
Abstract
Sleep disturbance is common in people with multiple sclerosis and may worsen fatigue; however, the assessment of sleep-fatigue relationships varies across studies. To better understand sleep-fatigue relationships in this population, we conducted a systematic review and random effects meta-analyses for the associations between fatigue and 10 sleep variables: Sleep-disordered breathing, daytime sleepiness, sleep quality, insomnia, restless legs, number of awakenings, sleep efficiency, sleep latency, sleep duration, and wake after sleep onset. Of the 1062 studies screened, 46 met inclusion criteria and provided sufficient data for calculating Hedges’ g. Study quality was assessed using the Newcastle-Ottawa Scale. Sample characteristics did not differ between the 10 analyses. Results indicated that sleep quality and insomnia (assessed via self-report or diagnostic criteria) were strongly associated with fatigue (all gs ≥ 0.80 and all ps < .001). In contrast, the number of awakenings and sleep duration (assessed objectively) were not significantly associated with fatigue. Remaining sleep variables yielded moderate, significant effects. Most effects did not vary based on study quality or sample demographics. Results highlight that insomnia and perceptions of poor sleep have a stronger link than objective sleep duration to fatigue in multiple sclerosis and may represent a more effective target for intervention.
Keywords
Introduction
Multiple sclerosis (MS) is a chronic neurodegenerative disease of the central nervous system that causes a wide range of physical, cognitive, emotional, and behavioral health issues. MS affects more than 2.3 million people worldwide and is the most common neurological disease leading to disability in young adults. 1
Fatigue and sleep disturbance are common co-occurring symptoms reported among persons with MS, and both can significantly diminish quality of life.1–4 Notably, fatigue affects up to 90% of persons with MS and is characterized by subjective feelings of unrelenting exhaustion, lassitude, or tiredness. MS fatigue is one of the leading contributors to unemployment, early retirement, and disability in this population.2,5 MS-related fatigue is especially challenging to assess and treat due to its multidimensional presentation (e.g., physiological, cognitive, and behavioral),6,7 its inherently subjective nature, and its overlap with other symptoms and comorbidities, including sleep disturbance. 8 Sleep disturbance—an umbrella term that encompasses a wide range of sleep problems, symptoms, and diagnoses—is also prevalent in persons with MS, with more than 50% of person with MS reporting disruptions in or dissatisfaction with sleep.9,10 Sleep disorders are more prevalent in persons with MS compared to the general population and include insomnia, sleep-disordered breathing, restless leg syndrome, and narcolepsy.11,12
Given the negative impact of fatigue on functioning and quality of life in persons with MS, emerging research has aimed to better understand the role of sleep disturbance as a potential contributor to MS fatigue.6,13 Pathophysiological mechanisms of chronic fatigue in MS (e.g., widespread neuroinflammation and oxidative stress that disrupt metabolic pathways and reduced available energy for essential functions, including homeostatic regulation of sleep and alertness) is a growing area of investigation.7,13 Several observational studies over the past decade have examined associations between sleep disturbance and fatigue in persons with MS; however, these associations vary greatly in significance and magnitude, with some studies reporting little to no relationship, and others reporting strong, significant associations. 6 This observed variability in effects may at least in part be due to the wide range of methodological approaches used to assess or define sleep disturbance. Although some studies have used self-report inventories of insomnia symptoms, sleep quality, or excessive daytime sleepiness to assess symptom severity, others have used objective measures such as actigraphy or polysomnography to quantify common sleep parameters (e.g., apnea-hypopnea index, total sleep time, sleep efficiency). Given that discrepancies between objectively and subjectively assessed sleep are well documented in the literature, 14 it is likely, and to a degree expected, that associations between sleep and fatigue may vary between studies employing different methodological approaches. However, to date, patterns of variability in sleep-fatigue relationships in MS have not yet been systematically and quantitatively characterized or evaluated.
The present systematic review and meta-analysis aimed to comprehensively assess sleep disturbance-fatigue relationships in persons with MS and explore whether specific assessment procedures yield relatively stronger or weaker associations between these variables. Given the self-reported nature of fatigue, we hypothesized that when compared to objective measures, self-report measures of insomnia and global sleep quality would yield relatively stronger associations with fatigue and be at least moderate to large in size (i.e., Hedges’ g ≥ 0.50). Given that many patients with MS report fatigue despite achieving the recommended number of hours of sleep (i.e., total sleep time 6–10 h), we hypothesized that total sleep time would yield relatively weaker effects and be small to moderate in size (i.e., Hedges’ g < .50). Results may have significant implications for MS clinicians and researchers regarding the selection of optimal measurement approaches and intervention targets in the treatment of sleep-disturbance and its relationship with fatigue in individuals with MS.
Methods
Patient/population, exposures, and outcomes framework
The present study, which was conducted according to Meta-analysis of Observational Studies in Epidemiology guidelines, 15 featured a systematic review and meta-analysis of the association between sleep and fatigue among persons with MS. Our research question was formulated using the patient/population, exposures, and outcomes framework for observational designs, 16 with sleep and fatigue conceptualized as the exposure and outcome variables of interest, respectively (see Table 1).
Patient/population, exposure, and outcome (PEO) research framework.

As shown in Table 1, variables of interest for the assessment of sleep disturbance included (a) response on self-report instruments validated for use in MS or other chronic health conditions (e.g., the Pittsburgh sleep quality index 17 ); (b) objective sleep parameters assessed via polysomnography, the multiple sleep latency test, or actigraphy (e.g., wake after sleep onset); or (c) presence of one or more sleep disorders based on established diagnostic criteria (e.g., rest leg syndrome diagnosis per the International Restless Legs Syndrome Study Group). 18
Variables of interest for the assessment of fatigue included responses on validated self-report instruments (e.g., the Fatigue Severity Scale 19 ). A fatigue measure was determined to be valid based on the data reported about the measure in the included studies. If adequate information about the validity of a fatigue scale was not included in a certain article, we conducted a literature search to find the original articles that published and validated the fatigue measures.
Search strategy
Five electronic databases were initially searched in January of 2018: PubMed, Excerpt Medica Database, Cumulative Index to Nursing and Allied Health Literature, Psychological Information Database, and the Cochrane Library, and all study abstracts were examined using Covidence software. However, due to the lag in time between the initial search and the submission of this review, searches were repeated and expanded in December 2019. Searches were conducted by the senior author and validated by the primary author during the same week. All searches were conducted without publication date restrictions and filtered to include articles only written in or translated into English. Although unpublished studies or abstracts were not eligible for inclusion in this review, publication bias was assessed, as described in the data analytic strategy. Two authors independently completed initial study screening and full-text reviews (primary and third authors). Discrepancies were resolved by a third author (senior author). Reference lists from articles that underwent full-text review were reviewed for additional eligible articles. Approximately 60% of the articles included were reviewed by the senior author for agreement. Table 2 presents the search strategy used for each database and the resulting number of articles.
Literature search strategy by database.
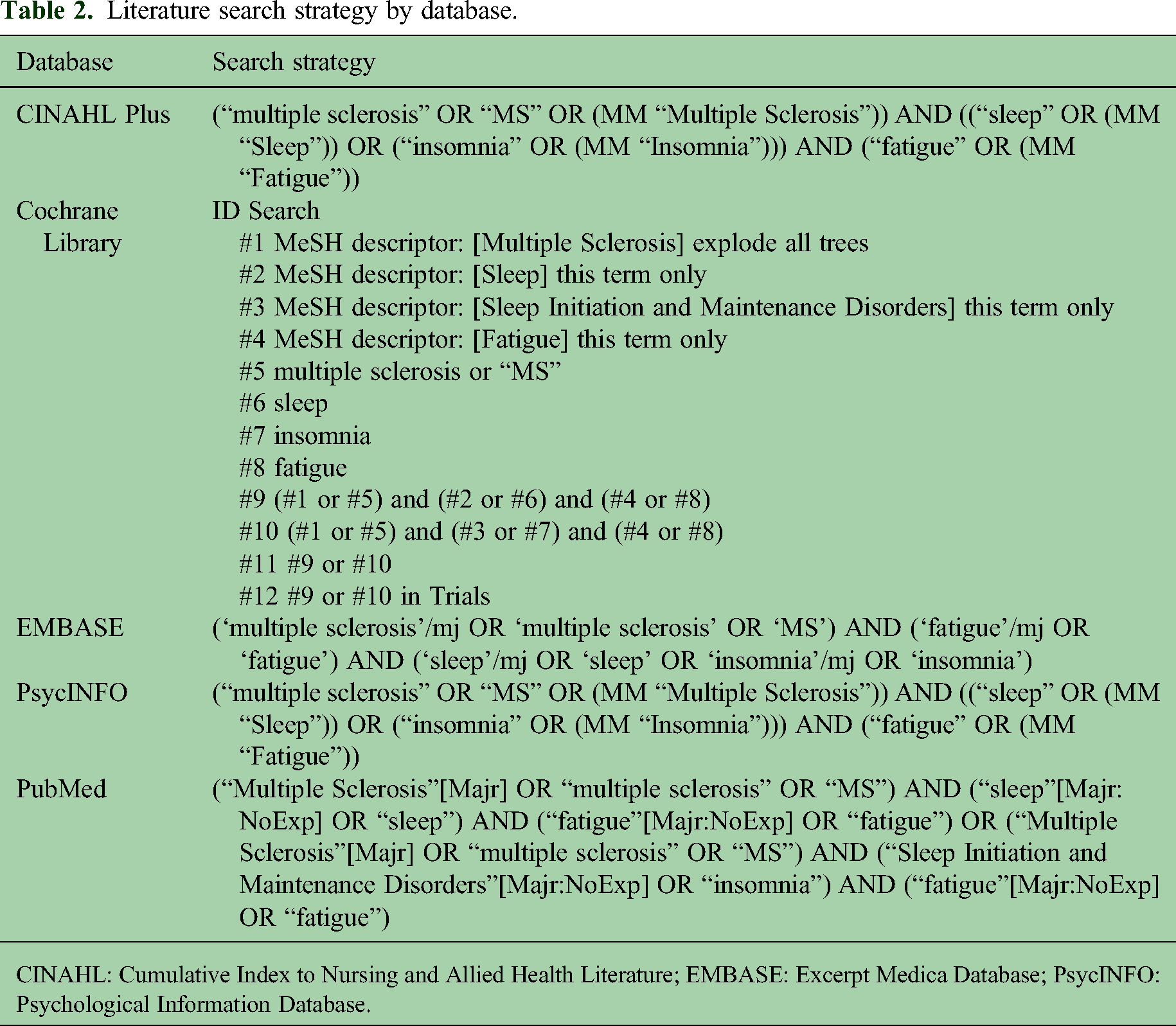
CINAHL: Cumulative Index to Nursing and Allied Health Literature; EMBASE: Excerpt Medica Database; PsycINFO: Psychological Information Database.
Study screening criteria
Study titles and abstracts were screened and included for full-text review if they (a) were published or in press; (b) were written in/translated to English; (c) included a sample of adults (age 18 or older) with a self-reported physician-confirmed MS diagnosis; and (d) featured either an observational (e.g., case-control, cohort, or cross-sectional) design or an experimental design with baseline (pre-randomization) data. Of the 1062 studies, 372 duplicates were removed, and 659 records were screened; this resulted in 100 studies included in the full-text review.
Full-text review criteria
In addition to meeting screening criteria, articles were included in the systematic review if they met the following criteria: (a) included at least one valid measure of fatigue; (b) included at least one valid measure of sleep 20 ; and (c) either reported at least one effect size for the association between sleep and fatigue, or provided sufficient data to calculate the effect size. Potential effect sizes included standardized mean differences (i.e., Cohen's d for the unadjusted mean difference in fatigue between participants with and without sleep disturbance, or for the difference in sleep disturbance between participants with and without fatigue), bivariate correlation coefficients (i.e., zero-order Pearson or Spearman's correlations between sleep and fatigue), or proportional differences (i.e., odds ratios for unadjusted proportions of fatigued and non-fatigued individuals with and without sleep disturbance). If studies reported only adjusted effect sizes and did not provide sufficient data for effect size calculation, authors were contacted to obtain the unadjusted values. Although some authors responded, they indicated data were no longer available.
If two studies used the exact same sample and both reported the information necessary to calculate effect size, the original study was used (e.g., if a randomized controlled trial was published and then later a secondary analysis with the same sampled, used the randomized controlled trial). If the two studies used slightly different samples (e.g., one study used a whole sample, but the other study excluded progressive patients, we used the study with the larger and more complete sample. If one study didn’t report the metrics necessary to calculate the effect size, the study with the adequate data was used. This method was used to avoid data dependency.
Of the 100 studies reviewed, 46 articles were included. A flow diagram depicting the number of articles excluded at each stage, and the reason for exclusion, are provided in Figure 1.

Flow diagram of included studies. CINAHL: Cumulative Index to Nursing and Allied Health Literature; EMBASE: Excerpta Medica Database.
Study quality assessment
The Newcastle-Ottawa Scale was used to determine quality assessment ratings for the 46 included studies. 21 Studies were assessed independently by the primary author and one of the second or fourth co-authors, and any resulting discrepancies were resolved by a different co-author. The Newcastle-Ottawa Scale assesses methodological quality of non-randomized observational (e.g., case-control, cohort, or cross-sectional) studies based on three criteria: Selected population, comparability of groups, and the exposure and outcome of interest (i.e., sleep and fatigue).21,22 Studies were assigned a numerical score ranging from 0 to 9, with scores between 0 and 3 indicating low quality, scores between 4 and 6 indicating fair quality, and scores between 7 and 9 indicating high quality.
Data extraction and synthesis
For each included article, the following variables were extracted and recorded in a secure database: article citation; sleep variable(s) assessed (e.g., insomnia); method or measure(s) used to assess sleep (e.g., insomnia severity index) 23 and fatigue (e.g., fatigue severity scale); sample size; demographic and disease characteristics, specifically age, gender, MS disease duration, disability severity as assessed by the expanded disability status scale (expanded disability status scale 24 ); MS type; Newcastle-Ottawa Scale quality ratings; effect sizes for the association between sleep and fatigue; and, if applicable, data used to calculate effect sizes. For each article, one author extracted, and at least one different author verified the data.
Many studies included in this review reported data for multiple sleep variables (e.g., insomnia and excessive daytime sleepiness), yielding multiple effect sizes per study. To maintain the independence of observations, effect sizes were categorized according to the sleep variable or sleep disorder assessed, with separate meta-analyses performed for each category and a minimum of three studies per category. A total of 10 categories of sleep variables were identified to maintain independence of observations and maximize the inclusion of all eligible effects. A diagram of the 10 categories is presented in Figure 2.

Conceptual framework for categorization of 10 sleep variables predicting MS fatigue. Sleep variables identified based on a systematic search of the literature in PubMed, EMBASE, CINAHL/PsycINFO, and the Cochrane Library, and through data synthesis, with no category having fewer than 3 studies. CINAHL: Cumulative index to Nursing and Allied Health Literature; EMBASE: Excerpta Medica Database; MS: multiple sclerosis; PsycINFO: Psychological Information Database.
Data analysis
To establish a common effect size metric, all ds, rs, and odd-ratios were transformed to a bias-corrected Hedges’ g and weighted by variance. Given significant heterogeneity in effects and study characteristics, a random effects model was used to estimate the mean effect size (g), standard error of the estimate, 95% confidence interval, and statistical significance (p < 0.05) for each of the 10 analyses. We used JASP open-sourced software to construct (a) a single forest plot for the mean effect sizes and confidence intervals for the 10 sleep variable categories 25 ; and (b) ten separate forest plots for the individual studies’ effect sizes and confidence intervals within each of the 10 sleep variable categories.
Additional analyses were performed to assess for potential sources of variability and bias within each sleep category. First, we assessed differences in sample characteristics between studies that were versus were not included in each sleep category analysis (e.g., differences in average sample age between studies that assessed versus did not assess sleep-disordered breathing). Second, sensitivity analyses assessed whether effect sizes differed between high-, fair-, and low-quality studies. Third, publication bias was assessed by computing fail-safe numbers and their significance. Finally, given the significant conceptual overlap of sleepiness with both sleep disturbance and fatigue, a sensitivity analysis was conducted on studies that assessed excessive daytime sleepiness and at least one other sleep variable. The analysis compared sleep-fatigue effect sizes between studies with high (Hedges’ g ≥ .80) versus low-to-moderate (Hedges’ g < .80) concordance between excessive daytime sleepiness and fatigue.
Results
Demographic characteristics and quality ratings
Individual study characteristics (k = 46) are presented in Table 3. Studies were published between 2004 and 2019 and featured a mix of cross-sectional, case control, and longitudinal cohort designs. The 46 studies included a total of 7404 participants (range: 20–2375), a median sample size of 100, and a total mean age of 47.41 (range: 28.25–58.10). Participants across studies were predominately female (71%), with only two studies reporting a sample more than 50% male.8,26 Racial and ethnic backgrounds were largely unreported, or samples were predominately White. Study samples were predominately comprised of participants with relapsing-remitting MS (relapse-remitting MS; M = 71%), and with MS disease durations ranging from 3.00 to 21.10 years (M = 12.65). Scores on the expanded disability status scale ranged from 1.50 to 7.73, with the mean expanded disability status scale (M = 3.29) in the mild to moderate range.
Characteristics of included studies (k = 46).

AHI: apnea-hypopnea index; EDSS: expanded disability severity status; ESS: Epworth sleepiness scale; Insomnia: insomnia diagnosis; ISI: insomnia severity index; MOS-SS: medical outcome survey sleep scale; MS: multiple sclerosis; NoA: number of awakenings; PSQI: Pittsburgh sleep quality index; RLS: restless legs syndrome diagnosis; RRMS: relapsing remitting multiple sclerosis; SE: sleep efficiency; SOL: sleep onset latency; STOP-Bang: snoring, tiredness, observed apneas, blood pressure, body mass index, age, neck circumference, and gender; TST: total sleep time; WASO: wake after sleep onset.
Individual study quality ratings based on the Newcastle-Ottawa Scale are presented in Table 4. Overall study quality ranged from fair to good, with 22 (48%) studies rated in the fair range (Newcastle-Ottawa Scale scores from 4 to 6), and an average rating across studies of 5.84. No studies were rated in the poor range, and there were no consistent patterns of weaknesses across the three quality domains.
Methodologic quality of studies based on the NOS. 21

MS: multiple sclerosis; NOS: Newcastle-Ottawa Scale.
Selection, scored from 0 to 4, is based on the definition and representativeness of the case/cohort, selection and ascertainment of exposed or non-exposed cases.
Comparability, scored from 0 to 2, is based on the comparability of the cases/cohorts based on the design or analysis.
Exposure or outcome, scored from 0 to 3, is based on ascertainment of exposure or assessment of outcome.
NOS total, the sum of the subscores for selection, comparability, and exposure/outcome, ranged from 0 to 9 and classified each study as low quality (total score between 0 and 3), fair quality (between 4 and 6), and high quality (between 7 and 9).
Descriptive statistics for demographic characteristics and study quality ratings within each of the 10 sleep categories are presented in Table 5. The number of studies included in each analysis ranged from 3 (number of awakenings) to 23 (sleep quality).
Sample characteristics, study quality ratings, and publication bias for each sleep variable analysis.

EDS: excessive daytime sleepiness; EDSS: expanded disability severity status; INS: insomnia; NoA: number of awakenings; NOS: Newcastle Ottawa Scale; RLS: restless legs syndrome diagnosis; RRMS: relapsing remitting multiple sclerosis; SDB: sleep-disordered breathing; SE: sleep efficiency; SQ: sleep quality; SOL: sleep onset latency; TST: total sleep time; WASO: wake after sleep onset.
Fail-safe Ns were calculated for all analyses yielding significant effects (i.e., all sleep categories except NoA and TST). ***p < .001.
Primary analysis: Associations between sleep and fatigue
Results of this review's primary analysis—associations between sleep and fatigue within each of the 10 identified sleep categories (i.e., sleep-disordered behaviors, excessive daytime sleepiness, sleep quality, insomnia, number of awakenings, rest leg syndrome, sleep efficacy, sleep latency, total sleep time, and wake after sleep onset)—are presented in a Forest plot in Figure 3. Effect sizes ranged from 0.26 (total sleep time) to 1.02 (insomnia), with statistically significant effects for all but two categories (total sleep time and number of awakenings). The largest effects were observed for insomnia (g = 1.02, p < 0.001) and sleep quality (g = 0.92, p < 0.001), followed by moderate effects for rest leg syndrome (g = 0.76, p < 0.001) and excessive daytime sleepiness (g = 0.70, p < 0.001). Although the number of awakenings exhibited a moderate association with fatigue (g = 0.62), the three studies assessing the number of awakenings yielded highly variable effects, resulting in a non-significant mean effect.

Forest plot of associations between sleep and fatigue across 10 sleep categories. *p < .05; **p < .01; ***p < .001. EDS: excessive daytime sleepiness; INS: insomnia; NoA: number of awakenings; RLS: restless legs syndrome diagnosis; SDB: sleep-disordered breathing; SE: sleep efficiency; SQ: sleep quality; SOL: sleep onset latency; TST: total sleep time; WASO: wake after sleep onset.
Additional Forest plots for each of the 10 analyses are presented in Figures 1 through 3. Across all 10 analyses, every effect size reported showed a positive relationship between sleep disturbance and fatigue; however, the magnitude and variability (i.e., 95% CIs) of these effects varied significantly.
Sources of variability and bias
As described in the data analysis section, sources of variability were explored, including study sample demographic characteristics, quality ratings, publication bias, and sleepiness-fatigue concordance. There were no significant differences between the 10 separate meta-analyses regarding sample age, gender, MS disease duration, expanded disability status scale rating, or MS type (all p values < 0.05). Mean study quality ratings also did not significantly differ between the 10 analytic groups. Within each of the 10 groups, effect sizes did vary as a function of study quality for the three studies that assessed the number of awakenings (z = 2.62, p < .01), and the seven studies that assessed rest leg syndrome (z = 1.99, p < .05), where high-quality studies yielded significantly stronger sleep-fatigue associations than fair-quality studies. No other sleep domains exhibited significant differences in effects between high- versus fair-quality studies.
Regarding potential publication bias, Rosenthal's fail-safe Ns (i.e., the estimated number of non-significant effects that would need to make the overall effect non-significant) are reported in Table 5 for each sleep variable category that yielded a significant mean effect (i.e., all categories except total sleep time and number of awakenings). Fail-safe Ns ranged from 18 (wake after sleep onset) to 3619 (sleep quality), suggesting a large number of studies with non-significant effects would be needed to change the overall results of this study. Of the 10 categories assessed, nine (all except insomnia) included studies that assessed excessive daytime sleepiness and at least one other sleep variable. For those categories, sleep-fatigue relationships were able to be assessed for differences in excessive daytime sleepiness-fatigue concordance. Significant differences were noted for the number of awakenings, where one study with high sleepiness fatigue concordance (Hedges’ g ≥ 0.80) exhibited significantly stronger effect sizes than the remaining studies with low-to-moderate concordance (z = 2.62, p < 0.01).
Discussion
The present review was the first to comprehensively assess sleep disturbance-fatigue associations in persons with MS and explore the degree to which methodological variations in sleep assessment contribute to variability in sleep-fatigue relationships. Consistent with our hypotheses, self-report measures of insomnia and global sleep quality yielded strong associations with fatigue that were larger relative to associations resulting from other measurement approaches, especially the use of objective sleep parameters. This finding is consistent with extant literature showing stronger effects for subjectively assessed sleep. Also, consistent with our hypotheses, total sleep time yielded the weakest and non-significant association with fatigue. The primary clinical and research implications for these findings are that while some objective sleep assessments (e.g., total sleep time) may yield results in the normal range, patients can continue to experience severe fatigue as a function of poor sleep. Specifically, meeting diagnostic criteria for insomnia or rest leg syndrome and reporting poor sleep quality and severe sleepiness are significant risk factors for, and are likely to cause, or exacerbate, MS fatigue.
Results also demonstrated a strong overlap between sleep disturbance, sleepiness, and fatigue. In the presence of both high fatigue and sleepiness as measured by subjective assessments, nocturnal awakenings exhibited a stronger relationship to fatigue. However, sleep efficiency and delayed sleep onset were not found to have a strong relationship to fatigue. This may suggest that the sleepiness-fatigue relationship may be low in the variance of the sleep-disturbance and fatigue relationship. With this finding, measures of sleep disturbance are distinct from measures of excessive daytime sleepiness.
Another important finding from this review was that demographic characteristics and MS-related disease characteristics did not significantly impact the strength of sleep-fatigue relationships. In contrast, the extant literature shows potential differences in the sleep-fatigue relationship among certain demographic groups. For example, older adults with MS and individuals with progressive MS generally exhibit a greater risk for sleep disturbance. 30 This group of participants in our study sample, however, was not experiencing disproportionally significant fatigue.
An important limitation of this review was the low number of studies that assessed objective sleep disturbance, especially relative to the high number of studies that assessed subjective sleep. This observation is not limited to this review but is generally reflective of the broader literature, where objective sleep assessment in MS confers numerous logistical and financial challenges. Although fail-safe Ns were in the acceptable range for this review, more studies are needed that include polysomnography, multiple sleep latency test, actigraphy, and other objective measurement approaches. Of note, it remains unknown if objective measures of sleep disturbance differ significantly in relation to MS-related fatigue.
One of our aims with this research was to summarize the varying number of sleep disturbance measures published in the literature and how, if at all, their relationship with fatigue differs. This paper focuses on the synthesis of data based on the different sleep disturbance measures and consequently, does not include the wide array of fatigue measures that exist. Fatigue measures that were subjective (i.e., self-report) and had previously been validated in the MS or a related patient population were included in this study. Assessment of general self-report fatigue symptoms has commonly been linked with sleep disturbance or sleepiness (as a result of the disturbance) in MS. However, this does not capture the nuances among different types of fatigue, including state vs. trait fatigue, central vs. peripheral fatigue, and cognitive vs. psychosocial vs. physical fatigue. The different types of fatigue and how they are evaluated, especially in the context of the sleep-fatigue relationship in individuals with MS is an important area for future research. The examination of the use of both objective and subjective fatigue measures and their relationship to MS-related sleep disturbance would provide a more comprehensive picture of the sleep-fatigue relationship and likely also elucidate additional, novel areas to target for clinical intervention.
Another limitation of this review was the relatively homogenous study sample demographics and MS-related characteristics (e.g., mostly female, White, with relapse-remitting MS and low-to-moderate disability). Although these demographic distributions are consistent with the general MS literature, underrepresentation of men and people with progressive MS preclude any general conclusions regarding these subgroups, who also experience severe fatigue and may exhibit a different pattern of the sleep-fatigue relationship. Finally, given that all of the studies included in this review were observational in design, conclusions regarding causal relationships between sleep disturbance and fatigue remain speculative.
Conclusions
The present review was the first to quantify associations between MS-related sleep disturbance and fatigue. Results demonstrate that these relationships vary substantially as a function of the type of sleep variable assessed. Insomnia, poor sleep quality, restless legs syndrome, and excessive daytime sleepiness were the strongest predictors of fatigue in MS. In the clinical context, our findings support regular assessment of insomnia symptoms, sleep quality, and excessive daytime sleepiness when assessing and treating MS-related fatigue. A combination of subjective and objective measurement is ideal, though one can expect subjective symptoms to correlate more reliably with fatigue. A primary focus on increasing sleep duration is not recommended, given the lack of support for sleep duration as a modifiable target to improve fatigue.
Continued work is needed to characterize the mechanisms underlying sleep-fatigue relationships. Future research efforts should emphasize the inclusion of objective assessment methods to provide more nuanced characterizations of sleep profiles and their relationship to fatigue in MS. Additional research on cognitive behavioral therapy for insomnia in MS, and other evidence-based behavioral approaches to treating sleep disturbance in MS, is needed to determine if improvements in sleep confer improvements in fatigue.
Footnotes
Glossary of terms
Authors’ contributions
All authors contributed to the manuscript in a significant way as follows: (a) JB designed the study, developed technical materials, acquired data, interpreted the data, and drafted the manuscript; (b) KP acquired, validated, and interpreted the data; developed technical materials, and drafted the manuscript; (c) KD designed the study, developed technical materials, acquired data, and interpreted the data; (d) AB acquired, validated, and interpreted the data; (e) BO drafted and reviewed the manuscript, and (f) AH developed technical materials, acquired data, interpreted all of the data, and reviewed the manuscript. All authors have evaluated the intellectual content critically, have read and approved the final manuscript, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the article are appropriately investigated and resolved.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JB was funded by the National Multiple Sclerosis Society Mentor-Based Fellowship (Grant MB0032; Principal investigator: Beier), the National Institute of Health (Grant 1K23MD014176; PI: Bhattarai). BO was supported (in part) by a National Multiple Sclerosis Society Mentor-Based Postdoctoral Fellowship (Grant #MB-1907-34637; PI: Hughes). AJH is funded by the National Instituets of Health (Grant K23HD086154, PI: Hughes).
The funding agencies had no role in the following: (a) design and conduct of the study; (b) collection, management, analysis, and interpretation of the data; and (c) preparation, review, or approval of the manuscript.