
Abstract
Background
Cognitive impairment is common in multiple sclerosis (MS). Transcranial direct current stimulation (tDCS) combined with adaptive cognitive training (aCT) may improve clinical outcomes.
Objective
To evaluate the effect of active vs. sham home-based tDCS + aCT on cognitive function.
Methods
Participants with MS and fatigue, without depression or severe cognitive impairment, were randomized to complete 30 remotely supervised 20-minute sessions of active (2.0 mA) or sham tDCS targeting the left anodal dorsolateral prefrontal cortex, paired with aCT. Randomization was stratified by high (H) vs. low (L) EDSS. The Brief International Cognitive Assessment in MS (BICAMS) was administered at baseline and intervention end, with scores converted to demographics-adjusted z-scores.
Results
Out of 117 participants, 106 completed BICAMS assessments. Compliance was high; 92% completed >25 sessions. Mean change in BICAMS z-score was significantly greater in the active (n = 55: 0.06 ± 0.56) versus sham (n = 51: −0.16 ± 0.50) group (p = 0.035). The interaction between treatment and EDSS for BICAMS z-score was not significant (p = .254), but benefits were greater in H EDSS (−0.00 ± 0.57 vs. −0.37 ± 0.39; p = .022) than L EDSS (0.11 ± 0.56 vs. −0.01 ± 0.53; p = .411).
Conclusions
Active vs. sham tDCS + aCT resulted in significantly better cognitive outcomes, with the greatest benefit in those with high neurologic disability.
CLINICALTRIALS.GOV; https://clinicaltrials.gov/study/NCT03838770; IDENTIFIER: NCT03838770
Introduction
Cognitive impairment is a common symptom in multiple sclerosis (MS), often starting with slowed information processing, a consistent early deficit.1–3 This can progress to affect executive function, verbal fluency, learning, memory, and reasoning.4,5 Growing evidence supports combining transcranial direct current stimulation (tDCS) with adaptive cognitive training (aCT) to address cognitive impairments in various neurological conditions.6–8
tDCS is a noninvasive brain stimulation technique that delivers low electrical currents through electrodes placed on the scalp, positioned to direct the current to specific cortical regions of interest. 9 These currents, typically ranging from 1 to 2 mA, modulate neural activity and promote neuronal plasticity. Targeting the dorsolateral prefrontal cortex (DLPFC), which plays a central role in attention, working memory, and executive function, 10 enhances task-based functional connectivity and may improve cognitive performance in these domains.7,8
When combined with cognitive training, tDCS enhances and prolongs training effects.9,10 Intensive aCT complements tDCS by engaging the same targeted substrate of the DLPFC, reinforcing neural plasticity and enhancing cognitive function. aCT delivers repetitive, real-time adaptive exercises through web-based programs designed to strengthen synaptic connections and enhance processing-level cognitive functions such as attention, working memory, and executive control.11–14 By continuously adjusting task difficulty based on user performance, aCT maintains an optimal cognitive challenge, ensuring sustained engagement while minimizing frustration. It has demonstrated significant cognitive benefits in neurological conditions, including MS. In a large randomized trial, 60 hours of aCT over 12 weeks led to greater neuropsychological improvements compared to computer games. 15 Findings from additional MS trials further support aCT's efficacy for cognitive rehabilitation.16,17
To enable extended dosing, which is essential for maximizing tDCS and aCT effects, we developed a remotely supervised tDCS (RS-tDCS) protocol. This telehealth-based approach allows participants to complete tDCS sessions at home with clinician oversight, improving accessibility, adherence, and scalability for real-world implementation. 18 A pilot study in MS using this protocol showed significant improvements in information processing speed after 10 sessions compared to aCT alone, with participants also reporting reduced fatigue.6,19 Fatigue, affecting up to 70% of MS patients, 17 is a debilitating symptom with few effective treatments. 20 Hypothesizing that fatigue reduction results from increased arousal and modulation of frontally mediated systems,21,22 a sham-controlled pilot of 20 tDCS + aCT sessions found significant fatigue reduction in the active condition. 19 Building on these findings, the BOOST-MS-FATIGUE trial, a large sham-controlled randomized control trial (RCT), tested 30 sessions of home-based tDCS + aCT in MS patients with significant fatigue as the primary outcome, with cognitive functioning assessed as a secondary outcome. 23 The primary trial findings found no significant difference in fatigue reduction between the active and sham groups, though both groups experienced improvements. 23 Here, we report the secondary cognitive outcomes of this trial, providing additional evidence for the efficacy of tDCS + aCT in addressing cognitive impairments in individuals with MS and fatigue, after screening out those with severe cognitive impairment. Here, we report the secondary cognitive outcomes of this trial, providing additional evidence for the efficacy of tDCS + aCT in addressing cognitive impairments in individuals with MS, fatigue, and screened out for severe cognitive impairment.
Methods
Participants
Participants were 18–75 years old; were diagnosed with clinically definite MS, 24 any subtype, and with at least moderate MS-related fatigue (Fatigue Severity Scale [FSS] 25 score ≥ 36); and did not have clinically significant depression (Beck Depression Inventory-Fast Screen [BDI-FS], 26 score ≤ 10). The BDI-FS was included to assess the intervention's effect on fatigue-specific symptoms while minimizing confounding from depressive symptoms, which often overlap with MS-related fatigue. It was selected for its strong psychometric properties in MS, including high internal consistency (Cronbach's alpha = ∼0.85–0.90).27,28
Participant eligibility was confirmed by an NYU Langone Health MS division neurologist, who ensured that the participant met medical eligibility including no other primary neurological or psychiatric disorder other than MS, as well as having medical clearance to undergo tDCS (i.e., not pregnant or breastfeeding, no medical devices implanted in the head or neck, no skin disorders/sensitivity near the area of stimulation); and was visually, physically, and cognitively competent to take part in study procedures. Participants had not had a relapse or begun any new pharmacological treatments for fatigue in the month before the commencement of the study.
To ensure their ability to understand and participate in study procedures, potential participants were required to have no more than moderate cognitive impairment (Symbol Digit Modalities Test [SDMT] 29 age-normative z-score ≥ –3.0) and estimated premorbid level of cognitive functioning in at least the average range (Wide Range Achievement Test [WRAT-4] 30 reading recognition subtest standard score ≥ 85).
Study design
This sham-controlled RCT employed a 6-week, double-blind, parallel-arm design (Figure 1). Randomization was stratified based on low vs. high Extended Disability Status Scale (EDSS) 31 score (low: 0–3.0, high: 3.5–7.5) to ensure a balanced representation of MS neurologic impairment across intervention groups. Study tDCS devices were preprogrammed to administer either active or sham tDCS by an unblinded team member, who was not involved in the study, ensuring double-blinded delivery of the intervention. This study was approved by the institutional review board of NYU Langone Health (New York, NY, USA). Before any study procedures, all participants provided written informed consent.
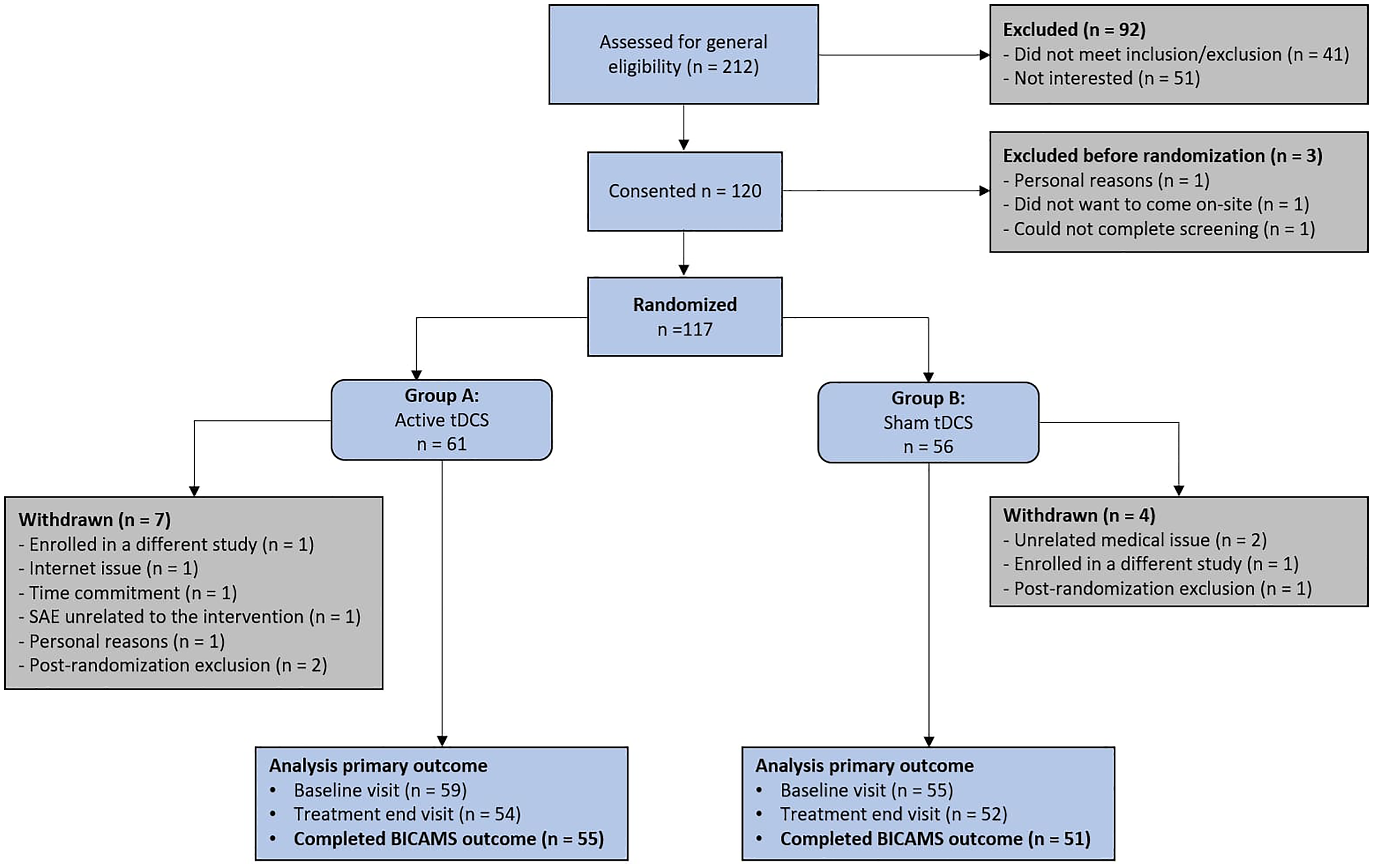
CONSORT diagram showing the progress of participants through the study.
During the initial tDCS visit, participants were introduced to the study equipment and received training on its operation. Before the first treatment session, participants underwent a 90-second tolerability test to ramp current up and down to the target stimulation intensity of 2 mA, ensuring their comfort during stimulation. If a participant reported a pain rating of 7 or higher on a visual analog scale from 1 (minimal) to 10 (most severe), or intolerable discomfort during the test, the current strength was reduced from 2.0 to 1.5 mA. If intolerable discomfort persisted at the lower current intensity, the participant was withdrawn from the study.
Following randomization, participants underwent a baseline assessment including the PROMIS Fatigue 32 questionnaire (primary outcome reported elsewhere) and the Brief International Cognitive Assessment in MS 33 (BICAMS) battery of cognitive tests (secondary outcome reported here).
All baseline assessment measures were repeated at the end of treatment for all participants. Participants were compensated $100 for their time.
Treatment protocol
Study equipment (Figure 2): The tDCS treatment sessions employed 1 × 1 mini-CT devices (Soterix Medical Inc., Woodbridge, NJ, USA). These devices feature large buttons and built-in safety features, facilitating supervised use at home. To ensure controlled access, study staff provided each participant with a unique, one-time use code to unlock the stimulation for their daily 20-minute sessions.

Study equipment overview. Panel A: 1 × 1 Mini-CT tDCS device; Panel B: SNAPstrap Headgear; Panel C: EASYpad Electrodes. The Soterix Medical tDCS device ensures safe and reliable stimulation using certified medical grade equipment.

Changes in BICAMS z-score, SDMT z-score, RAVLT z-score, and BVMT z-score outcomes between treatment groups, stratified and non-stratified by low versus high EDSS.
The device uses 5 cm × 5 cm sponge electrodes placed on the head following the OLE-system to effectively shape brain current flow to target the left DLPFC. 34 The way the headset and the sponge electrodes are designed makes them easy to put together properly with high reproducibility across sessions and participants. 34
To ensure consistency in screen size for the cognitive training, and to facilitate the video visit connections, all participants were provided with a standard study laptop (Lenovo or ASUS). The laptops were preconfigured for uniformity and secure connection with study staff via videoconferencing, data collection, and completion of cognitive training exercises.
tDCS intervention: tDCS was delivered with our remotely supervised protocol. 18 For both active and sham tDCS intervention, the sponge electrodes were positioned to target the DLPFC with the anode over the F3 area and the cathode over the F4 area (based on the 10–20 EEG system). For the active tDCS setting, the electrical current was gradually increased to 2 mA over 30 seconds and was maintained steady for 19 minutes, then slowly reduced over the last 30 seconds. For the sham tDCS setting, the device was preprogrammed to deliver three 60-second periods of gradual increase and decrease in the electrical current during the 20-minute session: initially, randomly at either the 7-, 10-, or 13-minute time point, and finally at the session's conclusion.
Adaptive cognitive training: Participants completed aCT via Posit Science's BrainHQ research portal during the stimulation period. 35 Five preselected exercises targeting auditory and visual processing and working memory (“Sound Sweeps,” “Memory Grid,” “Syllable Stacks,” “To-Do List Training,” and “In the Know”) were used. The portal's closed-loop algorithm dynamically adjusted task difficulty in real-time, focusing on weaker areas and expanding as skills improved. Exercises rotated each session, progressively increasing in complexity and speed to drive cognitive improvements over the 6-week intervention.
Intervention daily sessions: The intervention consisted of 30 DLPFC RS-tDCS sessions, conducted on consecutive business days (Monday through Friday) for 6 weeks. The stimulation session lasted 20 minutes at an intensity of 2.0 mA (active) or three periods of ramp up/down (low dose sham). During each daily session visit, participants connected with study staff via videoconference using the study laptops. This allowed staff to ensure proper headset placement, provide the single-use unlock code to initiate the session, and supervise the preprogrammed active or sham tDCS session in real time. 18
Study outcomes
Safety and tolerability outcomes: After each tDCS treatment session, safety was evaluated by assessing the types of minor adverse events (AEs) experienced and recording pain ratings. Participants were prompted to report and rate any AEs they experienced using a visual analog scale from 1 (minimal) to 10 (most severe). Any pain rating above 7, if not tolerable, led to discontinuation from the study.
Cognitive outcomes: With the combined tDCS + aCT intervention, participants were enrolled based on fatigue. The primary study outcome was change in the self-reported PROMIS Fatigue 36 scale and the secondary outcome was cognitive functioning. Participants were administered the BICAMS as a brief and repeatable assessment for assessing cognitive function in MS. 37 The BICAMS consists of three neuropsychological tests: the SDMT, 29 and the learning trials from the Brief Visuospatial Memory Test-Revised (BVMT-R) 38 and the Rey Auditory Verbal Learning Test (RAVLT, as an alternate to the California Verbal Learning Test-II). 39 The BICAMS measures have been validated for remote administration40,41 as followed in this study. The raw scores for each measure were calculated and converted to age- (BVMT-R; RAVLT)38,42 or age-, gender-, and education-(SDMT) normative z-scores. 43 These z-scores were averaged across the three measures to obtain a representative BICAMS z-score for each participant.
Analyses: We recorded baseline demographic and clinical characteristics. Baseline assessments were compared for participants randomized to active vs. sham tDCS. The primary statistical analyses that compare changes from baseline in the two intervention groups were performed on data from 106 participants who completed baseline and treatment end assessments (active tDCS: n = 55; sham tDCS: n = 51).
Statistical Methods: Baseline demographic and clinical variables are summarized by descriptive analyses. The secondary outcomes, including changes from baseline to the treatment end (TE) in BICAMS composite z-scores—comprising age-normative z-scores from the SDMT, RAVLT, and BVMT—are summarized using descriptive statistics (means, SDs, medians, ranges) and graphical displays (e.g., boxplots) by treatment group (Sham and Active) and strata (EDSS Low and High).
A 2 × 2 repeated-measure ANOVA analyzed cognitive outcomes, assessing the effect of Time (Baseline vs. TE), Intervention Group (Active vs. Sham), and their interaction. This was conducted on the full sample and within EDSS low and high strata. To further investigate significant interactions, post hoc pairwise comparisons were conducted using the Sidak correction to control for multiple comparisons, ensuring a more accurate assessment of group differences.
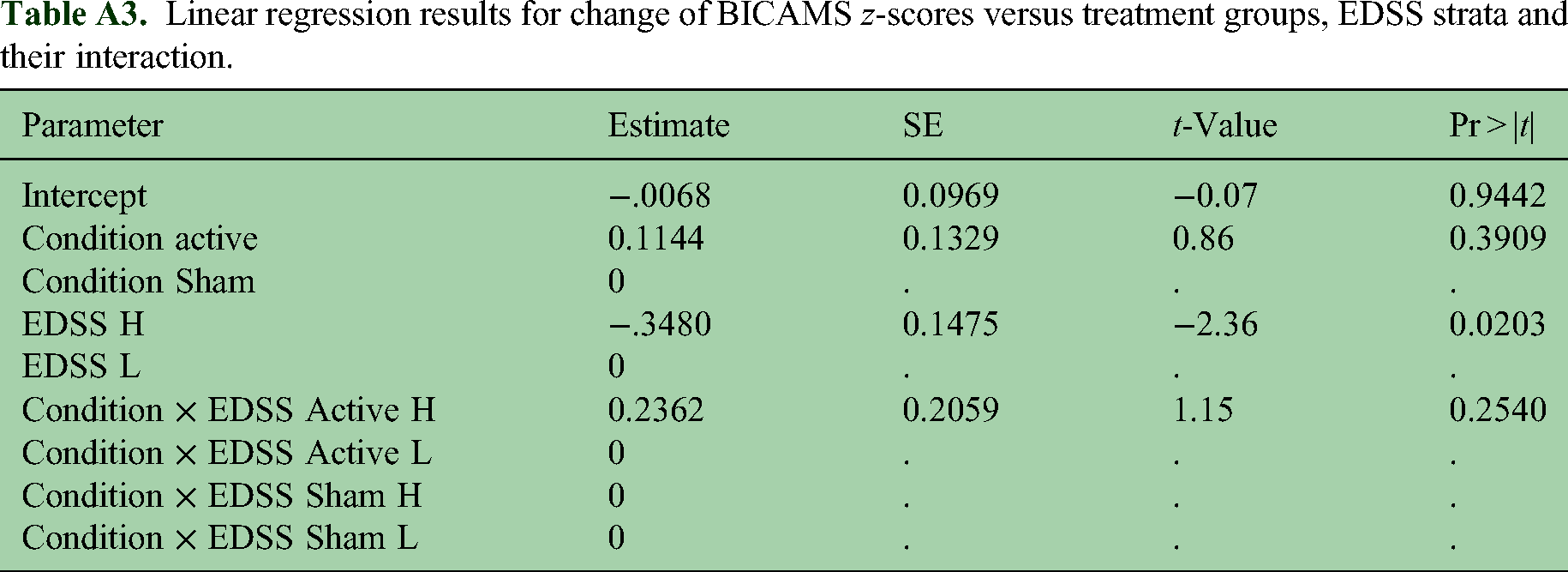
Two-sample t-tests were used to compare the means of these variables between the sham and active groups individually in EDSS low and high strata separately. Interactions between binary EDSS and treatments groups on these continuous variables were calculated using linear regression models and p-values are provided. The complete results of the linear models are provided in Tables A3‒A6 in the appendix. Similar analyses were conducted for these variables on the pooled non-stratified data. Descriptive analyses were also conducted for the randomized patients without endpoint data, with respect to baseline BICAMS, SDMT, RAVLT, and BVMT z-scores to evaluate potential bias. These results are provided in Tables A1‒A6 in the appendix. No multiple testing adjustments were used. All p-values reported here are unadjusted p-values (two-sided). p-values less or equal to .05 were considered statistically significant. R 4.2 and SAS 9.4 were used in the analyses.
Standard protocol approvals, registrations, and patient consents. The institutional review board of NYU Langone Health (New York, NY) approved this study. All participants provided written informed consent prior to any undergoing study procedures. The clinical trial is registered with clinicaltrials.gov (protocol ID: NCT03838770).
Results
Participants were recruited between April 2019 and February 2021 (Figure 1). Initially, n = 212 interested participants underwent prescreening, of whom n = 120 consented, and n = 117 were randomized using an intent-to-treat design. Exclusion from randomization occurred for three participants due to personal reasons (n = 1), inability to attend the baseline assessment on-site (n = 1), or inability to provide necessary screening information (n = 1). Of the randomized participants, n = 117 began their assigned interventions (n = 61 active, n = 56 sham), with n = 11 withdrawing from the study (Figure 2). Ultimately, n = 106 participants completed both baseline and follow-up assessments for the cognitive outcomes and were included in the analyses (n = 55 active, n = 51 sham). We also summarized the baseline BICAMS, SDMT, RAVLT, and BVMT z-scores for the 11 randomized patients without outcome evaluations in Tables A1‒A2 in the appendix.
As the intervention was conducted remotely, enrollment for the trial continued throughout the COVID-19 pandemic until its conclusion. The protocol was adjusted to deliver study equipment to participants’ homes, and baseline assessments (n = 54) and/or follow-up visits (n = 63) were conducted remotely using established and validated remote procedures. Table 1 provides an overview of the demographic and clinical characteristics of the n = 117 participants included in the intent-to-treat analyses.
Demographic and clinical characteristics of randomized participants (n = 117) by treatment group (active vs. sham tDCS) and strata (low vs. high EDSS score).

EDSS: Extended Disability Status Scale; PPMS: primary progressive MS; RRMS: relapsing-remitting MS; SPMS: secondary progressive MS.
Safety and tolerability
There were no serious AEs, and the intervention was well tolerated. Across all participants in both conditions, n = 9 AEs were rated > 7 on the visual analog scale; in all instances, after a safety check clearance by the study technician, the session resumed. One participant discontinued one session due to discomfort at the stimulation midway check-in point. Otherwise, all AEs were reported as mild in intensity and resolved after the session ended.
Feasibility. In the 117 individuals randomized, an average of 26 ± 9 sessions were completed; only four patients withdrew before completing any sessions and seven withdrew who completed fewer than 10 sessions. Attrition remained minimal, demonstrating a high level of fidelity to treatment, with 92.0% of participants completing at least 25 of the 30 sessions by the end of treatment.
Blinding. Blinding effectiveness was tested by asking participants after the follow-up assessment to guess their group assignment (active or sham) at study end. Specifically, 38% of the participants assigned to the active group and 52% of those in the sham group believed they received the active treatment condition (p = .179).
Cognitive outcomes. At the baseline, the active vs. sham groups did not differ in their performance on the BICAMS cognitive outcome (including SDMT-z, RAVLT-z, and BVMT-z, individually and combined).
Following intervention, at the group level BICAMS z-scores increased slightly in the active tDCS group (Baseline: −0.42 ± 1.14; TE: −0.36 ± 1.17) but declined in the sham group (Baseline: −0.48 ± 0.99; TE: −0.64 ± 0.97). There was no significant main effect of Time [F(1, 104) = 0.83, p = .37; η² = 0.008] or Intervention [F(1, 104) = 0.69, p = .41; η² = 0.007]. However, a significant Time × Intervention interaction [F(1, 104) = 4.52, p = .036; η² = 0.042] indicated greater decline in the sham group. Post hoc analysis confirmed a significant decline in BICAMS scores for the sham group (p = .038) but not the active group (p = .383).
No significant changes were observed for SDMT scores. RAVLT scores showed a significant main effect of Time [F(1, 102) = 9.71, p = .002; η² = 0.087], with a decline in the sham group (Table 2). BVMT scores also showed a main effect of Time [F(1, 91) = 5.43, p = .022; η² = 0.056], with improved performance in the active group, suggesting enhanced cognitive function in this domain (Table 2).
Post-hoc comparisons of primary and secondary outcomes between treatment groups (and stratified by binary EDSS).

In the EDSS High stratum, a 2 × 2 RM-ANOVA revealed a significant main effect of Time [F(1, 42) = 5.95, p = .019; η² = 0.124], indicating overall changes in BICAMS scores from baseline to the end of treatment. Additionally, a significant Time×Intervention interaction was observed [F(1, 42) = 5.68, p = .022; η² = 0.119], suggesting that the magnitude of change over time differed between the two groups. Post-hoc analysis showed a significant decline in BICAMS scores for the sham group (p < .001), but not the active group (p = .973). Similarly, a significant Time × Intervention interaction was found for SDMT [F(1, 42) = 4.39, p = .042; η² = 0.095], RAVLT [F(1, 40) = 5.89, p = .020; η² = 0.128], suggesting that the pattern of change in SDMT and RAVLT z-scores differed between the two groups.
In the EDSS High stratum (Figure 3), the changes in BICAMS z-score, SDMT z-score, and RAVLT z-score in the active group (−0.00; 0.07; −0.08, respectively) are greater than those in the Sham group (−0.35; −0.46; −0.77 respectively) [t(1, 42) = −2.34, p = .022, d = 0.72; t(1, 42) = −2.09; p = 0.42, d = 0.62; t(1, 40) = −2.42, p = .020, d = 0.76; respectively]. The interaction between EDSS and treatment group is significant for RAVLT z-score (interaction = 0.762, p = .043), suggesting that the effect of active vs. sham treatments is higher in the high EDSS group than in the low EDSS group.
There was a significant benefit of active tDCS compared to sham at the full group level. The active group showed a slight increase in their BICAMS z-score (+0.06), while the sham group experienced a slight decrease (−0.16), with this difference in change being statistically significant [t(1, 104) = −2.12, p = .035, d = 0.40]. Among the individual BICAMS tests, there was a trend toward greater improvement in the SDMT for the active group compared to the sham group, with the active group showing a slight increase in the SDMT z-score (+0.09) and the sham group showing a decrease (−0.16). This difference approached statistical significance [t(1, 103) = −1.66, p = .098, d = 0.33].
We noticed the significance of the interaction term for RAVLT z-score in Table 3, implying that we should report separately for EDSS Low and High strata for the comparisons of sham and active treatments. Therefore, Table 4 does not include the overall comparison results for RAVLT z-score.
Comparison of primary and secondary outcomes between treatment groups stratified by binary EDSS (stratified) (n = 106a).

EDSS: Extended Disability Status Scale; SDMT: Symbol Digit Modalities Test; BVMT-R: Brief Visuospatial Memory Test-Revised; RAVLT: Rey Auditory Verbal Learning Test; BICAMS: Brief International Cognitive Assessment for Multiple Sclerosis.
There are 11 patients either missing the baseline or TE values.
*P-values obtained by using independent two-sided t-tests to compare the change from baseline to TE (CHG) for the sham and active groups when stratified by low or high EDSS score.
Comparison of primary and secondary outcomes between treatment groups (nonstratified) (n = 106a).

EDSS: Extended Disability Status Scale; SDMT: Symbol Digit Modalities Test; BVMT-R: Brief Visuospatial Memory Test-Revised; BICAMS: Brief International Cognitive Assessment for Multiple Sclerosis.
There are 11 patients either missing baseline or TE values.
*P-values obtained by using independent two-sided t-tests to compare the change from baseline to TE (CHG) for the sham and active groups.
To examine whether the baseline cognitive impairment influenced intervention response, we conducted subgroup analyses stratifying participants by baseline SDMT z-score (z < 0, z < −0.5, z < −1.0, z < −1.5, z < −2.0). Across all cognitive impairment levels, intervention effects did not significantly differ between those with greater vs. lesser impairment. Instead, the primary moderator of cognitive benefits was neurological disability (EDSS), with greater cognitive improvements observed in participants with EDSS ≥ 3.5. In contrast, those with lower neurological disability (EDSS < 3.5) did not show significant cognitive differences between active and sham conditions. These findings suggest that neurological impairment, rather than baseline cognitive status, determines intervention response. To evaluate the potential bias in our results due to missing endpoint data, we compared the distributions of age, sex, race, ethnicity and the BICAMS Baseline z-scores of participants with missing endpoints to those with complete data using summary statistics and t-tests and Fisher's exact tests (Table A1 in the appendix). No multiple comparison adjustments were used. There were no statistically significant differences between the two groups with respect to any of the characteristics
Discussion
Cognitive impairment is a prevalent issue in MS and can significantly impact patients’ quality of life. This large sham-controlled RCT evaluated tDCS paired with aCT as an at-home intervention targeting fatigue in MS 23 , demonstrating its potential for improving cognitive function. The active tDCS group showed a significantly greater and slight positive mean change in the composite BICAMS score (mean increase of z-score = 0.06) from baseline to the end of the intervention compared to the sham group, suggesting a more favorable outcome in preventing the decline seen in the sham group.
The high fidelity to the intervention, with 92% of participants completing more than 25 tDCS + aCT sessions, underscores its feasibility and acceptability as a home-based approach for MS patients. This is noteworthy given the challenges of remote supervision and adherence to such interventions. As we previously demonstrated in a survey study, this telerehabilitation approach has the potential to be implemented at scale, offering opportunities to reduce costs and time commitment (e.g., minimizing commuting time) 44 while enabling much longer intervention periods (e.g., up to 50 daily sessions).45,46
This study reinforces the efficacy of remotely supervised tDCS with web-based aCT, which enhances accessibility, scheduling flexibility, and adaptive difficulty, improving adherence and engagement.15,44 Previous research indicates comparable cognitive benefits between remote and in-person CT.15,47,48 While home-based tDCS with aCT provides a scalable and accessible intervention, real-world implementation requires consideration of logistical challenges, clinician oversight, and cost-effectiveness. Ensuring long-term adherence and integrating this approach into standard clinical care will be critical for sustainability. Future research should explore strategies to optimize implementation, including logistical feasibility, clinician oversight, and cost-effectiveness, to support broader clinical adoption.
Overall, these findings are consistent with the large and growing literature supporting tDCS paired with training for recovery of function and prevention of cognitive decline,7,49 building on our earlier smaller sample results. 13 The BrainHQ training in this trial, with 10 hours over six weeks, was underdosed for producing measurable cognitive benefits compared to our original trial of 60 hours over 12 weeks. 13 While the cognitive benefit of tDCS alone has been reported, 40 our findings support the “boost” model, where tDCS targets the brain region engaged during training for functional targeting.50,51 Further research is warranted to explore mechanisms underlying these synergistic effects and optimize tDCS use in MS management.
The findings suggest that cognitive benefits in the active tDCS group primarily reflect stabilization rather than recovery. While tDCS + aCT has been associated with neuroprotection and cognitive maintenance, further longitudinal studies are needed to determine whether these effects persist over time and contribute to long-term cognitive prevention. While MS-related cognitive decline is typically gradual, certain subgroups, particularly those with higher EDSS scores, may be more vulnerable to decline over shorter timeframes. The decline observed in the sham group highlights this possibility, reinforcing the need for longer-term follow-up studies to assess the durability of these effects. The sham group experienced a decline, deviating from the typical stability in MS over months or years,52,53 but aligning with cognitive decline patterns in more severe disease. 53 These findings suggest that tDCS may help maintain cognitive stability and slow deterioration, but longer studies are needed to confirm its role in preventing sustained cognitive decline.
As with all sham-controlled trials, placebo effects remain a consideration. However, the lack of cognitive improvements in the sham group suggests that expectancy effects were unlikely to account for the observed benefits in the active condition. Future studies should continue refining sham control methods to further rule out subtle placebo influences.
The synergistic effects of tDCS combined with BrainHQ have been reported in MS,11,46 and other neurological conditions.40,45,55,56 Most relevantly, a recent review found tDCS + aCT effective for slowing cognitive decline in major depression and MCI. 57
Participants with higher neurological disability, as indicated by EDSS scores, experienced greater cognitive benefits. This suggests that individuals with more severe impairment may derive more significant advantages, highlighting the need for dosing optimization and predictive markers for response. However, EDSS primarily measures physical disability 58 and does not capture other critical aspects of MS-related disability, such as cognitive function, fatigue, and quality of life.
To evaluate whether baseline cognitive impairment influenced intervention response, we tested multiple SDMT cutoffs and found no evidence that cognitive function moderated outcomes. Instead, cognitive benefits were primarily observed in those with higher neurological disability (EDSS ≥ 3.5), regardless of baseline cognitive status. These findings suggest that intervention effects may be more dependent on the level of overall neurological impairment rather than cognitive status alone. Following current convention in MS clinical trials, we relied on the EDSS as a standardized measure at the level of global disability classification. While EDSS is widely used and provides a standardized assessment of physical disability, 58 it has notable limitations in capturing the full spectrum of disability in MS. Alternative measures, such as the patient-determined disease steps 59 and multicomponent functional assessments like the multiple sclerosis functional composite, 60 offer broader evaluations that incorporate motor function, upper limb function, and cognition. Additionally, symptom-focused scales, such as the SymptoMSscreen, 61 and quality-of-life measures capture aspects of disability beyond mobility, including the full spectrum of symptoms and psychosocial impact. Future studies may benefit from integrating multidimensional disability measures to provide a more comprehensive understanding of MS-related impairment.
In this trial, fatigue did not influence cognitive outcomes, as detailed in our previously published study. 23 Fatigue levels were equivalent between active and sham groups at baseline and study end, with both groups experiencing similar reductions. The lack of correlation between changes in fatigue and cognitive outcomes further supports this conclusion. The nonstandard sham used in this trial, featuring three current ramp-ups/-downs based on earlier designs, aimed to maximize blinding.16,54,55 Future studies should explore whether consistent current delivery is necessary for functional targeting or general symptom relief.
There are limitations to this study. Fatigue was the primary outcome, and participants were not enrolled based on cognitive impairment but were screened to exclude those with severe impairment. This exclusion criterion limits generalizability to individuals with moderate or less cognitive impairment. However, the sample characteristics align with prior BrainHQ trials, 19 where participants exhibited mild slowing on SDMT. 13 The lack of long-term follow-up is a key limitation, preventing assessment of whether cognitive benefits persist beyond the intervention period. Future studies should evaluate the durability of effects over extended timeframes and determine whether tDCS + aCT contributes to long-term cognitive stability or neuroprotection. External factors, including the COVID-19 pandemic, may have influenced results. Heightened distress and social isolation, especially among immunocompromised MS patients, 62 could have affected cognitive functioning. While remote delivery of interventions was a strength, administering cognitive outcomes remotely—though validated—40,41,63 may have affected performance, especially if participants were experiencing heightened distress.
Conclusion
In conclusion, our study demonstrates the efficacy of tDCS paired with aCT (BrainHQ) as an at-home intervention to improve cognitive function in MS patients, particularly those with high neurological disability. Active tDCS significantly outperformed sham in cognitive outcomes, with greater benefits observed in patients with higher baseline neurological disability. The findings suggest cognitive benefits align more with preventing decline than recovery. Future research should investigate optimal intervention duration, frequency, and long-term cognitive effects in this population.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LC and GP received a speaker fee from Soterix Medical Inc. The City University of New York holds patents on brain stimulation with MB as inventor. MB has equity in Soterix Medical Inc.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This trial was sponsored by the National Multiple Sclerosis Society (RG-1803-30492).
Data availability statement
The data supporting the findings of this study are available upon request from the corresponding author.
Appendix
Comparison of baseline characteristics for patients with and without endpoint for the 117 randomized patients. Fisher's exact test was applied to compare categorical variables (sex, race, and ethnicity). Baseline descriptive analyses for the 11 randomized patients without endpoint. EDSS: Extended Disability Status Scale; SDMT: Symbol Digit Modalities Test; BVMT-R: Brief Visuospatial Memory Test-Revised; RAVLT: Rey Auditory Verbal Learning Test; BICAMS: Brief International Cognitive Assessment for Multiple Sclerosis. Linear regression results for change of BICAMS z-scores versus treatment groups, EDSS strata and their interaction. Linear regression results for change of SDMT z-scores versus treatment groups, EDSS strata, and their interaction. Linear regression results for change of RAVLT z-scores versus treatment groups, EDSS strata and their interaction. Linear regression results for change of BVMT z-scores versus treatment groups, EDSS strata and their interaction.
With endpoint
(n = 106)
Without endpoint
(n = 11)
Mean (SD)
Mean (SD)
t-Test
Age
48.69 (12.16)
48.2 (12.64)
.909
BICAMS baseline z-score
−0.45 (1.07)
−0.86 (1.62)
.567
N (%)
N (%)
aFisher exact
test p
Sex
Female
85 (93.41)
6 (6.59)
.213
Male
20 (83.33)
4 (16.67)
Race
White
79 (94.05)
5 (5.95)
.155
Black
21 (84)
4 (16)
Asian
4 (80)
1 (20)
Ethnicity
Hispanic
2 (66.67)
1 (33.33)
.291
Non-Hispanic
97 (91.51)
9 (8.49)
Other
5 (100)
0 (0)

Sham
Active
Variable
N
Values
N
Values
Baseline BICAMS z-score
EDSS = L
2
−1.89, 1.83
1
−2.77
EDSS = H
1
0.11
2
−1.18, −1.28
Baseline SDMT z-score
EDSS = L
1
−1.67
0
NaN
EDSS = H
0
NaN
0
NaN
Baseline RAVALT z-score
EDSS = L
2
−2.15, 1.9
1
−1.99
EDSS = H
1
1.04
2
0.05, −1.35
Baseline BVMT z-score
EDSS = L
2
−1.84, 1.76
1
−3.54
EDSS = H
1
−0.81
2
−2.4, −1.21
Parameter
Estimate
SE
t-Value
Pr > |t|
Intercept
−.0068
0.0969
−0.07
0.9442
Condition active
0.1144
0.1329
0.86
0.3909
Condition Sham
0
.
.
.
EDSS H
−.3480
0.1475
−2.36
0.0203
EDSS L
0
.
.
.
Condition × EDSS Active H
0.2362
0.2059
1.15
0.2540
Condition × EDSS Active L
0
.
.
.
Condition × EDSS Sham H
0
.
.
.
Condition × EDSS Sham L
0
.
.
.

Parameter
Estimate
SE
t-Value
Pr > |t|
Intercept
0.0717
0.1431
0.50
0.6180
Condition active
0.0257
0.1949
0.13
0.8956
Condition Sham
0
.
.
.
EDSS H
−0.5321
0.2162
−2.46
0.0155
EDSS L
0
.
.
.
Condition × EDSS Active H
0.5085
0.3006
1.69
0.0938
Condition × EDSS Active L
0
.
.
.
Condition × EDSS Sham H
0
.
.
.
Condition × EDSS Sham L
0
.
.
.

Parameter
Estimate
Standard
t-Value
Pr > |t|
Intercept
−0.1528
0.1733
−0.88
0.3801
Condition active
−0.0712
0.2374
−0.30
0.7650
Condition Sham
0
.
.
.
EDSS H
−0.6187
0.2673
−2.31
0.0227
EDSS L
0
.
.
.
Condition × EDSS Active H
0.7621
0.3732
2.04
0.0438
Condition × EDSS Active L
0
.
.
.
Condition × EDSS Sham H
0
.
.
.
Condition × EDSS Sham L
0
.
.
.

Parameter
Estimate
Standard
t-Value
Pr > |t|
Intercept
0.1176
0.2084
0.56
0.5741
Condition active
0.3275
0.2844
1.15
0.2526
Condition Sham
0
.
.
.
EDSS H
0.0992
0.3172
0.31
0.7552
EDSS L
0
.
.
.
Condition × EDSS Active H
−0.3554
0.4386
−0.81
0.4200
Condition × EDSS Active L
0
.
.
.
Condition × EDSS Sham H
0.0000000000
.
.
.
Condition × EDSS Sham L
0.0000000000
.
.
.