
Abstract
Background and Purpose
Multiple sclerosis (MS) has a high incidence of debilitating spasticity. Central Nervous System (CNS) intrafusal settings have an impact on spasticity level. Mechanoreceptors of the Peripheral Nervous System (PNS) communicate monosynaptically with the central nervous system (CNS). This case series assesses feasibility of multimodal treatment of individuals with MS using a direct current electrical stimulation (DC) to influence mechanoreceptors.
Case Description and Intervention
Seven MS diagnosed participants with Expanded Disability Status Scale (EDSS) = 6.0–8.0 completed 18 visits over 6 weeks of using DC combined with neuromuscular reeducation. Design included pre-, post- outcome measures of EDSS, 12-item MS Walking Scale (MSWS-12), Range of Motion (ROM), Manual Muscle Testing (MMT), Modified Ashworth Test (MAT), Timed 25-Foot walk (T25WT), Timed Up and Go (TUG) and the Multiple Sclerosis Impact Scale-29 (MSIS-29).
Outcome
125 out of a possible 126 visits were completed, demonstrating a high level of tolerance. Individual results included trends towards improvement in spasticity and agonists.
Discussion
This case series design of seven heterogenous subjects with MS is a low sample size for statistical analysis and should be considered a pilot. The study demonstrates a high level of feasibility and possible correlations to consider. Further research is warranted.
Keywords
Introduction
Approximately 66% 1 –84%2,3 of individuals with multiple sclerosis (MS) experience spasticity. 1 The pathophysiology of spasticity best understood, demonstrates an imbalance between inhibitory dorsal reticulospinal tract (RST) fibers and excitatory bulbopontine tegmentum. RST neurons receive direct somatic, vestibular, tectal, cerebellar and motor excitatory input and are scattered in the ventral and lateral spinal cord columns intermingled with propriospinal fibers. 2 The peripheral Golgi tendon organ of muscle tendon and muscle spindle intrafusal fibers ubiquitous throughout the musculoskeletal system have monosynaptic connection to this central nervous system (CNS) propriospinal fibers and influence the degree of spasticity and overactive stretch reflexes.2,4
When mechanoreceptors function normally within a fully intact neurological system, they are protective against stretch in muscle, tendon and/or bone injury causing reflexive counterforce such as dropping a weight that is too heavy. 2 In an individual with MS the CNS causes the threshold for stretch reflex and muscle tightness to be set lower than normal. 2 This inhibits normal movement and causes abnormalities in ambulation, posture, stiffness and at times joint contractures.
If direct current electrical stimulation (DC) is able to alter the proprioception of the peripheral nervous system (PNS) with input to mechanoreceptors, it may be possible to find measurable change in CNS driven spasticity during treatment and after treatment. 5 If individuals with MS can experience a normalized stretch response, it may be possible to create CNS level changes within the bulbopontine tegmentum. This pilot study case series is designed with measures of spasticity, range of motion, muscle strength, gait speed and balance to assess feasibility. The purpose of this Pilot case series is to assess if treatment of individuals with progressive MS at the PNS level through targeting mechanoreceptors using the NeuBie (Neurological Fitness Equipment and Education LLC, Austin TX manufactured by Johari Electro Tech Company in Jodhpur India), a DC electrical stimulation device, has feasibility to inhibit spasticity and improve functional mobility in clinically significant measures. 6
Patient information
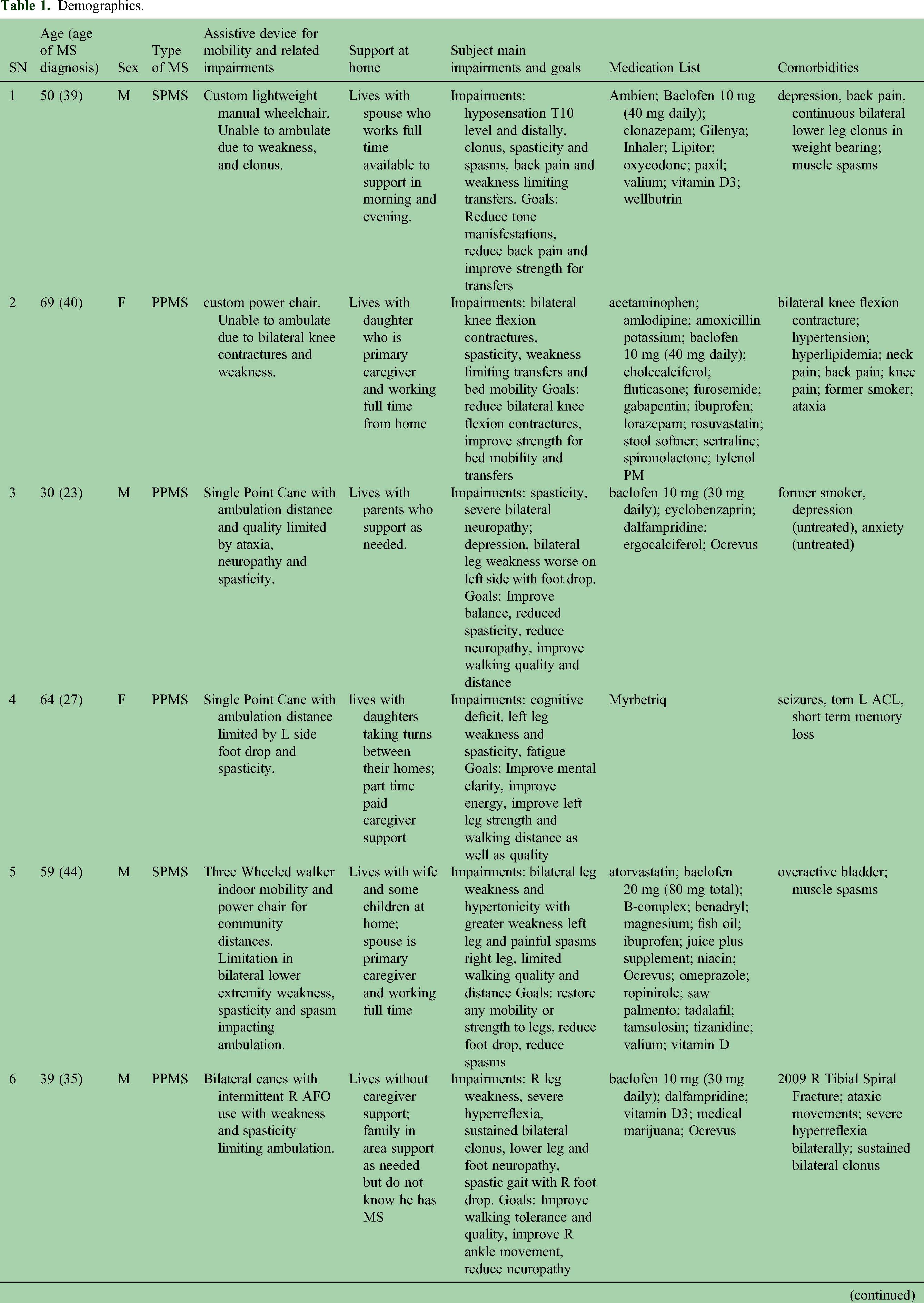
Courtney Ellerbusch, PT, DPT designed and implemented a repeatable study design of home health visits for progressive MS in partnership with Dr Julie Seibert, MD. Dr Ellerbusch completed all assessments and interventions. A case series of 7 participants with progressive MS with mobility impairment (Expanded Disability Status Scale = 6.0–8.0) completed 18 visits over 6 weeks of home health-delivered physical therapy from July 22, 2021 through June 3, 2022. The design utilized DC combined with neuromuscular reeducation in manual activations, 7 flexibility training, neuromuscular reeducation and functional training. Dr Seibert completed each subject's office visit prior to participation, consents and EDSS; then repeated EDSS upon intervention timeline completion. (See Table 1 for demographics).
Demographics.
Assessment and intervention timeline
The study assessment and intervention timeline (Table 2) details the assessments and intervention parameters provided for all seven subjects over a period of 6 weeks of home health physical therapy. The only exception is subject 7 who developed urinary tract infection (UTI) symptoms on the 18th visit and was not able to tolerate final ambulatory assessments.
Study assessment and intervention timeline.
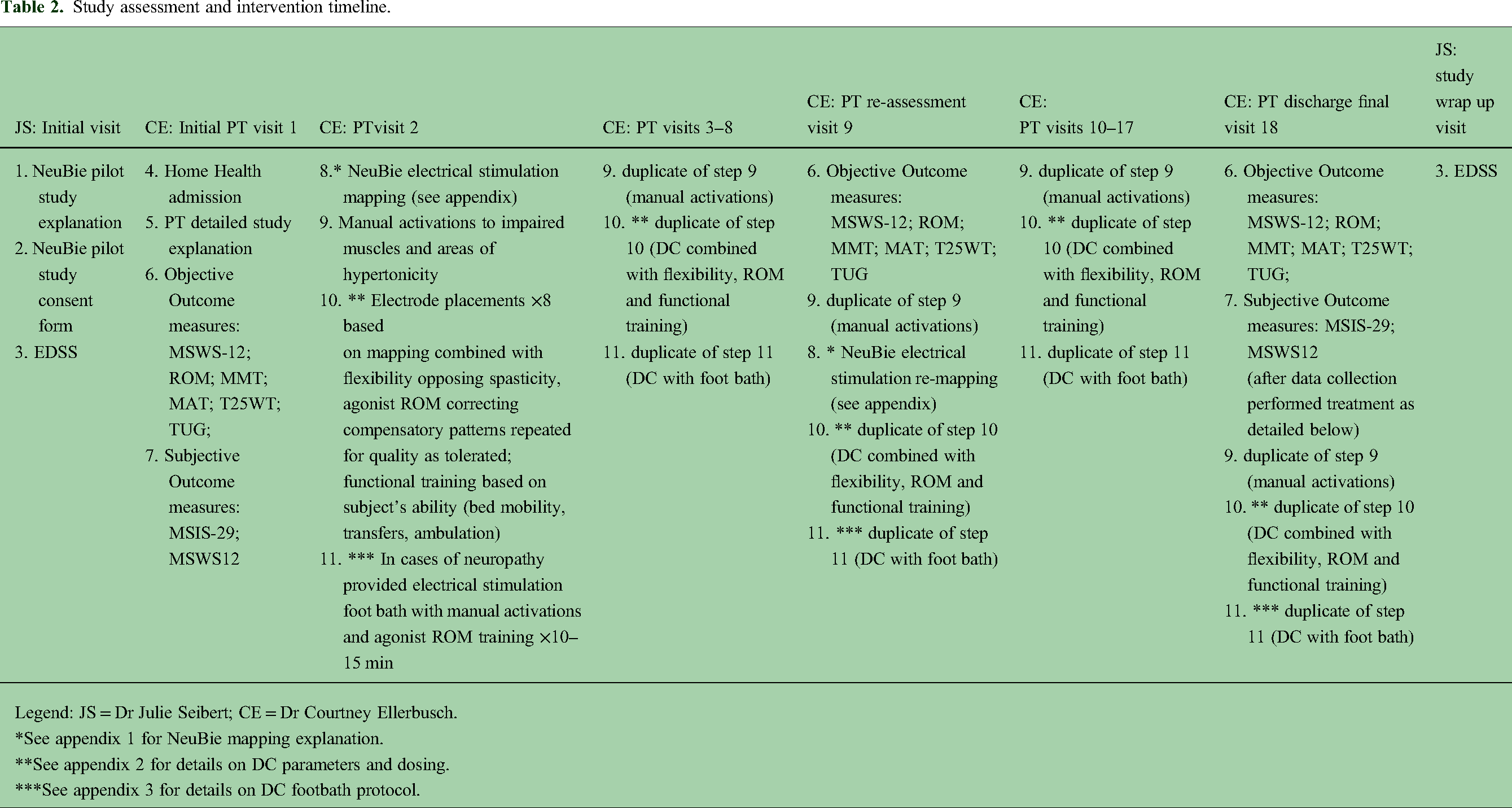
Legend: JS = Dr Julie Seibert; CE = Dr Courtney Ellerbusch.
*See appendix 1 for NeuBie mapping explanation.
**See appendix 2 for details on DC parameters and dosing.
***See appendix 3 for details on DC footbath protocol.
Initial PT visit included medical history, goals, assessment of functional impairments and outcome measures. Subjects 1–7 were a heterogenous group of non-ambulatory and ambulatory. A four-part intervention was used with each subject. Part 1*** targeted neuropathy with a DC footbath protocol, when neuropathy was reported. Part 2** targeted areas of measured spasticity through flexibility combined with DC to a range that elicited a stretch without creating a spasm or spasticity response. Part 3** combined DC with agonist strengthening through tolerated ranges without identified compensatory movements. Subjects were given work to rest ratio of 1:2 up to 1:4 depending on fatigue response within visit or reported at the next appointment. Part 4 applied DC while training subjects to the highest degree of functional training safely tolerated while reducing or eliminating compensatory patterns.
Group clinical findings
A PhD level statistician provided quantitative analysis MAT and MMT (see Table 3). Individual cases showed a variety of quantitative changes, with trends towards improvement in plantar flexor (PF) spasticity per MAT (71.4% of subjects improved in PF MAT). Subjects trended toward improvement in MMT of bilateral psoas, bilateral quadratus lumborum, bilateral vastus lateralis and medialis, bilateral gluteus medius, bilateral hip adductor group, bilateral tibialis anterior (TA) and bilateral biceps femoris. There are no trends across subjects demonstrating worsening measurements in spasticity, MMT or ROM. The re are no clear trends identified from subjective measures MSIS-29 or MSWS-12 across subjects. Out of a possible 126 total visits for seven subjects a total of 125 visits were completed, demonstrating a high level of tolerance. One missed visit occurred due to pre-existing comorbidities in subject 7 with UTI symptoms. All subjects were educated to the potential for neurological fatigue with careful assessment of response. 8 Subjects 1 and 5 required intervention modification in dosing and intensity due to fatigue response, but able to tolerate modified intensity. Subject 7 had hypertension at times and UTI symptoms requiring modifications. No other subjects required intervention modification in dosing or exercise intensity. There were no known adverse responses to the interventions provided.
Quantitative changes in MAT and MMT.

Legend: MAT = Modified Ashworth Test; MMT = Manual Muscle Test.
Individual clinical findings
Subject 1 (non-ambulatory power chair dependent) demonstrated improvements in right side hip flexor length improving from initial assessment (IA) of four fingers in prone from ASIS to mat surface and 0 degrees hip internal rotation associated with right 0/5 psoas MMT to a final assessment (FA) of three fingers in prone from ASIS to mat surface, 5 degrees hip internal rotation and 1+/5 right psoas MMT. Subject 1 also demonstrated improvement from 3/4 hip extension MAT at initial assessment to final assessment of 0/4 hip extension MAT with ability to contract psoas muscles for the first time since initial assessment at 1+/5 MMT. These improvements combined with ability to place electrical stimulation on bilateral PF to prevent clonus in weight bearing allowed this subject to stand without clonus, requiring maximum assistance from the investigator, while holding the sink. Prior to study participation, subject 1 was unable to stand due to weakness, clonus and spasticity. Subject 1 reports disappointment in his results, expressing hope to have improved his standing and control of spasms more substantially.
Subject 2 (non-ambulatory power chair dependent with bilateral knee flexion contractures) demonstrated reduction in bilateral PF spasticity from 3/4 MAT bilaterally at IA reduced to 1+/4 at FA and able to tolerate rolling from supine to prone. Prone positioning was not tolerated prior to study participation due to weakness and bilateral knee flexion contractures putting hip flexors into a shortened position. Subject 2 improved knee flexion contractures from bilateral IA 0-70-130 improved to FA 0-20-130 passive range of motion. Due to improved knee range of motion and elimination of clonus in weight-bearing during application of electrical stimulation to bilateral gastrocnemius and soleus region, Subject 2 was able to initiate standing training for the first time in 10 years (per self-report of the subject) at sink with bilateral upper extremity support and maximum assistance from primary investigator. Subject 2 reports feeling looser in her legs and stronger for transfers.
Subject 3 (bilateral spastic gait pattern with unilateral cane) demonstrated mixed results in spasticity, strength, ambulation tests and subjective reporting on MSWS-12 and MSIS-29 with a diagnosis of untreated depression. This subject demonstrated ninth visit reassessment (RA) of spasticity as worse in some categories and improved in others but significant improvement in muscle length and strength in most categories which is associated with improvement in T25WT from 15.86 s and TUG 15.38 s at IA to T25WT 14.52 s and TUG 14.5 s at RA. However, at FA, he demonstrates increased PF spasticity and strength as trending worse associated with slower T25WT time of 17.8 s and TUG time of 16.06 s. At FA, Subject 3 experienced an increase in bilateral pedal edema, spasticity in lower legs and feet seen in increased PF spasticity and decreased gait testing speed but was able to generally maintain progress in spasticity and strength of hips and knees at FA. Subject 3 reports frustration with his diagnosis and disappointment that the intervention did not improve his neuropathy spasticity and walking beyond a 24-h period of improvement.
Subject 4 (spastic left lower extremity impacting gait with unilateral cane) demonstrated improvement in left lower extremity MAT, MMT, T25WT and TUG tests from IA to FA. Subject 4 improved TUG IA of 19.34 s and T25WT 17.64 s to FA TUG 15.6 s and T25WT 16.36 s. She also demonstrated improvement in ankle spasticity from 3/4 MAT PF tone with TA MMT of 3+/5 at IA to FA of 2/4 L ankle MAT associated with improved FA 4/5 TA MMT. Subject 4 reports walking further than she had been able to in years, correcting her left ankle foot drop at times and feeling encouraged.
Subject 5 (Left lower extremity spasticity and right lower extremity spasm impacted gait using 3WW indoor household distances for ambulation) demonstrated improvement bilaterally in MAT, MMT, T25WT and TUG tests from IA to FA. Subject 5 improved from IA TUG 19.5 s and T25WT 15.34 s to FA TUG 17.37 s and T25WT 13.53 s. He also demonstrated improvement in ankle spasticity from 3/4 MAT PF tone with TA MMT of 2/5 at IA to FA of 2/4 L ankle MAT associated with 2+/5 TA MMT strength. Subject 5 also demonstrated reduction in all categories of measured spasticity at IA down to 0/4 except residual but reduced spasticity of bilateral PF (right 1+/4 and left 2/4) MAT. Subject 5 reports feeling his left leg improved slightly in ability to loosen his left knee during the toe-off portion of walking which allowed him to use his hip better and walk further. Subject 5 states plan to invest in a version of electrical stimulation due to his response.
Subject 6 (Bilateral canes with intermittent right ankle foot orthotic use with weakness and spasticity limiting ambulation) demonstrated significant improvement in PF MAT, TA MMT, T25WT and TUG tests from initial assessment to final assessment. Subject 6 improved TUG from 54.75 s at initial assessment to 16.81 s at final assessment and T25WT from initial assessment of 36.88 s to 12.15 s at final assessment. He also demonstrated improvement in ankle spasticity from 3/4 MAT PF tone with TA MMT of 1+/5 at initial assessment to final assessment of 2/4 L ankle MAT associated with improved 2/5 TA MMT strength. Subject 6 reports feeling very supported by the visits and learning how to work with his body as well as improved walking especially from 10 pm to 11 pm with significantly reduced spasticity.
Subject 7 (Right lower extremity spasticity associated foot drop corrected with R AFO and 4WW for household ambulation) demonstrated improvement in MAT in PF, MMT and muscle length but was unable to tolerate ambulation testing at final assessment due to intolerance in probable urinary tract infection. At RA subject 7 demonstrates improvement in spasticity, strength and muscle length however a decline with worsened ambulation speed. At IA TUG 46.15 s and T25WT 27.94 s with RA TUG 47.5 s and T25WT 47.05 s. At IA, right lower extremity PF spasticity 3/4 with associated right TA strength of 2/5. At RA right PF spasticity down to 1+/4 with associated 3/5 TA MMT. At FA right PF spasticity remains 1+/4 associated with trending improvement right ankle dorsiflexion of 3+/5 MMT. Subject 7 reports despite the final appointment being disappointing due to her new urinary tract infection symptoms, that she feels stronger in her right leg and more comfortable with walking in her home overall.
In Table 3, MAT improvement is defined as at least 1 grade difference from IA to FA on a scale of 1+/4, 2/4, 3/4, and 4/4. MMT improvement is defined as at least 1/2 grade improvement. From IA to FA on a scale of 0/5, 1+/5, 2/5, 2+/5, 3/5, 3+/5, 4/5, 4+/5, 5/5. Per the American Physical Therapy Association Multiple Sclerosis Outcome Measure Taskforce, intrarater reliability for lower extremity assessment in subjects with MS is 71.1% but neither of these assessments have MCID or MDC data to reference. 9 Table 3 contains assessments for categorical measures shown by the count and percentage of patients who improved, stayed the same, and worsened over time (from pre to post).
Discussion
This case series of seven heterogenous subjects with MS is a low sample size for strong statistical analysis of results and should be considered a pilot study. The design is a multi-modal treatment approach which demonstrates a high level of feasibility and tolerance but cannot conclude cause and effect relationships, only possible correlations to further investigate. Possible other explanations for results measured include antispasmodic (baclofen) medication in 5 out of 7 subjects, the high frequency of PT visits, rapport with the primary investigator and multimodal interventions. There are no known adverse responses of DC and antispasmodics. Baclofen combined with therapy interventions including electrical stimulation improve functional outcomes in neurological patients. 10
Trends across subjects in spasticity and agonist strength show a possible correlation between mechanoreceptor input from DC allowing greater stretch and improved agonist strength. 71.4% of subjects demonstrated reduction in bilateral PF spasticity. 71.4% of subjects improved MMT of bilateral TA. Two subjects stood for the first time in more than 3 years with elimination of clonus they normally experience. Subject 6 demonstrated significant improvement in right lower extremity neuropathy and spasticity allowing significant improvement in gait mechanics and velocity over 25 to 50 feet. Subject 4 and 5 also demonstrated improvement in gait mechanics and gait velocity with reduction in spasticity and improvement in agonist strength. Subject 3 experienced FA worsening symptoms which caused a decline in gait mechanics and velocity. Impact on gait is inconclusive due to sample size and timeline.
Per findings by Etoom et al. (Systematic Review and Meta Analysis) 11 spasticity may be beneficial functionally by counteracting muscle weakness. 11 The goal in spasticity reduction interventions needs to be focused on preserving safe levels of function, while simultaneously improving an individuals’ access to normalized anti-gravity sagittal and frontal plane functional muscles. The article indicates that the best available quality of evidence is for robot assisted gait training and outpatient exercise programs on hypertonicity. This finding is in line with previous research. 12 Robot assisted gait training combines functional training with electrical stimulation demonstrating reduction in spasticity. This elucidates the benefit of combining functional training with electrical stimulation training.1,6,11,13 The reviewed articles demonstrate benefits in muscle tone, EMG muscle activity, biomechanical properties of movement and self-reported spasm but no effect on clonus or deep tendon reflex. 11 Per findings in this pilot, subjects 1 and 2 demonstrated elimination of clonus during and temporarily after treatment. This finding may distinguish this version of electrical stimulation (DC) from the TENS (AC) assessed in the systematic review. Clonus is a phasic jerk response as a result of a stretch at the extrafusal muscle fibers detected by the muscle spindle and transmitted to the CNS by Ia afferents that connect to propriospinal fibers. 2 In order for clonus to reduce, the mechanoreceptors and/or CNS Ia pathway needs to have input that allows normalized stretch.
Summary
Based on literature findings, the use of electrical stimulation in the form of FES bike and NMES is feasible for persons with progressive MS. These treatments may reduce falls, improve mobility, reduce physiological deconditioning and reduce spasticity. In all of these outcomes, further studies are indicated to make more definitive conclusions.3,14–17 In this pilot we can conclude that in individuals with progressive MS, DC is feasible and well tolerated when closely monitored and modified. This form of DC demonstrates the potential to reduce hypertonicity in forms of spasticity and clonus. In some cases, this treatment also demonstrates improvement in agonist muscle strength with trends toward improvement in functional outcome measures.
Traditional TENS application may reduce spasticity through the 1b inhibitory pathway short-term1,18,19 and the form of DC 5 used in this case series shows potential to reduce spasticity during treatment and carryover after treatments. In this pilot, this is demonstrated in trends of improving agonist strength especially dorsiflexion while simultaneously reducing spasticity, especially at PF. Due to subjects 1 and 2 being non-ambulatory and subject 7 not tolerating FA ambulatory gait speed testing, inconclusive evidence for gait speed improvement is available. However, 3/5 of ambulatory subjects showed trends towards improving gait biomechanics and speed. Most subjects show trends towards improvement in spasticity, strength and ROM. Subjects 1 and 2 with EDSS 7.5–8.0 were unable to ambulate or change their dependence on a chair for mobility, however, able to initiate functional standing during their study participation. The case series findings suggest further research is warranted.
Limitations
The primary limitations of this case series pilot study include a small sample size and treatment scope limited to 18 visits over 6 weeks, which limits generalizability of the findings and potential therapeutic effect of the study design on subjects with progressive MS. The study included a heterogenous mix of non-ambulatory and ambulatory individuals with multiple comorbidities limiting tolerance of treatment and impacting assessments. Inherent to the study is a multi-modal treatment approach which demonstrates a high level of feasibility and tolerance but cannot conclude direct cause and effect relationships, only possible correlations to further investigate. Inherit bias may occur with the study design of the primary investigator as primary author within a case series.
Future research would benefit from isolating the effect of DC on spasticity using a single or double blind randomized control trial with DC as the main therapy and a larger sample size limiting all subjects to either ambulatory or non-ambulatory and performed over a longer duration to increase generalizability and validity of findings. This unfunded study was limited in scope to one primary investigator and one Neurologist. All expenses in Institutional Review Board approval fees and publication fees have been covered by Neurological Fitness Equipment and Education LLC, Austin TX.
Future study designs of electrical stimulation or this specific version of DC should consider continued emphasis on functional application performed simultaneously with electrical current assessed with objective measurements in spinal reflex, spasticity and biomechanical properties of the gait cycle in order to best understand quantity and duration of reduced spasticity with correlation into functional changes.1,6
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The use of the NeuBie was approved by Centura Health biomedical department. This DC unit is an FDA approved unit (AP439; HILL IFC Interferential Unit; Neubie; Neuro-M Trainer Model A). CommonSpirit Health Research Institute Institutional Review Board provided approval of this study design and consent form (FWA Number: FWA 00019514 OHRP IRB Number: IRB00009715).
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure statement
NeuFit has covered the expenses required for institutional review board approval process as well as the fees associated with a third-party statistician. The investigators have not received any reimbursement for this study. The authors declare no potential conflicts of interest with respect to the research, authorship or publication of this article.
NeuBie by Neurological Fitness Equipment and Education LLC, Austin TX.
Manufacturer: Johari Electro Tech Co. (Jodhpur, India).
Appendix 1 (NeuBie direct current mapping)
A unique application of NeuBie direct current is mapping. The practitioner places a red electrode on the distal lumbosacral region of the subject and uses the black electrode lead attached to a carbon fiber electrode with wet sponge and scans across the surface of the skin at continuous 500 Hz current. The goal is to locate areas of interest indicating orthopedic hot spots, locations that allow increased range of motion from baseline, locations that demonstrate increased spasticity or spasm response and locations that have lower sensation than the established baseline. Once these locations are identified, the practitioner can place electrodes to specifically target orthopedic concerns, range of motion improvements, hypertonic regions and neuropathy.
Appendix 2 (NeuBie direct current electrical stimulation parameters used in study interventions)
NeuBie direct current electrical stimulation utilized for neuromuscular re-education, spasticity reduction and strengthening of lower extremity and trunk region based on mapping and motor points. Direct Current treatment is always combined with PT-based interventions and functional training lasting 15–45 min depending on tolerance with the following parameters:
Frequency is adjusted based on patient response from 35–500 Hz with goal of increasing time with 500 Hz. In mid-range frequency of 35–75 Hz the subject was given a 1:4–1:2 ratio of current on to current off time to allow for repolarization. In high frequencies of 100–500 Hz the current was used continuously. Intensity is to be adjusted to remain 70%–80% client reported perceived intensity and/or to be under threshold of any spasticity or pain.With electrodes in place emphasizing reduction in spasticity and improvement in range of motion out of hypertonic patterns, subjects were given flexibility treatment for gastrocnemius, soleus, hamstrings, adductors, quadratus lumborum, quadriceps and hip flexors. Following flexibility training subjects given AROM, AAROM and manual cues to guide non-compensatory agonist movement to greatest degree possible in movements such as dorsiflexion and eversion, knee extension, knee flexion, hip flexion, hip bridging, hip external rotation. Next, subjects trained at highest functional mobility challenge they were able to perform with controlled compensation possible in bed mobility, sitting posture, sit to stand, ambulation and standing balance.
Appendix 3 (NeuBie direct current foot bath neuropathy protocol used in study interventions)
Foot Bath for multiple sclerosis performed for 8–15 min for the affected side (if both affected then treated both simultaneously with different channels). Use 500 Hz continuous current. **Assessed with the client on comfortable range of temperature for water and adjusted temperature accordingly for comfort** Immersed the entire foot and ankle and high ankle in the water. Provided the following electrode placements target the locations nerve fibers are closest to the surface. The lumbar nerve roots to fill out as much of the sciatic and femoral nerve pathways and many bifurcations as possible
channel 1: Lumbar nerve roots to the affected side vertical electrode placement (red) channel 2: Mid adductor vertically placed electrode (red) channel 3: Popliteal fossa horizontally placed electrode (red) channel 4: Distal quad horizontally placed electrode (red)(all black electrodes were floating carbon fibers in the water, kept out of the way of the treated foot/feet.) During foot bath provided manual activations for lower leg muscles; talocrural glides (to encourage the calcaneous remain in contact with floor surface) grade 2–4 depending on tolerance, metatarsal glides, proximal phalanx glides and bilateral tendon massage just lateral to achilles .With locations that allowed for greater desired ankle or foot ROM continued to work and have client move through improved range as tolerated. With areas that cause reflexive response, decreased the intensity of manual work below a threshold that elicited the reflex and worked with client on diaphragmatic breathing with the work. After manual work assess for quality of movement especially into ankle dorsiflexion and eversion. When noticing compensation into inversion or weakness was present, then provided either AAROM, isometric hold or eccentric control into dorsiflexion and eversion and had the client move with correction or sustain a position. Throughout this process ensured the current was at just below the level that would cause spasticity and/or 7/10 intensity.