
Abstract
Despite the growing prevalence of Public–Private Partnerships in healthcare, scholars have paid little attention to their consequences for the workforce. Public–Private Partnerships may have important consequences in labour-intensive services such as healthcare, since staff reductions and higher working loads may lead to a decrease in service quality and patient safety. In this paper, we analyse the extent to which Public–Private Partnership schemes have influenced employment in Madrid, one of the most enthusiastic adopters of Public–Private Partnership models in Spain. To do so, we compare clinical staff employment levels across three types of hospital management models, including two types of Public–Private Partnerships. Our findings illustrate that clinical staff employment levels seem to be substantially lower in Public–Private Partnership hospitals than in directly managed public hospitals, particularly as regards nursing staff, and in those types of hospitals where the private sector manages both clinical and non-clinical staff.
Introduction
Since the 1980s, many policy-makers have argued that healthcare management can be improved by the introduction of market-oriented reform (Krachler and Greer, 2015; Sen, 2003). While out-and-out privatization of healthcare is uncommon, of increasing importance is the use of contracting services. In Europe, initiatives such as Public–Private Partnerships (PPP) have become increasingly common in healthcare. Governments have used PPP above all as a mechanism to support the finance, building and operation of hospitals (Hellowell, 2013; McKee et al., 2006). The principal reasons governments adopt PPP in sectors such as healthcare are to deliver infrastructure projects while avoiding up-front capital expenditures, and to benefit from the private sector’s capabilities to provide innovative solutions, while enhancing efficiency and achieving cost savings (Barlow and Köberle-Gaiser, 2008; Barlow et al., 2013).
Despite the growing popularity of the ideas advocating the use of PPP in healthcare, some scholars have identified potential disadvantages in practice, including costs, quality, flexibility and complexity issues (see, e.g., Sclar, 2015; Torchia et al., 2015). Indeed, the benefits and drawbacks of PPP in healthcare are hotly debated topics among policy-makers. One important argument which would caution against implementing PPP in healthcare is that it may lead to lower staff levels. PPP may have particularly important consequences in labour-intensive services such as healthcare, since staff reductions and higher working loads may lead to a decrease in service quality and patient safety (Heimeshoff et al., 2014). Building on different theoretical approaches to public service privatization, we may expect employment to be impacted in a variety of ways; first, profit-maximization incentives and cost-reduction pressures faced by PPP hospitals may mean they hire a smaller number of staff. Second, this reduced staff body may end up working a longer day. In addition, implementing PPP may erode the notion of the state as model employer, modifying the terms and conditions of employment, including job security (Smith, 2012; Vrangbæk et al., 2015). Empirical evidence of the consequences of PPP on employment, however, is neither conclusive nor extensive to date.
In this paper, we analyse the extent to which PPP schemes have influenced employment in Madrid, one of the most enthusiastic adopters of PPP models in Spain. To do this, we deploy two non-parametric multiple comparison tests and multivariate regression panel data models comparing employment levels across different hospital management alternatives, namely directly managed public hospitals, Private Finance Initiative (PFI) models, and an indigenous PPP model known as the ‘Alzira’ model. 1 We use data for hospitals belonging to Madrid’s regional health service over the period 2011 to 2014. The case of Madrid is of particular interest because it is, to the best of our knowledge, one of the few cities in the world where different PPP types for hospitals co-exist. Madrid seems to be, therefore, a useful site to assess differences between hospital governance models. PPP schemes in Madrid were introduced from 2002 as a consequence of the implementation of the Law on Health Organization of the Community of Madrid (LOSCAM-Law 12/2001). This law encouraged the introduction of market-driven mechanisms into healthcare and the contracting out of some or all hospital services, including clinical services (Alonso et al., 2015; Bayle and Cal, 2001). As a result, from 2007 onwards, all newly-built hospitals belonging to the regional government followed (PFI) PPP schemes.
The rest of the paper is organized as follows. In the next section, we explore the major theoretical arguments which deal with the relationship between privatization and its potential effects on employment levels. Next, we describe our data and methods, before presenting and discussing the results of our statistical analysis. Our results suggest that clinical staff employment levels are substantially lower in PPP hospitals than in directly managed public hospitals, particularly as regards nursing staff and in hospitals known as the Alzira model, where the private sector manages both clinical and non-clinical staff. The paper concludes with a summary of our findings, their theoretical, practical and policy implications and possible directions for further research.
Background for assessing employment effects of PPP implementation
From the perspective of economics, the conventional arguments made by advocates of private management of public service delivery focus on the way in which the pressure of competition and the profit-incentive drive greater cost-consciousness and may lead to substantial efficiency gains (see, e.g., Bel and Fageda, 2009; Bel and Warner, 2016; Brown and Potoski, 2003; Gradus et al., 2014; Hefetz and Warner, 2012). These cost-savings and efficiency gains arguments advocating the private management of service delivery have clear implications for employment in general, and for the workforce size in particular (Fernandez et al., 2007).
Firstly, many scholars expect private management to deliver cost savings principally because of the efficiencies gained by transferring the production and delivery of goods and services away from a monopoly to a competition scenario. Competition is, therefore, one of the fundamental ideas justifying the involvement of the private sector in public service delivery, due to the potential cost savings generated by market forces (Downs, 1967; Jackson, 1982; Niskanen, 1968; Savas, 2000). In our PPP case, one if its distinctive features in our study context is that service contracting is performed in a special type of marketplace, via a competitive bidding process. Following Domberger and Jensen (1997: 68), in this sort of scenario, the market ‘is defined by the contract specification, and the bidding process resembles an auction’. This may generate an ex-ante competition, whereby privatized public services may be delivered at the lowest cost and price, thus it is conceivable that the use of competitive bidding may result in staff reductions in order to reduce costs, since the ex-ante competition process may force private firms to enhance labour force productivity.
A second, major, reason why private sector involvement on public service delivery should cut costs was the relatively superior efficiency of the private sector over the public one, a view which justified much of the privatization movement (Clifton et al., 2006). A key argument when explaining the perceived superior efficiency of the private sector is the view that private firms may have more incentives to cut costs and improve efficiency because, unlike the public sector, cost reductions and efficiency enhancements may generate benefits (Hart and Moore, 1990; Miranda, 1994; Shleifer and Vishny, 1994). Incentives are thought to promote efficiency, for instance, if a manager – or owner – personally benefits from cost reductions; the incentives to find those savings are bigger than one who is simply trying to increase their chance of promotion, such as the case of public managers (Frant, 1996). On the contrary and, following Davies (1971: 151), in the case of public property – and management – costs and/or benefits of a decision are not fully supported by the decision maker, unlike under a scheme of private property rights.
Finally, it is also argued that private firms are thought to be relatively free of political inference (King and Pitchford, 1998), so if outsourced activities are less politicized, politicians will be less interested in over-staffing public services (Boycko et al., 1996), resulting in staff reductions. This may be so because politicians and government bureaucrats, public choice theorists argue, behave according to the typical neoclassical individual who seeks to maximize his or her profit and personal interests whilst neglecting the citizens they purportedly serve, resulting in public service over-supply and over-staffing in order to maximize politicians and bureaucrats’ individual personal utility or political power (see, for example, Niskanen, 1971). In this line, Donahue (1989) and Kettl (1993) argued that much of the expected savings from privatization would come from public employment reduction.
In sum, though all these theoretical perspectives offer different rationales for involving the private sector in public service delivery, each seems to lead to the same effect as regards the size of the workforce. However, although there seem to be strong theoretical reasons to believe that private management of public service delivery will lead to lower employment levels, the empirical evidence is not clear, suggesting that though under some circumstances private management may have a negative effect on employment, there seem to be different factors that can reduce this effect (Fernandez et al., 2007: 61). Therefore, we enquire here: are PPP schemes in Madrid hospitals associated with lower employment levels?
Data and methodology
To explore differences in employment across different hospital management models, we draw upon an unbalanced panel of Madrid hospitals from the period 2011 to 2014. We include in our sample three groups of management models for which we have enough data, namely directly managed public hospitals and two types of PPPs (indirect management), i.e. PFI models and the so-called ‘Alzira’ models.
Directly managed public hospitals are operated by the regional government. Most of these hospitals do not enjoy their own legal status and are ruled by public law. In addition to the directly public managed models, two types of PPPs co-exist in Madrid: the Design, Build, Finance and Operate (DBFO)-PFI model, similar to the UK’s PFI, and a Spanish-born variant, the so-called ‘Alzira’ model. (DBFO) PFI models constitute a long-term arrangement between the public and private sectors, whereby the private sector finances and constructs hospitals and then proceeds to deliver non-clinical services for a period of approximately 30 years (Acerete et al., 2011; Hellowell and Pollock, 2009). In other words, the contractor designs, builds and finances the hospital, and the regional government pays a fee for using the hospital infrastructure during the duration of the contract. In addition, the contractor also provides non-clinical services such as hospital maintenance, waste management, laundry, clinical files storage, sterilization, catering services, and so on. In this model, clinical services and clinical staff are managed by the regional government through public enterprises, which are configured as organizations with legal personality and ruled by private law. This opens the door, among other things, to including private stakeholders in the hospital Board of Directors, and also to managing clinical staff resources through labour legislation instead of public law and statutory personnel regimes (Alonso et al., 2015). The ‘Alzira’ model is a PPP model that goes further: in this case, the private sector finances, constructs and operates the hospital’s physical infrastructure, and is also responsible for the delivery of clinical and non-clinical services (Acerete et al., 2011), hence one could consider this type of management model as a ‘full private’ model.
It is important to acknowledge that differences in managerial structures between both types of PPP imply that they may face different kinds of incentives to promote efficiency and reduce costs through employment reductions; while the theoretical arguments advanced in the previous section clearly apply to the ‘full private’ model, i.e the ‘Alzira’ model, incentives to reduce costs at the expense of employment reductions may be present too in PFI hospitals, where clinical services and clinical staff are managed by the regional government through a public enterprise. The reason is that although there is no profit to gain in the latter case, surpluses can be used within a year for those types of hospitals, and deficits could be considered as evidence of management failure (Propper et al., 2004).
In 2014, there were 35 hospitals belonging to the SERMAS (Servicio Madrileño de Salud-Madrid Regional Health Service). For the purposes of our analysis, we excluded psychiatric, geriatrics and long-stay hospitals, in order to work with a relatively homogeneous sample. The final sample thus consists of 29 public hospitals, 18 of which were operating under direct public management, seven were PFI models and four were considered Alzira models. 2
Empirical approach
In order to test whether the employment levels in alternative management models within the SERMAS differ, we first compare employment numbers across the three types of management models described above, using a simple non-parametric Kruskal–Wallis test (Kruskal and Wallis, 1952), followed by a non-parametric Dunn’s (1961) test, when the Kruskal–Wallis test is rejected. Then, to control for potential confounding covariates affecting these non-parametric comparisons, we estimate two different regression models predicting each dependent variable (described below). Therefore, our baseline regression model specification is the following:

where yit is a measure of one of the two dimensions of employment in hospital i at time t; PEIit is the itth observation of the PFI management dummy; Alzirait is the itth observation of the ‘Alzira’ model management dummy; Zit the itth observation on P control variables; T is a time trend; and ∊it the remainder disturbance term. To test the effect of different models in employment levels, the coefficients of interest are β and γ in each of the three regression models.
Given the nature of our data, we use pooled Ordinary Least Squares (OLS) and panel Random Effects (RE) to estimate equation (1). It is important to highlight from the outset that, though a widely used approach when estimating models such as equation (1) has been the fixed-effects estimator, we were unable to use a fixed-effects specification because we do not have instances of hospitals exhibiting alternate governance models within the time frame of our data. Therefore, the variables PFI and ‘Alzira’ do not exhibit within-hospital variance. Nevertheless, the literature on panel data econometrics supports the view that with the inclusion of proper controls both approaches, i.e. OLS and RE, are consistent estimators (Wooldridge, 2012). It should be acknowledged, however, that the true underlying model describing hospital employment levels is unknown, hence we cannot rule out the possibility that some unobserved confounders may drive our results, i.e. the well-known omitted variable bias (OVB) problem. Although we include in our models a number of control variables which may affect hospitals’ employment levels to reduce OVB as much as possible (see below), due to potential OVB issues our results should be interpreted as correlations, not causal effects.
Independent variables
The analysis presented here focuses on publicly available measures of clinical-staff employment levels that are collected and published by the SERMAS. To assess the relative employment levels among different management models, we draw upon measures of two key dimensions of clinical staff; (a) number of physicians excluding personnel in formation; 3 and (b) nursing staff.
Dependent variables
The primary independent variables of interest are the hospital management types; a dummy variable is included in the model to capture each of the three hospital management types described above, i.e. directly managed public hospitals, PFIs and ‘Alzira’ hospitals, with directly managed public hospitals as the omitted reference group. This approach is used in nearly all regression-based analyses comparing different characteristics of public sector organizations (Alonso and Andrews, 2016; Andrews et al., 2011). To ensure that our models are well-specified, we include in addition a set of control variables which may affect hospitals’ employment levels, as identified by previous research (see, for example, Heimeshoff et al., 2014), and for which data are publicly available, such as patient heterogeneity or complexity (case-mix) and hospital characteristics such as hospital activity (measured as the number of inpatients) and the teaching status, measured through a dummy variable keeping as the reference group those hospitals without teaching status.
While hospital characteristics such as number of inpatients and teaching status are straightforward measures, hospital case-mix index may require additional explanation; the case-mix index of a hospital reflects the heterogeneity, clinical complexity and the needs for resources of hospital inpatients. Hospital case-mix indices are constructed as a weighted average of all discharges according to their Diagnosis Related Group (DRG)-weights (Sánchez-Martínez et al., 2006). In Spain, the DRG system classifies hospital cases based on clinical data, demographic data (such as age and gender) and resource consumption data (for a comprehensive explanation of DRGs in Spain see, e.g., Cots et al., 2011; Schreyögg et al., 2006). Hence, this indicator accounts for both, patient characteristics such as age and clinical complexity, and estimated resources consumption for each inpatient. We extracted figures on Madrid’s hospitals characteristics between 2011 and 2014 using official hospital annual reports (retrieved from www.madrid.org; accessed on January, 1st, 2016.).
Results and discussion
Table 1 presents differences among directly managed public hospitals, PFI and Alzira hospitals in terms of employment levels. Turning first to the number of physicians, both including and excluding physicians in formation, a quick look to the data reveals that there seem to be substantial differences in means between directly managed public hospitals and both PFI and Alzira models. Starting with the total number of physicians, the results of the Kruskal–Wallis test clearly suggest rejection of the null hypothesis of no differences in mean ranks across the three management models (p = 0.013). In addition, Dunn’s test reveals that directly managed public hospitals employ significantly higher levels of physicians than PFI and Alzira models (direct public vs. PFI, p = 0.003; direct public vs. Alzira, p = 0.045). Regarding nursing staff, our results reveal a similar pattern, i.e. directly managed public hospitals employ significantly higher levels of nursing staff than the other two groups (Kruskal–Wallis p = 0.002; Dunn’s test: direct public vs. PFI, p = 0.002; direct public vs. Alzira, p = 0.005).
Employment levels and hospital characteristics by type of management.
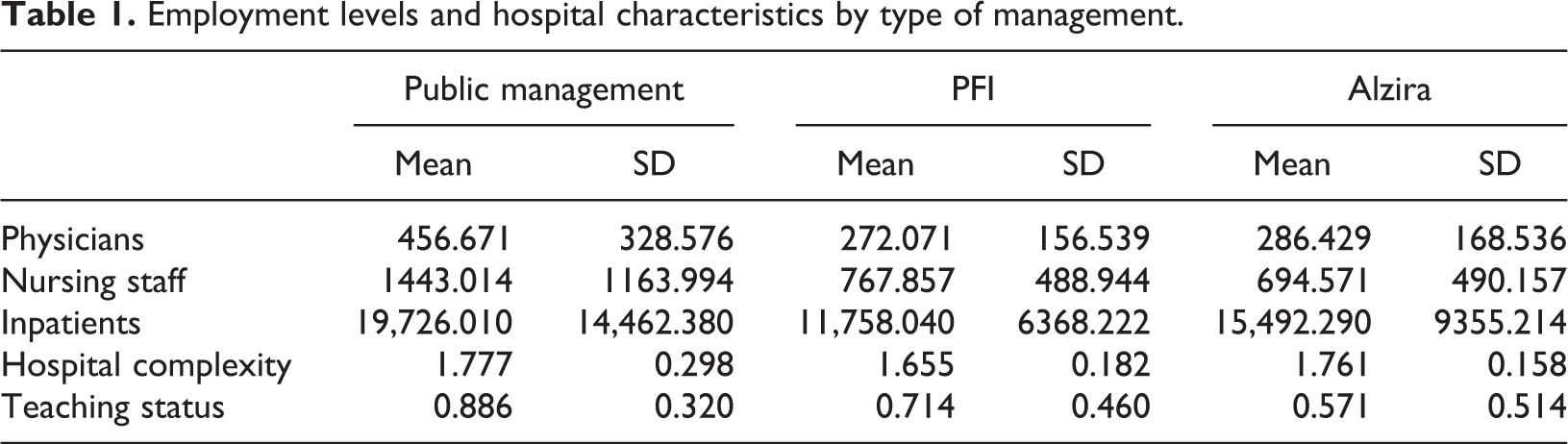
It should be noted, however, that these non-parametric comparisons do not control for other variables that may affect employment levels. For instance, directly managed public hospitals seem to have more activity in terms of inpatients, are slightly more complex and a majority of them have teaching status, which may likely affect employment levels. The remainder of this section, therefore, addresses whether in fact these apparent higher employment levels of clinical staff in directly managed public hospitals remain when other factors are controlled for.
Tables 2 and 3 present point estimates for the proposed multivariate regression models, starting with physicians’ levels in Table 2, before moving onto nursing staff levels in Table 3. Breusch-Pagan Lagrange Multiplier (LM) tests for the random effects are used to examine whether RE models should be preferred to pooled OLS. Although diagnosis tests point to the RE estimator for each regression model, we present estimation results for both pooled OLS and RE estimators for robustness check purposes. Further diagnostic tests revealed that the data may suffer from heteroscedasticity. This problem has been commonly solved by using the Huber-White sandwich estimators. However, asymptotic standard errors based on sandwich estimators may be biased with low number of observations. To overcome this potential problem, we compute robust standard errors through a non-parametric paired bootstrapping procedure (see, for example, MacKinnon, 2002).
Estimated differences of physician levels by type of management.
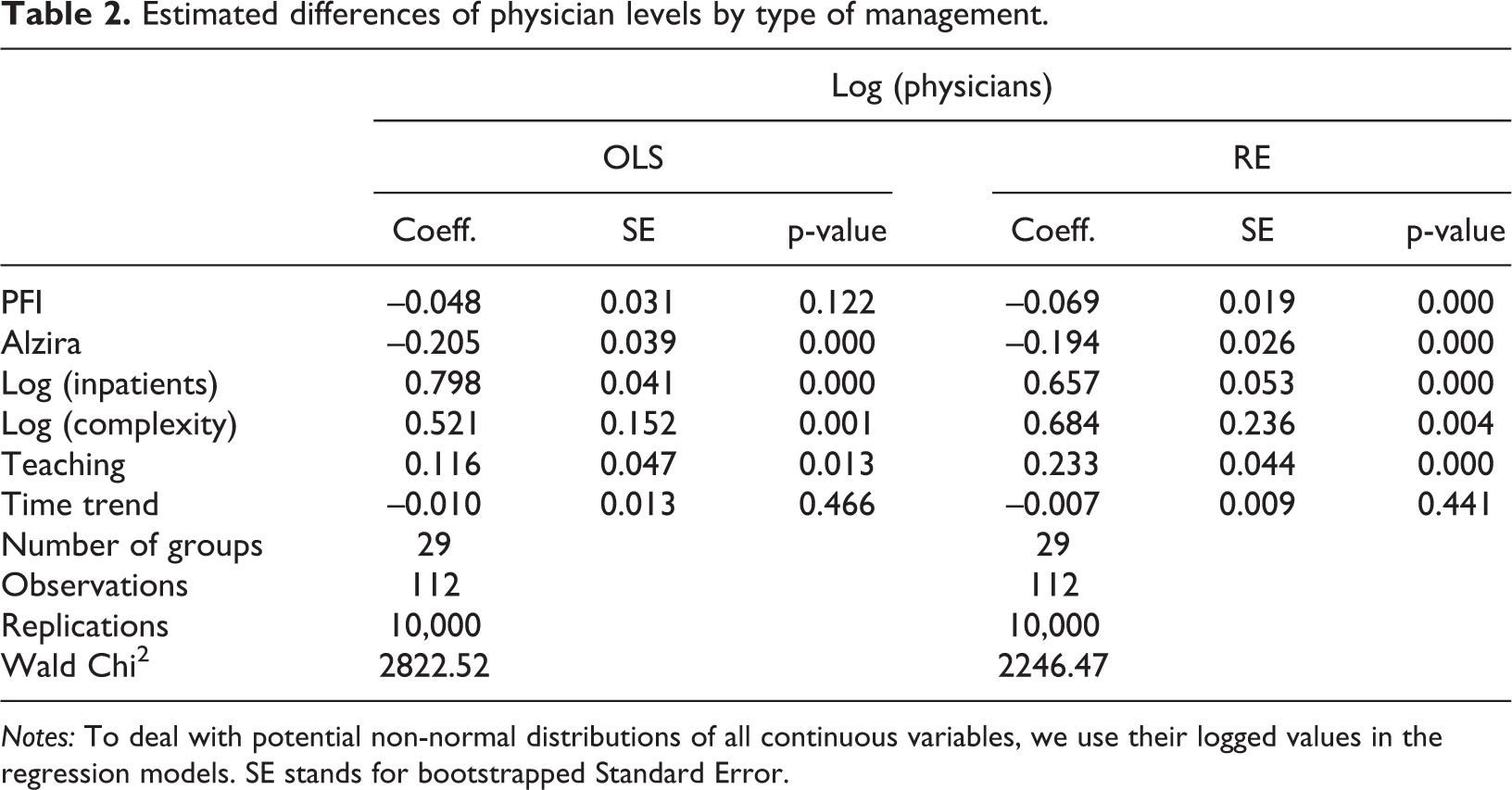
Notes: To deal with potential non-normal distributions of all continuous variables, we use their logged values in the regression models. SE stands for bootstrapped Standard Error.
Estimated differences of nursing staff levels by type of management.
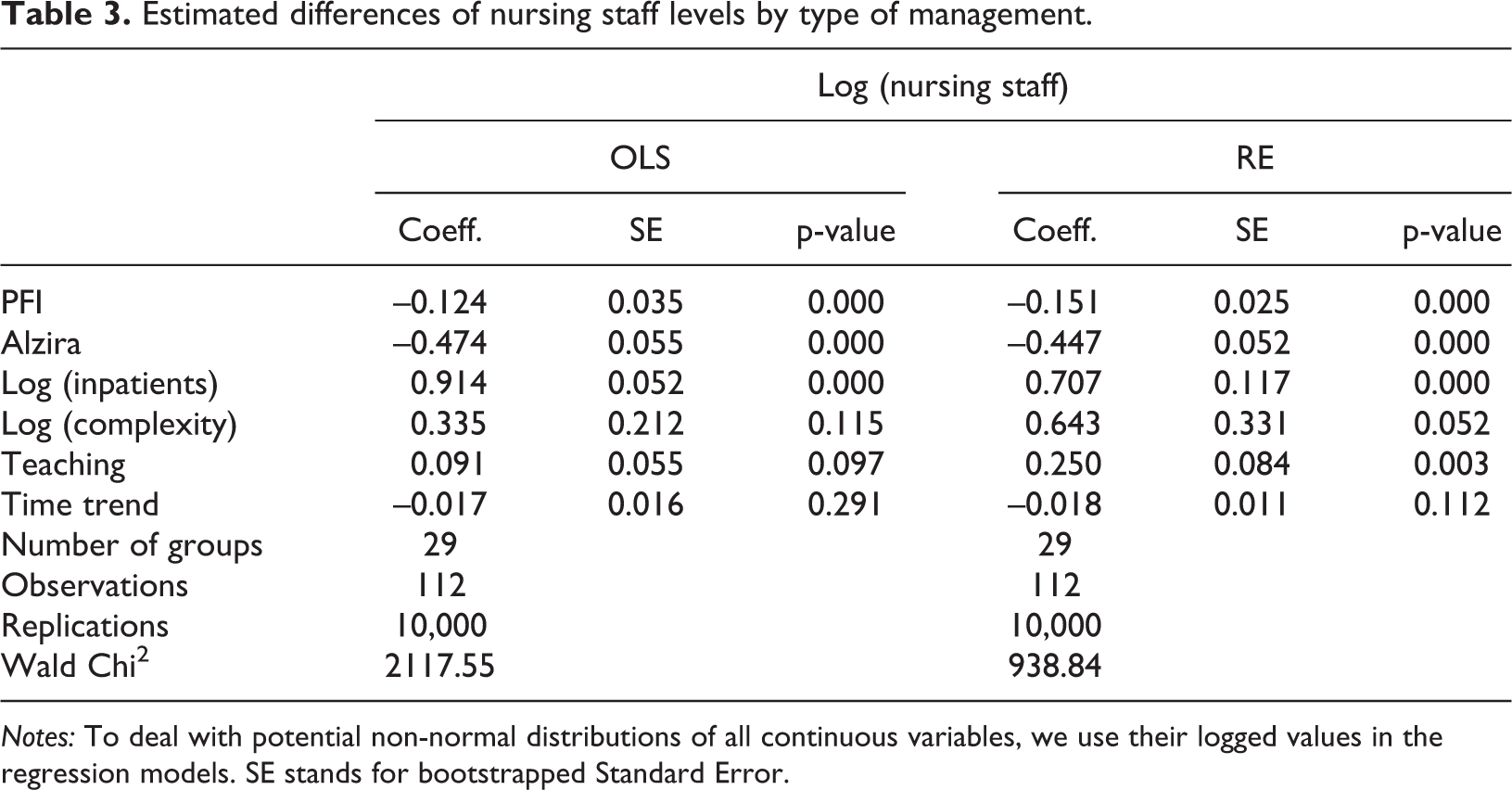
Notes: To deal with potential non-normal distributions of all continuous variables, we use their logged values in the regression models. SE stands for bootstrapped Standard Error.
Starting with the analysis of the total number of physicians, the regression model confirms our previous findings, i.e. that directly managed public hospitals employ substantially higher levels of physicians than Alzira models, which employ, on average, 20% fewer physicians than directly managed public hospitals; on the other hand, there is no clear evidence that PFI models are associated with lower physician levels; although PFI models seem to employ 7% fewer physicians than public managed hospitals when estimating an RE model. These results do not seem to be robust to an alternative model specification, i.e. the OLS model, which prevents us from clearly concluding that there is a substantial difference between PFIs and directly managed public hospitals in terms of physician levels. Turning now to the relationship between nursing staff levels and the management model, we find again that employment levels seem to be significantly lower in PFI hospitals and, particularly, Alzira models, compared to directly managed public hospitals; the coefficients associated with the PFI and Alzira management variables exhibit both a negative sign (about 15% and 45% fewer nursing staff respectively).
These results, we believe, have important theoretical and practical implications. From a theoretical perspective, our results are consistent with the efficiency and cost reduction rationales for private management of public service delivery. It is interesting, however, that clinical staff employment levels seem to be much lower in Alzira models, i.e. in those hospitals where the private sector operates both the clinical and non-clinical staff. This can be explained because of the different contractual characteristics of both models; while clinical staff in PFI models are managed through a public enterprise, in Alzira models the clinical staff are managed by a private firm, thus affected, a priori, by different incentive schemes. The profit maximization argument presented in the second section clearly applies to Alzira models but, as discussed, also to those management models involving public enterprises, such as clinical staff management in PFI models. Our results, however, suggest that profit maximization incentives seem to be way more powerful, in this case, than managerial/reputational incentives.
From a practical standpoint, however, it is interesting to note that these potential efficiency gains derived from better labour productivity do not seem to hold in practice; a recent study by Alonso et al. (2015) found that reform of hospitals belonging to the SERMAS did not lead to technical efficiency gains. Their results suggest that market-based hospital governance models are not to be necessarily better – or worse – than public management models. Thus, it seems that those lower employment levels associated with PPP models did not lead, in practice, to technical efficiency gains. Subsequent research is needed, therefore, to investigate the relationship between efficiency and employment in PPP hospitals. Further, an additional key question arises about the implications of employment reductions on service quality. The empirical evidence in this matter suggests, overall, that lower clinical staffing levels, particularly as regards nursing staff, are associated with worse patient outcomes (Aiken et al., 2002a, 2002b; Rafferty et al., 2007; Rogers et al., 2004). This may be so because reduced staffing may increase the workloads of clinical staff which adversely affects not only patient safety but also job satisfaction and staff burnout (Carayon and Gurses, 2008; Stimpfel et al., 2012). These poorer working conditions may contribute, in turn, to higher turnovers and may also help to explain why PPPs employ fewer clinical staff, since physicians and nursing staff may be reluctant to work in privately managed hospitals (Acerete et al., 2011; Bach and Givan, 2010; Stimpfel et al., 2012).
In sum, our findings illustrate that clinical staff employment levels seem to be substantially lower in PPP hospitals than in public direct managed ones, particularly as regards nursing staff and in those types of hospitals known as Alzira models, where the private sector manages both clinical and non-clinical staff. Despite the strengths of our analysis, the contributions of this study should be interpreted with care in light of several limitations. The main limitation of this study lies in our data characteristics and number of observations, which prevent us from using alternative identification strategies to approximate causal effects. In addition, although it would be of great interest to analyse the implications of employment reductions in working conditions and patient outcomes, the lack of publicly available data limited our ability to further investigate these important issues in our context.
Conclusion
In this paper, we have analysed variations in clinical staff employment levels attributable to implementing different types of PPPs in the SERMAS. In so doing, we compared employment numbers across three types of management models, namely, directly managed public hospitals, PFIs and Alzira models, using simple non-parametric statistical techniques and multivariate panel regression analysis. The case of Madrid is of particular interest because contracting out services in healthcare has led to the adoption of different PPP schemes to govern public hospitals from the 2000s; Madrid seems to be, therefore, a useful set up to assess differences between hospital governance models. To date, there is little scholarly work on the employment effects of different forms of PPP, which may have important detrimental consequences for service quality and patient safety.
Our findings suggest that PPP schemes in Madrid are associated with substantially lower levels of clinical staff, when compared to directly managed public hospitals, particularly regarding those hospitals governed through the so-called Alzira model. Our research suggests, therefore, that hospitals managed under private schemes are motivated to cut costs and increase efficiencies, and a major way of doing this is to reduce the number of staff hired. It is a moot point whether these hospitals actually attain efficiency improvements and cost reductions. What is clear is that these lower employment levels associated with PPP schemes, particularly as regards nursing staff, may have a number of undesirable consequences in terms of patient safety, since understaffing may lead to increased workloads which, in turn, seem to be associated with higher rates of some adverse patient outcomes. From a policy perspective, the implications of lower staffed hospitals may be, therefore, that a larger number of patients will suffer avoidable adverse outcomes, which, potentially, will increase patients’ length or stay and/or readmissions rates, thus increasing the final costs of healthcare and reducing any potential efficiency gains derived from reducing clinical staff.
Despite the strengths of the findings, there are several limitations of our analysis that offer opportunities for further research. Particularly, it should be highlighted that whilst some of the differences in employment levels may be due to cost-cutting and efficiency gains pressures faced by PPP schemes, the literature suggests the possibility that physicians and nursing staff refuse to work in PPP hospitals, particularly in Alzira models, because of their dissatisfaction with poorer working conditions and longer working hours. Unfortunately, due to lack of available data, we were not able to analyse those issues on this occasion. Subsequent qualitative research, exploring healthcare professionals’ perceptions of the effects of PPP implementation on contracts, job terms and working conditions and their potential relationship with worker stress, patient safety and satisfaction, would undoubtedly cast considerable further light on these important issues.
Footnotes
Acknowledgements
The research leading to these results has received funding from the European Community’s Horizon 2020 Programme under grant agreement No. 726755 (Project CITADEL: H2020-SC6-CULT-COOP-2016-2017). The authors also wish to thank the Editor and two anonymous referees for their helpful comments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.