
Abstract
This study investigated the effect of mindfulness-based cognitive therapy (MBCT) on mathematics anxiety among students in Nigerian secondary schools. Eighty-six senior secondary class one students (aged 15–16 years) participated, comprising 43 students allocated to the experimental group and 43 students allocated to the control group. Mathematics anxiety was measured using the Mathematics Anxiety Rating Scale (MARS). The experimental group participated in a MBCT intervention, whereas the control group underwent conventional counselling. Both conditions lasted 6 weeks and included 12 sessions, 90 min each. Results revealed that MBCT reduced students’ mathematics anxiety from pre- to post-test, and the effect remained consistent at follow-up, compared to the control group. One of the recommendations was that teachers should be trained in applying MBCT to anxious mathematics students to remove the fear response of mathematics.
Introduction
In Nigeria, students’ performance in external examinations, such as the West Africa Examination Council (WAEC) in mathematics, has not been encouraging (Mosimege & Egara, 2023). WAEC Chief Examiners’ Reports indicated students’ poor achievement in mathematics, especially in areas involving geometry and word problem-solving (WAEC, 2018). Factors responsible for students’ poor performance in mathematics may be pedagogical, economic, social or psychological or a combination of these factors (Evans et al., 2019). Previous studies on the causes of students’ poor performance in mathematics have focussed mainly on pedagogy (Nzeadibe et al., 2019; Okeke, Egara, Orga, & Chinweike, 2023; Okeke, Egara, Orga, & Nzeadibe, 2023; Onu et al., 2012; Osakwe, Egara, Inweregbuh, Nzeadibe, & Emefo, 2023; Osakwe, Egara, Inweregbuh, Nzeadibe, Okeke, et al., 2023); and psychological factors such as depression, feelings of inferiority, blushing, anger, worry, stress and anxiety (Asikhia, 2014). The present study focussed on mathematics anxiety as a primary cause of poor mathematics outcomes and its treatments for improving performance.
Mathematics anxiety is a complex psychological construct that involves responses associated with a lack of confidence, a threat to self-ability and low self-esteem towards mathematics tasks/concepts. Mathematics anxiety involves feelings of fear, tension and apprehension that many students experience when solving mathematical tasks (Ashcraft, 2002; Sarfo et al., 2020, 2022). Teachers must understand mathematics anxiety because it can negatively impact students’ learning (Soumen & Susanta, 2018). Therefore, mathematics anxiety should be considered when examining students’ problems in mathematics because it interferes with manipulating numbers and solving mathematical problems in ordinary life and academic situations (Alam & Halder, 2018). According to Mollah (2017), poor test results, unfavourable classroom experiences, a lack of willingness to complete tough assignments and a negative attitude towards mathematics learning all contribute to mathematics anxiety. Other causes of students’ anxiety in mathematics include the attitude and behaviour of mathematics teachers, boredom, learning difficulty, societal attitude, lack of adequate resources, tests and examinations and lack of confidence towards mathematics (Sule, 2017).
There are physical, psychological and behavioural indicators associated with mathematics anxiety (Mollah, 2017). Physically, anxiety is associated with an increased heartbeat, sweaty hands, light-headedness and stomach upset. Psychological symptoms include problems with concentration, helplessness, disgrace and worry. Behavioural symptoms include avoidance of mathematics classes, ignoring homework until the last moment and irregular study (Plaisance, 2009). Mathematics anxiety symptoms may occur through exposure to problematic situations or sometimes merely through thinking about the subject or situation when engaged in learning. Numerous psychological therapies have been designed to reduce anxiety, including systematic desensitisation, stress inoculation training, rational emotive behaviour therapy, cognitive behavioural therapy, acceptance and commitment therapy and mindfulness-based cognitive therapy (MBCT) (Egara, 2021). The MBCT is of interest in the current study.
MBCT is a psychotherapy introduced by Segal, Williams and Teasdale in the 1990s. MBCT is used to modify an individual’s perceptions, thoughts and behaviours to influence emotions positively. Its basic concept is that a person’s mood is inextricably linked to their cognitive processes (Egede, 2015). Operationally, MBCT is a psychological intervention that regulates students’ fear of failure and anxiety over cognitive tasks and subsequently reduces or eliminates anxiety. It aims to help people transform negative thoughts and behaviours by presenting more positive and gratifying alternatives. MBCT can help students to be attentive to their environment, recognise negative thought patterns, assess their validity and replace them with healthier alternatives. One of the foremost characteristics of MBCT is its realistic approach to changing behaviour rather than altering personality dynamics (Cairns, 2013).
MBCT uses the foundation of mindfulness-based theory and integrates cognitive strategies to ‘help patients achieve affective self-regulation through the development of mindful attention’ (Semple et al., 2010, p. 222). Specifically, the Decontextualising Model of Mindfulness (DMM) suggests that mindfulness techniques operate to decontextualise mental events from their web of hierarchically organised levels of abstraction and associated meaning, which opens up the cognitive ‘space’ to introduce more adaptive strategies (White, 2014). Maladaptive appraisal of mathematics learning experiences, which was suggested as a main cause of mathematics anxiety, is closely linked to maladaptive self-centeredness and dispositional mindfulness (David et al., 2022). MBCT has been shown to positively impact academic success, as the core of mindfulness is to increase awareness and regulation specific to emotions (Erisman & Roemer, 2010; Gratz & Roemer, 2008). Furthermore, emotion regulation has positively impacted grade point averages, standardised test scores, school adjustment and pro-social skills in students (Eisenberg et al., 2010; Rapp-Paglicci et al., 2011; Weinberg & Klonsky, 2009).
MBCT has been effective in treating some psychological factors, such as depression (Kaviani et al., 2012) and anxiety, including the symptoms of social anxiety disorder (Carlton et al., 2020; Semple et al., 2010; Strege et al., 2018). MBCT has also been effective in reducing mathematics anxiety. For instance, Samuel et al. (2022) investigated the mindfulness and growth mindset approach for reducing mathematics anxiety among college students in various STEM-related courses in the USA. The study used a sample of 102 college students with a mean age of 18 years. The intervention was delivered by teachers of the STEM-related courses that lasted one semester. Their findings revealed that the mindfulness intervention and the growth mindset approach significantly decreased the mathematics anxiety of the students in the experimental group compared to their control counterparts. Similar results were found by Pinthong (2018) with college students in the USA. Pinthong determined the effect of a mindfulness-based intervention on reducing mathematics anxiety among college students. However, the mindfulness-based intervention lacked the cognitive components of MBCT.
Lague et al. (2019) investigated the effect of MBCT on mathematics anxiety in three grade 8 and 9 high school students in the USA. The study used a simple case study design. A professional guidance counsellor administered the MBCT intervention for 6 weeks. They found that MBCT effectively reduced mathematics anxiety among the students. Henderson (2019) explored the impact of a mindfulness-based intervention on primary school children with mathematics anxiety in England. However, the mindfulness-based intervention also lacked the cognitive components of MBCT. The study sample had 184 primary school children between 8 and 9 years. The class teachers administered the mindfulness-based intervention for 6 weeks. The data revealed that children who received the mindfulness-based intervention reported reduced mathematics anxiety compared to controls.
While these existing studies provide promise for MBCT to reduce mathematics anxiety, they are not without some limitations. Some studies utilised quasi-experimental, repeated measures designs (e.g. Henderson, 2019; Samuel et al., 2022); to date, no study has reported using a randomised controlled trial. Most of the studies used the students’ regular teachers to deliver the mindfulness-based intervention rather than counselling professionals, which may have jeopardised the fidelity of the MBCT programme. Furthermore, none of the studies reported the intervals between pre- and post-test or follow-up.
The current study deployed a randomised controlled design, which included random allocation to the experimental and control conditions. The MBCT intervention was administered by qualified counsellors/therapists and delivered for 6 weeks (see Burgess et al., 2021; Henderson, 2019; Lague et al., 2019; Pots et al., 2014). Data was collected a week before the first treatment session, that lasted for 6 weeks; post-test data was collected in the seventh week, while the follow-up data was collected twelve weeks after post-test data collection. This is the first study that we know of that has applied MBCT in reducing mathematics anxiety among school students in Nigeria. We hypothesised that participants in the MBCT experimental group would report decreased mathematics anxiety at post-treatment and follow-up compared to the control group who received conventional counselling.
Methods
Participants
One hundred and fifty senior secondary students (aged 15–16 years) showed interest in participating in the study. Out of the 150 students, after eligibility screening, only 86 students met the eligibility criteria. The researchers’ eligibility criteria were that: (1) participants must be secondary school students in senior secondary class one from Nsukka Education Zone; (2) the students must show symptoms of mathematics anxiety, that is, students with a score ⩾50 on the MARS were considered to have mathematics anxiety. Volunteers who did not match the eligibility requirements were not chosen. The 86 participants who met the eligibility criteria comprised 44 males and 42 females. The sample size for this research was calculated using G*Power 3.1 software (Faul et al., 2007) based on the following parameters: effect size f = 0.25, alpha (
Demographic characteristics of the students (Within-group analysis).
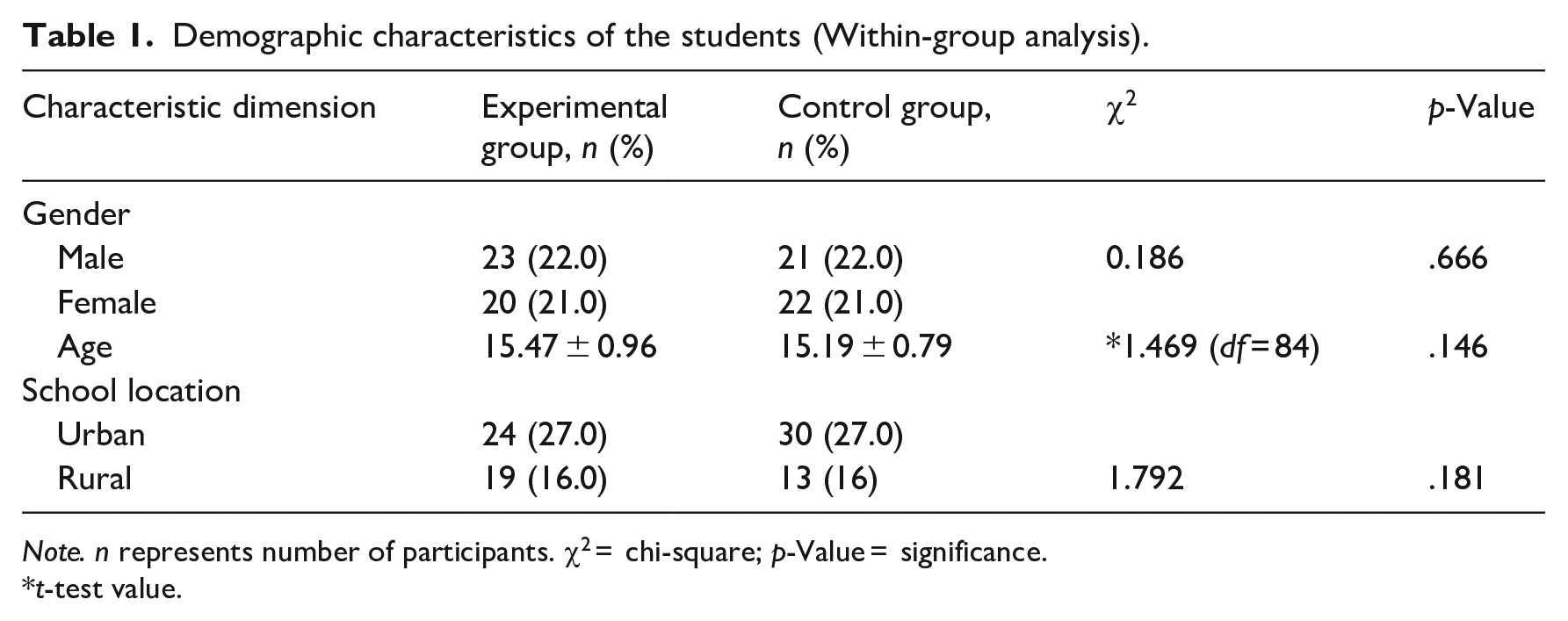
Note. n represents number of participants. χ2 = chi-square; p-Value = significance.
t-test value.
Measures
Mathematics Anxiety Rating Scale (MARS)
The MARS used in this study was adapted from the Mathematics Anxiety Scale developed by Zakariya (2018). The MARS has 4-point response options of Strongly Agree, Agree, Disagree and Strongly Disagree. It consists of 20 items and is assigned a weight of 1, 2, 3 and 4 points. Participants indicated their response on a 4-point scale, showing their degree of agreement or otherwise to each statement. For example, participants who scored the item ‘I hate mathematics because it is a difficult subject’ whether high or low scores mean high or low mathematics anxiety. The adequate screening cut-off set for the study was 50, which was determined using the Angoff method of obtaining the average score (Sarkın & Gülleroğlu, 2019). This means that students with a score ⩾50 were considered to have mathematics anxiety. For the present study, Cronbach’s alpha was .79, suggesting good internal consistency.
Procedure
Ethical statement
The Faculty of Education Research Ethics Committee, University of Nigeria (REC/UNN/2019/00024) approved this study. Schools granted gatekeeper permission to the researchers to carry out the research. The parents of eligible students also provided informed consent. The secondary school students also provided informed assent. Data were collected in three separate stages, namely, the pre-test stage, post-test stage and follow-up stage.
Pre-test
Of the 150 students who expressed interest in participation, 86 students scored ⩾50 on the MARS (i.e. considered to have mathematics anxiety) and were randomly assigned to either the experimental or control group. The researchers addressed the participants of both groups about the reason for the programme (i.e. to assist with managing their anxiety towards mathematics) and the need for them to feel free to ask questions.
Intervention
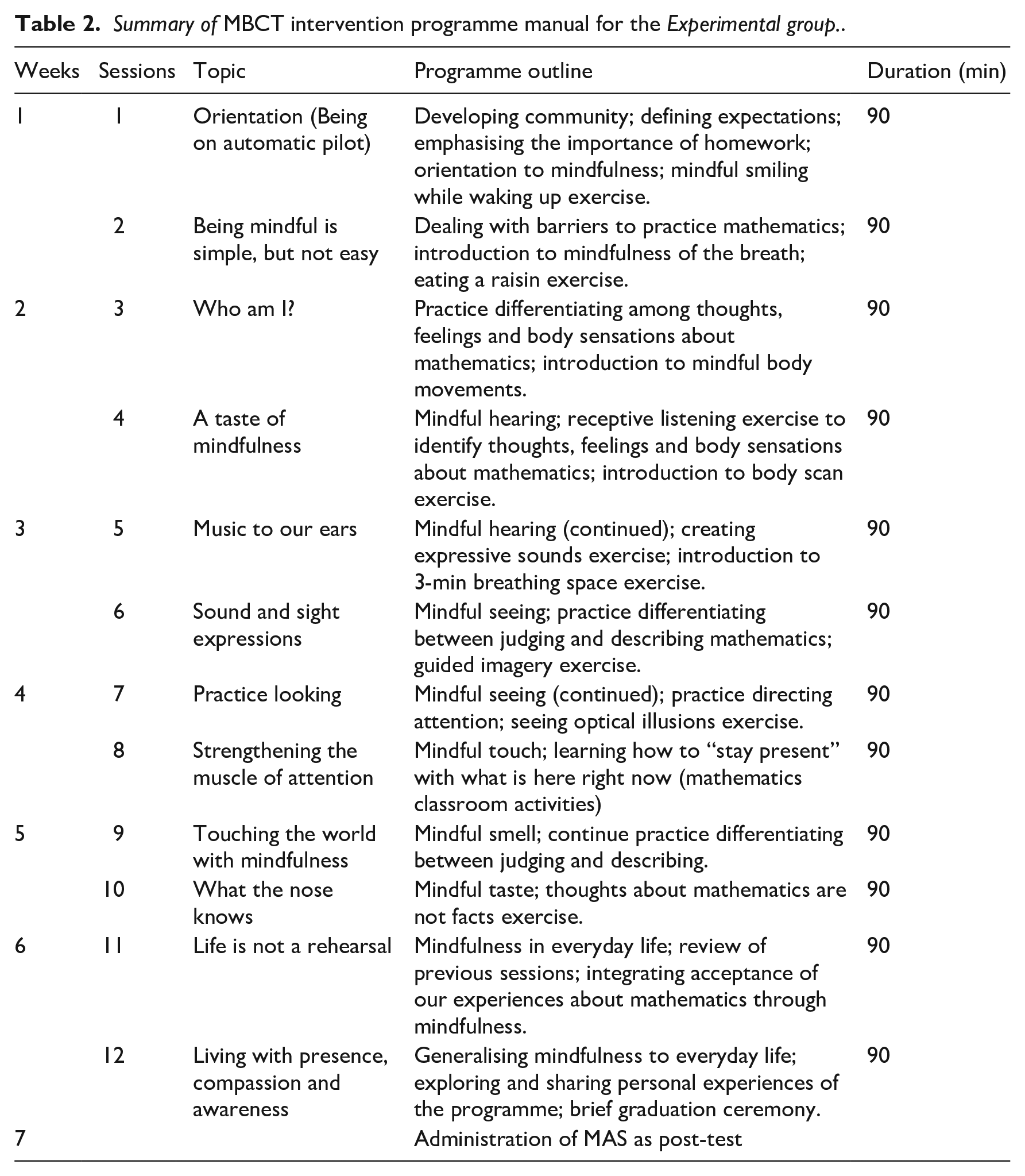
The experimental and control groups were subjected to 12 sessions (twice per week) of 90 min each for 6 weeks. The programmes for both groups were conducted after school hours to ensure full participation and commitment. For the experimental group, participants completed an MBCT intervention. The MBCT consists of four stages: assessment, cognitive, behaviour and learning (Dimidjian & Segal, 2015). During the assessment stage, the therapist and the students familiarised themselves with each other, and the pre-test was conducted. In the cognitive stage, the therapist and the students worked together to understand the students’ thoughts. They spent time together discussing past events that made the students think the way they did. During the behaviour stage, the students and the therapist collaborated to develop new thought patterns and behaviours, such as using mathematics in teaching. In the final learning stage, students and the therapist worked together to ensure the changes to students’ behaviour were permanent. The MBCT programme was adapted from Semple and Lee (2014). The MBCT programme included a specific theme for each session that focussed on the following: Being on automatic pilot; Being mindful is simple but not easy; Who am I?; A taste of mindfulness; Music to our ears, sound expressions; Practice looking; Strengthening the muscle of attention; Touching the world with mindfulness; What the nose knows; Life is not a rehearsal; Living with presence, compassion and awareness; A recap and evaluation of the entire programme. The contents of each session were supported by Socratic questioning and homework. Each session began with a recap of the previous session, followed by a brief discussion of the homework and an explained agenda of the current session and warm-up activities. Finally, sessions were rounded up by summarising and giving feedback. The activities of the MBCT intervention and how 12 sessions were allocated throughout 6 weeks are shown in Table 2. For the control group, participants completed conventional counselling sessions focussed on the following: orientation concerning study habits to reawaken the essence of reading and studying; independent study, peer learning, group discussion and searching for relevant information online; how to scan through the examination questions, picking the questions that participants are conversant with, answering questions with confidence; anxiety and causes of math anxiety among students; how to manage anxiety before answering any math exam questions; optimising the time given to answer questions and reading through the questions answered before submitting papers.
Summary of MBCT intervention programme manual for the Experimental group..
Post-test
The post-test was done a week after the last session (Time 2) with both groups. Participants completed the MARS, the same instrument used for the pre-test; however, the items in the instrument were reshuffled during the post-test to make it look parallel to the pre-test items.
Follow-up
The MARS was administered again (Time 3) as a follow-up after 12 weeks of the treatment programme for participants in both groups.
Data analyses
Statistical Package for Social Sciences (SPSS) version 23 was used for the analyses. Mauchly’s test of sphericity was used to test the assumption of the sphericity of test statistics. The effect of MBCT was analysed using a mixed between-within analysis of variance (ANOVA). The data were analysed using a 2 × 3 mixed design that considered Group (Experimental; MBCT vs. Control; Counselling) as a between groups factor and Time (pre-test vs. post-test vs. follow up) as the within groups factor. Partial η2 value was reported as a measure of the effect size. Following the convention, a small effect size: >0.01, medium effect size >0.06 and large effect size >0.14 (Cohen, 1988).
Results
The result reveals the students who were exposed to MBCT to have a pre-test mean score of 55.28 (SD = 12.70) and a post-test mean score of 41.14 (SD = 10.04) and a follow-up mean score of 32.00 (SD = 12.24). The students that were exposed to conventional counselling had a pre-test mean score of 55.16 (SD = 15.39) and a post-test mean score of 55.65 (SD = 14.20) and a follow-up mean score of 55.47 (SD = 14.38). The mean difference of the pre-test, post-test and follow-up of the groups were 0.12, 14.51 and 23.47, respectively.
The results for secondary school students’ mathematics anxiety (Greenhouse-Geisser corrected) revealed a significant effect of Group (G) [F(1, 84) = 28.504, p < .001, η2p = .253], Time (T) [F(1.663, 139.66) = 34.134, p < .001, η2p = .289] and Time by Group interaction (G × T) [F(1.663, 139.66) = 25.201, p < .001, η2p = .301] (see Figure 1). Results of the follow-up analysis show that the effect of MBCT treatment on secondary school students’ mathematics anxiety scores in the treatment group remained consistent [F(1, 83) = 77.670, p < .001, η2p = .527, ∆R2 = .515].
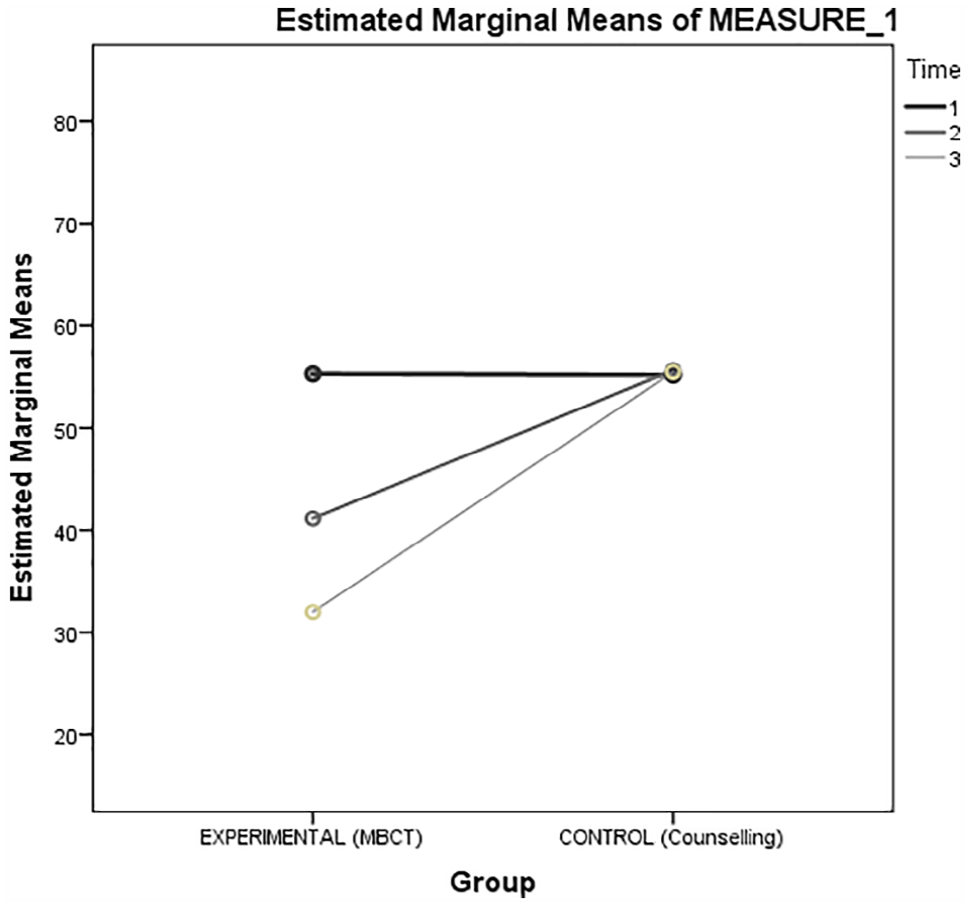
Time × Group interaction effect.
Pairwise comparisons (Sidak corrected) regarding the main effect of the group revealed that the secondary school students in the MBCT group demonstrated lower mathematics anxiety than secondary school students in the control group (mean difference = −12.620, SE = 2.36, p < .001, 95% CI [−17.321, −7.920]). In addition, the pairwise comparisons (Sidak corrected) regarding the main effect of Time revealed a significant decrease in secondary school students’ mathematics anxiety scores from pre-test to post-test (mean difference = −6.826, SE = 1.08, p < .001, 95% CI [−9.447, −4.204]), and from pre-test to follow-up (mean difference = 11.488, SE = 1.64, p < .001, 95% CI [7.501, 15.476]). Likewise, the significant decrease in students’ mathematics anxiety scores from post-test to follow-up was consistent (mean difference = 0.4.663, SE = 1.43, p < .001, 95% CI [1.190, 8.136]).
Discussion
We hypothesised that participants in the MBCT intervention group would report decreased mathematics anxiety at post-treatment and follow-up compared to the control group who received conventional counselling. Our data revealed that the effect of MBCT among secondary school students was significant, with evidence of reduced mathematics anxiety scores for students in the experimental group compared to those in the control group. Our findings suggest that 12 sessions of MBCT effectively reduce mathematics anxiety among school students, that is, reducing irrelevant thought patterns, tension and worries about mathematics. It is, therefore, likely that students with greater mindfulness can better manage mathematics anxiety-producing situations.
Our results correspond with Samuel et al. (2022) and Pinthong (2018) who also found MBCT and mindfulness-based intervention, respectively, effective in reducing mathematics anxiety among college students compared to their control group counterparts. Our results also support the findings of Lague et al. (2019) and Henderson (2019) who investigated the effects of MBCT and mindfulness-based intervention (respectively) on mathematics anxiety of school students and revealed that the interventions effectively reduced mathematics anxiety in the experimental group more than the control group. Given that these studies have shown positive results with college students (Pinthong, 2018; Samuel et al., 2022) and secondary school students (Henderson, 2019; Lague et al., 2019), in USA (Lague et al., 2019; Pinthong, 2018; Samuel et al., 2022) and England (Henderson, 2019), combined with our work with secondary school students in Nigeria, we conclude that MBCT is considered helpful for reducing the issue of mathematics anxiety among school students.
While the randomised controlled design was a strength of the current work, there was one weakness worth noting. We only included students in senior secondary one class (same year level). Therefore, future studies could examine whether MBCT is an effective treatment for mathematics anxiety across other secondary year levels, that is, determine whether our results are generalisable.
Educational implications
The results of the current study have some obvious educational implications for mathematics teachers, school counsellors and government agencies. The study provided empirical evidence of the effectiveness of MBCT in reducing mathematics anxiety among secondary students. Mathematics teachers could be encouraged to assist students who are mathematics anxious and enhance their well-being by referring them to school counsellors/psychologists for professional help. However, if practical, school counsellors could also upskill teachers to use components of MBCT to reduce students’ manifestation of mathematics anxiety. School counsellors could also utilise MBCT 1:1 with students to reduce mathematics anxiety or implement a group programme such as the one used here, which may be more time-efficient to implement. Lastly, in collaboration with non-governmental agencies, government agencies could develop and implement programmes through training, seminars and workshops for mathematics teachers and guidance counsellors on applying MBCT, which is geared towards reducing the consequences of mathematics anxiety among secondary school students.
Conclusion and recommendations
The present study investigated the effect of MBCT on mathematics anxiety among secondary school students. Results showed that 12-sessions of MBCT produced a significant positive effect on mathematics anxiety among the students at the post-test, and the effect was consistent at follow-up compared to students in the control (conventional counselling) group. Based on the finding of the current study, the following recommendations were made by the researchers: (1) Mathematics teachers should consult with school counsellors regarding students that face psychological challenges related to performance in mathematics, (2) School counsellors should ensure they are trained in using MBCT to reduce mathematics anxiety among secondary school students, which could be achieved through professional development seminars, workshops and conferences and (3) School counsellors could upskill mathematics teachers on how to apply MBCT to mathematics-anxious students.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.