE, CINAHL, PsycINFO, EBSCOhost, and The Cochrane Library. Snowball searching from the reference lists of the included studies was also conducted to ensure no relevant studies were left out. The search strategy (keywords) for all the databases is described in Supplemental Table S1. Databases were searched for articles published in English from January 2000 to May 2023 and an updated search was conducted from June 2023 to November 2024. This represents a period during which research on screen time increased alongside the widespread adoption of social media and smartphones (LeBlanc, 2017).
Inclusion/Exclusion Criteria
The present review included interventions aimed at managing any aspect of screen use in typically developing children aged 5 to 18 years, with at least one family member or caregiver participating in interventions conducted in home, school, community, or digital settings. This age range represents the school-aged population globally, as well as an age where most teens live with their families (X. Liu et al., 2024; OECD, 2025). Interventions were eligible if they targeted screen time (e.g. total duration, TV viewing, and gaming time), content (e.g. violent media and harmful digital material), context (e.g. home environment and family media use), or interactions (e.g. problematic internet or gaming, cyberbullying, and online safety). Randomised controlled trials (RCT), cluster randomised controlled trials (cRCT), non-randomised trials (NRT), quasi-experimental (QES), and pre-post study designs with any relevant comparator or non-intervention control group were included. There were no restrictions on the study’s geography, race/ethnicity, gender, and income status of the country. Likewise, no restrictions were set on intervention duration, components, and strategies, except for the primary outcome of interest, which had to be some form of screen use. Children with medical or neurodiverse conditions, young adults over 18 years, pre-school children below 5 years, non-intervention studies, observational studies, review articles, interventions with primary outcomes other than screen use, studies not in English, studies conducted prior to January 2000, and articles with no access to full text were all excluded.
Study Selection Process
Once the searches were completed, results were exported to EndNote X9 reference manager and then into Covidence software (www.covidence.org) to remove duplicates. Overall, 16,992 articles were identified from the eight electronic databases search; 2,997 articles were removed as duplicates. In the first phase, one reviewer (AR) independently screened each study by title and abstract (n = 13,995); next a random sample of 5% screened by the second reviewer (MN) to assess the degree of agreement (Ben Charif et al., 2022; Gaeddert et al., 2024). Full-text screening (n = 207) was conducted by two independent reviewers (AR and MN). The inter-rater reliability (κ = .89) was good (Koo & Li, 2016), indicating strong agreement between the two reviewers. After full-text screening, article reference lists were also searched. Any disagreements and conflicts regarding study inclusion or exclusion at all screening stages were resolved by two reviewers (AK and EE). Upon excluding articles based on the inclusion and exclusion criteria, a final set of 45 articles was included in this systematic review for data extraction and analyses as mentioned in the PRISMA flow diagram (Figure 1).
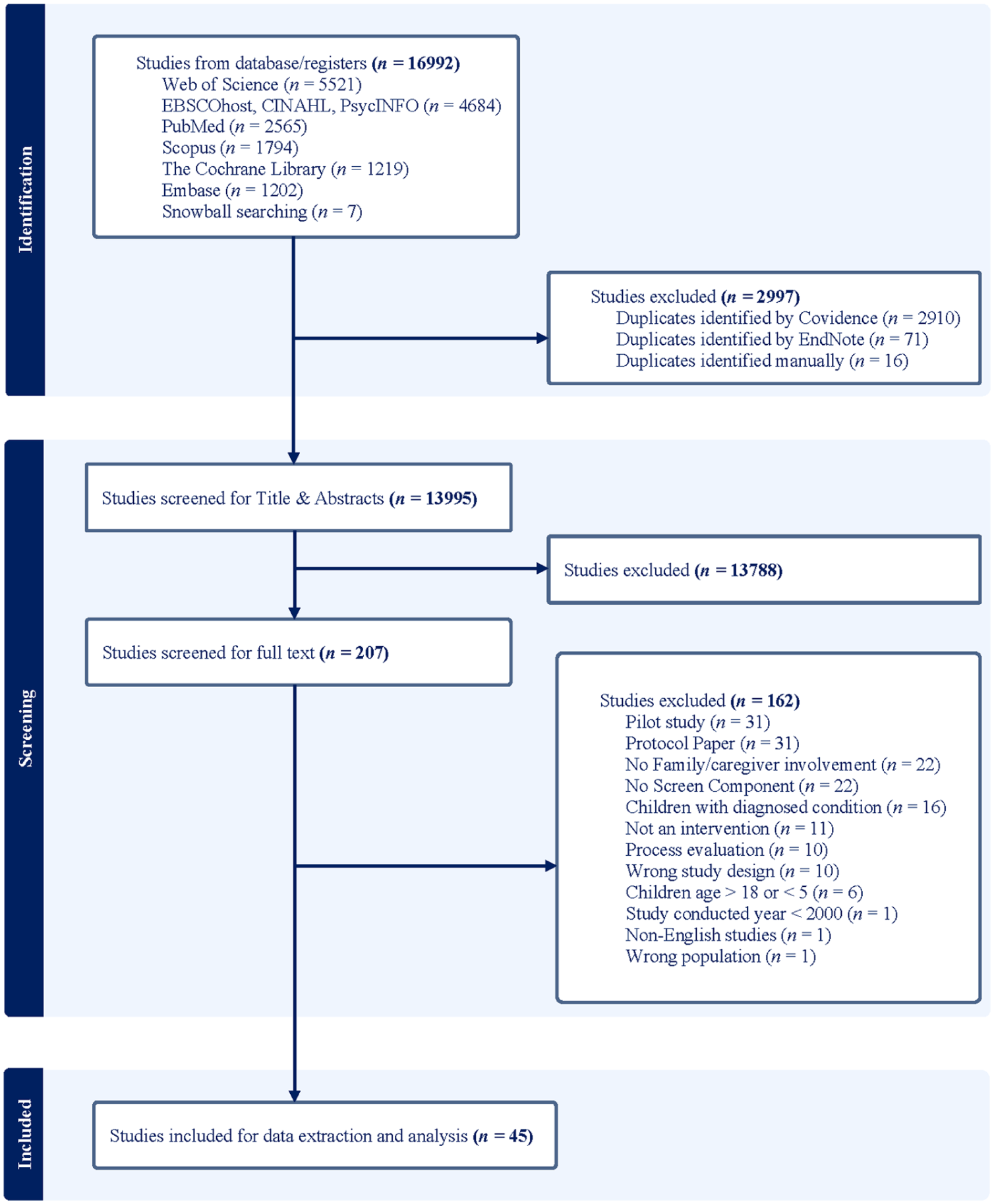
PRISMA flow chart of study selection process.
Data Coding, Extraction, and Quality Appraisal
Data coding and extraction from the selected studies was conducted and reviewed by two researchers (AR and MN) in an Excel spreadsheet. The data extraction form included: study characteristics (intervention duration, setting, strategy types, country, and design), sample characteristics (size, age, and gender), screen use measurements (screen time and type of screen), and results (descriptive statistics, effect size estimates, and statistical test results). Quality assessment was performed using the Cochrane risk-of-bias tool for randomised trials (RoB 2) for randomised studies, and the ROBINS-I tools for non-randomised studies (quasi-experimental and pre-post studies; Sterne et al., 2019). The risk of bias in each study was assessed across several quality criteria based on the guidelines for both randomised and non-randomised studies: allocation concealment, selective reporting, blinding of participants and personnel, blinding of outcome assessment, controlled confounders, random sequence generation, and incomplete outcome data. All studies were assessed by two independent reviewers (AR and MN) and any disagreements were resolved by discussing them with the other reviewers (AK and EE). The overall risk of bias judgement across all domains was identified as low, some concerns, or high risk of bias based on an assessment algorithm (Sterne et al., 2019).
Meta-Analysis
Meta-analysis was undertaken using the ‘meta’ package in R to examine the overall effectiveness of family-based interventions and to quantitatively synthesise homogenous studies (Schwarzer et al., 2015). In line with guidance from Cochrane, which cautions that meta-analyses may be misleading when based on methodologically weak or highly heterogeneous evidence, only studies assessed as moderate or high quality were included in the primary meta-analysis (Deeks et al., 2019). Therefore, studies (n = 21) of moderate and high quality with relevant outcome measures were considered. Only 12 studies were included in the meta-analysis based on availability of four relevant outcomes (total screen time, television time, gaming time, and computer time) and post-intervention data (n, mean, and SD) for both intervention and control groups.
Total screen time was defined as the overall duration of leisure-based screen use, with television time as time spent viewing television, gaming time as recreational electronic gaming on any platform, and computer time as non-work use of computers or laptops, as operationalised and measured in the included studies. Meta-analysis were conducted for each outcome if there were at least two studies in each of the analyses (Deeks et al., 2019). All the measures were converted to the same unit of measurement (min/day) to ensure comparability. A random-effects model was applied to account for expected heterogeneity across studies, rather than a fixed-effect model which assumes a common effect size. Heterogeneity was assessed using the I2 statistic. Study specific estimates were calculated as standardised mean differences (Hedges’ g with 95% CI) comparing intervention and control groups post-intervention and pooled effect estimates were obtained for the four outcomes at 5% significance level. Funnel plots and Egger’s test were used to check for any publication bias. To assess the robustness of findings to study quality, a sensitivity analysis was conducted by including studies with high risk of bias.
Component Analyses
Intervention Component Analysis (ICA) and Qualitative Comparison Analysis (QCA) were combined to identify effective components that are likely to contribute to the intervention’s success (Melendez-Torres et al., 2019). Integrating ICA-derived theoretical insights into QCA helps prevent data dredging and is well-suited for small trials with high heterogeneity and intervention complexity (Sutcliffe et al., 2022). These approaches have been widely applied in systematic reviews of complex public health interventions (Ahmed et al., 2024; Zahroh et al., 2023). To ensure methodological Rigour, reliability, and validity in identifying key intervention components, only 15 studies of effective interventions from the 21 moderate- and high-quality studies were selected. An intervention was classified as ‘effective’ if it demonstrated a statistically significant improvement (p < .05) in at least one screen use outcome at post-intervention. Excluding low-quality studies reduced the risk of bias and ensured that the identified components were drawn from interventions with stronger evidence, thereby increasing the robustness and credibility of the findings, as well as aligned with best practices in ICA and QCA (Melendez-Torres et al., 2019; Thomas et al., 2014). ICA employed inductive thematic analysis to code these components (Braun & Clarke, 2006).
Two independent researchers (AR and MN) first familiarised themselves with intervention materials and published descriptions of the 15 effective interventions. Through line-by-line review, they identified discrete strategies or components (e.g. ‘classroom lessons on screen use’, ‘parent newsletters’, and ‘goal-setting activities’). These components were then iteratively compared across studies and grouped into broader themes based on conceptual similarity (e.g. individual-focussed education strategies vs. family-focussed support strategies). This process continued until thematic saturation was reached and a stable coding framework emerged. A third researcher (AK) reviewed the coding framework to ensure consistency and resolve any discrepancies.
Structured comparisons across diverse study outcomes strengthened the reliability and applicability of findings, ensuring that recommendations are grounded in empirical evidence (Kane et al., 2014). Consistency of components was assessed based on frequency of occurrence in effective studies (Kane et al., 2014; Melendez-Torres et al., 2019) as:

QCA was then applied to determine whether these components were necessary and/or sufficient for achieving the desired outcome (Melendez-Torres et al., 2019). The first step in QCA involved constructing a truth table, a matrix of all possible combinations of intervention components alongside their associated outcomes. Each row in the truth table represents one intervention, with columns indicating the presence (1) or absence (0) of each component, plus a final column showing whether the intervention achieved a successful outcome. This table enables systematic comparison of component configurations across interventions to identify patterns associated with success (Sutcliffe et al., 2022). Through an iterative process, QCA identified key intervention combinations. Components were categorised based on emerging themes, and those with high consistency were selected to construct possible intervention pathways using Boolean expressions (Thomas et al., 2014). Any logical remainders (combinations of features not present in the interventions) were examined to refine the model and ensure a strong theoretical foundation (Suen et al., 2023). The most effective intervention pathways were determined by systematically evaluating component consistency across interventions. Consistent with prior research, a threshold of Y ⩾0.60 was adopted to identify components with ‘high consistency’ (Thomas et al., 2014). Using truth tables and Boolean analysis, key intervention components were expected as necessary and/or sufficient for success and were integrated into a theoretical model to optimise intervention design (Melendez-Torres et al., 2019).
Results
The 45 included studies were systematically analysed and qualitatively synthesised to determine (1) the effectiveness of family-based interventions for managing discretionary screen use in school-aged children and adolescents; and (2) the components or strategies included in effective interventions.
Study Characteristics
An overview of the characteristics of the 45 identified studies is provided in Table 1. As can be seen, the included studies were published between 2006 and 2024, with more than half (n = 28) of the articles published in the last 10 years. The studies were conducted across 21 countries. Most were from the USA, accounting for one-fifth (n = 9) of the total, followed by Australia (n = 6) and China (n = 5). According to the World Bank classification of countries by income status, majority (n = 31) of the studies were conducted in high-income countries, compared to upper-middle-income countries (n = 13), and lower-middle-income countries (n = 1). Thirty studies were conducted with children aged 5 to 12 years, while the remaining (n = 16) focussed on adolescents aged 12 to 18 years. Of the studies included, (n = 14) were delivered in schools, another (n = 14) in both schools and homes, (n = 10) took place in home only, (n = 4) were community-based, and (n = 3) in home, school, and community settings, making school-based delivery the most popular implementation site. Interventions were facilitated either by trained teachers in schools or by research staff, with parental involvement ranging from attending health education sessions, engaging in parent–child interactive homework to receiving newsletters and feedback from staff. The majority of the studies focussed on reducing screen time (n = 29), while only few targeted regulating content (n = 1), context of use (n = 1), and interactions (n = 3), such as problematic internet use or cyberbullying. The remaining studies (n = 11) addressed combinations of these aspects, for instance, an intervention raised awareness of problematic internet use while also modifying household media practices (Şermet Kaya et al., 2022). The most common study design was RCT, accounting for nearly half of the studies (n = 21), followed by cRCTs (n = 18), and only small number of studies were QES and pre-post (n = 6). Notably, all of the studies utilised self-reported measures of screen use for adolescents and parent-reported measures for younger children (n = 44), only four studies collected data using activity diaries and one study utilised objective assessment of screen time using an app.
Overview of the sample and intervention characteristics of n = 45 included studies.
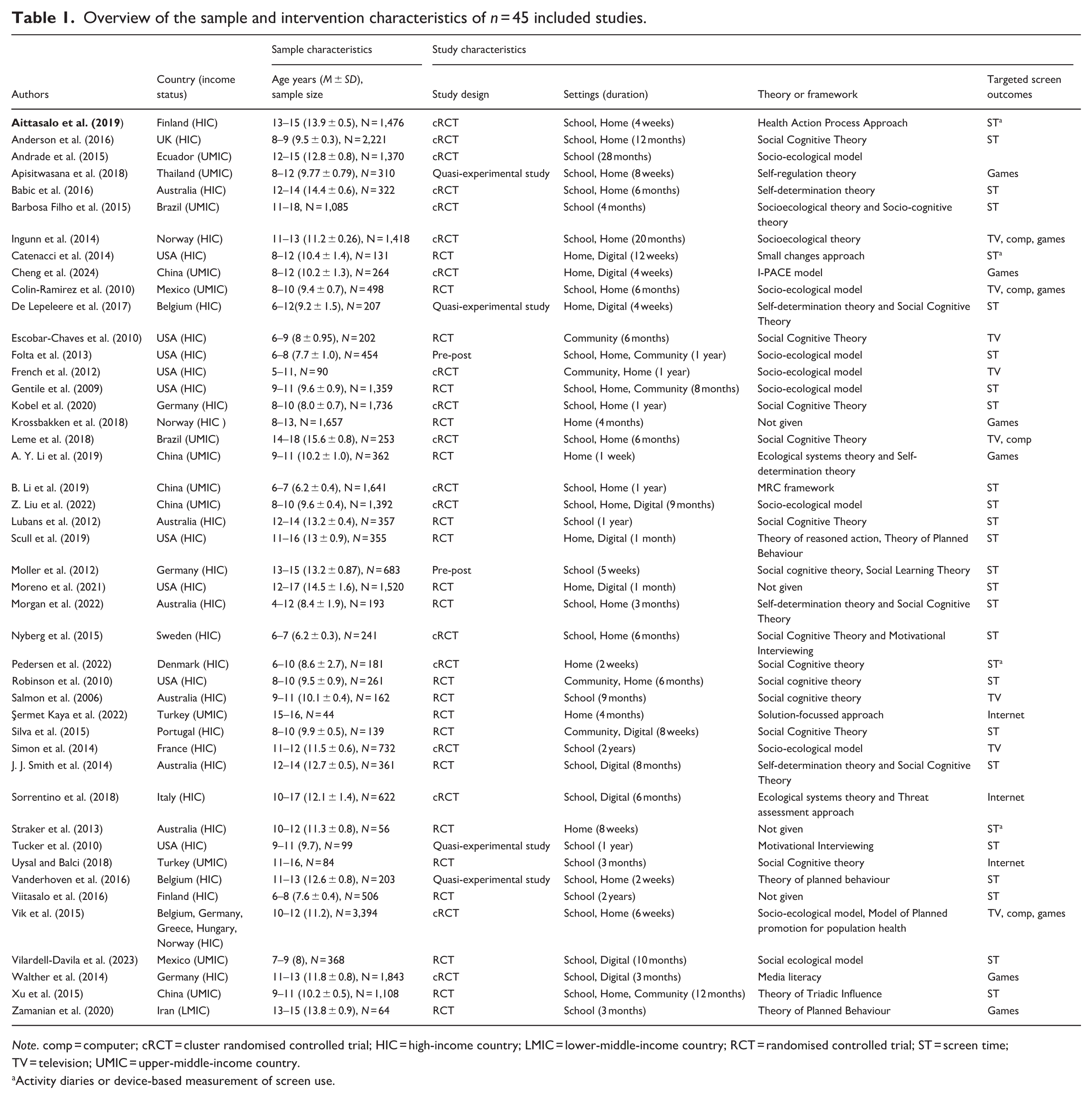
Note. comp = computer; cRCT = cluster randomised controlled trial; HIC = high-income country; LMIC = lower-middle-income country; RCT = randomised controlled trial; ST = screen time; TV = television; UMIC = upper-middle-income country.
Activity diaries or device-based measurement of screen use.
Study Quality
According to Cochrane’s risk of bias assessment tools, 33% (n = 15) of studies were assessed as low risk of bias, 13% (n = 6) had some concerns, and 55% (n = 24) were of high risk. Study-wise quality assessment and overall risk of bias across different study designs are depicted in Supplemental eFigure 1. Among the RCTs and cRCTs, 24 studies were of low quality. Only 12 RCT and cRCT studies were high quality. The QES and pre-post studies (n = 6) had two low quality studies, one study with moderate quality and three high quality studies. Most common reasons for concerns with study quality were deviations from the intended interventions, missing outcome data, such as loss to follow-up or participant drop-out and bias in methods of measuring the outcomes. Details of components and intervention effects on screen use outcomes of moderate and high quality studies (n = 21) are described in Supplemental Table S3.
Results of Meta-Analysis
The inclusion of studies for meta-analysis and subsequent component analyses is summarised in Supplemental eFigure 2. The meta-analyses, based on moderate and high quality studies with relevant outcome data, assessed the effectiveness of family-based interventions across four distinct outcomes: computer time (n = 4), gaming time (n = 4), television time (n = 4), and total screen time (n = 9). Meta-analysis across outcomes showed that pooled estimate was negative, indicating that the intervention group had less screen time than the control group. Family-based interventions therefore led to a small but significant reduction in total screen time (SMD = −0.11, 95% CI [−0.20, −0.02], I2 = 19.6%, n = 9), whereas no significant effects were observed for computer time, gaming time, or television time (Figure 2). Heterogeneity across studies was low, with I2 values ranging from 0% to 28%, indicating limited variability in effect sizes.
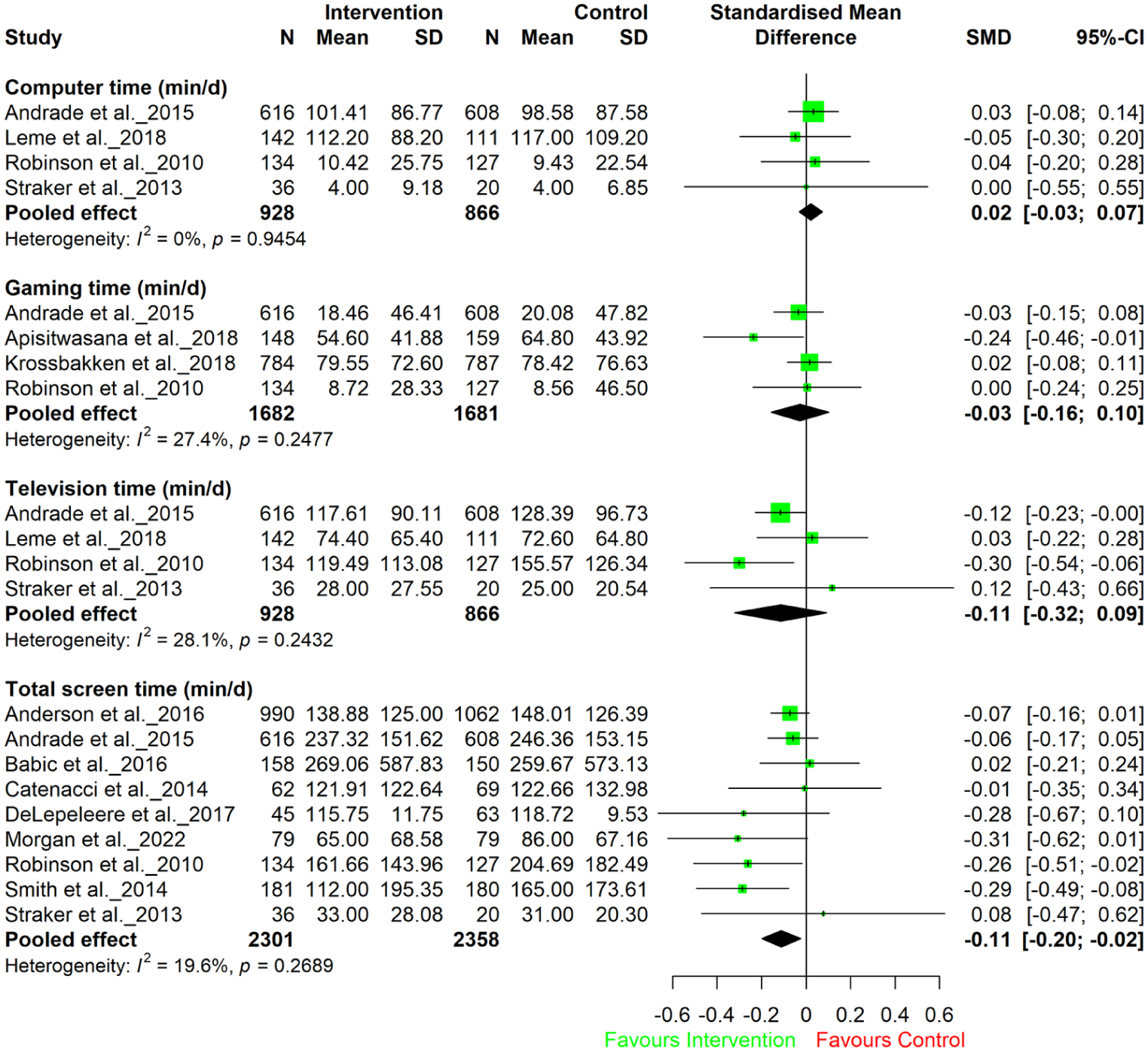
Forest plot of meta-analyses of computer time, gaming time, television time, and total screen time (min/d).
To evaluate potential publication bias, a contour-enhanced funnel plot was visually inspected (Supplemental eFigure 3). Publication bias was assessed only for total screen time (n = 9), since combining different screen-use outcomes would result in incomparable effect estimates. Funnel plot showed asymmetry, could be the presence of small-study effects, where smaller studies with negative or null findings may be underrepresented. However, Egger’s regression test did not indicate significant publication bias (p = .3300), suggesting that the apparent asymmetry may be due to chance rather than systematic bias. As fewer than ten studies were available, both the funnel plot and Egger’s test have limited reliability and should be interpreted with caution. Sensitivity analyses that included studies with high risk of bias showed an attenuation of the pooled effect for total screen time, which was no longer statistically significant (SMD = −0.04, 95% CI [−0.30, 0.21], n = 16), with substantial heterogeneity observed (I2 = 97.8%). Therefore, restricting meta-analysis to studies of low and moderate risk of bias minimised mishandling of pooled estimates arising from methodological limitations in high-risk studies.
Interventions With Family Involvement
Family involvement varied widely across the included studies. Several interventions involved parents actively through interactive sessions such as workshops, parental meetings, health education classes, and group discussions facilitated online or at school premises or community centres (Andrade et al., 2015; Krossbakken et al., 2018; B. Li et al., 2019; Z. Liu et al., 2022; Moller et al., 2012; Morgan et al., 2022; Viitasalo et al., 2016; Xu et al., 2015). These sessions promoted parenting skills such as role modelling, reinforcement, self-control, resilience, and managing conflicts (Andrade et al., 2015; Babic et al., 2016; Morgan et al., 2022; J. J. Smith et al., 2014; Xu et al., 2015). Others provided educational materials, including online modules, videos, written guides, newsletters, and pamphlets to support parents in managing their children’s screen use (Anderson et al., 2016; Andrade et al., 2015; Apisitwasana et al., 2018; Babic et al., 2016; Catenacci et al., 2014; De Lepeleere et al., 2017; Krossbakken et al., 2018; Leme et al., 2018; B. Li et al., 2019; Moller et al., 2012; Moreno et al., 2021; Morgan et al., 2022; Robinson et al., 2010; Scull et al., 2019; J. J. Smith et al., 2014). The content of the sessions and materials often focussed on building parental knowledge and awareness around screen time recommendations, consequences of excessive screen time, reducing screen time and exposure to inappropriate media, and strategies for critical viewing and protecting children online (Anderson et al., 2016; Andrade et al., 2015; Apisitwasana et al., 2018; Babic et al., 2016; Catenacci et al., 2014; De Lepeleere et al., 2017; Krossbakken et al., 2018; Leme et al., 2018; B. Li et al., 2019; Moller et al., 2012; Moreno et al., 2021; Morgan et al., 2022; Robinson et al., 2010; Scull et al., 2019; J. J. Smith et al., 2014). Some interventions included parent-child interactive homework activities, such as replacing screen time with healthy alternatives like physical activity (Anderson et al., 2016; Leme et al., 2018; B. Li et al., 2019; Z. Liu et al., 2022; Moller et al., 2012; Morgan et al., 2022; Scull et al., 2019; Vanderhoven et al., 2016; Xu et al., 2015), while others supported parental monitoring by guiding parents to oversee children’s adherence to screen time goals and self-regulation practices and providing feedback (Apisitwasana et al., 2018; Cheng et al., 2024; B. Li et al., 2019; Z. Liu et al., 2022; Moller et al., 2012; Morgan et al., 2022; Robinson et al., 2010; Straker et al., 2013). Family agreements and changes to home environment were emphasised in a few interventions, such as creating screen-free zones, replacing devices with traditional games, media-free weekends, and setting household media rules (Babic et al., 2016; Cheng et al., 2024; Moller et al., 2012; Pedersen et al., 2022; Scull et al., 2019; Straker et al., 2013). In addition, there were also community events like family fun nights and after-school activities (Morgan et al., 2022; Robinson et al., 2010; Xu et al., 2015).
Component Analyses Results
An ICA of 15 studies of effective interventions that met quality criteria identified 17 components related to screen use, which were broadly categorised as either individual-focussed or family-focussed (Supplemental Table S2). These components were further evaluated for their consistency to understand how each was linked to positive outcomes (Table 2). Notably, four individual-focussed components consistently appeared among effective, moderate, and high quality studies (High consistency (Y) ≥0.6), such as structured classroom lessons on screen use and healthy lifestyle (Andrade et al., 2015; Apisitwasana et al., 2018; Babic et al., 2016; Leme et al., 2018; Z. Liu et al., 2022; Moller et al., 2012; J. J. Smith et al., 2014; Vanderhoven et al., 2016; Xu et al., 2015); screen-use related self-paced or teacher-distributed materials for children (Andrade et al., 2015; Apisitwasana et al., 2018; Cheng et al., 2024; Leme et al., 2018; B. Li et al., 2019; Z. Liu et al., 2022; Moller et al., 2012; Morgan et al., 2022; Scull et al., 2019); interactive activities that engaged adolescents in learning objectives and managing screen use (Andrade et al., 2015; Apisitwasana et al., 2018; Babic et al., 2016; Cheng et al., 2024; Leme et al., 2018; B. Li et al., 2019; Moller et al., 2012; Morgan et al., 2022; Scull et al., 2019; Vanderhoven et al., 2016; Xu et al., 2015); educational content on building knowledge and awareness on potential benefits and consequences of screen use for children (Andrade et al., 2015; Apisitwasana et al., 2018; Babic et al., 2016; Cheng et al., 2024; Leme et al., 2018; B. Li et al., 2019; Z. Liu et al., 2022; Moller et al., 2012; Morgan et al., 2022; Scull et al., 2019; J. J. Smith et al., 2014; Vanderhoven et al., 2016; Xu et al., 2015). Similarly, two family-focussed components showed high consistency, such as written and digital informative materials for parents on screen use (Andrade et al., 2015; Apisitwasana et al., 2018; Babic et al., 2016; Leme et al., 2018; B. Li et al., 2019; Moller et al., 2012; Morgan et al., 2022; Scull et al., 2019; J. J. Smith et al., 2014) and sessions focussing on educational content on knowledge, awareness on benefits and consequences of screen use in children (Andrade et al., 2015; Apisitwasana et al., 2018; Babic et al., 2016; Leme et al., 2018; B. Li et al., 2019; Z. Liu et al., 2022; Moller et al., 2012; Morgan et al., 2022; Scull et al., 2019; J. J. Smith et al., 2014; Vanderhoven et al., 2016).
Truth table for ICA and QCA with components and consistency values.
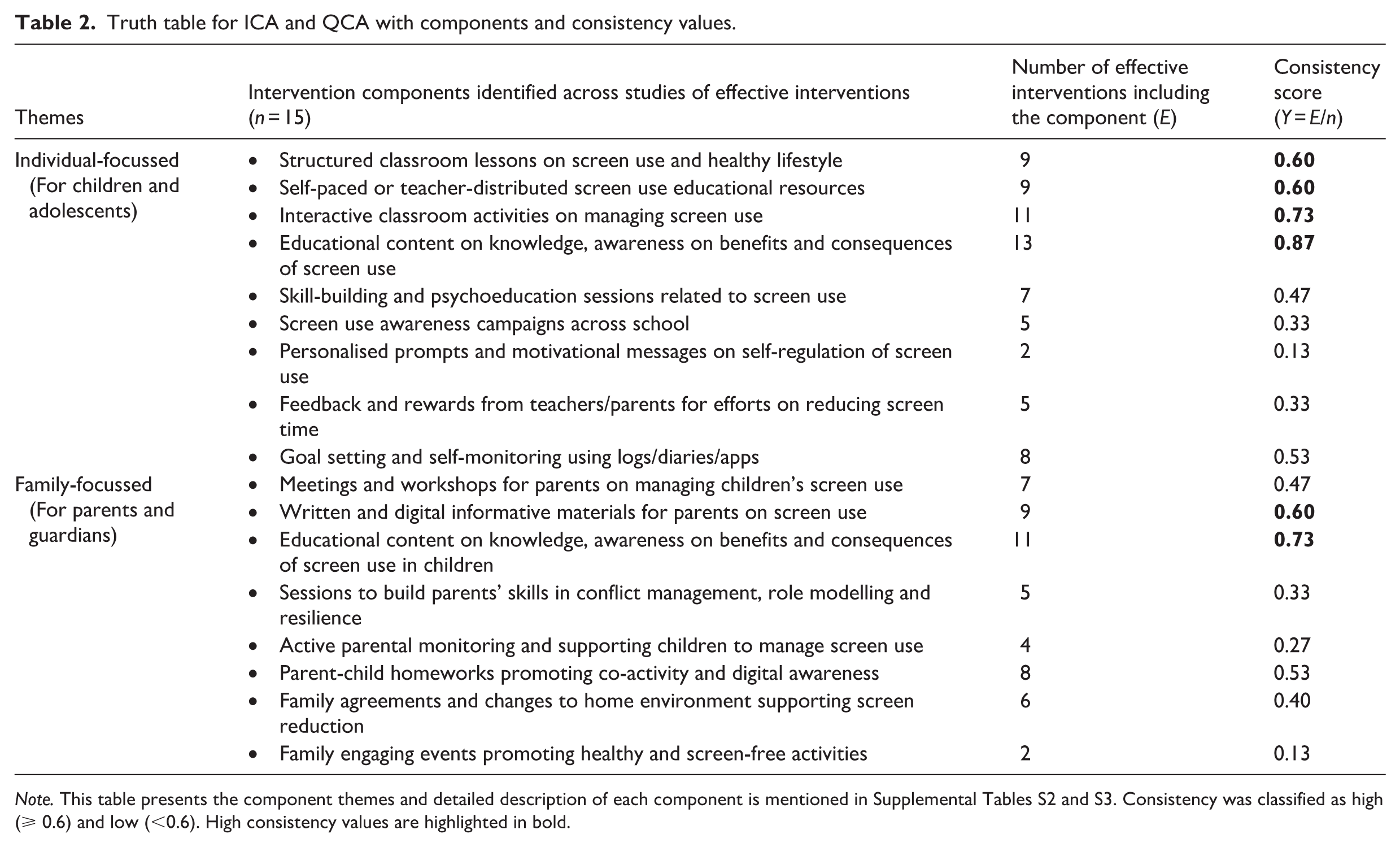
Note. This table presents the component themes and detailed description of each component is mentioned in Supplemental Tables S2 and S3. Consistency was classified as high (⩾ 0.6) and low (<0.6). High consistency values are highlighted in bold.
Building on ICA, QCA identified minimised pathways from the six components with high consistency (Table 3). Successful individual-focussed components incorporated classroom lessons, self-paced or teacher-distributed educational resources and content on knowledge, awareness and tips to manage screen use (Pathway P1), while effective family-focussed components utilised informative materials and educational content enhancing knowledge and awareness on screen use in children (Pathway P2). Given the high consistency of components, and implementing these findings to get significantly positive outcomes, the integrated theoretical model (M) proposes that combining both individual (P1) and family (P2) components optimises intervention effectiveness, ensuring a more contextual and impactful approach to manage discretionary screen use. This pathway configuration highlights that an intervention containing both P1 and P2 configuration may ensure a significant outcome.
Minimised pathways to effective interventions.
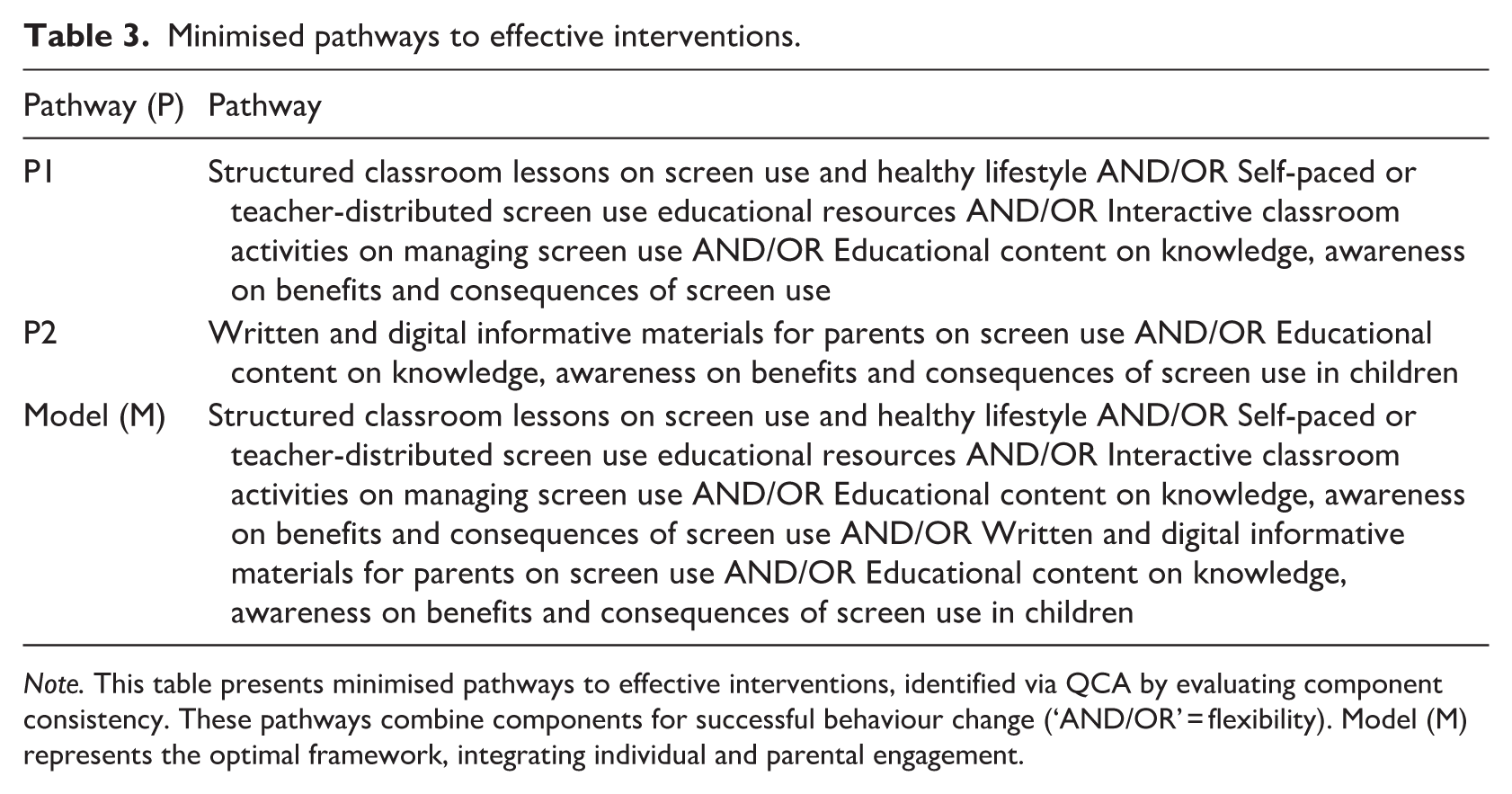
Note. This table presents minimised pathways to effective interventions, identified via QCA by evaluating component consistency. These pathways combine components for successful behaviour change (‘AND/OR’ = flexibility). Model (M) represents the optimal framework, integrating individual and parental engagement.
Discussion
This review employed a multi-method approach, including a qualitative synthesis of the findings of studies, meta-analysis to evaluate the effectiveness of family-based interventions and component analyses of effective studies for managing discretionary screen use among school-aged children and adolescents. Findings from meta-analysis suggest that family-based interventions are associated with a small and statistically significant reduction in total screen time. Unlike previous reviews that primarily focussed on reducing screen time, this review also included interventions focussing on the content, context, and interactions of screen use. Importantly, this review adds to the growing body of literature by demonstrating that multi-component family-based interventions, incorporating individually-focussed components aligned with behaviour change techniques (e.g. shaping knowledge, natural consequences, and action planning) and active parental involvement are consistently effective in managing screen use (Michie et al., 2013).
The meta-analysis showed that family-based interventions led to a small but statistically significant reduction in total screen time. In contrast, reductions in television, computer, and gaming time were non-significant, which is likely due to limited number of studies available for these outcomes (n = 4), small sample sizes and variability in how outcomes were measured. This finding suggests that while family-based interventions can lead to a small and statistically significant reduction in total screen time, their effectiveness may be limited when targeting specific screen activities (Giraudeau et al., 2022). When contextualised using typical variability in screen time reported across included studies, this effect likely corresponds to only a modest absolute reduction in daily screen time, around 7 to 13 min/days. Such a change may have limited clinical significance at the individual level; however, even small reductions may be meaningful at a population level or when sustained over time (Oh et al., 2022; Wu et al., 2016). Caution is warranted when interpreting publication bias, as the number of studies available was fewer, limiting the reliability of funnel plots and Egger’s test.
Although the included studies addressed diverse aspects of screen use, such as reducing violent media exposure, promoting critical viewing, improving family media routines, or awareness towards cyberbullying and problematic use, the meta-analyses focussed on screen duration outcomes. This restriction was due to limited, inconsistent, and heterogeneous outcomes, which made quantitative pooling unfeasible. Emerging evidence suggests that the health implications of screen use are shaped not only by duration, but also by what content is accessed and the context and purpose of use (Canadian Paediatric Society, 2019). Accordingly, the small reductions observed in screen time should be interpreted carefully, as changes in duration alone may not fully capture meaningful improvements in screen-related behaviours.
To identify key components consistently linked with intervention success, ICA and QCA were conducted on 15 effective interventions. Seventeen intervention components focussing on individual and family levels were identified. Effective family-based interventions tended to adopt multi-component approaches, integrating educational, self-regulatory, and family-support elements rather than relying on one strategy. Common features included structured learning activities, interactive engagement, and informational materials for adolescents and parents, which targeted shaping knowledge, building awareness of consequences, action planning, and social support (Michie et al., 2009). Consistent with existing research highlighting the importance of parental involvement and family support in adolescent behaviour change (Arundell et al., 2020; Nielsen et al., 2019), our findings also suggest that interventions, grounded in social cognitive and self-determination theories, are effective in modifying screen behaviours by emphasising self-regulation, motivation, and social support (Bandura, 1986; Ryan & Deci, 2017). To ensure broad impact, context-specific interventions integrating these theoretical components should be designed and rigorously tested across diverse populations and settings to determine their scalability and sustainability in promoting healthy screen behaviours.
Among the studies with acceptable rigour, some behavioural interventions (n = 6) did not lead to significant changes in screen use behaviours, which may be due to several factors. Limited parental engagement was present in some unsuccessful interventions, suggesting that programmes relying solely on schools may be less effective in reinforcing behaviour change at home (Krossbakken et al., 2018; Robinson et al., 2010). However, several effective interventions also had minimal parental involvement, indicating that this factor alone does not account for differences in effectiveness. Similarly, some ineffective interventions were brief in duration (less than 6 weeks) and lacked follow-up mechanisms, which may have allowed participants to revert to previous habits, thereby decreasing effectiveness (De Lepeleere et al., 2017; Krossbakken et al., 2018; Moreno et al., 2021).
In some cases, interventions that targeted multiple lifestyle behaviours (e.g. obesity, diet, and physical activity) along with screen time often diluted their effectiveness, reducing their effect on screen time specifically (Anderson et al., 2016; Catenacci et al., 2014; De Lepeleere et al., 2017; Robinson et al., 2010), though this pattern was also not universal among unsuccessful interventions. The reliance on self-reported screen use measures introduced potential recall bias and measurement inconsistencies across the major body of research (Anderson et al., 2016; De Lepeleere et al., 2017; Krossbakken et al., 2018; Moreno et al., 2021; Robinson et al., 2010), affecting both effective and ineffective studies equally and therefore limiting conclusions about differential effectiveness. These methodological limitations suggest that other unmeasured factors, such as retention rates, presence or absence of long-term follow-up, and feasibility may explain the observed differences in intervention outcomes.
Strengths, Limitations, and Future Directions
The key strength of this review is its rigorous methodology, which included a comprehensive search strategy, a focussed examination of family-based interventions, and the systematic identification of effective and consistent components using ICA and QCA. This integrated approach provided a structured framework for understanding how individual and family factors interact in screen use interventions, thereby supporting the development of more targeted and evidence-based strategies. The predominance of school-based interventions with a family component underscores the importance of school–family partnerships in achieving positive screen use outcomes among young people. Parents of school-aged children who exceeded screen time recommendations were found to have low self-efficacy in managing screen use, underscoring the need for greater support for parents (B. J. Smith et al., 2010). This work offers effective strategies for families, schools, and practitioners to managing screen use in this age group.
However, several limitations should be considered when interpreting the findings. Although statistical heterogeneity was low, variability remained in how screen time outcomes were operationalised across studies, with differences in self-report instruments, presence of significant publication bias, and overlap in intervention components (e.g. structured classroom lessons vs. interactive classroom activities for adolescents on managing screen use) may introduce measurement bias. Meta-analyses of four screen types were chosen because they were most consistently reported across the included studies. While outcomes such as smartphone use, social media use, and broader digital behaviours are of increasing relevance, they were less frequently measured, restricting comparability across studies. In addition, many studies could not be included in the meta-analysis because of high risk of bias and inconsistent outcome reporting, underscoring the need for interventions with stronger methodological rigour. The reliance on self-reported screen time is prone to recall and social desirability bias, and the concentration of studies in high-income settings further constrain the generalisability of findings.
Most included studies focussed on reducing screen time with limited evidence addressing content, context, and interactions, leaving gap in understanding strategies that holistically promote behaviour change (Griffith et al., 2024). In this review, although interventions were coded across these domains, content-, context-, and interaction-related outcomes were infrequently assessed and inconsistently operationalised, precluding quantitative synthesis beyond time-based outcomes. Furthermore, while this review focussed on family-based interventions, it also included predominantly school-based interventions that incorporated a family component. The extent and nature of family involvement varied substantially across studies, ranging from passive recipient of information to more active parental engagement, and could not be disentangled from other intervention components in the analyses. As a result, the findings reflect the effectiveness of multi-component interventions that include some level of family involvement, rather than the independent effect of family involvement itself. Subgroup analyses by age group, parent versus child-reported outcome, home versus school-based studies or study design were not conducted due to few studies, limiting exploration of potential differential effects across these characteristics. Another limitation of this review is that the literature searches were conducted more than 12 months prior to publication, therefore it is possible that some more recent relevant studies may not have been captured in the search. Also, restricting inclusion to English-language publications may have narrowed the evidence base and underrepresented findings from non-English speaking countries.
Future research should extend investigations into low- and middle-income countries and implement device-based measures to enhance measurement accuracy. Alternative approaches to self-reported screen use include ecological momentary assessment (EMA), device-generated usage logs, and passive tracking tools, which offer greater temporal accuracy and reduced recall bias but are limited by participant burden, privacy, and ethical concerns (Beynon et al., 2024). Furthermore, needs assessments and participatory approaches (adolescents, parents, and educators) should be prioritised to ensure interventions align with adolescents’ and parents’ perspectives (M. R. Sanders & Kirby, 2012). Long-term studies with extended follow-ups are also essential for ensuring sustainable, large-scale implementation. Also, the scope of managing screen use is broad and not well defined, and future studies may try to establish what constitutes ‘healthy screen use’ (Canadian Paediatric Society, 2019; Kaye et al., 2020). Policymakers and public health researchers should collectively develop a framework to define healthy screen use as guided by the Canadian Paediatric Society statement, test combinations of individual- and family-focussed components to empower families and manage adolescents’ screen use.
Implications for School Psychologists/Counsellors
For school-based professionals, these findings suggest a potential role in supporting family-inclusive approaches to healthy screen use within existing well-being frameworks. Rather than focussing solely on reducing screen time or restricting device access, school counsellors may support educational and awareness-raising strategies that encourage meaningful screen use and facilitate communication between adolescents and parents around shared expectations. Strong school–family partnerships may support behaviour change by enabling consistent messaging and reinforcement across school and home environments, which may help school-aged children and adolescents adopt and maintain healthy screen practices (Throuvala et al., 2020).
Conclusion
This review identified that family-based interventions offer promise in reducing total screen time and key components associated with successful outcomes for managing discretionary screen use in school-aged children and adolescents. Effective child-focussed strategies include structured education through classroom lessons, interactive activities, and resources that support behaviour change, skill development, and awareness of screen use consequences. Parent-directed strategies should prioritise informative materials and practical parenting tips aligned with the child’s learning content. Interventions that integrate both school-based education and parent-focussed components appear most promising, underscoring the critical role of schools as delivery platforms and families as reinforcement agents in empowering adolescents to develop healthy digital habits. These insights are particularly relevant for school counsellors, educators, and policymakers seeking collaborative approaches that bridge school and home environments. However, few interventions independently addressed the content, context, or interactions of screen use, indicating a gap for future research. To improve intervention quality and generalisability, future studies should adopt standardised outcome measures, incorporate objective tracking tools to reduce self-report bias, and include more diverse socioeconomic and cultural contexts.
Supplemental Material
sj-docx-1-spc-10.1177_20556365261423543 – Supplemental material for Family-Based Interventions for Managing Screen Use in Children and Adolescents: Systematic Review, Meta-Analysis, and Intervention Component Analysis
Supplemental material, sj-docx-1-spc-10.1177_20556365261423543 for Family-Based Interventions for Managing Screen Use in Children and Adolescents: Systematic Review, Meta-Analysis, and Intervention Component Analysis by Anjana Rajagopal, Mehwish Nisar, Alina Morawska, Elizabeth J. Edwards and Asaduzzaman Khan in Journal of Psychologists and Counsellors in Schools
Footnotes
Acknowledgements
Special thanks are extended to Marcos Riba, Librarian at The University of Queensland, for his assistance with the literature search terms.
Author Contributions
Anjana Rajagopal contributed to the conceptualisation, investigation, methodology, software, formal analysis, data curation, visualisation, and writing – original draft. Mehwish Nisar contributed to validation, data curation, formal analysis, and writing – review and editing. Alina Morawska contributed to conceptualisation, methodology, writing – review and editing, and supervision. Elizabeth J. Edwards contributed to conceptualisation, methodology, writing – review and editing, and supervision. Asaduzzaman Khan contributed to conceptualisation, methodology, writing – review and editing, and supervision. All authors have read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Protocol Registration
PROSPERO #CRD42023414857.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.