
Abstract

Keywords
The Director-General of the World Health Organization (WHO) declared the COVID‑19 outbreak a global public health emergency of international concern under the International Health Regulations on 30 January 2020. The same body characterized COVID-19 as a pandemic on 11 March 2020 upon the advice of the International Health Regulations Emergency Committee (WHO, 2020a). The rapidly evolving nature of the COVID-19 pandemic required hospitals to have in place all essential preparedness. Such measures varied with the designated role of the hospital and had to be synchronized with the country’s overall plan for managing the pandemic. These roles included testing people for COVID-19 and early investigations to identify confirmed cases that require hospital care. A critical role was hospitals’ risk communication strategy in coordination with the central response system and communities to contain and mitigate the pandemic (WHO, 2020b).
While volatile, uncertain, complex and ambiguous is a universally accepted phenomenon, the novel COVID-19 virus and associated uncertainties overwhelmed the healthcare systems around the world. Unprecedented situations do not have readymade solutions. As the situation continues evolving, countries must be prepared, adapt and respond swiftly. Central and state governments of India took a series of measures to break the chain of transmission. The Government of India (GoI) adopted a ‘whole of government approach’ for responding to the COVID-19 emergency. In India, dedicated COVID hospitals (DCH) provided comprehensive care primarily for those clinically assigned as severely infected. (Director General of Health Services, 2020) The total number of hospital beds in Delhi was 54,321 in the fiscal year 2019–2020 (Planning Department, 2021). Essentially, there were only 300 beds per 1 lakh people instead of 567 hospital beds per 1 lakh people as recommended by the Bhore Committee. The total number of hospital beds in the National Capital Region 1 (NCR) region was inadequate even during usual circumstances. The shortage of beds increased due to urgent COVID care requirements. Various ministries of the government initiated the construction of 1,000-bedded DCH to bridge the gap. Design, development and operationalization of a DCH facility in Delhi, the capital of India, started on a war footing on 24 June 2020. The DCH was made operational on 5 July 2020. In 12 days, this large makeshift facility, spanning 28 acres of land, was set up in a hangar-based temporary structure.
This DCH supported the increasing medical needs of the public and enhanced the ability to cope with the pandemic. This paper discusses the challenges faced in outsourcing services and facilities in such a hangar-based hospital.
The DCH took care of many COVID-19 patients. The Manual for Procurement of Consultancy and Other Services 2017 (Department of Expenditure, 2017), along with General Financial Rules 2017 promulgated by the Ministry of Finance (General Financial Rules 2017), was the backbone of planning and operationalizing the outsourcing in the DCH. Government guidelines were followed and are used to describe the outsourcing process of DCH throughout. They provide a blueprint for the early readiness of future facilities. In fact, they were utilized for quick construction of DCH in locations such as Patna (Bihar), Muzzafarpur (Bihar), Pune (Maharashtra) and Ahmedabad (Gujarat). The DCH was shut in November 2020 but was re-operationalized on a similar premise in April 2021. We believe this knowledge would be of benefit to administrators should similar situations arise in the future, and managerial interventions to alleviate them would be smoother.
OUTSOURCING
Government organizations procure various goods and services and undertake works to fulfil their duties and responsibilities. Outsourcing of services means deploying outside agencies on a sustained long term (for one year or more) for the performance of other services. Outsourcing is the procurement of products or services from sources that are external to the organization. Outsourcing is a choice when an outside organization can complete certain support functions faster, cheaper, or better. Tasks that are not core competencies of the organization are candidates for being contracted out (Lankford & Parsa, 1999). However, hospital administrators must ensure that the outsourced services are being, and continue to be, performed by qualified individuals regardless of the service they are providing. Although many positive aspects of outsourcing seem very enticing to senior hospital leadership, there are just as many potentially harmful aspects. The primary benefits of outsourcing in healthcare include cost-cutting.
There are cost savings from reducing in-house full-time and temporary staff. This cost saving allows healthcare organizations to invest capital in new medical equipment and supplies (Hazelwood et al., 2005). Externalizing non-core activities, critical to process-oriented organizations, allows them to concentrate on the core activities and leverage nuclear capacities (Wigglesworth et al., 1998). There are legal, ethical and perhaps moral issues when considering outsourcing. Legal issues are complex and diverse, but some are important to understand when entering an outsourcing contract (Roberts et al., 2013). A few disadvantages of outsourcing in healthcare could be losing control of suppliers and discontinuity of service quality levels (MacCutcheon & Griffin, 2002), accountability issues, loss of competencies (Hazelwood et al., 2005), information confidentiality problems, excessive supplier dependency and consequent loss of flexibility (Renner & Palmer, 1999). There is a need for transparency in decision-making and reducing the scope for subjectivity by government agencies while utilizing public money for procurement. Consonance with the fundamental principles of transparency, fairness, competition, economy, efficiency and accountability is a must.
OUTSOURCING IN 1,000-BEDDED DCH
The provision of assets (such as heating, ventilation and air conditioning (HVAC) systems), or services (such as catering) or both (such as laboratory) was identified for outsourcing. There was a predefined allocation of risk between the outsourced agency and the public entity. The outsourced agency received performance-linked payments that conformed (or were benchmarked) to specified and predetermined performance standards and deliverables. Measurable service-level agreements by the public entity or its representative for cases such as dietary services, where the number of meals provided determined the payments, were utilized.
The biggest challenge was the timeline for the construction and commissioning of a fully functional DCH. These constraints made adhering to standard protocols for outsourcing a challenge. As a result, a blanket waiver was granted by the Ministry of Finance from routine procedures of procurement and outsourcing, along with powers for emergency procurement and outsourcing of services. This timely financial carte blanche helped in ensuring timelines were met while outsourcing.
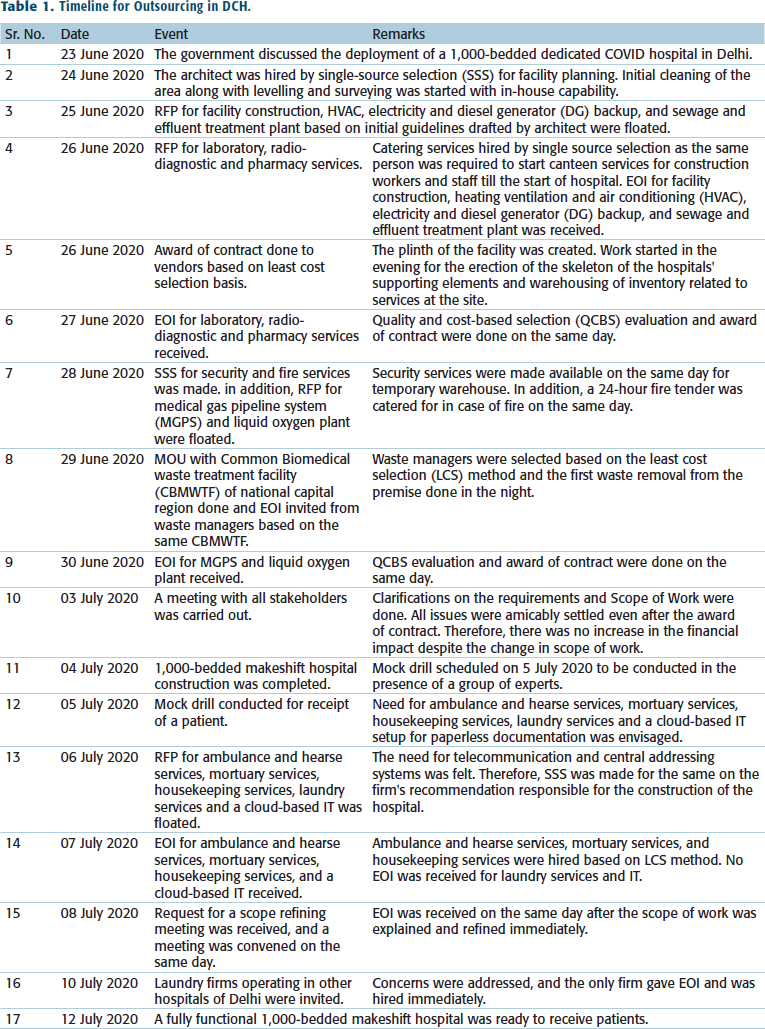
Table 1 depicts the timeline of the outsourcing exercise at different stages of the project, from conception to service delivery.
Timeline for Outsourcing in DCH.
Identifying the Need for Consultancy Services
In-house capability or capacity was inadequate for required services such as planning, designing and operationalizing in a highly infectious area. In addition, architectural planning and construction of the DCH, including mechanical-electrical-plumbing, HVAC and sewage and effluent treatment plant, were a challenge. The DCH administration also felt a need to transfer knowledge/training/capacity and capability building as a value addition to such engagement and utilize the opportunity to develop a cloud-based IT infrastructure. The need for qualified consultants who would provide specialized, high-quality services such as designing and operationalization of the highly sophisticated medical gas pipeline system (MGPS) and the source of oxygen (58 Kilo Litre Liquid Medical Oxygen Plant), fire safety services, security services, housekeeping services and biomedical waste management services was felt. Sourcing essential non-core services such as IT, security and fire safety did not pose an issue. They were available at established and immutable standards. Constitutional laws and regulations such as Biomedical Waste Management Rules 2016 regulate biomedical waste management as a service, which enforced mandatory hiring by the state.
In many instances, there was a definite existence of internal capacity/capability to do the job, but considerations of economy, speed and efficiency concerning additional requirement/commitment required outsourcing. Such services included laboratory, radio-imaging, pharmacy, ambulance and hearse services, mortuary and dietary services. All the services except pharmacy were hired based on output (i.e., number of meals provided or X-rays done per month).
Preparation of Procurement Proposal
Each service was assigned a separate nodal officer under a qualified hospital administrator. The administrator prepared a purpose/objective statement of services. A formal proposal and justification for the services was prepared, highlighting the requirement, purpose/objectives and scope/outcomes of the assignment. At this stage, the administrators identified eligibility and pre-qualification criteria to be met by the consultants/service providers. While it may seem elementary or academic, this step turned out to be a critical first step in adequately designing a procurement proposal. Finally, an outcome statement delineated all expected outcomes along with the time frame.
Shortlisting of Consultants/Service Contractors/Contractors and Their Technical Evaluation after Consideration of Quality
The technical and financial capability of consultants is a crucial though indirect determinant for quality and scope of performance. However, the quality and scope of consultancy/other assignments are not always tangible and consistently measurable. Thus, a two-stage process selected consultants. In the first stage, a shortlist of possible consultants/service contractors/contractors was done. In the second stage, the shortlisted consultants were sent a request for proposal (RFP) to submit an expression of interest (EOI) along with a bill of quantity. Evaluators evaluated the technical proposals without access to the financial part of the proposal. The same evaluators were involved in the financial evaluation after the quality evaluation. Such a two-stage bid (technical and commercial) is known as the quality and cost-based selection (QCBS).
Different selection systems of consultants/service providers were employed to achieve appropriate relative importance (weightage) of quality and price aspects. The decision on the system of selection was preceded by assessing the capacity of DCH to engage and supervise the implementation of the proposed assignment. The selection method chosen depended on this assessment.
A price-based system (also known as least cost selection) allows allotting marks for various technical criteria/attributes. These criteria were provided to shortlisted consultants/service providers. Consultants/service providers were required to submit both a technical and financial proposal simultaneously. The technical proposals were opened first and evaluated. The offers qualifying as per these technical evaluation criteria were considered technically responsive. The rest were dropped from the list. Financial proposals were then ranked for only eligible and responsive offers. The lowest offer out of the responsive offers was selected on price criteria alone after technical qualification. This method was used for services of a standard or routine nature with well-established practices and standards. Such services included housekeeping, ambulance and hearse, fire safety, security, dietary and laundry services. The respective nodal officers of the services had chalked out mandatory and inescapable quality parameters. They weighted them so that each parameter could be allotted marks to form 100. Initially, the minimum qualifying marks for the quality of the technical proposals prescribed as a benchmark was 85 out of a maximum of 100. However, they were reduced to 60 in laundry services due to the lack of vendors. The scheme of marking or its application could have been subjective. However, nodal officers were chosen based on their experience in the field. Technical criteria were not relevant in the case of dietary services. For instance, the firm’s financial standing had no overall impact on the quality of food offered. It was therefore instructed from the early stages that ingredients would be standardized and approved by the nodal officer before use. The contract could be terminated unilaterally without giving cause. However, such a situation never arose. The supply of meals became the highlight of all the services provided to the patients.
In contrast to the above method, QCBS was used for highly technically complex and critical assignments. It is justifiable to pay an appropriately higher price for higher quality. The minimum qualifying marks were benchmarked at 80 out of 100 marks for the technical proposal. Quality score was then assigned out of 100 marks to the technically viable vendors. The financial proposals were given a cost score based on the relative ranking of prices, with 100 marks for the lowest and pro-rated lower marks for higher-priced offers. The total score was obtained by weighing the quality and cost scores and adding them. The weightage given to the cost score was 30%, while the technical score was given a weightage of 70%. A system was evolved for conciliation and moderation of widely disparate markings by different evaluation committee members composed of nodal officers of various services. This system was utilized to outsource essential paramedical services such as laboratory, radio-diagnostics, pharmacy, mortuary, MGPS and liquid oxygen plant.
Outsourcing of facility planning and construction, including HVAC, electricity and diesel generator (DG) backup and sewage and effluent treatment plant, biomedical waste management, general waste management and IT services were procured through direct selection or single source selection (SSS). SSS was adopted due to the COVID emergency, where timely completion was of utmost importance. The evaluation of consultants’ capabilities and eligibility to undertake assignments was assessed beforehand. The assessment was based on their experience of handling similar types of projects, the strength of their workforce, and the firm’s financial strength. SSS was employed within the gambit of corporate sector responsibility, and price negotiations were easy.
Negotiations and Award of the Contract to the Selected Firms
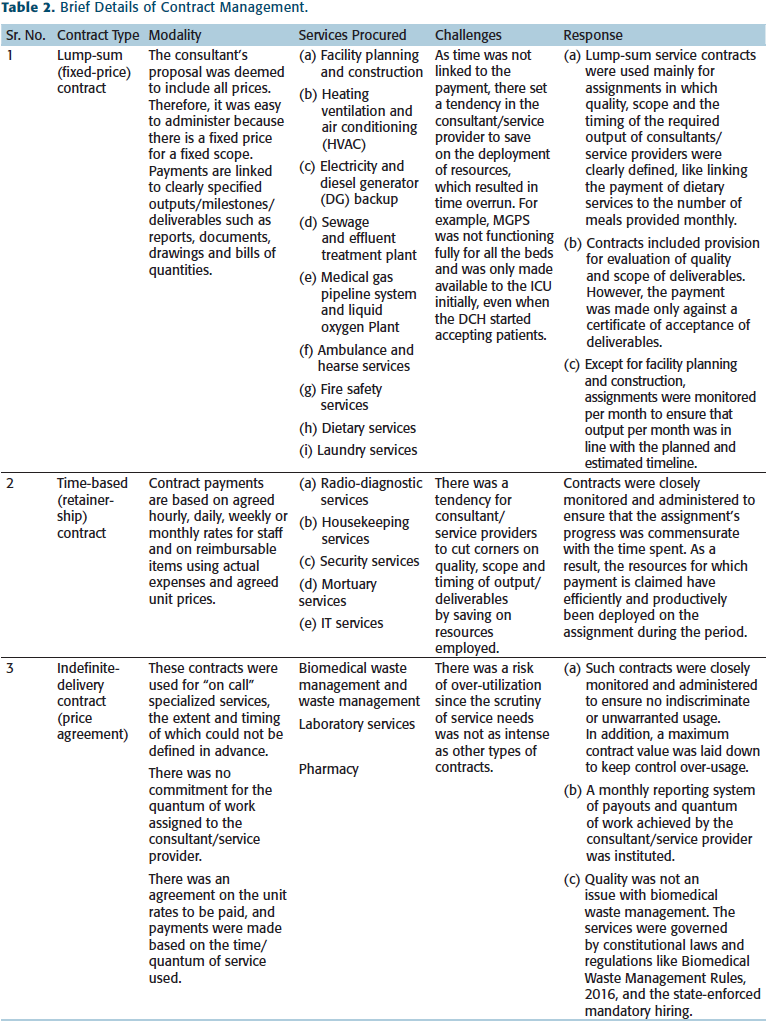
The different basis for linking payments to the performance of services was carefully chosen, as adopting the wrong type of contract could lead to contractual disputes and non-performance / failure. Depending on the nature of services, contracts were either lump-sum contracts, time-based (retainer-ship) contracts, or unit/rate-based contracts—or a mix of these. In some uncertain but regularly needed services, indefinite-delivery contracts were deemed appropriate based on time or unit rates. The details of contract management are given in Table 2.
Brief Details of Contract Management.
UNIQUE LEARNING SITUATIONS
Laundry Services
A suitable vendor for the hospital laundry services was hard to find. Administrators were unaware of the technical requirements for the service as not much was known about COVID. Many firms were also sceptical of losing business if other clients became aware that they were handling COVID-infected laundry. Some firms expressed an inability to attain break-even with the initial laundry load of DCH because most of the load comprised only scrubs. A list of suitable vendors was obtained from another functioning DCH in Delhi. The vendors on that list were contacted and subsequently selected. The selection of the laundry service vendor was based on the fact that the same vendor was handling laundry services for other COVID care hospitals and quarantine centres. Hospital administrators were consulted to frame the technical parameters for the final contract document. The turnover time for the launderette was increased to 72 hours to help the vendor achieve break-even for the mechanical laundry operationalization. This increase in the turnaround time to facilitate the break-even of the vendor led to the problem of an inadequate number of scrubs and other linen in the usable inventory of the hospital. Six sets of laundry and linen were maintained so that three sets were in circulation. This practice helped to tide over the prolonged turnover time of 72 hours. However, stock-taking became an issue. All the linen and laundry were dipped in Sodium Hypochlorite solution, increasing the weight of the laundry. However, the weight of the laundry returned was less. Manual counting of laundry could not be undertaken since the laundry was highly infectious. Therefore, a lump-sum contract was made, and all the linen and laundry were tagged. A fixed load was given to overcome the challenge of stock-taking and accounting of the laundry.
Housekeeping Services
The temporary nature of the DCH and the horizontal spread with segregations into red and green zones necessitated that a comprehensive set of technical parameters be included in the contract document to ensure the required standard of housekeeping services. Shifts of 8 hours and 30 minutes were planned with 30 minutes of overlap between preceding and subsequent shifts to allow for donning and doffing time for staff. The workforce was distributed such that there was maximum availability during daytime and a reduced but effective strength for the night-time as the services requirement was less. Regular information education and communication activities and training sessions for outsourced housekeeping staff were organized. The training effectiveness was assessed by checking service quality.
Pharmacy
Though operating in a COVID environment in other locations, the vendor selected had no experience functioning out of a hangar-based DCH. The vendor was also concerned about the health risk of the staff. However, these concerns were addressed when the pharmacy was placed in the green zone. The DCH is a Greenfield project, and the expected patient footfall was unknown at the outset. The vendor was unclear about how much and what inventory they had to maintain. Furthermore, there was no means of receiving a physical indent from the red zone as material and personnel could not enter the green zone where the pharmacy was located. The hospital information system was not equipped with e-signature facility. This proved to be a hindrance in the management of demands from and issued to wards in the red zone. Hospital administrators were consulted, and data from the COVID Nodal Centre was analysed to create a predictive model for the first fifteen days of operations after the inauguration of the DCH. The vendor was told to keep specified extra stocks on standby to cover any surge in footfall. Personnel from the hospital administration were embedded within the pharmacy. They were made responsible for noting the demand as conveyed telephonically by the staff on duty in the red zone. They signed the indent on behalf of the red zone staff member. They then verified the quantity being issued from the pharmacy and notified the red zone staff to collect it from the collection area created explicitly at the green and red zone interface.
CONCLUSION
Setting up and operationalizing a Greenfield 1,000-bedded DCH in a short while will always remain a challenge. The timeline and the shortage of trained workforce to take on non-core and specific core duties also meant that outsourcing such services was the only viable option. The usual timelines, processes for vendor selection, contract framing and implementation were unavailable. The GoI’s financial carte blanche to do the needful in a short time helped hasten the process. Despite having troubles with outsourcing various services, the active cooperation of hospital administrators ensured successful operationalization. Extraordinary times necessitate extraordinary measures; hence, situational sensitivity and behavioural flexibility are required while handling these situations. Time for proper vendor selection and vetting is deficient in emergencies. Every hospital should have a reliable vendor base for all services. The inclusion of requisite technical requirements was ensured in the contracts by the early involvement of the hospital administrators. Technical proposals for consultancy services are an intellectual product and not an arithmetic exercise. Their evaluation must be based on the individual professional judgement of competent evaluators. Every hospital and government should make standard operating procedures for such emergencies to sail through swiftly and efficiently during such testing times.
Footnotes
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
FUNDING
The authors received no financial support for the research, authorship and/or publication of this article.
NOTE
e-mail:
e-mail:
e-mail:
e-mail:
e-mail: