
Abstract
Assessment and management of youth suicide risk is a key role for school psychologists. However, prior research indicates that psychologists commonly lack confidence and feel unprepared when they graduated to conduct risk assessments. This qualitative study explored nine Victorian early-career school psychologists’ role in risk assessment, and their self-perceived preparedness, self-efficacy, postgraduate training experiences and methods used to assess risk. Results identified that the frequency of student suicidal ideation and acute mental health presentations exceeded participants’ expectations. Participants identified confidence in assessing risk, but less confidence in the follow-up actions. Participants reported employing comprehensive risk assessment practices and most received exposure to risk assessment during training. Key factors identified for building risk assessment preparedness and confidence were supervision, experience, professional development and research. As participants identified core risk assessment competencies that may require further coverage in curricula, these findings have important implications for universities to maximise graduates’ risk assessment preparedness.
Youth suicidal behaviour is a significant public health concern (Schmidt, 2016) and school psychologists play a pivotal role in mitigating suicide risk in children and adolescents (Erps et al., 2020). It is (conservatively) estimated that in any given 12-month period in Australia, approximately 7.5% of 12 to 17-year-olds will experience suicidal ideation; 5.2% will make a suicide plan; and 2.4% will attempt suicide (Zubrick et al., 2016). Although accurate suicide prediction is difficult, suicide risk assessment is a crucial prevention strategy (Debski et al., 2007). To accurately assess a young person’s risk of suicide, a school psychologist must feel well-prepared to comprehensively evaluate risk factors and judge the level and urgency of risk. However, research indicates that school psychologists commonly lack confidence in their abilities and feel that their training did not adequately prepare them to assess suicide risk (Erps et al., 2020).
The primary role of a school psychologist is to address barriers to student learning, improve educational achievement and enhance psychological health (Australian Psychological Society [APS, 2016]) by providing counselling, and diagnostic and psychoeducational assessment (Campbell & Colmar, 2014). However, this role has likely evolved to include more demand for risk assessments due to the statistically significant increase in 15 to 19-year-olds meeting the criteria for a probable serious mental illness (from 18.7% in 2012 to 22.8% in 2016; Mission Australia, 2017). The profound educational and social disruptions linked to the COVID-19 pandemic have also led to a statistically significant increase in Australian 12 to 18-year-olds’ self-reported psychological distress (Li et al., 2021) putting additional pressure on youth mental health services (Raballo et al., 2020). Having a mental health disorder is the largest significant associated risk factor for youth suicidal behaviours (Zubrick et al., 2016); thus there will be a greater need for school psychologists to triage and support young people with acute mental health needs than ever before (Debski et al., 2007). Consequently, it is imperative that school psychologists feel competent to assess for risk.
Suicide risk assessment
School psychologists use their knowledge of evidence-based suicide risk factors and warning signs to conduct a risk assessment, the necessary process when a young person presents with suicidality. Risk assessment involves gathering data (via clinical interview and risk assessment tools) about an individual’s reported and observable symptoms, behaviours and history to judge the immediacy of their suicide risk (Silverman & Berman, 2014). This judgement requires an understanding of how the combination of the individual’s unique risk and protective factors interact to heighten or lower the individual’s likelihood of engaging in suicidal behaviours in the short-term, which also informs the selection of suitable interventions (e.g. a client at imminent risk may require hospitalisation; Silverman & Berman, 2014).
Assessing risk is one of the most complex and demanding aspects of clinical practice (Barzilay et al., 2019). Furthermore, population-based risk factors and risk assessment tools have been found to be inaccurate methods for predicting suicidality. Meta-analytic research indicates that no single or combination of population-based suicide risk factors are sufficiently accurate at predicting suicide to be clinically useful (Large et al., 2011). Additionally, risk assessment tools are reported to have low positive predictive value: the proportion of individuals who die by suicide, relative to those who are correctly and falsely identified as being at risk for suicide (Runeson et al., 2017). However, the efficacy of these tools in predicting short-term behaviour can be enhanced by utilising sound clinical judgement, leading to improved decision-making about the most appropriate intervention required for the client in the short-term (Barzilay et al., 2019). Despite its limitations, risk assessment remains standard practice (Silverman & Berman, 2014). Other recommendations that are reported to enhance the clinical utility of risk assessment include: treating risk assessment as an ongoing process which determines the ‘here and now’ needs of the individual, rather than as a method for predicting future suicidal behaviours (Hawgood & de Leo, 2016); employing various data-gathering methods rather than solely relying on risk assessment tools (Runeson et al., 2017); including safety planning (Melvin et al., 2016); and employing a developmentally-sensitive approach which equips caregivers with risk management strategies (Betterridge & Taylor, 2016).
Psychologists’ suicide risk assessment self-efficacy
As risk assessment requires clinical judgement, school psychologists must feel confident in their abilities (Douglas & Wachter Morris, 2015). Self-efficacy, which stems from Social Cognitive Theory, refers to one’s perceived confidence in their ability to perform specific tasks to achieve a desired goal (Bandura, 1997). Risk assessment self-efficacy is a multidimensional construct which may vary depending on the specific behaviour required (Douglas & Wachter Morris, 2015). Consequently, a school psychologist may be confident to ask a student about their suicidal thoughts but may feel less confident to employ appropriate action if that student presents with imminent risk. Applying Bandura’s (1997) theory, Elliott et al. (2018) proposed that psychologists’ experience, training and supervision play an important role in the development of their self-efficacy to enhance their readiness, ability and willingness to work with at-risk clients via four methods. Firstly, providing trainees with mastery experiences: direct experiences conducting risk assessments which serve as powerful indicators of one’s capabilities. Additionally, having supervisors model sound risk assessment practices, as well as providing positive reinforcement about a trainee’s risk assessment skills. And finally, addressing trainees’ anxieties about working with at-risk clients (Elliott et al., 2018).
Despite the importance of training in enhancing psychologists’ risk assessment self-efficacy, research indicates that psychologists commonly report perceiving their training to be inadequate and lack confidence in their ability to assess risk. Erps et al. (2020) found that only 66.3% of their American school psychologist participants felt confident to assess risk, and 63% of participants felt that their training was inadequate in preparing them to effectively assess risk. In an Australian study of clinical and counselling psychologists, only 42% of participants reported receiving university training in suicide risk, which ranged between less than two hours to more than eight hours (Trimble et al., 2000). Most of these participants had experience working with at-risk clients, yet few participants felt that their training adequately prepared them to manage client suicidal behaviours. Another study of Australian psychologists found that 31.5% of participants had experienced client suicide (Finlayson & Graetz Simmonds, 2016). Over 41% of participants in this study were in their first 5 years of practice. This study also found a significant positive association between participants’ feelings of responsibility for their client’s suicide and emotions such as guilt, shame and self-doubt about their competency. A third Australian study found that school guidance officers commonly feel inadequately trained to manage the increasing complexity and severity of youth mental health presentations in schools (Bramston & Rice, 2000). Updated research is needed to understand school psychologists’ risk assessment experiences.
Suicide risk assessment competencies
It is concerning that research indicates psychologists lack confidence and/or preparedness to assess risk given that risk assessment is a core professional competency of Australian psychologists (Australian Psychology Accreditation Council [APAC, 2019a]). In the event of a student exhibiting suicidal behaviours, school psychologists are expected to be competent in: responding to the client’s disclosure with empathy and concern (not alarm); assessing and formulating the individual’s level of risk and immediate safety needs; developing and implementing a treatment plan; adhering to crisis management policies and procedures in the educational system; understanding the psychologist’s legal and ethical responsibilities (e.g. the limits to confidentiality); notifying emergency services where necessary; documenting the clinical decisions made; and engaging in debriefing and self-care (APAC 2019a; APS, 2016; Australian Psychologists and Counsellors in Schools [APACS, 2019]; Cramer et al., 2013).
The current study
This review highlights that more research is needed to understand Australian psychologists’ current experiences with assessing risk in schools given the increase in youth mental health presentations. As psychologists with postgraduate training in educational and developmental psychology are specifically trained to work in educational settings (APAC, 2019a) and most of these programs are taught in Victoria (APAC, 2019b), this research sought to explore the experiences of early-career (within 5 years post-graduation) school psychologists in Victoria. A qualitative research methodology was used to explore their role in risk assessment, self-perceived preparedness, self-efficacy, postgraduate risk assessment training experiences and methods used to assess risk. The study aimed to address the following questions:
(1) What are early-career school psychologists’ perceived and reported roles in risk assessment?
(2) How efficacious do early-career school psychologists perceive themselves to be in assessing risk?
(3) What methods do early-career school psychologists use to assess risk?
(4) What risk assessment training have early-career school psychologists received?
(5) What experiences do early-career school psychologists perceive to have best prepared them and contributed to their confidence in assessing risk?
(6) What are the implications for postgraduate psychology risk assessment training?
Method
Participants
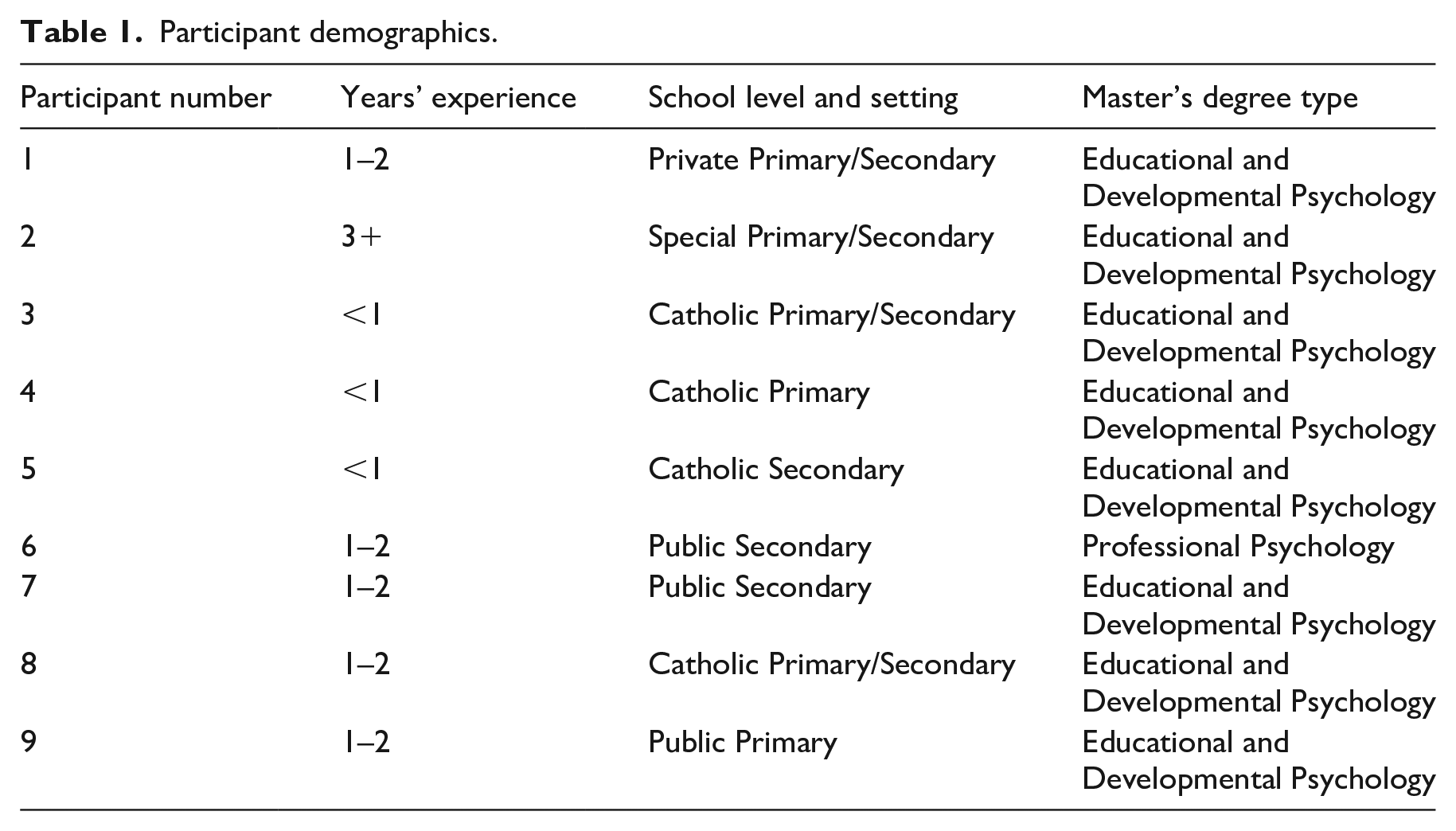
The sample comprised nine female school psychologists (M = 30.36 years, SD = 5.03) currently working in Victoria, Australia who had completed their postgraduate training in the last five years across four universities. See Table 1 for further demographic details.
Participant demographics.
Procedure
Ethics and recruitment
Ethics approval for the project was obtained from the Melbourne Graduate School of Education Human Ethics Advisory Group (HREC no. 21331-17888-3). Recruitment advertising was posted on relevant social media groups. Interested participants contacted the first author. Participants were emailed a Qualtrics survey which contained the consent form and plain language statement. Participants consented to the terms of the research by selecting a ‘yes’ checkbox at the beginning of the survey.
Data collection
Demographics were gathered from participants via an online survey using Qualtrics, and a 40-minute interview conducted via Microsoft Teams. The semi-structured interview comprised 23 open-ended questions which guided the discussion (see Supplemental Material). These questions were adapted from prior research (Erps et al., 2020; Schmidt, 2016; Stein-Erichsen, 2010). Interviews focused on participants’ roles in risk assessment in schools; how efficacious they feel about assessing risk (self-perceived competence and confidence); methods used to assess risk; risk assessment training received; what experiences best prepared them and contributed to their confidence to assess risk; and recommendations for how providers could improve risk assessment training.
Data analysis
Recordings were auto-transcribed by Microsoft Teams then the first author reviewed all interviews and edited transcripts to ensure accuracy. All data were de-identified to maintain participants’ confidentiality. Interview responses were analysed thematically utilising Braun and Clarke’s (2006) six-step methodology. A deductive approach to coding was employed, whereby the coding categories reflected the interview schedule (Braun & Clarke, 2006). Firstly, ‘familiarisation with data’ was conducted by reading the interview transcripts multiple times. Secondly, ‘generating initial codes’ occurred by identifying relevant features in the data and manually arranging them in groups based on common ideas. Thirdly, ‘identifying themes’ involved collating codes into broad level themes. Fourthly, the first author ‘review(ed) themes’ by evaluating the coded data within each theme and assessing the validity of the themes in relation to the larger data set. Agreement on the final themes was reached by consensus between both authors. Fifth, ‘defining and naming themes’ occurred by further describing and refining each theme. Finally, ‘producing the written report’ involved extracting data to provide evidence for each theme.
Results
Data analysis resulted in identification of three key themes and three subthemes within each, see Figure 1. These themes along with samples of interview quotes are reported below.
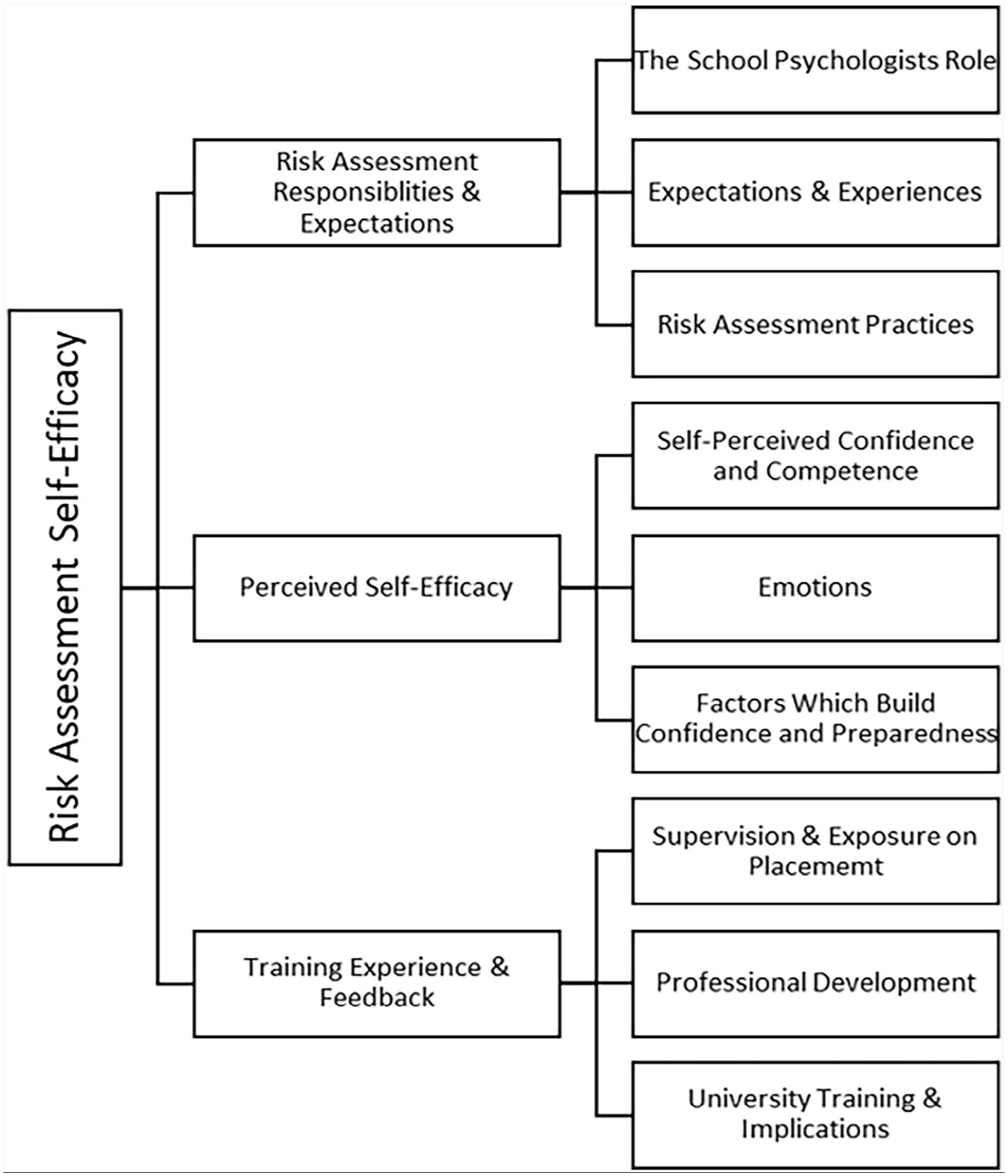
School psychologists’ risk assessment self-efficacy thematic representation.
Risk assessment responsibilities and expectations
This theme included three subthemes, addressing Research Questions 1 and 3, which represent the school psychologist’s role in assessing student risk; school psychologists’ expectations and the frequency of suicidal ideation and acute mental health presentations in schools; and methods employed to assess student risk.
The school psychologist’s role
Participants reported that school staff consider psychologists to be the ‘expert’ in assessing a student’s level of risk. They reported that it is their responsibility to: identify warning signs; support the student; develop and review safety plans with students; adapt their schedule if risk presents unexpectedly; notify students’ parents, the school leadership team and emergency services of risk (where necessary); decision-making regarding developing a treatment plan; recommending referrals to external services and supporting students whilst they wait for access to external agencies (e.g. an external psychologist); and monitoring ongoing risk. Participants also reported being responsible for developing school procedures relating to risk, providing professional development for teachers and upskilling parents on how to support their at-risk child.
My role is to basically assess the risk, make decisions based on that risk profile as to what next steps have to happen. Almost always, the parents are notified. And then from there a plan is . . . developed about how we manage that risk as to whether it’s an immediate risk or . . . not immediate. (Participant 6)
Participants reported that staff have a sound understanding of the school psychologist’s role in assessing risk and that staff worked collaboratively with them to support students at risk. However, some participants indicated a need to set firm boundaries with staff about the short-term nature of their services. Another participant indicated they were concerned that school staff expected a risk assessment to guarantee a student’s safety.
We’ve had to be firm sometimes in saying that this child needs to be referred out. We can’t see them ongoing (as) . . . we are a short-term service . . . we don’t have the capacity to see every single child that would need ongoing support. (Participant 5)
Expectations and experiences
Seven of the nine participants indicated that they work with clients exhibiting suicidal ideation at least weekly. For example, one participant estimated that half their caseload exhibit suicidal ideation and that they encounter several moderate-to-high risk cases a term. One participant was too new in their role to answer, and another reported that they had not encountered risk at their primary school. Six participants reported that the frequency of suicidal ideation was higher than they anticipated when they graduated.
I think I completed more risk assessments in my first week on the job than I did in my entire postgrad training. (Participant 7) I don’t think we (newly graduated psychologists) are prepared in any way, shape or form for that level (of suicidal ideation in schools). (Participant 8)
Interestingly, eight participants perceived that the frequency of acute mental health presentations in schools had substantially increased during their limited time in the field (most participants had 1–2 years’ experience). Four participants also indicated that they thought the COVID-19 pandemic and related lockdowns had contributed to perceived increases in suicidal ideation and acute mental health presentations in schools or had at least highlighted the unmet mental health needs of students.
Risk assessment practices
Participants reported employing diverse and comprehensive risk assessment practices. All participants indicated that they conduct clinical interviews with students to assess risk. Three participants reported using published risk assessment tools (e.g. the Suicide Tailored Assessment for Responding to Suicidality; Hawgood & de Leo, 2018). Another three participants indicated that they adapt these tools, such as modifying the questions to ensure that they are developmentally appropriate, or appropriate for neurodivergent clients with limited verbal skills.
I kind of made my own (risk assessment) . . . some of the questions were way too complex for some of the students (with autism) I work with . . . I just really simplified it . . . the language has to be very explicit, very blunt, short sentences, a lot of yes or no questions . . . I’ve taken out some of the really long Likert scales because they’re confusing for some of the students . . . So I get a lot more information that way. (Participant 2)
Finally, three participants employed ‘informal’ methods, such as asking their own list of questions based on common risk factors. All participants indicated that they use safety plans (e.g. BeyondNow; Beyond Blue, 2021). In formulating the level of risk, four participants indicated that they may gather additional information from school staff and seven participants reported that they may gather additional information from parents (e.g. stressors which may contribute to suicide risk).
I definitely inquire further from the parent around whether they’ve noticed any warning signs (from the child) and I try to gather a little bit more information about whether there are any additional stressors at home which might be contributing to the ongoing or current risk. (Participant 7)
Five participants acknowledged the limitations of risk assessment as a method to predict future suicidal behaviours. These participants reported that learning about such limitations led them to re-evaluate their risk assessment protocols, such as avoiding categorising risk as ‘low’, ‘moderate’ and ‘high’ and instead focusing on whether the current risk was ‘imminent’. Additionally, they reported treating risk assessment as a method for assessing their clients’ immediate safety needs given the ‘dynamic’ nature of risk, and regularly monitoring their clients’ risk. One participant reported that learning about the limitations of risk assessment tools lessened their risk assessment tool confidence and that they now feel more accepting of the ‘greyness of categorising risk’.
Perceived self-efficacy
This theme included three subthemes, addressing Research Questions 2 and 5, which represent participants’ self-perceived risk assessment confidence and competence; emotions experienced when assessing risk; and factors which contributed to participants’ risk assessment confidence and preparedness.
Self-perceived confidence and competence
Participants’ level of risk assessment confidence varied depending on the risk assessment task required. All participants reported feeling ‘confident’ or ‘very confident’ in assessing risk overall. Eight participants also felt well-prepared to assess risk, whereas one participant indicated feeling unprepared and that it would come as a ‘shock’ due to risk being rare in their primary school. All participants indicated feeling confident to ask students about suicidal behaviours.
Participants also commonly indicated feeling confident in their judgement about when a risk assessment is necessary; helping the student to feel comfortable to talk about suicidal behaviours; and validating the student’s feelings. All participants also reported feeling competent in their ability to identify suicide warning signs and their understanding of how certain factors increase risk (e.g. LGBTQIA+ clients). Seven participants also identified confidence in their formulation skills. Nevertheless, participants commonly indicated that assessing risk is challenging.
Sometimes I have those feelings like, Oh my God! Imagine if it (the risk) was a lot higher and I didn’t pick up on it or the student wasn’t being truthful with me. (Participant 2)
Eight participants indicated that they continue to seek advice from their supervisors, senior colleagues and peers when formulating a student’s level of risk, particularly if it is a complex case (e.g. family issues). Aspects of the risk assessment process participants felt less confident about included working with more complex risk presentations and the follow-up actions required when a student discloses risk. Other challenges of risk assessment included how risk presentations might differ at different ages and with neurodivergent clients. Follow-up actions which participants indicated that they were less confident about were deciding when to send a student home; when and how to notify parents and staff of risk; how to balance maintaining a student’s trust and breaching their confidentiality to protect them from harm; what their obligations and responsibilities are as an employee and a psychologist when a student presents with ‘high’ or ‘imminent’ risk; and the actions required in the broader education system.
So faced with a student that is actually saying ‘I am suicidal. If I walk out of here now, this is what I’m going to do’. I actually don’t know I’m so confident with what my next steps would be for that student. Because I haven’t really been faced with that before . . . I really should be feeling a bit more confident with (knowing) what we need to do to keep this person safe. (Participant 3)
Emotions
Participants reported experiencing various emotions when assessing risk. Seven reported feeling anxious and/or difficulties remaining calm during a risk assessment. Factors which contributed to their anxiety included when participants had less risk assessment experience, or if the case was complex or acute. One participant indicated that they experienced strong dread the first time that they were required to assess risk as they were concerned that they were not skilled enough to do it well.
I remember the first time I did it (risk assessment) . . . I really felt strongly that . . . I guess it was dread . . . but dread for me because I was like, will I do this right? (Participant 9)
Another participant reported that they were more likely to experience stress if they had completed a lot of risk assessments recently. Strategies participants reported utilising to manage these feelings included engaging in self-care, seeking support from their supervisor, monitoring their physiological arousal to students disclosing risk and self-reflection to ensure that their feelings did not interfere with the accuracy of the risk assessment.
Other emotions participants identified included feeling calm, sad, frustrated, pressured and guilty. Two participants reported finding it challenging to sit with their client’s pain. Additionally, two participants indicated that they could feel frustration if risk presented unexpectedly and disrupted their schedule, or when external services (e.g. the Child and Adolescent Mental Health Service) did not respond in a timely way. Two participants reported feeling additional pressure and responsibility when clients did not have adequate support at home. For example, one participant reported that when students do not have support at home, it is very challenging as a school psychologist to rely on external agencies as; At some point those agencies will let you down and they will ultimately let the child down. And this is where you kind of do this dance with them (and are) left holding the baby. As the school psychologist, you do the risk assessments. You’re not meant to be taking on long-term (care). But when that process doesn’t happen, there’s no protocols in place for (what to do next)’ . . . (and) this poor student’s mental health is just really spiraling . . . there’s no handbook for that. (Participant 6)
One participant indicated feeling guilty if a regular client’s risk increased because they thought they should have identified it sooner. Finally, one participant reported feeling ‘confronted’ by the prospect that it is ‘inevitable’ a client will complete suicide during their career.
Factors which build confidence and preparedness
Four experiences which participants most frequently endorsed as being beneficial for building preparedness and confidence were engaging in supervision and peer consultation, experience conducting risk assessments with clients, professional development and engaging in research. All participants reported that seeking guidance from a supervisor or colleague is crucial for building risk assessment confidence and preparedness. This included reviewing and refining their risk assessment protocol, sharing the challenges they experience with assessing risk and debriefing. For instance, one reported that ‘the most invaluable aspect of my practice is supervision’. Six participants indicated that exposure to risk with clients and doing risk assessments regularly enhanced their risk assessment confidence.
I’ve just got better at doing them (risk assessments) as I have done them more and more. Every risk assessment training has role-plays and like trying to practice the practical side of things, which is fine . . . but it is not the same as doing it with a student who is possibly suicidal . . . (Training) definitely doesn’t prepare you for actually talking to a person (who’s suicidal). (Participant 2)
Five participants reported that engaging in ongoing professional development and four participants indicated that engaging in research (including learning of the limitations of risk assessment tools and cultural considerations in assessing risk) increased their risk assessment confidence. Finally, one participant reported that it was helpful to view risk assessment self-efficacy as an ‘ongoing’ process that is something to strive for, rather than a destination.
Training, experience and feedback
This theme included three subthemes, addressing Research Questions 4 and 6, which represent supervision and exposure to risk on placement; risk assessment professional development undertaken; and participants’ risk assessment training experiences and recommendations to improve competencies in curricula.
Supervision and exposure on placement
Participants reported varied exposure to risk assessment during their postgraduate training. Five participants gained experience assessing risk on placement and two additional participants observed their supervisors conduct risk assessments. Two of these participants indicated that they only did ‘a few “low risk” assessments’, whereas another participant reported assessing risk ‘daily’ in their hospital placement. One participant indicated that risk did not come up due to the types of placements completed (e.g. cognitive assessment-based placements). The two participants who did not receive exposure to risk assessment on placement assumed that their supervisor would not allow interns to assess risk. No participants reported prior experience working with suicidality.
Supervisory experiences also varied. Five participants reported receiving adequate supervision related to risk assessment as provisional psychologists. However, three participants who felt that they did not receive adequate supervision indicated that this was because risk did not come up on placement. One of these participants indicated they did not prioritise developing their risk assessment competency during supervision because, prior to graduation, they underestimated how frequently school psychologists encounter risk.
I don’t think we realised how big a part of the role it (risk assessment) would be and so therefore (we) didn’t put as much time into practicing it, learning about it and seeking out the supervision (for it). (Participant 7)
Professional development
All participants reported completing risk assessment professional development, however two participants only did so post-graduation. Participants commonly reported that the role-play component of training was particularly helpful to become comfortable with using language related to suicide and learning that it was protective to ask clients about suicide explicitly.
Exposure to the language (and) types of questions (was) ground-breaking for me to be exposed to . . . (that) it’s ok to ask very directly (about suicide). In fact, it’s probably better . . . and that it’s not going to make things worse. It’s not going to plant an idea . . . that was important for me to know because prior to that I might not have thought it was ok to ask. (Participant 3)
University training and implications
All participants reported having at least one university class dedicated to risk assessment was ‘really important’ because risk could come up at any time when working with students. One participant indicated that learning about risk in class is fundamental because it may be the only opportunity for provisional psychologists to receive risk assessment training prior to graduation.
(Having a university class on risk assessment is) fundamentally important . . . because of the suicide rate and how high it is . . . in our lifetime we will come across a client who will suicide, we’re dealing with high-risk people. It is fundamentally important that they cover it and (help psychologists) understand that it’s going to happen so you can be prepared . . . as much as you can. (Participant 6)
The number of postgraduate university classes dedicated to risk assessment participants could recall ranged from zero to two, although some participants indicated that risk came up sporadically in other classes. Four participants reported feeling that risk assessment was not covered adequately in class and that their university training did not adequately prepare them for assessing risk.
The uni course was really good in providing us with those different risk assessment sheets and how to formulate it. But . . . the follow-up wasn’t really taught. It was just like . . . this is a risk assessment and they didn’t really focus on what to do after that. (Participant 1)
Two participants who were satisfied with their training still indicated that learning about it is no substitute for actual experience. Another participant reported that it was unrealistic to expect to feel ‘100% prepared’ for risk assessment at graduation. Aspects of postgraduate risk assessment classes that participants enjoyed included being given various risk assessment tools to use and hearing about their lecturers’ risk assessment experiences. One participant reported that reviewing Coroners Court documents to evaluate a psychologist’s decision-making process was a powerful prompt to reflect on their own risk assessment protocol to ensure that if one of their clients completed suicide, they could justify their decision-making. This activity also led the participant to realise that losing a client to suicide is not necessarily due to a psychologist’s negligence.
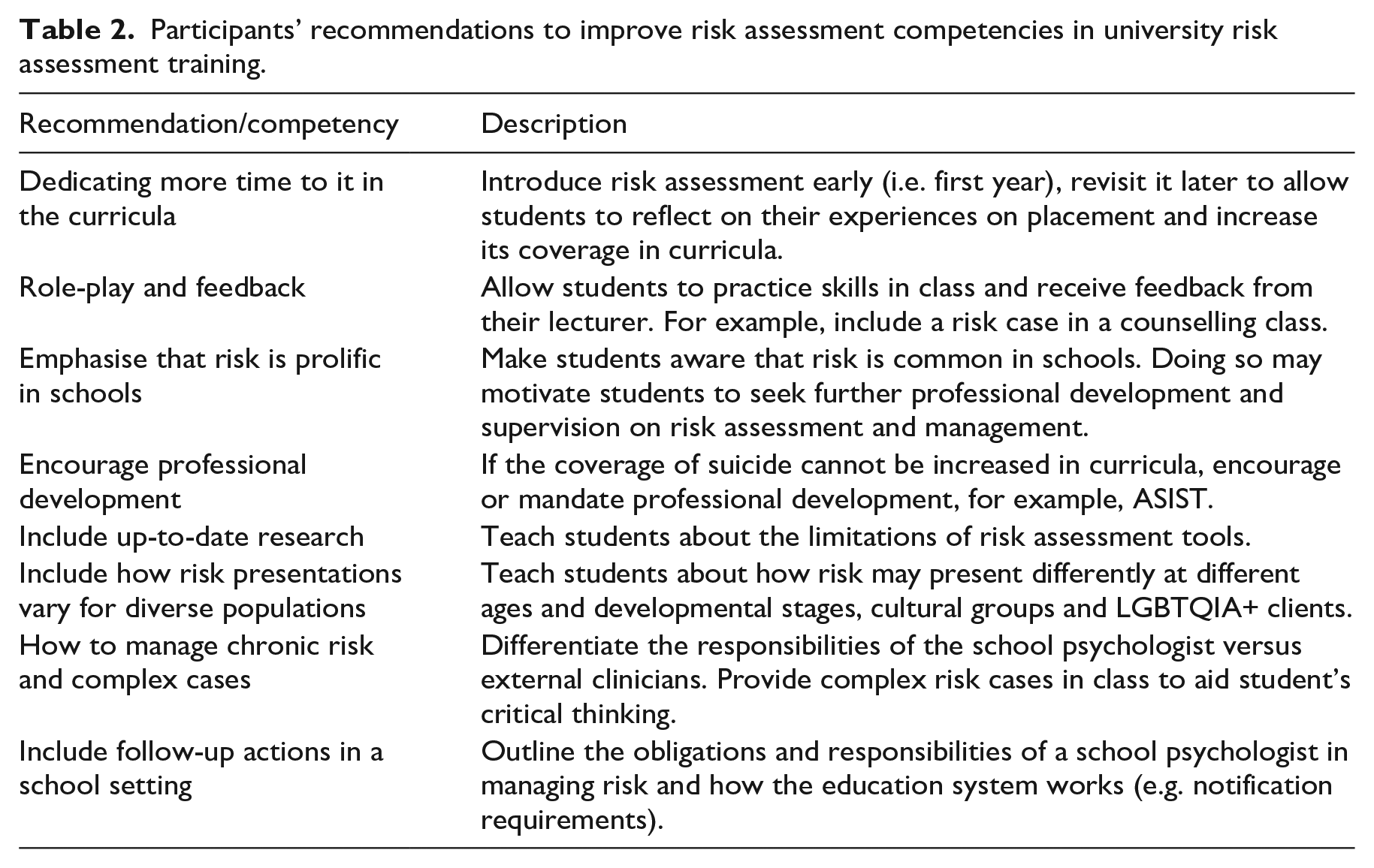
Finally, participants identified recommendations on risk assessment competences that may require further coverage in curricula to maximise graduates’ risk assessment preparedness (see Table 2).
Participants’ recommendations to improve risk assessment competencies in university risk assessment training.
Discussion
The aim of this qualitative study was to explore Victorian early-career school psychologists’ role and their self-perceived preparedness, self-efficacy, postgraduate training experiences and methods used in the assessment of suicide risk. The study’s main findings, implications, limitations and avenues for future research are discussed.
Participants reported being the identified ‘expert’ in schools to assess risk and that their responsibilities included notifying relevant stakeholders of risk, as well as treating and referring students to external services which addressed Research Question 1. Most participants did not perceive there to be major discrepancies between their obligations as a psychologist to assess risk and their school’s expectations. Most participants also reported that they support students with suicidal ideation at least weekly. Additionally, the frequency of student suicidal ideation and acute mental health presentations exceeded participants’ expectations when they graduated and were perceived to have increased. This corroborates Mission Australia’s (2017) finding of a statistically significant increase in the proportion of youth presenting with a probable serious mental illness which may heighten young people’s risk of engaging in suicidal behaviours (Zubrick et al., 2016). However, most of the participants commenced work relatively recently and close to the beginning of the COVID-19 pandemic which may have contributed to this perceived increase in young people’s psychological distress (Li et al., 2021).
Self-perceived confidence and competence as an indicator of risk assessment self-efficacy was explored to address Research Question 2. It was found that participants’ risk assessment confidence varied depending on the level of complexity of the specific risk assessment task required, suggesting that risk assessment self-efficacy is a multi-dimensional construct (Douglas & Wachter Morris, 2015). All participants felt confident to ask clients about suicide and competent to identify warning signs and risk factors, however approximately half of the participants reported lower confidence regarding the follow-up actions (e.g. when and how to notify others of risk) and the actions required in the broader education system. These findings highlight the complexity involved in risk assessment and the need to support early-career psychologists. Participants reported experiencing varied emotions when assessing risk including anxiety, guilt and frustration. These emotions were attributed to having limited experience or doubting their abilities. As risk assessment is professionally and personally challenging (Trimble et al., 2000), this finding suggests that supervisors can play an important role in helping trainees to develop adaptive coping responses to reduce the likelihood of self-blame for client engagement in suicidal behaviours (Finlayson & Graetz Simmonds, 2016). Doing so could also enhance risk assessment self-efficacy (Elliott et al., 2018).
Consistent with best practice, participants reported utilising comprehensive risk assessment approaches, addressing Research Question 3. These practices include employing multiple data-gathering techniques rather than solely relying on risk assessment tools (Runeson et al., 2017), and safety-planning (Melvin et al., 2016). Further, most participants also indicated that they understand the low positive predictive value of risk assessment tools (Runeson et al., 2017) which prompted them to adapt their risk assessment protocols, such as approaching risk assessment as an ongoing activity to meet the immediate safety needs of the student (Hawgood & de Leo, 2016) and placing less emphasis on risk categorisation due to the dynamic nature of suicide risk (Large et al., 2011).
Most participants reported exposure to risk assessment on placement and felt that they had received adequate supervision regarding risk, however they indicated a desire for more. This addressed Research Question 4. Additionally, all participants had completed professional development related to suicide risk. This suggests that the development of risk assessment competencies are being prioritised by trainees and are well-supported by their supervisors in this work. Further, all participants felt that it was important that postgraduate psychology programs offered at least one class dedicated to risk assessment. The majority could recall attending at least one risk assessment class and over half felt that their university coursework adequately prepared them to assess risk. Nevertheless, most participants would have liked more of the curriculum dedicated to risk assessment.
The four most common factors which participants endorsed for building risk assessment confidence and preparedness were supervision and peer consultation, experience, professional development and research. This addressed Research Question 5. Participants indicated that supervision was useful for reviewing their risk assessment practices and managing their own emotions. Additionally, participants reported that experience conducting risk assessments is imperative as no other activity could authentically simulate the experience of working with at-risk clients. These findings are congruent with Bandura’s (1997) Social Cognitive Theory which posits that positive reinforcement, modelling, physiological arousal and mastery experiences are the four most important sources for influencing the development of self-efficacy. Professional development was also highly valued by participants for developing risk assessment preparedness and confidence. These results have potential implications for university delivery of risk assessment training such that more scaffolding is recommended in crafting the experience of students to ensure greater equity of exposure to at-risk clients via applied experiences where possible, or by enhancing authenticity of simulations. Additionally, base minimum training hours could also be considered by universities.
Finally, participants’ reflections on their training also provides evidence for key risk assessment competencies which are adequately covered in educational and developmental psychology programs and those which may require further coverage, addressing Research Question 6 (APAC 2019a; APS 2016; APACS, 2019; Cramer et al., 2013). Competencies which participants indicated proficiency in were empathising with clients; eliciting suicide risk and protective factors; attending to clients’ immediate safety needs; formulation; treatment; and debriefing. Risk assessment competencies which could be developed further include managing their own reactions toward client suicidality; knowing when and how to notify others of risk; understanding the short and long-term actions required to manage risk; and what their ethical and legal obligations are within the education system. Additionally, participants identified a desire to learn strategies for managing chronic and complex risk, which may be particularly relevant given the current COVID-19-related strain on external youth mental health services (Raballo et al., 2020).
Limitations
A limitation of this study is that it relied on participants’ self-perceived confidence and competence rather than their actual risk assessment competence. It is possible that participants may perceive themselves to be highly competent regardless of whether they actually employ evidence-based risk assessment practices (Cramer et al., 2013), inclusion of a competency measure would help to quantify this information. The sample was also limited to early-career school psychologists working in one Australian state, inclusion of participants from other parts of Australia may have provided a broader perspective on this population. Additionally, inclusion of other associated parties, that is, placement supervisors, academics and psychology trainers would allow the validation of participant experiences and should be considered in future research.
Conclusion
This study explored Victorian early-career school psychologists’ role and self-perceived preparedness, self-efficacy, training experiences and methods used in the assessment of suicide risk. A major contribution of this study is that it provides understanding of key factors that influence the development of early-career school psychologists’ risk assessment self-efficacy, and identifies elements of risk assessment which early-career school psychologists commonly find more challenging. This understanding is critical given the rising rates of complex mental health presentations in schools and the need for school psychologists to manage risk. Consequently, this study identifies various opportunities for universities to review their risk assessment training to ensure key risk assessment competencies are adequately addressed in curricula.
Supplemental Material
sj-docx-1-spc-10.1177_20556365231206230 – Supplemental material for Early-career school psychologists’ risk assessment self-efficacy: An Australian perspective
Supplemental material, sj-docx-1-spc-10.1177_20556365231206230 for Early-career school psychologists’ risk assessment self-efficacy: An Australian perspective by Erin Quigley and Chelsea Hyde in Journal of Psychologists and Counsellors in Schools
Footnotes
Acknowledgements
None.
Authors’ note
This manuscript is an original work that has not been submitted to nor published anywhere else. All authors have read and approved the paper and have met the criteria for authorship listed above.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
Data available on request due to privacy/ethical restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.