
Abstract
Background
Comorbidity is a current area of interest in multiple sclerosis (MS) and is essential for multidisciplinary management. Although recent studies suggest that patients with MS have an elevated risk of developing inflammatory bowel diseases (IBD), this systematic review and meta-analysis aimed to estimate the overall risk of developing ulcerative colitis (UC), specifically in patients with MS.
Methods
In 2021, a comprehensive literature search was performed on PubMed, Scopus, Embase, and Web of Science to identify studies investigating the association between UC and MS. The selected papers were utilized to estimate the associations, risk ratios (RRs), and a 95% confidence interval (CI).
Results
The analysis revealed a slightly elevated risk of UC incidence in patients with MS compared to controls, but this finding was not statistically significant (RR: 1.27 [95% CI: 0.96–1.67]). In contrast, the study found that patients with UC have a significantly higher risk of developing MS than controls (RR: 1.66 [95% CI: 1.15–2.40]).
Conclusion
Our findings highlight that the presence of UC increases the risk of developing MS by more than 50%, whereas the presence of MS does not increase the risk of UC occurrence. These results underscore the importance of considering the potential development of UC in the clinical management and early diagnosis of patients with MS, as it may contribute to better therapeutic outcomes.
Highlights
Ulcerative colitis (UC) can increase the risk of multiple sclerosis (MS) by more than 50%.
MS does not increase the risk of UC occurrence.
Clinical management and early diagnosis of UC in MS are vital for achieving better therapeutic results.
Introduction
Multiple sclerosis (MS) is an immune-mediated disease (IMD) of the central nervous system that affects individuals in their early and middle-aged years. However, women are affected more than men. 1 The exact underlying mechanisms leading to the development of MS are unclear yet. Both genetic predisposition and environmental factors are thought to have a role. Incidence rates vary according to ethnicity; for example, the Nordic nations are known as high-risk zones. 1 Inflammatory bowel diseases (IBDs), including Crohn's disease and ulcerative colitis (UC), are associated with altered immune system function. Persons with certain IMD or a family history of IMD appear to have a higher risk for other IMDs.2–4 Although the etiology and pathogenesis of IBD and UC are not precisely known, certain environmental and genetic factors in a susceptible host are suggested to affect commensal microbiota, intestinal epithelial cells, and immune cells within tissues, causing the disruption of homeostasis and leading to a chronic state of dysregulated inflammation. 5
Many clinical and pathological characteristics of MS, including autoantibodies and perivascular aggregation of autoreactive T cells, are the same as other dysimmune diseases.6–9 For decades, speculation has existed about a possible link between MS and IBD.4,10 Recent research findings indicate an increased risk of IBD among patients with MS compared to the general population.2,11 The correlation between MS and IBD has been shown not only by their common epidemiological and immunological patterns but also by reports of the rising prevalence of IBD and MS among the general population.12–14 The effect of comorbidities in patients with MS is vital. It can cause misdiagnosis following disability progression and alter these patients’ quality of life and clinical care.15–18 This systematic review and meta-analysis aimed to estimate the cumulative risk of MS and UC as comorbidity.
Methods
This systematic review and meta-analysis were performed under the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement guidelines.
Search strategy
A comprehensive literature search was conducted on PubMed, Scopus, Embase, and Web of Science in June 2021. The following search strategy was used: (comorbid OR Comorbidity OR Comorbidities OR Colitis, Ulcerative OR Idiopathic Proctocolitis OR Ulcerative Colitis OR Colitis Gravis OR UC OR colitis ulcerative OR colitis ulcerosa OR mucosal colitis OR ulcerative colorectitis OR ulcerative proctocolitis OR ulcerative proctocolitis OR ulcerous colitis) AND (Multiple Sclerosis OR chariot disease OR disseminated sclerosis OR insular sclerosis OR multiple sclerosis OR sclerosis multiplex). Moreover, we manually searched references to expand the yield of further relative studies.
Eligibility criteria
All types of comparative studies (randomized controlled trials, case-control, cross-sectional, and cohorts) without language limitations were included. We looked for citations for UC among patients with MS and those looking for MS among the UC population. Case reports, case series, editorials, commentaries, literature reviews, and qualitative studies were excluded.
Study selection
First, titles and abstracts were evaluated for their relevance by two researchers (AM and AA). In the next step, the remained studies were reviewed via their full text for final selection. Any disagreements were resolved by discussion among investigators.
Data extraction
The same reviewers (AM and AA) extracted the data from selected studies using a predesigned form. The following information was removed: study characteristics (author, year of publication, country, and study design), number of controls, patients with MS and UC, mean age, control setting, and number of females.
Quality assessments
We used the Joanna Briggs Institute (JBI) checklist to assess the quality of included studies. 19 The JBI checklist is mainly used to evaluate the quality of studies on the prevalence of conditions.
Data synthesis and analyses
The difference between odds ratio, hazard ratio, and relative risk (RR) is ignored. 20 Risk ratio and 95% confidence interval (CI) were performed to measure the associations. Also, we used a random-effect model in all statistical analyses. The heterogeneity was evaluated using I-squared (I2) statistics among included studies. The heterogeneity is considered high if the I2 value is > 50%. Egger's regression test and funnel plot were used to assess publication bias. This review performed all analyses using the Stata 11.0 (College Station, TX).
Results
Study selection
A total of 3828 articles were identified through the initial search. After removing duplicates, 2532 studies were entered into our screening process. After the title and abstract review, 2390 papers were excluded according to our eligibility criteria. Finally, the remained studies went under full-text review, and 17 were included for qualitative and quantitative synthesis (Figure 1). Finally, 11 studies reported the incidence of UC in patients with MS, while 6 others investigated the risk of MS in patients with UC.

PRISMA flowchart of studies included in this systematic review and meta-analysis.
Characteristics of included studies and a qualitative summary
The complete characteristics of the included studies are detailed in Tables 1 and 2. Among included studies, 11 were cohorts, 4 were case controls, and the other 2 were cross-sectional. Most of the studies were conducted in North America and Europe. Studies reporting the occurrence of UC among patients with MS included 62,330 patients with MS, and those writing the event of MS among patients with UC had a total of 112,303 patients with UC. Based on quality assessments, none of the studies earned less than 5 “YES” responses in the JBI checklist, considered an acceptable range for included studies (Table 3).
Characteristics of included studies reported UC in MS population.

MS: multiple sclerosis; NR: not reported; UC: ulcerative colitis.
Characteristics of included studies reported MS in the UC population.

IBD: inflammatory bowel disease; MS: multiple sclerosis; NR: not reported; UC: ulcerative colitis.
Results of quality assessments.

Meta-analysis
To assess the risk ratio of UC in MS, we included 11 studies in our random-effect model. The results indicated that there is no statistically significant risk of UC incidence among patients with MS compared to the controls (RR: 1.27 [95% CI: 0.96–1.67]) (Figure 2). Also, we found a high level of heterogeneity among studies in the model (Q statistics = 80.44, p < 0.001, I2 = 87.6%). On the other hand, we calculated the risk of MS incidence among patients with UC and controls using the same model. We found that patients with UC have a higher risk of developing MS compared to controls (RR: 1.66 [95% CI: 1.15–2.40]) (Figure 3). The included studies in this model had a high level of heterogeneity (Q statistics = 21.70, p = 0.001, I2 = 77.0%).

Forest plot of the risk of UC incidence among patients with MS compared to the controls. MS: multiple sclerosis; UC: ulcerative colitis.
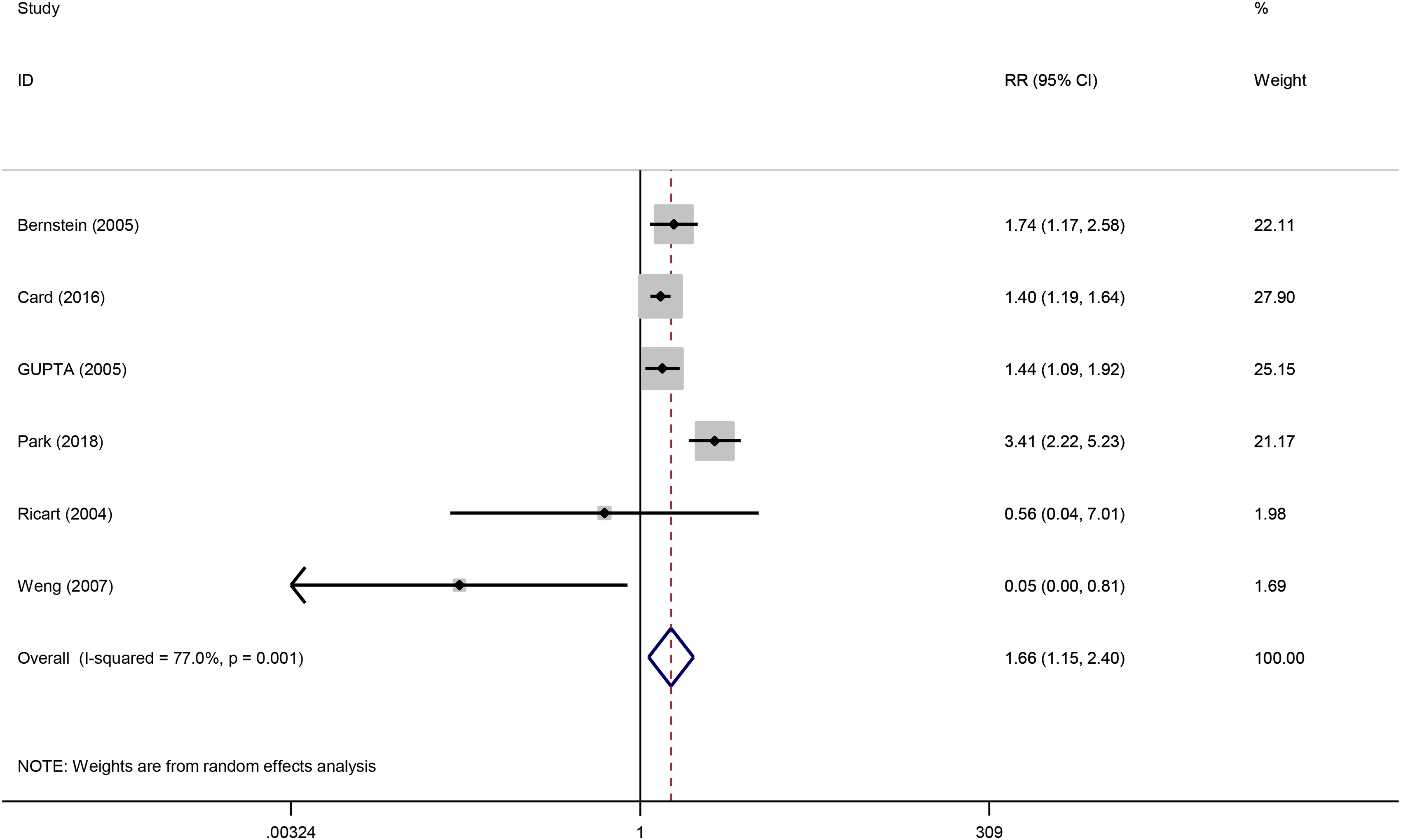
Forest plot of the risk of MS incidence among patients with UC compared to the control group. MS: multiple sclerosis; UC: ulcerative colitis.
The pooled prevalence of UC among patients with MS was 0.8% (95% CI: 0.5–1.1%, I2: 93.7%, p < 0.0001) compared to 0.4% among the controls (95% CI: 0.3–0.6%, I2: 99.3%, p < 0.0001).
The mean point prevalence of MS was 0.31% (95% CI: 0.17–0.61%, I2: 98.5%, p < 0.0001) among patients with UC, while it was 0.21% among controls (95% CI: 0.14–0.28%, I2: 99.1%, p < 0.0001). As shown, the level of heterogeneity was considered high in these studies.
Publication bias
The funnel plots and Egger’s test reveal no evidence of publication bias in the studies reporting the risk ratio of UC in MS (bias = −1.8385, 95% CI: −5.2591–1.5825, p = 0.237) (Figure 4). Similarly, for studies reporting MS incidence in patients with UC compared to control groups, the funnel plots and Egger’s test suggest no publication bias (bias = 1.6660, 95% CI: −6.4054–9.7375, p = 0.468) (Figure 5).

Funnel plot with pseudo 95% confidence limits for detection of publication bias of risk of UC incidence among patients with MS compared to the control group. MS: multiple sclerosis; UC: ulcerative colitis.

Funnel plot with pseudo 95% confidence limits for detection of publication bias of risk of MS incidence among patients with UC compared to the control group. MS: multiple sclerosis; UC: ulcerative colitis.
Discussion
We found that the presence of UC can increase the risk of MS by more than 50%. However, MS does not increase the risk of UC occurrence. Our findings do not confirm the results of previous systematic analysis12,16 on UC comorbidity among patients with MS, which found that MS increases the risk of UC occurrence (risk ratio 1.21–3.13) compared to the general population.
To answer why MS and UC might be associated, we should look into the recent studies on the molecular immunology of MS and UC. These studies have shown the role of the T helper (Th) 17 cell domain in both MS and IBD.13,21 The local immune response in UC is less polarized, although it may produce more interleukin (IL) 5, IL-13, and Th17 cytokines. 22 In MS, however, stress-induced Th17 cell activation was thought to promote central nerve degeneration and inflammation. 23 Increased IL-17 production in patients with MS and UC suggests that the Th17 cell is involved in the disease etiology.
There are several possible explanations for why the association between UC and MS may only go one way, with UC increasing the risk of MS but not the other way around. One possible explanation is that the immune mechanisms involved in UC may be more directly linked to the development of MS than the immune mechanisms involved in MS are to the development of UC. For example, UC is a chronic inflammatory condition primarily affecting the gastrointestinal tract. The inflammation associated with UC may trigger or exacerbate the immune response involved in the development of MS. Another possible explanation is that the genetic or environmental factors that contribute to the development of UC may also increase the risk of developing MS. Still, the genetic or environmental factors that contribute to the development of MS may not increase the risk of developing UC. For example, specific genetic or environmental factors may increase the risk of both UC and MS, but these factors may be more strongly associated with UC than with MS.15,24
The current study has the following strengths over the previous systematic reviews on this topic: first, we narrowed down the issue and focused on patients with UC rather than all patients with IBD. Second, we analyzed the two patient populations: UC and MS. Also, we included the data in control groups in our analysis to improve the reliability of the results and conclusions. Third, we did not apply any language restrictions and had one paper written in Persian. 25
A few limitations should be considered: First and most critically, treatment status is not fully disclosed in the included publications, particularly the percentage of patients with IBD treated with anti-tumor necrosis factor alpha (TNFα) drugs. Anti-TNFα drugs should be regarded as a possible confounder in the MS–IBD connection since they have been related to drug-induced demyelination. 26 UC and MS are both chronic inflammatory illnesses with remissions and exacerbations; there is also the issue of determining which started first and selecting the predominance of one disease throughout the other. 12 Because of methodological variations between studies, the findings are heterogeneous and frequently difficult to compare: different measures, such as absolute prevalence or incidence rates versus risk ratios determined using statistical inferences (p values and CIs), study group sizes, time scales (e.g. using defined time points or different follow-up periods), and the lack of age-specific, sex-specific, and ethnicity-specific risk estimates or controls for certain risk factors were also variables. The survey techniques and diagnostic criteria employed to measure conditions were similarly diverse, as were the classifications and definitions of symptoms and comorbidities. Study quality was inconsistent, and various study designs made cross-study comparisons challenging. Due to modifications to McDonald's diagnostic criteria in 2005 27 and 2010, 28 the variety of techniques of ascertainment for cases and controls within individual research and between included studies may constitute another substantial source of bias, particularly in diagnosing MS.
Moreover, UC and MS are chronic inflammatory diseases with different types and phases. However, not enough data was reported in the included studies of these diseases. For example, Gavlas 29 only provided data on patients with relapsing–remitting MS which might be the reason for the overestimated prevalence of UC in patients with MS in this study. Finally, the quality of the data sources used in some studies was not sufficiently verified.
We chose to include all publications reporting comorbidity in MS, regardless of whether the declared goal was to assess comorbidity's incidence or prevalence, to enhance our search's sensitivity. This undoubtedly exacerbated the heterogeneity problem and resulted in the identification of lower-quality studies.
While numerous studies were conducted in Europe and North America, including many high-powered epidemiological studies from Canada, Italy, the United States, Sweden, and the United Kingdom, establishing region-specific comorbidity trends in patients with MS remains challenging since most world regions have been understudied. There were no research from Africa and only a handful from Asia. At the same time, data from European and North American studies mainly came from several locations within those continents. Estimates based on ethnicity were considerably less commonly supplied. Furthermore, statistics were seldom adjusted to a common population, such as the worldwide population, making it impossible to determine whether comorbidity prevalence varies considerably between geographic areas.
In essence, frequent neurological examinations of patients with UC and routine gastroenterological monitoring of patients with MS may be needed due to the higher risk of MS and UC comorbidity emphasized in the current meta-analysis.
Conclusion
In summary, this systematic review and meta-analysis show that UC's presence probably increases the risk of MS by more than 50%. However, MS may not increase the risk of UC occurrence. This highlights the importance of considering the development of UC in clinical management and early diagnosis for achieving better therapeutic results. Our study should encourage further research to estimate the correlation between UC and MS.
Footnotes
Acknowledgements
The authors thank Dr Mahmoud Yousefifard (Physiology Research Center, Iran University of Medical Sciences) for writing aid and Dr Omid Mirmosayyeb (Isfahan Neurosciences Research Center) and Dr Alireza Afshari-Safavi (Department of Biostatistics and Epidemiology, Faculty of Health, North Khorasan University of Medical Sciences) for data extraction support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Since the data in this article were obtained from the ADNI database (adni.loni.usc.edu), it does not include any research involving human or animal subjects.
Availability of data and material
The datasets analyzed during the current study are available upon request with no restriction.
Consent for publication
This manuscript has been approved for publication by all authors.